The Use of Augmented Reality for Navigation in Minimally Invasive Abdominal and Thoracic Soft-Tissue Surgery: A Systematic Review
Inga Steinberga, Victor Gabriel El-Hajj, Laura Cercenelli, Mario Romero, Kenny A. Rodriguez-Wallberg, Erik Edström, Adrian Elmi-Terander

TL;DR
Augmented reality shows promise for guiding minimally invasive abdominal and thoracic surgeries, but more large-scale studies are needed to validate its effectiveness.
Contribution
This systematic review identifies the current state and limitations of AR in soft-tissue surgery, highlighting the need for standardized studies and integration with robotic systems.
Findings
AR improves anatomical guidance and procedural planning in complex surgeries.
Integration with robotic systems may enhance visualization and precision.
Research is limited in gynecologic surgery and lacks large-cohort validation.
Abstract
What are the main findings? Evidence supporting the use of augmented reality (AR) technology in minimally invasive abdominal and thoracic soft-tissue surgery is mostly limited to small-scale or preliminary studies and lacks comprehensive validation. In gynecologic surgery, current research is scarce and does not provide adequately validated outcomes.Guidance with AR systems requires deformable anatomical tracking and multimodal intraoperative data fusion to ensure safety and effectiveness. Evidence supporting the use of augmented reality (AR) technology in minimally invasive abdominal and thoracic soft-tissue surgery is mostly limited to small-scale or preliminary studies and lacks comprehensive validation. In gynecologic surgery, current research is scarce and does not provide adequately validated outcomes. Guidance with AR systems requires deformable anatomical tracking and…
Click any figure to enlarge with its caption.
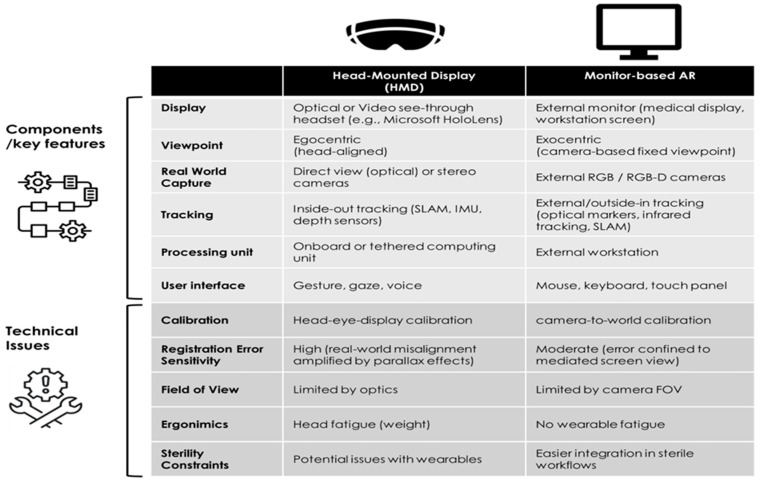 Figure 1
Figure 1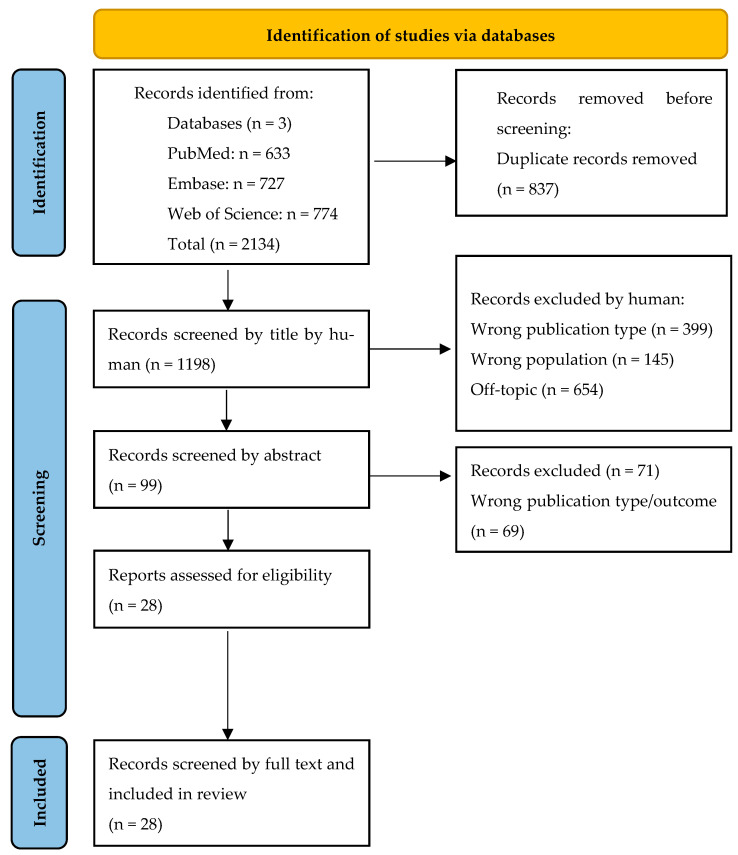 Figure 2
Figure 2- —Swedish Innovation Fund
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAugmented Reality Applications · Surgical Simulation and Training · Soft Robotics and Applications
1. Introduction
Surgical navigation has been used for decades in neurosurgery, spine surgery [1], and orthopedic procedures [2], relying on fixed anatomical references for patient coregistration. More recently, augmented reality (AR) has emerged, adding digital information from imaging modalities such as MRI, CT, and 3D US directly to the surgeon’s view [3]. Fusion, the process of combining information from different sources within AR systems, can be achieved through separate video displays, projection techniques, or, most commonly, head-mounted displays (HMDs) [4]. However, according to this systematic review, only a few studies reported the use of HMDs in AR [5,6]. HMDs improve intraoperative orientation by overlaying anatomical structures onto the patient, enhance spatial understanding, and reduce external distraction, but their weight (approximately 400–800 g) may cause neck strain, motion sickness, and visual fatigue during prolonged use.
