Molecular Transmission Dynamics of HIV-1 in Migrant Populations: Transmission Clusters and Demographic Diversity in Hangzhou, a Key Migration Hub in Eastern China
Sisheng Wu, Ling Ye, Xingliang Zhang, Min Zhu, Wenjie Luo, Zhou Sun, Junfang Chen, Ke Xu

TL;DR
This study explores how HIV spreads among migrant populations in Hangzhou, China, using genetic data to identify transmission clusters and demographic patterns.
Contribution
The study provides new insights into the role of migrant populations in HIV transmission and identifies population-specific factors influencing molecular transmission networks.
Findings
Migrant populations form multiple large HIV transmission clusters in Hangzhou.
PMP and NMP have higher inclusion rates in molecular transmission networks compared to TMP.
Factors like current residence and STD history are associated with network inclusion for migrants.
Abstract
Objective: Population mobility complicates the prevention and control of HIV. To address these challenges, this study explored the molecular epidemiology of HIV among migrant populations in Hangzhou. Methods: People newly diagnosed with HIV/AIDS from 2020 to 2023 were divided into permanent migrant population (PMP), temporary migrant population (TMP), and non-migrant population (NMP). HIV-1 pol gene sequencing was performed to calculate genetic distance. Sample pairs with genetic distances ≤0.005 were used to construct the molecular transmission network. Results: PMP comprised people living with HIV in Hangzhou, characterized by younger age, higher education, and predominantly homosexual transmission. This population forms multiple large molecular clusters together with NMP. TMP accounted for the highest proportion of females and people infected through heterosexual contact, but the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
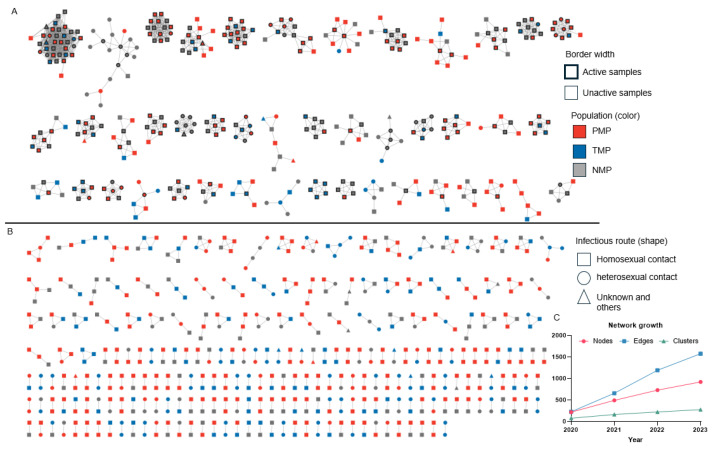 Figure 1
Figure 1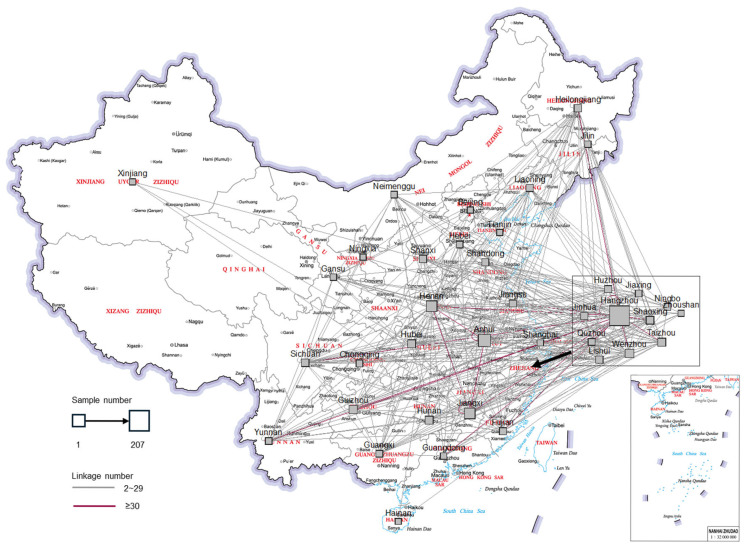 Figure 2
Figure 2- —Disease Prevention and Control Innovation Team of Zhejiang Province
- —Zhejiang Provincial Key Laboratory Construction Project
- —Construction Fund of Key Medical Disciplines of Hangzhou
- —Science and Technology Program for Disease Prevention and Control in Zhejiang Province
- —Open Research Fund of Zhejiang Key Lab of Vaccine, Infectious Disease Prevention and Control
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHIV Research and Treatment · HIV, Drug Use, Sexual Risk · HIV/AIDS Research and Interventions
1. Introduction
Hangzhou, the capital of Zhejiang Province and a central city in the Yangtze River Delta region, is the primary destination of migrant populations in Zhejiang Province. Data from the seventh national census indicate that Hangzhou attracts 18% of inter-provincial migrants and 75% of intra-provincial migrants to Zhejiang [1]. While migrant populations contribute to urban development and construction, they also present challenges to HIV/AIDS prevention and control. Sexual transmission had been the main channel of HIV transmission in Hangzhou [2]. Migrants engage in a considerable level of unprotected sexual behavior, presenting a significant HIV risk [3,4]. Their knowledge of infectious disease prevention is often insufficient, and they are prone to being infected with diseases [5]. If infected with HIV, their high mobility and broad activity range can expand transmission scope.
