Efficacy, Immunogenicity, and Safety of Enterovirus 71 Vaccines in Children: A Systematic Review and Meta-Analysis
Guan Xing Lai, Albert Ka Wing Au, Edmond Siu Keung Ma

TL;DR
This study reviews the effectiveness, immune response, and safety of EV71 vaccines in children, showing high efficacy and safety.
Contribution
The study provides a comprehensive meta-analysis of EV71 vaccine efficacy, immunogenicity, and safety in children.
Findings
EV71 vaccines showed high efficacy (90-97%) against HFMD in children under 5 years.
Seropositive and seroconversion rates were over 96% after two vaccine doses.
Serious adverse events were slightly lower in the vaccine group compared to placebo.
Abstract
Background/Objectives: Hand, foot and mouth disease (HFMD) caused by enterovirus 71 (EV71) may cause severe complications and death in children. It is also a common cause of outbreaks in the Asia-Pacific Region. Incidence among children 1 to <2 years was over 3000/100,000 population in China. A systematic review and meta-analysis was performed to review evidence on vaccine efficacy (VE), immunogenicity, and safety of two doses of EV71 vaccine in children. Methods: Randomized controlled trials (RCTs) comparing EV71 vaccine with placebo or with another EV71 vaccine in children and adolescents aged ≤18 years were searched on PubMed, Medline, Embase, CENTRAL, and CNKI (Chinese) in week 5 November 2024. The reference list of each study and the websites of vaccine manufacturers were also searched. The Cochrane Risk of Bias 2 tool (RoB2) was used to assess the risk of bias. VE, immunogenicity…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
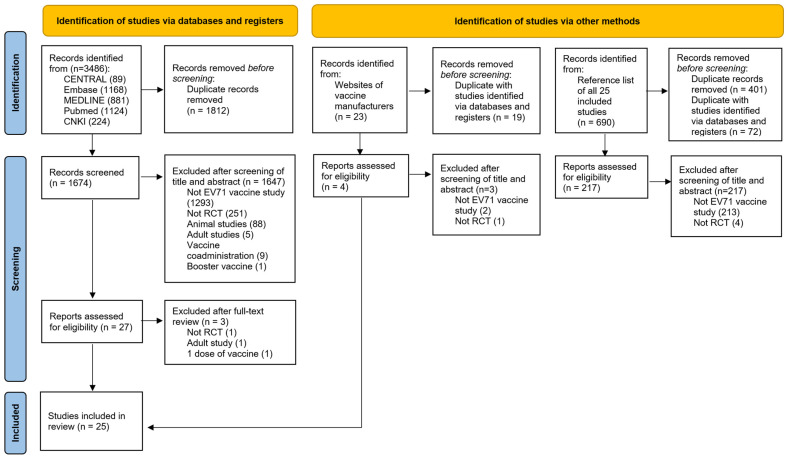 Figure 1