In contrast, surgical navigation in abdominal and thoracic procedures has progressed slowly. The main challenge is maintaining accurate coregistration. Aligning preoperative 3D models with intraoperative anatomy is technically demanding and tracking real-time deformation of mobile soft tissues—such as the liver, kidneys, lungs, and uterus—is difficult due to continuous changes during surgery. Real-time algorithms are needed to compensate for tissue elasticity and manipulation. AR offers promising solutions to enhance navigation in abdominal and pelvic surgery by overlaying key structures (e.g., blood vessels or tumors) onto the patient, improving orientation and safety during complex, minimally invasive procedures [3]. Displaying vital structures in real time, AR helps prevent accidental injuries and improves both preoperative and intraoperative planning. AR also enhances surgical training by providing a clear, stable combined view of real anatomy [7,8]. For example, robotic platforms with stabilized endoscopic cameras offer reliable visualization, allowing accurate AR overlays [9,10].
The establishment of AR in minimally invasive abdominal and thoracic soft-tissue surgery depends on several key technological strategies. First, computational segmentation and 3D model creation generate virtual anatomical models for projection onto the surgical field, with the accuracy of these overlays depending on the quality of image acquisition and segmentation. Second, registration aligns preoperative 3D models with the patient’s intraoperative anatomy. Because soft tissues change shape and position during surgery, reliable registration requires strong algorithms and dependable landmarks. Real-time deformation tracking is critical, as organ deformation is the main challenge in soft-tissue surgery compared to bone-based navigation [11,12,13,14]. Third, real-time motion compensation and continuous tracking keep AR overlays aligned, even when the endoscope moves. Manual manipulation and repositioning of the endoscope create challenges for computer-assisted systems, making it difficult to maintain dynamic, real-time adaptation of AR overlays [9,10]. Finally, AR systems must also synchronize with physiological movements, such as breathing and heartbeat, to reduce motion-induced errors.