The HIV genome is highly variable, and its genetic sequence undergoes constant change within the host due to selection pressure [6,7]. Genetic distances derived from the gene sequence reflect sequence similarity and viral relatedness [8]. Through the topological mapping of these distances, cases with similar sequences cluster together, and all clusters form the molecular transmission networks [9,10]. The molecular transmission networks provide a visual representation of HIV molecular epidemiological patterns, help warn outbreaks and identify HIV transmission chains. They allow public health workers to target limited prevention resources more effectively. The large volume of sequences generated from HIV drug resistance testing has enabled countries, including China, the United States, and Bulgaria, to use these data for constructing molecular transmission networks and monitoring transmission dynamics [11,12,13,14,15].
The mobility of migrant populations who temporarily live in Hangzhou was stronger than those who permanently live in Hangzhou. The follow-up methods of the two groups are different: temporary migrant population receives follow-up at their household registration, while permanent migrant population receives follow-up therapy in Hangzhou. Therefore, in this study, based on the degree of population mobility, the people newly diagnosed with HIV were classified into permanent migrant population (PMP), temporary migrant population (TMP), and non-migrant population (NMP). We built the molecular transmission network in Hangzhou to analyze and compare the molecular epidemiological characteristics among the three groups, aiming to facilitate the precise prevention and control of HIV.
2. Materials and Methods
2.1. Study Population and Sample Collection
Plasma samples were collected from people newly diagnosed with HIV before receiving antiviral therapy in Hangzhou from 2020 to 2023. The inclusion criteria for the samples were as follows: (1) cases reported in Hangzhou; (2) the successful acquisition of HIV sequence; and (3) informed consent of the patient. Demographic and epidemiological information (e.g., age, gender, ethnicity, education, current residence, household registration, infectious route, and other HIV infection-related information) was obtained through face-to-face surveys.
In this study, people living with HIV were classified into permanent migrant population (PMP), temporary migrant population (TMP) and non-migrant population (NMP). PMP was the population whose current residence was Hangzhou but whose household registration was not. TMP was the population whose current residence and household registration were both not Hangzhou. NMP was the population whose current residence and household registration were both Hangzhou. The determination of the infectious stage at the time of diagnosis in this study was performed as follows: Early stage: People at this stage were infected with HIV within\6 months, and people had a high viral load and incomplete antigen–antibody reaction. The early stage should meet one of the following conditions: (1) the baseline viral load is greater than 10^6^ CPs/mL with positive serologic testing results and (2) the positive nucleic acid testing plus negative or indeterminate serologic testing results, and the patient is not in the late stage [16,17]. Samples in the early stage were not verified by Lag-Avidity, i.e., determination may be erroneous [18]. The late stage, also known as the AIDS stage, is determined according to the diagnosis and treatment guidelines [19]. Intermediate stage involves a person living with HIV who is neither in the early stage nor the late stage.
