Gastric Polyposis Due to Foreign Bodies and H. pylori Infection: Case Report and Literature Review
Cătălina Dănilă, Lucian Mocan, Ovidiu Laurean Pop, Andrea Pop-Crisan, Lucian Faur, Simona Daniela Cavalu

TL;DR
A 23-year-old man with a history of ingesting foreign objects developed gastric polyposis, which improved after removing the objects and treating H. pylori infection.
Contribution
This case report highlights the rare association between gastric polyposis, chronic irritation from foreign bodies, and H. pylori infection.
Findings
Endoscopic removal of foreign bodies and H. pylori eradication led to mucosal improvement and remission of hypereosinophilia and splenomegaly.
Histological analysis revealed dysplasia and inflammatory changes in gastric polyps.
The patient showed complete remission of gastric polyposis after 3 years and 8 months of treatment.
Abstract
Background and Clinical Significance: Foreign body ingestion represents an endoscopic emergency, with a risk of organ perforation of up to 35%, where increased prevalence was noticed among people with mental disorders and institutionalized patients. Case Presentation: The patient—male, 23 years old, and institutionalized for sequelae of infantile encephalopathy—was admitted for epigastric pain and hyperemetic syndrome that began 10 days earlier. Endoscopically, 12 hard plastic foreign bodies