Figure 1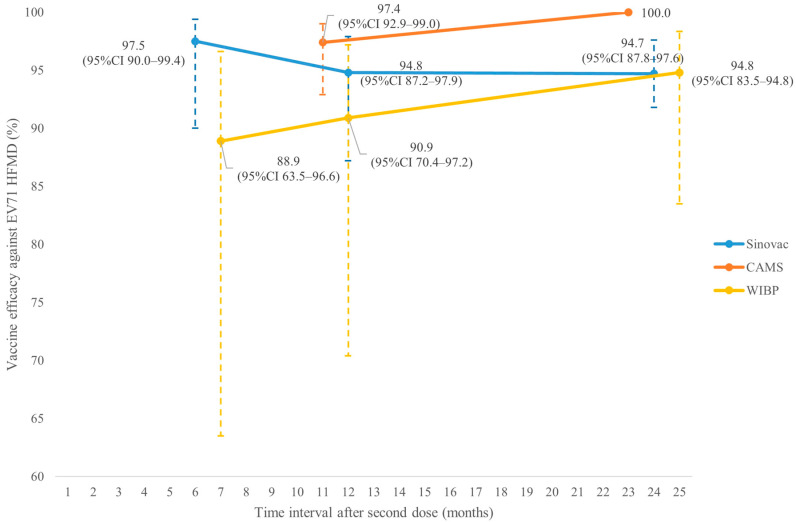 Figure 2
Figure 2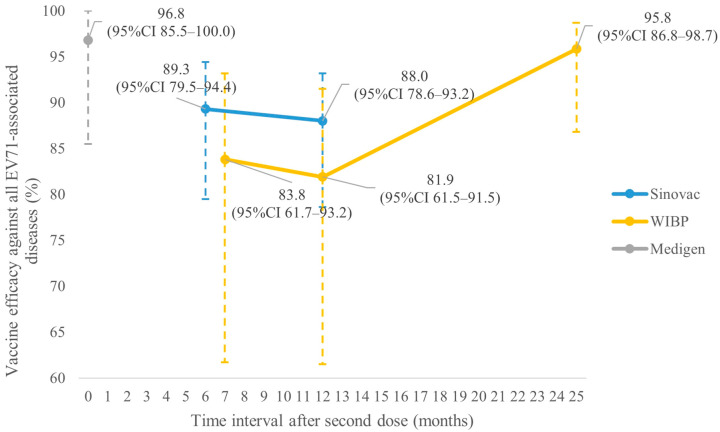 Figure 3
Figure 3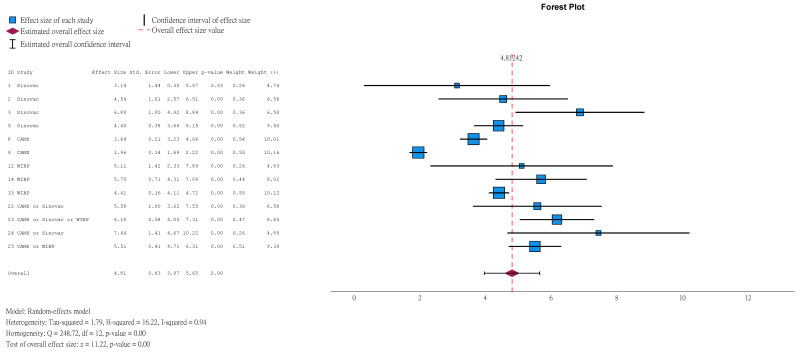 Figure 4
Figure 4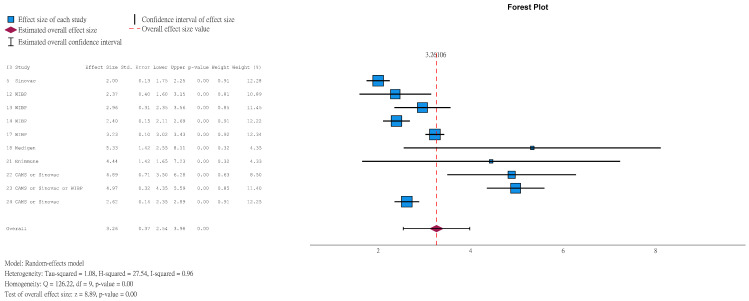 Figure 5
Figure 5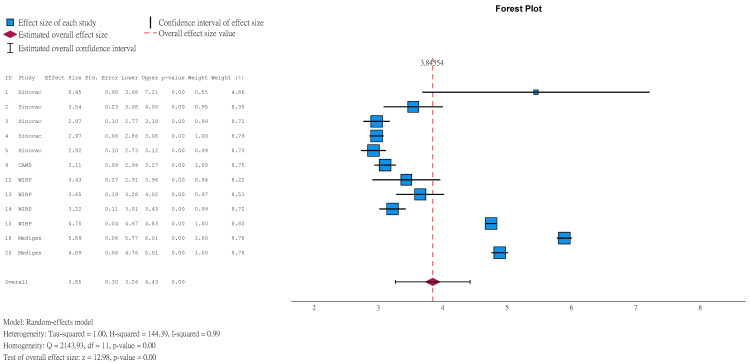 Figure 6
Figure 6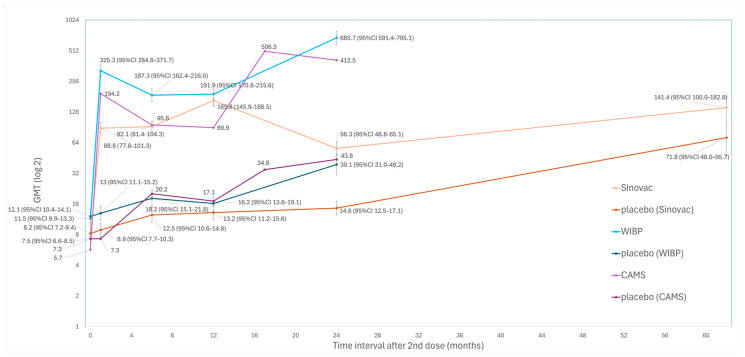 Figure 7
Figure 7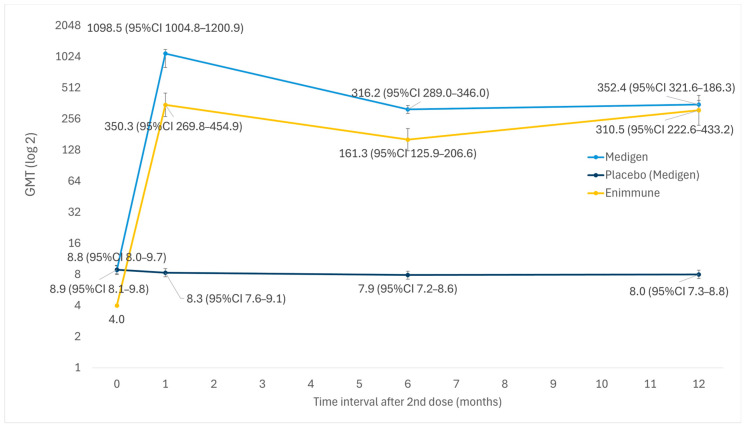 Figure 8
Figure 8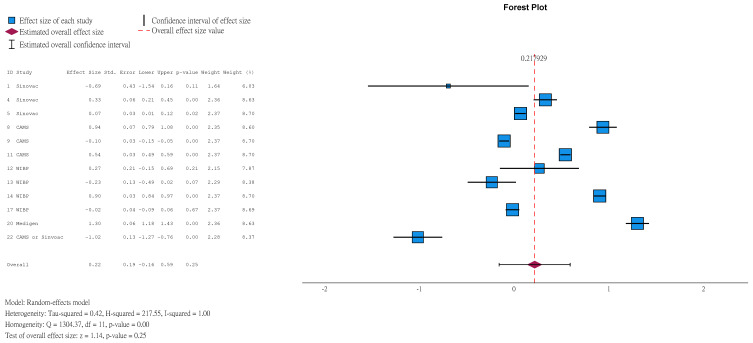 Figure 9
Figure 9Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsViral Infections and Immunology Research · Animal Disease Management and Epidemiology · Virology and Viral Diseases
1. Introduction
According to the World Health Organization (WHO), hand, foot and mouth disease (HFMD) is a ‘febrile illness with papulovesicular rash on palms and soles, with or without vesicles/ulcers in the mouth’. HFMD is caused by enteroviruses, mainly affecting children. It is transmitted by fecal–oral and respiratory secretions [1]. HFMD is mostly self-limiting and resolves in 7–10 days [2]. However, Enterovirus 71 (EV71) infection is of particular concern since it may cause severe complications in children, especially those aged ≤5 [3]. According to the World Health Organization, approximately 10–30% of hospitalized cases during EV71-associated HFMD epidemics in Asia developed central nervous system complications, including aseptic meningitis, encephalitis and acute flaccid paralysis. Fatal cases often developed acute refractory myocardial dysfunction and fulminant pulmonary oedema [1]. Long-term sequelae were related to greater clinical severity at the acute stage, neurological damage and younger age of onset. These may include: dysphagia