2.2. Nucleic Acid Extraction and Sequence
HIV-1 RNA was extracted from plasma samples using QIAamp Viral RNA Mini Kit (QIAamp, Hilden, Germany). The viral pol gene (including the full length of protease and the first 300 amino acid sites of reverse transcriptase, corresponding to positions 2253–3500 of the international reference strain HXB2) was amplified by reverse transcription PCR and nested PCR, and the primer design was based on reference [20]. The PCR products were sent to Shanghai Sangon Biological Engineering Co., Ltd. (Shanghai, China) for Sanger sequencing.
2.3. Sequence Processing
Sequencher 5.4.6 was used to splice the sequences; MEGA X was used to correct the spliced sequences; COMET [21], HIV Blast [22] and phylogenetic tree were used for subtype analysis of the sequences. Surveillance drug resistance mutations (SDRMs) and drug resistance were analyzed using HIV Drug Resistance Database (hivdb.stanford.edu). SDRMs were designed to be sensitive and the specific indicators of antiretroviral drug selection pressure, compared with drug resistance mutations: (a) they are commonly recognized as causing or contributing to resistance; (b) they are nonpolymorphic in untreated persons; and (c) they are applicable to all HIV-1 subtypes [23]. The R package ape was used to calculate the pairwise gene distance, and the calculation model was TN93 [24].
The molecular transmission network was constructed by screening molecular pairs with gene distance ≤0.005, and the molecular transmission was observed. Samples associated within the molecular propagation network are connected by line segments, independent graphical units are molecular clusters, and the number of samples connected by a single sample is the degree value. The molecular cluster size of ≥5 samples was defined as a large molecular cluster, and the samples with degree rank in the top 25% (degree ≥4 in this study) were defined as active samples. Sample inclusion rate was calculated by samples in network/all samples. If a certain group has a high inclusion rate, it means that this group is highly likely to enter the molecular network, and the virus transmission within this group is also intensive.
2.4. Statistical Analysis
R 4.4.2 was used for statistical analysis. The count data were expressed as the number of cases (constituent ratio), and the comparison between groups was analyzed by χ^2^ test. p < 0.05 was considered statistically significant. Multiple logistic regression was used to calculate odds ratios (ORs) and 95% confidence intervals.
3. Results
3.1. Demographic Information on Populations
From 2020 to 2023, a total of 4235 people were newly diagnosed with HIV in Hangzhou. Among them, 3615 people with successfully obtained sequences were included in this study, including 1583 PMP cases (43.79%), 1172 TMP cases (32.42%) and 860 NMP cases (23.79%), achieving a sample coverage of 85.36%. The household registrations of migrant populations, in the descending order of frequency, were Zhejiang Province, Anhui Province, Henan Province, Jiangxi Province, Guizhou Province, and other provinces with fewer cases (Table 1).
As shown in Table 1, all three groups were predominantly male, and TMP had the lowest proportion of male (86.35%), while PMP had the highest (94.06%). Most people were 16–40 years old, with PMP having the highest proportion in this range (77.57%). Regarding occupation, PMP had the highest proportion of business service staff (47.06%) and students (5.69%); TMP had the highest proportion of workers (17.24%), farmers (21.42%), and domestic service staff (15.61%); NMP had the highest proportion of employees (10.70%). Regarding marital status, PMP had the highest proportion of unmarried people (71.51%), while over 30% of both TMP and NMP were married. Regarding education, PMP had the highest proportion of people with college and above degrees (47.19%); TMP accounted for the highest proportion with junior high school education or below (54.27%). Regarding sample sources, PMP accounted for the highest proportion of voluntary counseling and testing (VCT, 29.37%) and sexually transmitted disease (STD) clinic (20.34%) sources. Regarding sexual experiences, PMP accounted for the highest proportion reporting only homosexual experiences (73.66%), TMP accounted for the highest proportion reporting only heterosexual experiences (43.17%), and NMP accounted for the highest proportion reporting both homosexual and heterosexual experiences (7.21%). PMP had the highest proportion with an STD history (20.09%). Regarding the infectious route, PMP accounted for the highest proportion of people transmitted through homosexual contact (78.08%), while TMP and NMP had higher proportions of people transmitted through heterosexual contact than PMP. NMP accounted for the highest proportion of people diagnosed at the early (5.81%) and late (37.79%) stages. All reported results were statistically significant (p < 0.05).