Figure 1 describes differences between VR Head-Mounted Display (HMD) System and Non-HMD (Monitor-Based) VR.
This systematic review aims to capture the current state of the art in the use of augmented reality (AR) for navigation in minimally invasive abdominal and thoracic soft-tissue surgery. It explores and summarizes literature from 2014 to 2024, focusing on highly mobile anatomical structures that may change shape during procedures. Following PRISMA guidelines, we detail the methodology and present key findings from the included studies, covering general setup, devices employed, accuracy levels, usability outcomes, and challenges. The review concludes with the main findings and future perspectives.
Our specific goals are to investigate the following research questions:
- -In which organs and procedures of minimally invasive abdominal and thoracic soft-tissue surgery has AR been used?
- -How is AR applied to highly mobile anatomical structures whose shape changes during surgical procedures?
- -What devices are used in recent research on this topic?
- -What accuracy levels and usability outcomes have been reported for the augmentation?
- -What challenges and unresolved problems still need to be addressed to advance the development and effective use of AR?
2. Materials and Methods
This systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [15]. The PRISMA 2020 checklist and further methodological details are available in the Supporting Information [Files S1–S4].
The review protocol is registered in the International Prospective Register of Systematic Reviews (PROSPERO) [16] (Registration ID: CRD42024597021; registration date: 24 October 2024).
2.1. Eligibility Criteria
All original studies published between 2014 and 2024, written in English, and focusing on AR applications in minimally invasive abdominal and thoracic soft-tissue surgery on humans were eligible for inclusion in this systematic review (Table 1).
2.2. Types of Studies
The systematic review encompasses published, peer-reviewed original human studies, including randomized trials, observational studies, and case series with a sample size of 4 or more.
Non-original publications, including reviews, editorials, letters to the editor, conference abstracts, unpublished studies, and prior systematic reviews, were excluded. Additionally, studies on augmented reality navigation in orthopedic, neurosurgical, vascular, and plastic surgery were omitted.
Single case reports and studies with fewer than 4 participants were excluded due to their limited sample sizes, which reduces the level of evidence.
2.3. Type of Population
Studies that recruited adults aged 18–64 years were included and were considered representative of adult age.
Studies that recruited adolescents aged ≤17 years or adults aged ≥65 years were excluded as falling outside the adult age range.
2.4. Type of Intervention
Only articles focusing on the use of AR applications on humans within minimally invasive abdominal and thoracic soft-tissue surgery were considered for inclusion in this review. Studies addressing the use of other technologies of extended reality (XR) such as mixed reality (MR) and virtual reality (VR) were excluded.
2.5. Type of Comparators
There were no restrictions with respect to the type of comparator.
Data are categorized according to the following:
- -Comparison is made between groups with and without AR,
- -Technology is classified according to types of devices and the use of head-mounted displays (HMDs),
- -The use of additional technologies in conjunction with AR is documented.
This categorization will form the basis for descriptive narrative synthesis.
2.6. Type of Outcome Measures
Data is pooled as total counts and frequencies to assess the state of the literature on the use of AR in abdominal and thoracic soft-tissue surgery.
The certainty of evidence is evaluated by examining the individual risk of bias in each study and the strength of the combined body of evidence.
No subgroup investigation is planned.
2.7. Databases and Search Strategy
Three electronic bibliographic databases relevant to the medical field—PubMed, Web of Science, and Embase—were utilized. The literature search was confined to the period 2014 to 2024 and was restricted to articles published in English. The database search was completed on 28 October 2024.