requiring tube feeding, central hypoventilation with ventilator support, neurodevelopmental delay, impaired cognition, seizure, limb weakness and behavioral problems [4]. EV71 infection also caused significant economic loss. A USA study published in 1998 estimated direct medical costs of USD63–422/case, mainly attributable to parental missed work [5,6]. Another Chinese study published in 2017 estimated medical costs of USD113–677/case [7]. The Asia-Pacific region had cyclical EV71 outbreaks affecting Malaysia, China, and Vietnam, with major outbreaks occurring every 3–4 years [8,9,10]. From 2008 to 2017, around 18 million HFMD cases were reported in China (incidence = 134.59/100,000 population), 151,194 (0.85%) of which were severe, and most of those (89.66%) were children < 5 years old; 3623 (0.02%) of which died, and most of those (97.96%) were children < 5 years old. Incidence in children < 5 was much higher than that of the general population: incidence at age < 1 years, 1 to <2 years, 2 to <3 years, 3 to <4 years and 4 to <5 years was 1084, 3184, 2547, 2052 and 1151 per 100,000 population, respectively. Among laboratory-confirmed HFMD cases, 42.97% were caused by EV71 [11]. Management of HFMD is mainly supportive, and no antivirals are available. In places without the EV71 vaccine, the mainstay of prevention of HFMD is maintaining personal and environmental hygiene. Control measures of school outbreaks include strengthening infection control, excluding sick children from school, or even school suspension. Although these public health measures are shown to be effective in controlling HFMD [12], vaccination is considered of utmost importance in reducing the disease burden.