3.2. Drug Resistance and Subtype
The surveillance drug resistance mutation rate among confirmed cases from 2020 to 2023 was 3.87% (140/3615), and the pretreatment drug resistance rate was 8.63% (312/3615). The major drug resistance mutations in drug resistance viruses were Q58E in the protease region and S68G/N, M14V/I, K103E/N/S, E138A/G/K/Q, and V179D/E/L/T in the revertase region. No significant difference in drug resistance was observed among the three populations (Table S1). A total of 23 circulating recombinant forms (CRFs) and multiple unique recombinant forms (URFs) were identified. The main subtypes for PMP were CRF07_BC (48.07%), CRF01_AE (35.69%), and CRF55_01B (4.80%); for TMP, they were CRF07_BC (44.37%), CRF01_AE (31.06%), CRF08_BC (7.85%), and CRF55_01B (4.27%); and for NMP, they were CRF07_BC (44.30%), CRF01_AE (34.19%), and CRF08_BC (5.58%). The differences in viral subtypes were statistically significant (p < 0.001, Table 1).
3.3. Molecular Transmission
The molecular transmission network was constructed using a genetic distance threshold of <0.005 (Figure 1), and it included 833 people forming 275 molecular clusters, with a sample inclusion rate of 23.04%. The network comprised 767 males and 66 females, with 610 cases infected through homosexual contact and 201 through heterosexual contact. Inclusion rates for PMP, TMP and NMP were 27.04%, 18.94% and 21.28%, respectively. All molecular clusters involved migrant populations, PFP were present in 78.5% of molecular clusters (216/275), and TMP in 54.5% of molecular clusters (150/275). Network growth rate decreased annually, with node increase rates of 126%, 48% and 26% in 2021, 2022 and 2023, respectively (Figure 1C).
The molecular network obtained 44 large molecular clusters, with the largest molecular cluster containing 35 cases. There were 219 active samples, and the highest degree value was 32. The proportion of active samples was 35.16% for NMP, 26.17% for PMP, and 19.28% for TMP. The proportion of samples located in large molecular clusters was 51.65% for NMP, 39.72% for PMP and 28.25% for TMP. These differences were significant (Table 1). The frequency of connections between the groups from the highest to the lowest, was PMP-NMP (449), PMP-PMPs (355), PMP-TMP (260), NMP-NMPs (211), TMP-NMP (210), and TMP-TMP (91).
We analyzed the geographical distribution of household registration for samples within the molecular transmission network and present its map in Figure 2. Outside Zhejiang Province, many samples were from Anhui, Jiangxi, and Henan Provinces. Inside Zhejiang Province, most samples were from Hangzhou. Correspondingly, the most frequent inter-regional links were Hangzhou–Hangzhou, Anhui–Hangzhou, Jiangxi–Hangzhou, and Henan–Hangzhou.
To identify factors associated with network inclusion among migrants, multivariable logistic regression was performed with network entry as the dependent variable (Table 2). The cases that were easier to enter the network had higher inclusion rates. The results showed that cases with current residences in Hangzhou had higher inclusion rates than in others. Cases with household registration in Zhejiang Province had a higher inclusion rate than outside Zhejiang Province. Population with unknown STD history had a lower inclusion rate than population with STD history. Cases from VCT had higher inclusion rates than cases from other clinical sources and other sources. Cases at the late stage of diseases had a lower inclusion rate than the early stage.