2.8. Study Selection
The search identified 2134 papers across databases. After removing duplicates, 1297 papers remained. These records were uploaded to Rayyan [17]. Two independent, non-blinded reviewers (I.S. and V.G.E.-H.) screened 1297 records by title and then by abstract. Disagreements concerning two articles were resolved through discussion and consultation with a third reviewer (K.A.R-W.). Subsequently, data extraction from the full texts of the 28 remaining articles was conducted by two independent, non-blinded reviewers (I.S. and L.C.). Ultimately, 28 studies were deemed eligible for inclusion in this review, as illustrated in the PRISMA flow chart in Figure 2.
2.9. Data Extraction
Data from selected records were extracted using a predefined template. This template included general information such as:
- -Study title, study purpose, first author, and record publication year, surgical specialty, and organ treated.
- -Population characteristics, such as the number of patients and surgeries.
- -Intervention characteristics, such as the type of minimally invasive surgical approach (laparoscopy or robot-assisted laparoscopy).
- -Technology characteristics such as the type of AR navigation system used, the imaging guidance used (MRI, ultrasound, CT), and the use of a head-mounted display (HMD).
- -Outcome characteristics, such as outcome accuracy and assessment of the control group.
- -Other outcomes were usability, surgical outcome, operative time, complications, reoperation, and any specific complications related to AR system use.
- -A conclusion, summary, and an assessment of study limitations.
2.10. Data Synthesis and Risk of Bias Assessment
Due to heterogeneity and significant methodological differences across studies, particularly in study designs, procedures, and technologies, a descriptive narrative synthesis is employed to better understand the use of augmented reality navigation in minimally invasive abdominal and thoracic soft-tissue surgery. Statistical testing of heterogeneity is unnecessary given the evident methodological differences across studies. Meta-analysis is not applicable due to the insufficient number of homogeneous studies with comparable procedures.
2.11. Related Works
An updated PROSPERO search (January 2026) confirmed our project is the only ongoing one in this area. No PubMed systematic reviews between 2014 and 2026 address AR for navigation in minimally invasive abdominal and thoracic soft-tissue surgery. To further assess the literature, a PubMed search on 23 February 2026, using our predefined inclusion criteria, showed publications on augmented reality remain concentrated in liver [18,19] and thoracic surgery [20,21].
3. Results
Out of 1297 studies screened, only 28 (2%) met the inclusion criteria and were ultimately included in this systematic review (Figure 2).
Studies focusing on minimally invasive abdominal and thoracic soft-tissue surgery span different domains, with 28% (n = 8) conducted using robot-assisted laparoscopic techniques and 71% (n = 20) performed using conventional laparoscopy. An overview of the 28 included studies is shown in Table 2.
3.1. AR Use in 28 Studies of Minimally Invasive Abdominal and Thoracic Soft-Tissue Procedures
The AR was used on the following organs and procedures within minimally invasive abdominal and thoracic soft-tissue surgery is shown in Table 3.
3.2. The Use of AR on Highly Mobile Anatomical Structures
Among the 28 included studies, AR was applied to deformable and mobile anatomy using five major strategies, shown in Table 4.
3.3. Devices Used in the 28 Included Studies
While 26 studies (92%) reported using static monitors as AR displays, 2 studies (7%) reported employing head-mounted displays (HMDs) as holographic AR displays in lung and liver surgery.
Expanding on the use of AR technologies, indocyanine green (ICG) fluorescence imaging combined with AR navigation was employed in four studies (14%), primarily in liver surgery. In these studies, real-time ICG fluorescence visualization was integrated with AR overlays to improve tumor boundary identification, vascular mapping, and resection accuracy. Hardware, software, AR navigation, and analysis/tracking systems are shown in Table 5.
3.4. Accuracy Levels and Usability Outcomes of the AR
Workflow efficiency regarding intraoperative setup and registration times was described qualitatively, without mean ± SD or statistical analysis [5,24,27,32,33,34,35,36,41,42,43].
Data showed that the combination of 3D printing and augmented reality reduces operative time (OT) [5], whereas intraoperative navigation and AccuVein show no meaningful impact on procedure duration [34,41].