The first EV71 vaccine was approved in the Chinese Mainland in December 2015 [13]. Currently, there are five vaccines approved worldwide, with all approved in China (three in the Chinese Mainland, and two in Taiwan, China) (Table 1). All approved vaccines are inactivated vaccines. The three vaccines approved in the Chinese Mainland were developed from sub-genotype C4 and approved for use in children aged 6–71 months. The remaining two vaccines approved in Taiwan, China, were developed from sub-genotype B4 and approved for use in children aged 2–71 months. The interval between doses is 28 days for all vaccines except Medigen. We aimed to review evidence on vaccine efficacy (VE), immunogenicity, and safety of two doses of EV71 vaccine in children.
2. Methods
This study was conducted following the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guideline [24]. This review was registered with PROSPERO (registration number: CRD420261306764).
2.1. Search Strategy
PubMed, Medline (via Ovid, 1946 to week 5 November 2024), Embase (via Ovid, 1974 to week 5 November 2024), Cochrane Central Register of Controlled Trials (CENTRAL) (via Cochrane Library issue 10/2024), and China National Knowledge Infrastructure (CNKI) were searched in week 5 November 2024. The reference lists of each study and the websites of vaccine manufacturers [25,26,27,28,29] were also searched to identify all relevant studies. Keywords used for the search included: (‘enterovirus’ or ‘EV’) AND (‘71’ or ‘A71’) AND (‘vaccin*’). For Chinese literature, keywords included: (‘腸病毒’ or ‘腸道病毒’) AND (‘71’ or ‘A71’) AND (‘疫苗’). Both traditional and simplified Chinese characters were used for searching.
2.2. Eligibility Criteria
Randomized controlled trials (RCTs), conducted in children and adolescents aged ≤18 years, comparing EV71 vaccine with placebo or with another EV71 vaccine were included. Exclusion criteria included: (1) non-RCT study; (2) conducted in animals, or adults; (3) studies on coadministration of vaccines (since coadministration might affect immunogenicity of vaccines); and (4) studies using 1 vaccine dose only, or booster doses (>2 doses). The first author conducted the literature search, screening and trial selection.
2.3. Data Extraction
The following data were extracted from the included studies by the first author: (1) first author and year of publication; (2) phase of trial; (3) location of study; (4) age of study population; (5) sample size; (6) vaccine dosage and its interval between 1st and 2nd dose; and (7) outcomes assessed. The outcomes assessed included VE (%), immunogenicity (including seropositive rate, seroconversion rate, geometric mean titer (GMT), Geometric Mean Fold Increase (GMFI)), and rate of adverse events in both vaccine and placebo groups.
2.4. Risk of Bias Assessment
The Cochrane Risk of Bias 2 tool (RoB2) [30] was used by the first author to assess risk of bias in included studies.
2.5. Certainty of Evidence Assessment
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) tool was used to judge the certainty of evidence.
2.6. Data Synthesis and Statistical Analysis
Meta-analysis was performed for each outcome in each group using IBM SPSS 29. Heterogeneity was assessed by Cochran’s Q and I2 statistic and interpreted according to Cochrane guidelines (0–40%: might not be important; 30–60%: moderate heterogeneity; 50–90%: substantial heterogeneity; 75–100%: considerable heterogeneity) [31]. A random effects model was adopted due to significant heterogeneity. The restricted maximum likelihood estimator was employed. Study results were weighted by the inverse of their variance. Subgroup analysis for children with a seronegative baseline was conducted. For studies that did not report an overall result for subgroups, subgroup results were combined before meta-analysis. For study results of 0% or 100%, a fixed continuity correction of 0.5 was applied. Sensitivity analysis was performed by the leave-one-out method for meta-analyses with ≥3 studies. For meta-analyses with more than one study requiring continuity correction, further sensitivity analysis was performed by excluding all studies requiring continuity correction. For meta-analyses with ≥10 studies, publication bias was evaluated by visual inspection of a funnel plot and Egger’s test.
3. Results
3.1. Literature Search
Figure 1 shows that 3486 (3262 English and 224 Chinese), 23, and 690 articles were identified from electronic databases, websites of vaccine manufacturers, and reference lists of all included studies, respectively. A total of 2304 duplicates were removed, and 1867 were excluded after screening the title and abstract. Three studies were excluded after full-text review. A total of 25 studies were finally included in this systematic review (Table 2). The number of studies on Sinovac, CAMS, WIBP, Medigen and Enimmune vaccines was seven, four, six, three and one, respectively. Four studies were head-to-head trials between different vaccines.
3.2. Risk-of-Bias Assessment
Figure S1 showed the RoB2 risk-of-bias assessment result. Study 8 had high bias risk. Studies 6, 10, 16 and 17 had ‘some concerns’. The rest had low risk.
3.3. Certainty of Evidence Assessment
Study results were mostly of high certainty (Table S1).