4. Discussion
Hangzhou, as a central city in the Yangtze River Delta, experiences substantial population mobility, and migrant populations constitute 76.19% of people living with HIV, with PMP and TMP outnumbering NMP. The three populations showed significant differences in both demographic and molecular epidemiological characteristics. In this study, all the samples successfully obtained viral sequences, indicating high viral load infectiousness. This study reflects the ongoing HIV epidemic in Hangzhou and analyzes prevalent characteristics across populations, holding implications for targeted prevention. However, we have limitations in the method to detect accurate viral subtype, which only detect the pol gene. Moreover, phylogenetic analysis would somewhat be different from the real world and cannot reflect the direction of transmission. All participants of this study remain anonymous, and refusal by participants would not result in any consequences. Newly infected people received antiviral therapy upon their own request.
PMP constitutes nearly 40% of permanent residents in Zhejiang Province [25]. This population typically consists of formally employed individuals with stable work and residence, mostly of working age and highly educated, contributing significantly to regional development. These characteristics suggest PMP is more open-minded and adept at utilizing online platforms to seek same-sex sexual partners. The highest proportion of the CRF55_01B subtype in PMP may be related to this group’s higher rate of homosexual behavior, consistent with previous reports that this subtype primarily circulated among MSM populations [26].
We found PMP had relatively high self-testing awareness, as indicated by their highest proportions from VCT and STD. This likely contributed to their lower proportion of late-stage diagnoses. Motivation for self-testing among PMP may stem from partner notifications or personal hindsight. However, their higher education level is associated with a greater use of anonymous online platforms for partner-seeking, which can complicate contact tracing and delay testing, resulting in a lower early-diagnosis proportion compared to NMP. Further health promotion via new media targeting this unmarried, highly educated group is needed to enhance their protective behaviors and self-testing awareness.
TMP exhibits higher mobility than PMP, and they mainly comprise temporary visitors to Hangzhou and informal workers without local social insurance. Hangzhou’s robust healthcare system and cross-regional medical insurance policies attract patients from other regions [27]. The willingness of temporary visitors to seek medical care in Hangzhou is also strong; therefore, people living elsewhere had tested positive for HIV in Hangzhou. Informal workers are characterized by irregular hours, diverse workplaces, variable pay, informal labor relations, and weak social security, resulting in lower social integration than formal workers [28,29]. Although they are persistently living in Hangzhou like PMP, it is more difficult to track sexual partners and conduct testing for informal workers.
Homosexual contact remained the primary transmission route for TMP. This group of men who have sex with men (MSM) was difficult to track due to the prevalence of anonymous online platforms and high mobility. The molecular transmission network in Hangzhou was mainly composed of the MSM population, and utilizing this network can help identify sexual partners within the MSM population, reducing the difficulty of sexual partner tracking. To lower the incidence of TMP, efforts can focus on informal workers, providing humanitarian care tailored to their high working hours and low social security, alleviating psychological pressure, and effectively promoting awareness.
Following infection, HIV continuously mutates, increasing genetic distance between donor and recipient strains. HIV pro/rt diverges from the founder strain at a rate of about 0.1~0.2% per site per year. A threshold of 0.005 was recommended to identify molecular transmission relationships within about 3 years. This threshold can sensitively identify recent links and avoid false links [30,31]. The primary inter-regional links observed were from Jiangxi, Anhui, and Henan Provinces to Hangzhou, suggesting that migrants from these regions are deeply involved in local transmission. This pattern extends beyond Hangzhou; our previous study found genetic similarities between sequences from Hangzhou and those from other major economic hubs such as Shenzhen, Beijing, and Guangzhou [32]. Collectively, these cities are key migration destinations due to their economic development. The data presented in Figure 2, combined with these genetic links, support the hypothesis that migrants from developing provinces such as Jiangxi, Anhui and Henan contribute significantly to HIV transmission across multiple economically developed cities. Several larger molecular clusters included cases infected via both homosexual and heterosexual contacts, the latter primarily being men. This suggesting that some individuals may not disclose heterosexual behavior during investigations or may have undisclosed female partners.