Cognitive load, measured through surgeon feedback on usability and orientation, was collected via questionnaires and Likert scales but reported narratively, without nu-merical distributions or structured data. There was no formal evaluation of overall usabil-ity, cognitive load, or safety, nor were there structured surgeon satisfaction scores, stand-ardized workload measures, or objective assessments of mental or cognitive effort [24,25].
Surgeon-reported outcomes were not formally measured; impressions were presented only narratively without validated questionnaires [36]. Moreover, there was no formal assessment of anatomical understanding, training quality, or educational utility [37]. There was only indirect addressing of training quality and educational utility from a technolog-ical perspective, without validated anatomical comprehension assessments [48].
In terms of accuracy, the use of 3D models was associated with improved surgical margins [32,33].
A summary of reported accuracy levels and usability outcomes of AR systems is shown in Table 6.
3.5. Challenges in the Development and Effective Use of AR
Several methodological limitations were identified in the included studies regarding the use of AR systems for minimally invasive abdominal and thoracic soft-tissue surgery. Specifically, common issues included retrospective study designs, single-center settings, and non-randomized methodologies [5,6,7,26,38,41,42,43,44]. In addition, small sample sizes and the absence of control groups were noted in many studies [6,26,27,31]. Furthermore, surgery was often performed by a single surgeon or team [23,32,34,35,36,37,38,41,43]. Variable imaging and operative protocols, along with short follow-up durations, were also reported, limiting the assessment of long-term outcomes [40].
Technical limitations, including inadequate deformation tracking, rigid 3D models [37], experimental settings [22,29,33], and the need for manual adjustments [33,39] or additional personnel, may reduce workflow efficiency. Accuracy levels and usability outcomes are presented in Table 7.
4. Discussion
Substantial heterogeneity in the AR devices employed worldwide in minimally invasive abdominal and thoracic soft-tissue surgery between 2014 and 2024 was found. No publications meeting the inclusion criteria were identified within the field of gynecological surgery. However, a few small case series (n = 3) were published in 2017 using AR in gynecological surgery [7] and demonstrating AR-guided localization of small- and medium-sized intramural myomas during conventional laparoscopy. The software ran in real time on a standard Intel i7 PC and required no artificial landmarks. The preoperative uterus model was matched to the 3D model obtained during surgery using a semiautomatic registration process. This method required a small amount of manual input, in which the edges of the uterus were marked to help the system define the organ’s boundaries. The matched models were overlaid on each video frame, making the uterus appear partly transparent. This allowed the surgeon to clearly see the exact position of the myoma inside the uterus. This new AR system was able to track a highly mobile organ such as the uterus, something that had not been previously described.
Building on early gynecological AR research, later work introduced a robot-assisted AR system for identifying sentinel nodes during laparoscopic surgery. This 2022 study, using an animal model, used real-time multimodal fusion of laparoscopic images with preoperative imaging during pelvic lymphadenectomy. Notably, CT overlay accuracy was greater than 90%, and overlap rates were less than 6%. AR significantly improved the identification of target structures for both experienced surgeons and trainees [14].
However, published data within gynecological surgery remain preliminary and experimental, with small study cohorts limiting the level of evidence.
In addition to studies in gynecology, research using AR systems for minimally invasive soft-tissue surgery within the pelvic region has been conducted in urology [32,33,39]. For example, AR enhances the accuracy of targeted prostate biopsies by providing a 3D virtual reconstruction [33]. In robot-assisted radical prostatectomy (RARP), 3D model overlays, manually aligned with the endoscopic view, helped tailor nerve-sparing surgery and reduce positive surgical margins. This was especially useful for patients with extracapsular tumor extension [32,39]. The AR model correctly identified 70% of cancerous areas (sensitivity) and all healthy areas (100% specificity). Overall, it matched the actual cancer distribution 92% of the time (accuracy) [39]. These findings suggest AR systems are highly accurate and minimize false positives. This supports their use as a reliable surgical guidance tool.