3.4. Vaccine Efficacy
Figure 2 shows that VE (%) against EV71 HFMD in children aged ≤5 years of Sinovac at 6, 12 and 24 months after the second dose were 97.5% (95%CI 90.0–99.4), 94.8% (95%CI 87.2–97.9) and 94.7% (95%CI 87.8–97.6), respectively (studies 5 and 6). For WIBP, the corresponding results at 7, 12 and 25 months were 88.9% (95%CI 63.5–96.6), 90.9% (95%CI 70.4–97.2) and 94.8% (95%CI 83.5–94.8), respectively (studies 14 and 16). The corresponding results for CAMS at 11 and 23 months were 97.4% (95%CI 92.9–99.0) and 100.0%, respectively (studies 9 and 10). Figure 3 shows that VE (%) against all EV71-associated diseases of Sinovac at 6 and 12 months after the second dose was 89.3% (95%CI 79.5–94.4) and 88.0% (95%CI 78.6–93.2), respectively (study 5). The corresponding results for WIBP at 7, 12 and 25 months were 83.8% (95%CI 61.7–93.2), 81.9% (95%CI 61.5–91.5) and 95.8% (95%CI 86.8–98.7), respectively (studies 14 and 16). For Medigen, the corresponding result at 14 days was 96.8% (95%CI 85.5–100.0, study 20). The VE against EV71 HFMD severe complications of Sinovac at 6 and 12 months after the second dose was 100% (95%CI 42.4–100) and 100% (95%CI 42.6–100), respectively (study 5). At 11 months, no severe case was reported in the vaccine group of CAMS (study 9). The VE against EV71 HFMD hospitalization of Sinovac at 6 and 12 months after the second dose was 100% (95%CI 83.7–100) and 100% (83.7–100), respectively (study 5). The corresponding results for WIBP at 7 months and Medigen at 7 days were 100% (95%CI 41.6–100) and 81% (95%CI −12.3–100), respectively (studies 14 and 20).
3.5. Immunogenicity
Neutralizing antibody titer (NAbT) after vaccination was measured by assays involving serial dilution of serum. NAbT ≥ 1:8 indicated seropositivity. The greater the dilution, the higher the NAbT (e.g., NAbT ≥ 1:16 is higher than NAbT ≥ 1:8). The higher the NAbT, the more likely the child is protected from infection.
3.5.1. Seropositive Rate
Among children aged ≤5 years in the vaccine group, 99.19% (95%CI 98.15–99.65) achieved NAbT ≥ 1:8 at 1 month after the second dose (Figure 4), compared to 17.50% (95%CI 10.58–27.57) in the placebo group (Figure S2). Among those with a seronegative baseline (pre-vaccination NAbT < 1:8), the corresponding results were 99.30% (95%CI 96.99–99.84, Figure S3) and 7.95% (95%CI 3.41–17.44, Figure S4). At 1 month after the second dose, 98.52% (95%CI 96.40–99.40, Figure S5) and 10.92% (95%CI 2.01–42.25, Figure S6) of children aged ≤5 years in the vaccine and placebo groups achieved NAbT ≥ 1:16, respectively. Among those with a seronegative baseline, results were 99.25% (95%CI 96.12–99.86, Figure S7) and 2.08% (95%CI 1.26–3.42, Figure S8), respectively. Similarly, 97.01% (95%CI 93.00–98.76, Figure S9) and 8.96% (95%CI 3.62–20.52, Figure S10) of participants in the vaccine and placebo groups achieved NAbT ≥ 1:32, respectively. Among those with a seronegative baseline, results were 96.24% (95%CI 90.23–98.61, Figure S11) and 3.09 (95%CI 1.32–7.05, Figure S12).
3.5.2. Seroconversion Rate
Seroconversion was defined as NAbT ≥ 1:8 for participants with a seronegative baseline, or at least a 4-fold rise in NT after vaccination for participants with baseline NAbT ≥ 1:8. Results showed that 96.30% (95%CI 92.71–98.17) of children aged ≤5 years in vaccine group achieved seroconversion at 1 month after the second dose (Figure 5), compared to 4.96% (95%CI 2.37–10.08, Figure S13) in the placebo group. Among those with a seronegative baseline, results were 98.93% (95%CI 96.85–99.64, Figure S14) and 3.63% (95%CI 1.83–7.08, Figure S15).
3.5.3. Geometric Mean Titer (GMT)
GMT is a measure of NAbT. The greater the value, the higher the NAbT. In children aged ≤5 years, at 1 month after the second dose, the GMT in the vaccine group was 46.78 (95%CI 26.18–83.61) times that in the placebo group (Figure 6). Among those with a seronegative baseline, the ratio was higher at 60.99 (95%CI 28.58–130.17, Figure S16).