The deep participation of PMP in social and economic activities was accompanied by the local transmission of HIV. Over half of samples in the molecular transmission network were of PMP, and most molecular associations also involved PMP. TMP is present in over half of molecular clusters, and primarily linked to PMP, suggesting they bridge multiple intercity and inter-provincial transmission chains. NMP had the highest proportion of active samples, and the highest presence in large molecular clusters, suggesting that it could be serve as starting points for contact tracing, potentially extending to migrant contacts.
Logistic regression analysis indicated that TMP residing in other cities within Zhejiang Province had the lowest network inclusion rate, possibly because their social and sexual networks remain centered outside Hangzhou. Cases with STD testing histories had stronger self-testing awareness, making them more likely to be found in the networks. Due to the long infection period, it was difficult to find people that were associated with late-stage-diagnosed people. Late-stage-diagnosed people may acquire HIV outside Hangzhou. To trace their sexual partners outside Hangzhou, we recommend improving intercity cooperation and information sharing.
In summary, most people living with HIV in Hangzhou are migrant populations, who played a major role in ongoing HIV transmission. PMP entails young and highly educated people, primarily comprising the MSM population, and serves as the main driver of local transmission, forming large molecular clusters with NMP. TMP has complex origins, with a relatively high proportion infected through heterosexual contact, playing an important role in viral flow. Informal workers in TMP are a key target for intervention. To reduce undiagnosed infection and transmission, targeted health promotion for unmarried, highly educated individuals and informal workers should emphasize condom use, correct post-exposure prophylaxis, and timely self-testing. The use of molecular transmission networks can help uncover transmission chains, optimize resource allocation, and address the challenges of rapid intercity and inter-provincial viral mobility.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Zhejiang Provincial Bureau of Statistics The Seventh Series Analysis of Population Census in Zhejiang Province: Floating Population Zhejiang Provincial Bureau of Statistics Hangzhou, China 2022
- 2Ye L. Xu K. Zhang X. Luo W. You J. Wu S. Zhu M. Analysis of HIV-1 Subtypes and Pretreatment Drug Resistance in Newly Reported HIV/AIDS Cases in Hangzhou, 2020–2022 Chin. J. Microbiol. Immunol.20234354154610.3760/cma.j.cn 112309-20230330-00077 · doi ↗
- 3Dai S. Shen Y. Liu A. Zhang J. Wu J. Awareness of AIDS Knowledge and HIV Infection Status among Male Floating Population in Anhui Province China Prev. Med. J.202436674678,68210.19485/j.cnki.issn 2096-5087.2024.08.007 · doi ↗
- 4He B. Qin M. Nong L. Tang H. Liu J. Huang Z. Analysis on Condom Use in High-Risk Sexual Behavior among Male Floating Population in Nanning City from 2017 to 2021 Occup. Health 202440484489+49510.13329/j.cnki.zyyjk.2024.0097 · doi ↗
- 5Du J. Zhang W. Cao X. Wang N. Zhao M. Lin J. Factors Associated with the Health Education on the Prevention and Treatment of Infectious Diseases among Migrants in China China Prev. Med.20232429930410.16506/j.1009-6639.2023.04.004 · doi ↗
- 6Sun N. Yau S.S.-T. In-Depth Investigation of the Point Mutation Pattern of HIV-1Front. Cell. Infect. Microbiol.202212103348110.3389/fcimb.2022.103348136457853 PMC 9705751 · doi ↗ · pubmed ↗
- 7Cuevas J.M. Geller R. Garijo R. López-Aldeguer J. Sanjuán R. Extremely High Mutation Rate of HIV-1 In Vivo P Lo S Biol.201513 e 100225110.1371/journal.pbio.100225126375597 PMC 4574155 · doi ↗ · pubmed ↗
- 8Han X. Zhao B. An M. Zhong P. Shang H. Molecular Network-Based Intervention Brings Us Closer to Ending the HIV Pandemic Front. Med.20201413614810.1007/s 11684-020-0756-y 32206964 · doi ↗ · pubmed ↗