Beyond pelvic surgery, nearly half of the studies in our review (n = 12, 42%) focused on AR in minimally invasive liver surgery. The anterior approach is often used to expose the inferior vena cava (IVC) and enable safer transection of the short hepatic veins. This includes en bloc caudate lobe resection. AR systems project the left-right liver demarcation line and the course of the middle hepatic vein (MHV) from the 3D model onto the liver surface, guiding the parenchymal transection plane. Despite inaccuracies caused by respiratory motion and tissue deformation, combining AR with intraoperative ultrasound (IOUS) enables effective guidance [6]. AR has also been linked to a lower incidence of bile leakage, likely due to improved protection of vascular structures and bile ducts [6,40].
As mentioned earlier, the implementation of AR in minimally invasive abdominal and thoracic soft-tissue surgery relies on several key technologies. Computational segmentation and 3D model creation, using methods such as SmartLiver surface-based registration, CNN-based segmentation, and 3D deformation modeling, allow precise identification of anatomical structures and support detailed 3D surgical planning [22,23,24]. Registration and tracking, employing AI-based segmentation and algorithms like weighted point-based registration and 3D positional measurements (e.g., CNN/iKidney, 2D U-net), align preoperative models with the patient’s anatomy. That provides accurate intraoperative guidance and improves safety [23]. Real-time motion compensation and continuous tracking update AR overlays during organ or camera movement. This helps maintain accurate anatomical guidance throughout the procedure [25,26]. Finally, real-time deformation tracking monitors tissue shifts using IOUS, intraoperative CT, fluorescence/ICG imaging, and endoscopic vision tracking. This ensures that anatomical models remain up to date, thereby improving surgical precision and safety [26,27,28,29,30,31].
When comparing AR platforms, this review found that the software and hardware used in AR-assisted surgery vary in several capabilities, including image processing, visualization, and the intended purpose of the AR system. Through segmentation, surgical planning, and intraoperative navigation, clinically validated software platforms such as Mimics and iPilot improve the accuracy and safety of surgery [5,28,30]. Moreover, MI-3DVS and simple DICOM viewers support quick anatomical review, saving time in the operating room [6,43]. Tools like vMIX enable real-time integration of AR [39]. Hardware platforms such as Fluid™ and AccuVein portable devices provide real-time feedback and improve visualization, with AccuVein specifically focusing on vascular visualization. Precision tracking systems such as Volga-M, Polaris Spectra, NDI Polaris Vicra, and Optotrak ensure real-time, accurate tracking of anatomy, supporting safe navigation. 3D printing platforms like OBJET500 allow creation of patient-specific models for preoperative planning [5,6,29,37,45]. Intraoperative imaging systems DynaCT and PINPOINT/DPM-III-01 provide high-resolution updates and real-time perfusion assessment, which are important for surgeons to adapt to changes during surgery. Together, these tools improve anatomical mapping and guide interventions, thus reducing risks in complex surgical procedures.
Despite the advances described above, each AR platform also has limitations. AR-assisted navigation systems (AR-ANS) developed by individual research teams may be difficult to generalize and often lack regulatory approval. Generating accurate 3D models requires close collaboration between radiologists, surgeons, and engineers. Currently, superimposition of 3D virtual models (3DVMs) onto the operative field is often performed manually. This process typically requires assistance. Clinical platforms can be costly, less flexible, and tied to specific hardware. DICOM-based systems used in urological surgery can be complex without proper software support [23]. Intraoperative reliability and precision could be improved through fully automatic model superimposition [24,32].