Older children had a higher GMT than younger children. Four studies compared GMT in children aged 6–11 months with those aged 1–4 years at 1 month after the second dose. The GMT of those aged 1–4 years was 76% higher than that of younger children (ratio = 1.76, 95%CI 1.12–2.76, Figure S17). Three studies compared the GMT in children aged 6–35 months with those aged 3–5 years. The GMT of those aged 3–5 years was 79% higher than that of younger children (ratio = 1.79, 95%CI 0.93–3.46, Figure S18), though the result was not statistically significant.
Figure 7 showed that only several studies (studies 5, 6, 7, 10, 14 & 16) examined longer-term GMT. While longer-term GMT remained high, all sub-genotype-C4 vaccine groups showed a transient decrease in GMT at some timepoints in the first 2 years. The GMT of Sinovac increased from 88.8 (95%CI 77.8–101.3) at 1 month to 165.8 (95%CI 145.9–188.5) at 1 year, followed by a decrease to 56.3 (95%CI 48.8–65.1) at 2 years, then an increase to 141.4 (95%CI 100.0–182.8). The GMT of WIBP peaked at 325.3 (95%CI 284.8–371.7) at 1 month, decreased to 187.3 (95%CI 162.4–216.0) at 6 months, then increased to 685.7 (95%CI 591.4–795.1) at 2 years. The GMT of CAMS peaked at 194.2 at 1 month, followed by a decrease to 89.9 at 12 months and an increase to 506.5 at 17 months.
An increasing trend of GMT was observed in all placebo groups. The GMT of Sinovac’s placebo group increased from 8.2 (95%CI 7.2–9.4) at day 0 to 14.6 (95%CI 12.5–17.1) at 2 years and 71.8 (95%CI 48.0–95.7) at 5 years. The GMT of WIBP’s placebo group increased from 12.1 (95%CI 10.4–14.1) at day 0 to 39.1 (95%CI 31.0–49.2) at 2 years. The corresponding results for CAMS were 7.3 and 412.5, respectively.
The only study (study 7) that studied GMT at 5 years showed that GMT at 5 years was higher than that at 2 years in both the vaccine and placebo groups.
Medigen and Enimmune vaccines were based on sub-genotype B4. Figure 8 showed that vaccination led to a significant increase in GMT, which remained at high levels at 1 year after vaccination.
3.5.4. Geometric Mean Fold Increase (GMFI)
GMFI represents the fold increase in GMT before and after vaccination. GMFI in the vaccine group at 1 month after the second dose in children aged ≤5 years was 28.41 (95%CI 22.18–36.39) times that of the placebo group (Figure S19).
3.6. Safety
At 1 month after the second dose, there were no statistically significant differences in the rate of any adverse events (AEs) (55.43% (95%CI 46.08–64.41) vs. 58.57% (95%CI 50.09–66.56), Figure 9, Figures S20 and S21) and unsolicited AEs (20.19% (95%CI 3.50–63.83) vs. 33.56% (95%CI 9.17–71.65), Figures S28–S30) between vaccine and placebo groups in children aged ≤5 years. The rate of serious AEs was lower in the vaccine group than the placebo group (1.23% (95%CI 0.58–2.69) vs. 1.34% (95%CI 0.58–3.07), Figures S22–S24) in children aged ≤5 years at 1 month after the second dose. There were no significant differences in the rate of solicited AEs (50.15% (95%CI 46.32–53.98) vs. 47.80% (95%CI 41.66–54.00), Figures S25–S27), systemic AEs (45.69% (95%CI 43.28–48.11) vs. 44.08% (95%CI 42.58–45.59), Figures S31–S33), and local AEs (15.53% (95%CI 6.98–31.04) vs. 9.69 (95%CI 2.03–35.75), Figures S34–S36) between vaccine and placebo groups in children aged ≤5 years at 7 days after the second dose.
Three studies showed that AEs in the vaccine group were less frequent in older children than in younger children at 1 month after the second dose. Study 4 showed a lower incidence of AEs in children aged 3–5 years than in children aged 6–35 months (47.0% vs. 60.4%, p = 0.003). Study 11 showed that the incidence of AEs decreased with increasing age (age 36–71 months: 28.9%, 24–35 months: 30.73%, 12–23 months: 40.23%, 6–11 months: 42.34%, p < 0.001). In study 13, the incidence of AEs in children aged 12–36 months was lower than in those aged 6–11 months (30.8% vs. 57.5%, p < 0.001).