Taken together, the evidence presented shows that integrating deformable anatomical tracking with multimodal intraoperative data fusion has significant practical implications for safe and effective AR in surgery. These systems maintain accurate alignment, even in the presence of organ motion, deformation, or surgical manipulation, and provide reliable visual guidance. Real-time updates from video, fluorescence, ultrasound, or CT keep critical structures visible as anatomy changes. This reduces the risk of injury and improves precision. AI-enhanced platforms—such as Therapixel™, Visible Patient™, IGNITE, iKidney, and SmartLiver—create accurate 3D models from multimodal data. They support manual, semi-automatic, or fully automatic registration using internal landmarks, vessel positions, and surface points [23,24]. These features enhance the consistency, usability, and reliability of AR systems. When combined with robotic surgery, which stabilizes the endoscopic camera, AR overlays remain consistent, further improving surgical planning, precision, and safety.
4.1. Training and Education
This review provides only a narrative description of educational utility, without any validated objective performance metrics that would allow for a quantifiable assessment of trainee skills (e.g., precision, task completion, errors) or support consistent monitoring of learning progression. The study by Iop et al. [48] demonstrates that XR simulation can complement traditional training by providing evidence-based, data-driven feedback that facilitates skill acquisition in a safe, controlled environment, without risk to patients. The educational benefit lies in the use of objective performance metrics rather than in the formal assessment of cognitive or theoretical learning outcomes.
4.2. Cost–Benefit Analysis
None of the included studies presented cost–benefit calculations. The 2025 paper [49] presents a study protocol detailing planned cost–benefit and cost-effectiveness analyses comparing AR surgical navigation, conventional navigation, and the free-hand technique using QALYs and ICER metrics. As this is a protocol publication and not a report of trial results, the actual cost–benefit outcomes are still pending and will be available only after data collection and analysis are complete. According to the protocol, cost data will be collected at discharge and at 30, 90, and 365 days. These include inpatient and outpatient care costs, medications, sick leave, lost productivity, and total patient costs. Quality-adjusted life years (QALYs) will be calculated with the EQ-5D-3L instrument and, together with cost data, used to estimate the incremental cost-effectiveness ratio (ICER) between surgical techniques.
5. Limitations
Included studies on AR systems for minimally invasive abdominal and thoracic soft-tissue surgery showed methodological weaknesses. Most were retrospective, single-center, non-randomized, with small samples and limited follow-up, reducing statistical power and generalizability. Many lacked control groups. Procedures were often performed by a single surgeon or team, potentially introducing performance bias. Technical inconsistencies harmed accuracy, especially with variable imaging and rigid 3D models. Most platforms were experimental, needed frequent manual recalibration, and relied on extra staff and specialized hybrid theatres. High development and equipment costs further limited AR use in major academic centers.
6. Conclusions
Advancing AR requires larger, rigorously designed clinical studies that use standardized protocols, focus on relevant clinical outcomes, and include multicenter collaboration to strengthen the evidence base and support reliable adoption in gynecological surgery.
Evidence from urological procedures also demonstrates that AR enhances visualization and precision in minimally invasive pelvic surgery. Reports of high specificity and overall accuracy suggest that AR can serve as a reliable adjunct for intraoperative guidance, though broader validation is still needed to confirm its clinical impact.
In thoracic surgery, the combination of AR, 3D printing, and multimodal imaging has been shown to enhance anatomical visualization and support intraoperative localization of challenging lung nodules, suggesting the potential to improve surgical outcomes.
In minimally invasive liver surgery, AR is utilized to define anatomical resection planes and protect critical vascular structures. Despite persistent technical challenges, particularly those arising from organ motion and deformation, integrating AR with intraoperative ultrasound appears to improve procedural accuracy.
In summary, integrating deformable anatomical tracking with multimodal intraoperative data and 3D modeling enhances the clinical potential of AR in precision surgery. However, technical variability, frequent recalibration requirements, high costs, and dependence on specialized personnel limit its use. That keeps most AR systems experimental and confined to major centers. Future AR platforms should be affordable and compatible with standard operating rooms to ensure access for everybody to all healthcare systems.
7. Future Perspective
Future studies should prioritize prospective, multicenter randomized trials with sufficient sample sizes and extended follow-up. When possible, incorporate suitable control groups and blinded outcome assessments. Procedures should involve multiple surgeons with standardized training and be evaluated using objective, uniform metrics to enable comparison and minimize performance bias [48]. To date, evidence in gynecologic and urological surgery remains limited; however, emerging studies indicate these fields are beginning to evaluate and implement such techniques. These represent key areas for future investigation within minimally invasive soft-tissue pelvic surgery.
Technical robustness can be improved through developing deformable, real-time models and standardized imaging and registration protocols. Automated tracking methods may reduce dependence on manual recalibration. Ongoing research should aim to design AR platforms that operate reliably in standard operating rooms without specialized hybrid theatres or extra personnel. Cost-effective, interoperable hardware and software will support broader clinical use. Finally, transparent reporting of AR system performance and limitations is crucial to enable integration into routine surgical practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Frisk H. Jensdottir M. Coronado L. Conrad M. Hager S. Arvidsson L. Bartek J. Burström G. El-Hajj V.G. Edström E. Automatic image registration provides superior accuracy compared with surface matching in cranial navigation Sensors 202424734110.3390/s 2422734139599122 PMC 11597983 · doi ↗ · pubmed ↗
- 2Kurosaka K. Ogawa H. Hirasawa N. Saito M. Nakayama T. Tsukada S. Does augmented reality-based portable navigation improve the accuracy of cup placement in THA compared with accelerometer-based portable navigation? A randomized controlled trial Clin. Orthop. Relat. Res.20234811515152310.1097/CORR.000000000000260236862072 PMC 10344563 · doi ↗ · pubmed ↗
- 3Barcali E. Iadanza E. Manetti L. Francia P. Nardi C. Bocchi L. Augmented reality in surgery: A scoping review Appl. Sci.202212689010.3390/app 12146890 · doi ↗
- 4Lai M. Skyrman S. Shan C. Babic D. Homan R. Edström E. Persson O. Burström G. Elmi-Terander A. Hendriks B.H.W. Fusion of augmented reality imaging with the endoscopic view for endonasal skull base surgery; a novel application for surgical navigation based on intraoperative cone beam computed tomography and optical tracking P Lo S ONE 202015 e 022731210.1371/journal.pone.022731231945082 PMC 6964902 · doi ↗ · pubmed ↗
- 5Li C. Zheng B. Yu Q. Yang B. Liang C. Liu Y. Augmented reality and 3-dimensional printing technologies for guiding complex thoracoscopic surgery Ann. Thorac. Surg.20211121624163110.1016/j.athoracsur.2020.10.03733275930 · doi ↗ · pubmed ↗
- 6Yasuda J. Okamoto T. Onda S. Fujioka S. Yanaga K. Suzuki N. Hattori A. Application of image-guided navigation system for laparoscopic hepatobiliary surgery Asian J. Endosc. Surg.202013394510.1111/ases.1269630945434 · doi ↗ · pubmed ↗
- 7Bourdel N. Collins T. Pizarro D. Debize C. Grémeau A.S. Bartoli A. Canis M. Use of augmented reality in laparoscopic gynecology to visualize myomas Fertil. Steril.201710773773910.1016/j.fertnstert.2016.12.01628089570 · doi ↗ · pubmed ↗
- 8Lecointre L. Verde J. Goffin L. Venkatasamy A. Seeliger B. Lodi M. Swanström L.L. Akladios C. Gallix B. Robotically assisted augmented reality system for identification of targeted lymph nodes in laparoscopic gynecological surgery: A first step toward the identification of sentinel node: Augmented reality in gynecological surgery Surg. Endosc.2022369224923310.1007/s 00464-022-09409-135831676 · doi ↗ · pubmed ↗