3.7. Sensitivity Analysis and Publication Bias
Sensitivity analyses by the leave-one-out method showed that no single study significantly altered pooled estimates (Figures S37–S74). The results after excluding all studies requiring continuity correction did not differ significantly from the main analysis (Figures S75–S80). Potential publication bias was identified for the seropositive rate with NAbT ≥ 1:8 at 1 month, seroconversion rate at 1 month, ratio of GMT at 1 month, and rate of serious AEs at 1 month. However, publication bias was not identified for the rate of any AE at 1 month, and the difference in the rate of serious AEs between the vaccine and placebo groups at 1 month (Figures S81–S86, Table S2).
4. Discussion
The results showed that EV71 vaccines provided adequate protection to children (including those with a seronegative baseline), as evidenced by high VE, seropositive rate, seroconversion rate, GMT ratio and GMFI ratio. Overall increasing trend of GMT in the 5-year follow-up period in both sub-genotype-C4 vaccine groups and placebo groups suggested that exposure to community-circulating virus might have boosted immunity. Persistence of immunity might not be the sole result of vaccination but a result of vaccination and exposure to the circulating virus. However, all sub-genotype-C4 vaccine groups showed a transient decrease in GMT at some timepoints in the first 2 years, suggesting the possibility of some degree of immunity weaning after vaccination. The GMT in older children was much higher than that of younger children. Possible reasons included: more mature immune system [35] and higher baseline antibody level [42]. The safety profile was satisfactory since there was no statistically significant difference in AEs between the vaccine and placebo.
For the three vaccines approved in the Chinese Mainland, two review articles, published in 2016 [51] and 2021 [52], respectively, described the same phase 3 trials’ VE results against EV71 HFMD at 1 year follow-up. For the immunogenicity and safety analysis, our study included several more studies in addition to the five studies included in the 2016 article. A meta-analysis was performed to provide a better overview of results. Our study also provided longer-term immunogenicity results up to 5 years post-vaccination. Immunogenicity and safety were not studied in the 2021 article. For the two vaccines approved in Taiwan, China, studies were not yet published in 2016, while the phase 3 trial of Medigen was not yet published in 2021.
4.1. Limitations of the Included Studies
There were several limitations of the studies included in the review. Firstly, it was difficult to determine NAbT that is ‘protective’, and there was no international standard [32,49]. Secondly, most studies were unable to assess the duration of protection and antibody weaning due to limited follow-up time [22,32,38,39,47]. Thirdly, if background disease incidence was high, measured NAbT and VE would be higher due to immunity from natural infection [17,33,36,37,43,46]. Fourthly, underreporting of disease in vaccine recipients due to milder disease might overestimate VE [46]. Fifthly, the sample size was insufficient to detect very rare adverse events [9]. Lastly, cellular immunity and cross-genotype protection was not investigated [8,22,49].
4.2. Limitations of Meta-Analysis
Studies provided a wide range of results for GMT, GMFI and rate of AEs. This could be due to different study locations, study population, background epidemiology, and study methodology (e.g., differences in assays used for measuring GMT and different methods of monitoring AE). Heterogeneity might also cause asymmetry in funnel plots and significant results in Egger’s test in the absence of publication bias. Despite significant heterogeneity, the overall estimate by meta-analysis was compatible with the results of individual studies, i.e., vaccines were able to elicit an immune response, and there was no significant difference in AEs between the vaccine group and the placebo group. Sensitivity analyses also showed that results are robust.
VE, seropositive rate, and seroconversion rate in the vaccine group were affected by heterogeneity to a smaller extent, since all included studies provided a narrow range of similar results.
4.3. Implications for Policy and Future Research
Cross-protection against other viral strains should be studied. Currently marketed vaccines were developed based on sub-genotype C4 or B4. The ability of the vaccines to elicit an immune response against other strains warrants further investigation. The vaccine would likely be more effective if cross-protection was demonstrated. Some studies showed that the VE of C4 vaccines against HFMD caused by Coxsackievirus-A16 and other enteroviruses was low (<18%) [36,39]. Neutralization studies on C4 vaccines showed good cross-reactivity against EV71 sub-genotypes B4, B5, C2 and C5 [53,54]. Studies on B4 vaccines showed good immune response against EV71 sub-genotypes B5, C4 and C5 [9,20]. Secondly, real-world vaccine effectiveness had to be assessed. For example, post-marketing studies in the Chinese Mainland showed that VE against EV71 HFMD in children was >80% [55,56,57,58]. Thirdly, post-marketing surveillance of vaccine safety, particularly for extremely rare AEs, should be conducted. These events were often undetected in clinical trials due to limited sample size. The incidence of AEs reported in the Chinese Mainland was low, and most were mild or moderate [59,60,61,62]. Finally, the change in epidemiology after vaccine introduction should be reviewed. After vaccine introduction, the incidence of EV71 HFMD and its severe complications decreased significantly in many parts of the Chinese Mainland. However, this was accompanied by an increase in HFMD caused by other viruses, such as Coxsackievirus, and non-EV71 enteroviruses [63,64,65,66,67]. Serotype replacement and its potential consequences should be considered in risk–benefit assessments.
Before considering including EV71 vaccines in national childhood immunization programs, local epidemiology should be considered. Since sub-genotype C4 was the predominant strain in the Chinese Mainland, and the three vaccines approved in the Chinese Mainland were based on C4, the VE observed was mainly against C4 [37,46]. Secondly, cost-effectiveness studies need to be conducted. One study published in 2017 in the Chinese Mainland showed that routine pediatric EV71 vaccination would be cost-effective if the cost (including procurement, logistics and administration) was below USD14.6/dose [[68](#B68-vaccines-14-00235)]. Another study in 2017 demonstrated cost-effectiveness at USD9.2/dose [69]. A local economic evaluation would be necessary to assess whether inclusion as a national program is cost-effective. Thirdly, parents’ acceptance had to be assessed. Surveys can be conducted to explore the views and perceptions of parents or guardians. Lastly, practical issues, including availability of manpower, were important considerations for a successful immunization program. All currently approved vaccines are recommended to be stored at 2–8 °C. Some studies showed that coadministration of EV71 vaccine with other vaccines, including measles–mumps–rubella, influenza, hepatitis B, and meningococcal vaccines, was safe and did not interfere with immunogenicity [70,71,72]. Vaccine coadministration in the same visit would improve the uptake rate.
5. Conclusions
The results of the current meta-analysis support that EV71 vaccines are effective, immunogenic and safe. Areas with a high incidence of EV71 may consider introducing EV71 vaccines, taking into account the local epidemiology, economic analysis, parents’ acceptability and practical considerations of the immunization program. The latest development of EV71 vaccines should be closely monitored, including the multivalent vaccines (from bivalent to hexavalent) against HFMD, which cover different Coxsackievirus serotypes in addition to EV71 [73].
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization A Guide to Clinical Management and Public Health Response for Hand, Foot and Mouth Disease (HFMD)2011(accessed on 8 February 2026)Available online: https://iris.who.int/bitstream/handle/10665/207490/9789290615255_eng.pdf?sequence=1&is Allowed=y
- 2Centre for Health Protection Hand, Foot and Mouth Disease 2024 Available online: https://www.chp.gov.hk/en/healthtopics/content/24/23.html(accessed on 8 February 2026)
- 3Ma E. Chan K.C. Cheng P. Wong C. Chuang S.K. The enterovirus 71 epidemic in 2008—Public health implications for Hong Kong Int. J. Infect. Dis.201014 e 775e 78010.1016/j.ijid.2010.02.226520599410 · doi ↗ · pubmed ↗
- 4Chang L.Y. Lin H.Y. Gau S.S. Lu C.Y. Hsia S.H. Huang Y.C. Huang L.M. Lin T.Y. Enterovirus A 71 neurologic complications and long-term sequelae J. Biomed. Sci.2019265710.1186/s 12929-019-0552-731395054 PMC 6688366 · doi ↗ · pubmed ↗
- 5Liu F.C. Chen B.C. Huang Y.C. Huang S.H. Chung R.J. Yu P.C. Yu C.P. Epidemiological Survey of Enterovirus Infections in Taiwan From 2011 to 2020: Retrospective Study JMIR Public Health Surveill 202410 e 5944910.2196/5944939235279 PMC 11391656 · doi ↗ · pubmed ↗
- 6Pichichero M.E. Mc Linn S. Rotbart H.A. Menegus M.A. Cascino M. Reidenberg B.E. Clinical and economic impact of enterovirus illness in private pediatric practice Pediatrics 19981021126113410.1542/peds.102.5.11269794944 · doi ↗ · pubmed ↗
- 7Zheng Y. Jit M. Wu J.T. Yang J. Leung K. Liao Q. Yu H. Economic costs and health-related quality of life for hand, foot and mouth disease (HFMD) patients in China P Lo S ONE 201712 e 018426610.1371/journal.pone.018426628934232 PMC 5608208 · doi ↗ · pubmed ↗
- 8Chiu N.C. Lin C.Y. Chen C. Cheng H.Y. Hsieh E.F. Liu L.T. Chiu C.H. Huang L.M. Long-Term Immunogenicity Study of an Aluminum Phosphate-Adjuvanted Inactivated Enterovirus A 71 Vaccine in Children: An Extension to a Phase 2 Study Vaccines 20241298510.3390/vaccines 1209098539340018 PMC 11435984 · doi ↗ · pubmed ↗