with sharp edges and sizes of 6–7 cm were identified, followed by extraction that was successfully performed in two sessions using a polypectomy snare and a Foreign Body Hood Protector. Additionally, multiple sessile exulcerated polypoid lesions were observed, measuring around 1–3 cm each, occupying the entire antrum. Histological examination showed inflammatory/regenerative elements, with features…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
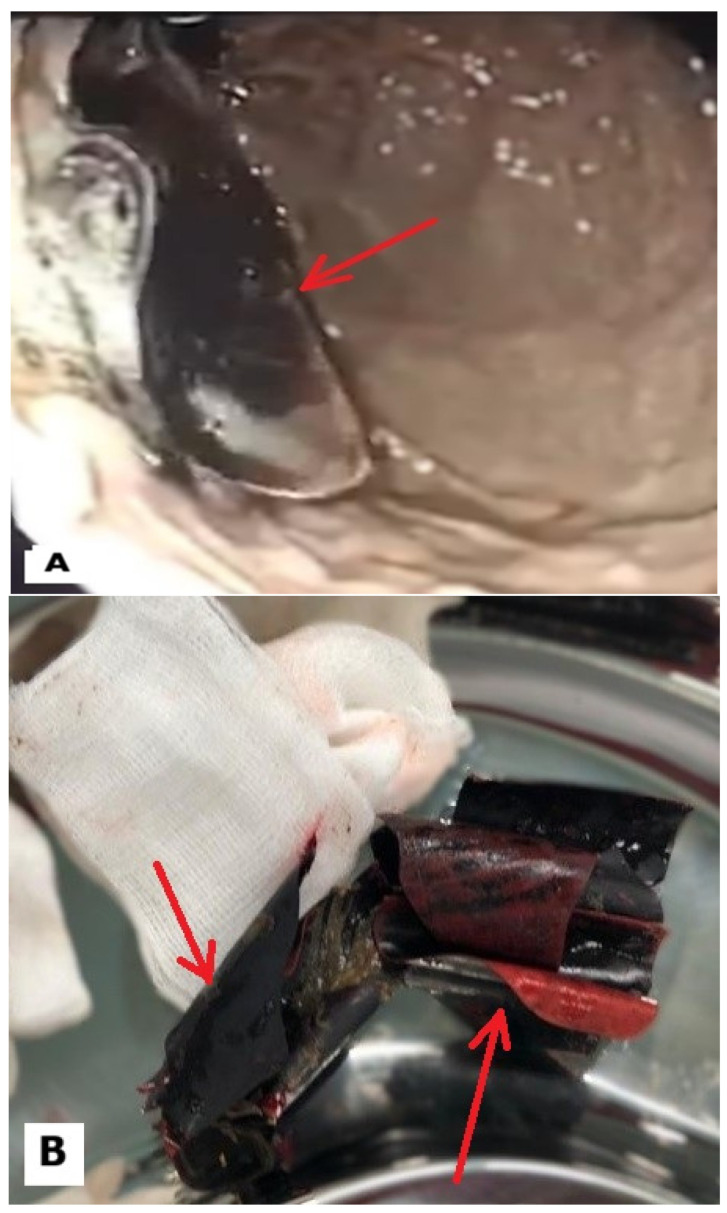 Figure 1
Figure 1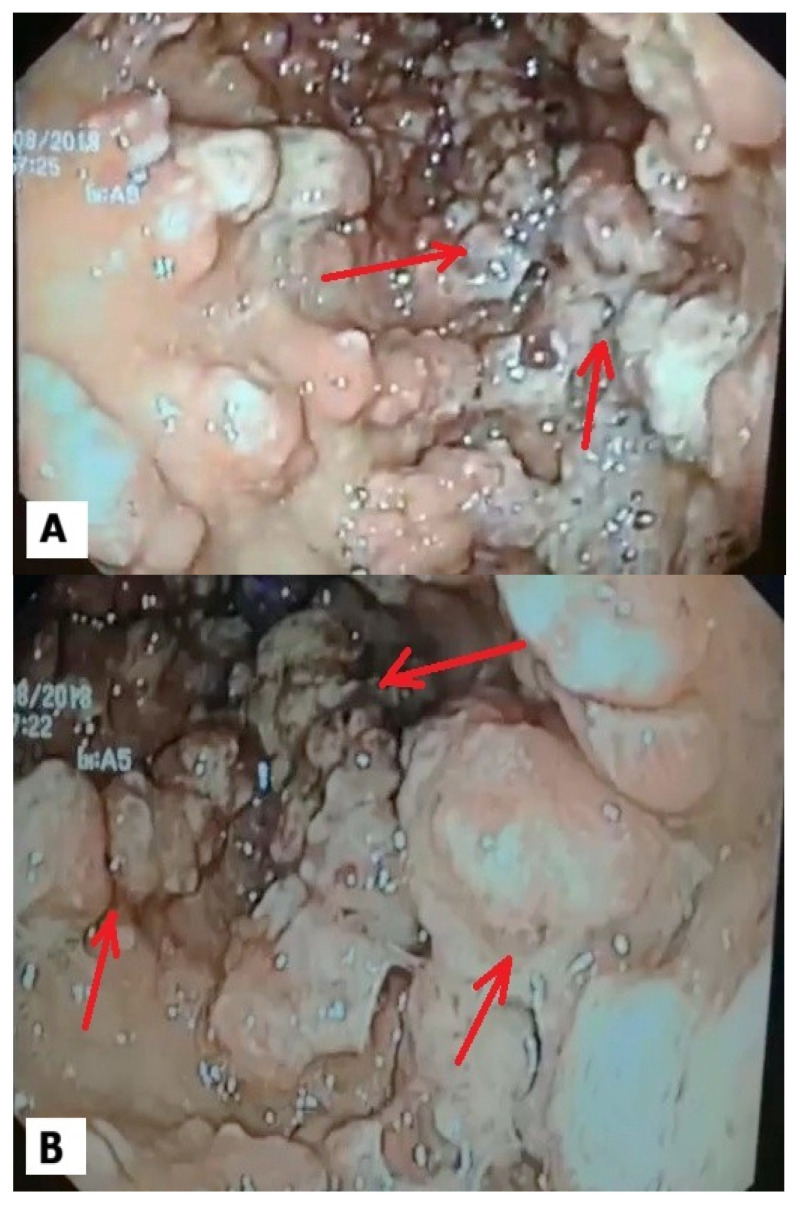 Figure 2
Figure 2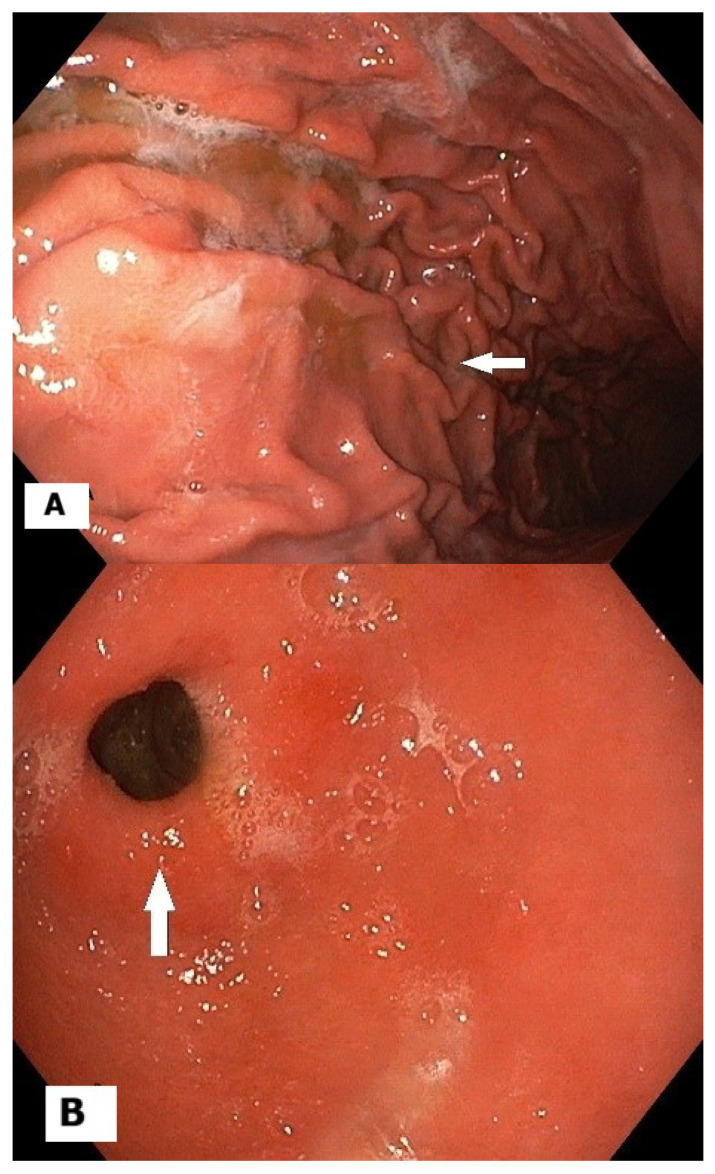 Figure 3
Figure 3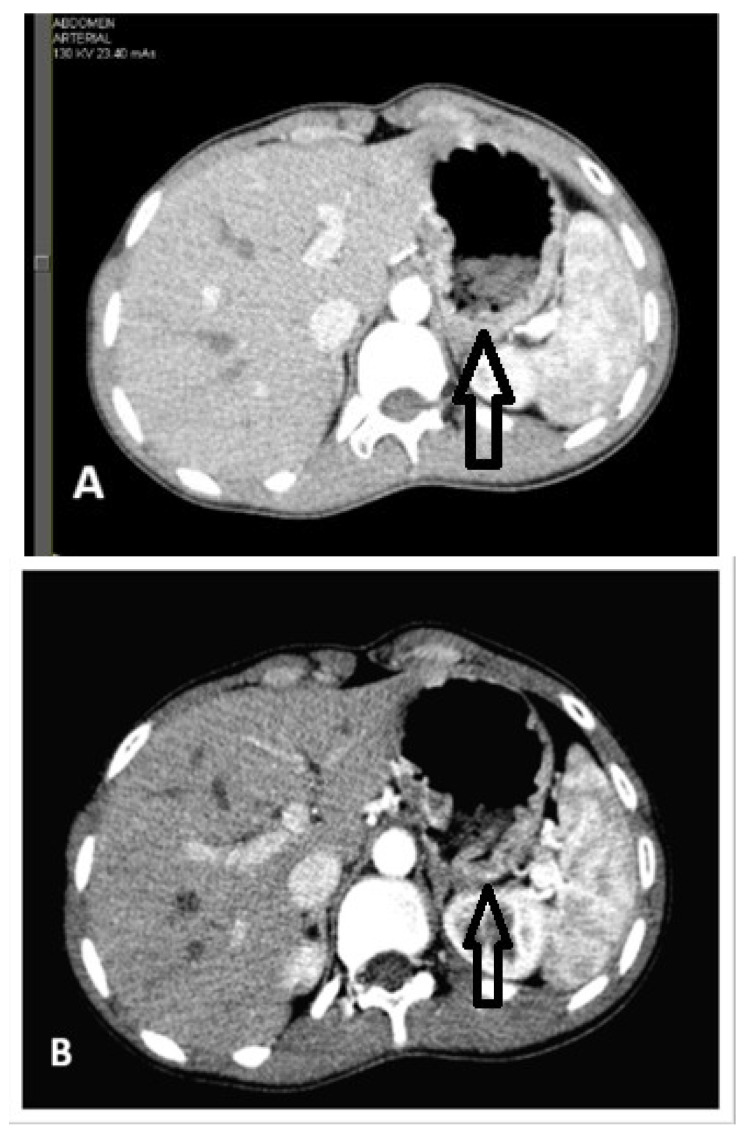 Figure 4
Figure 4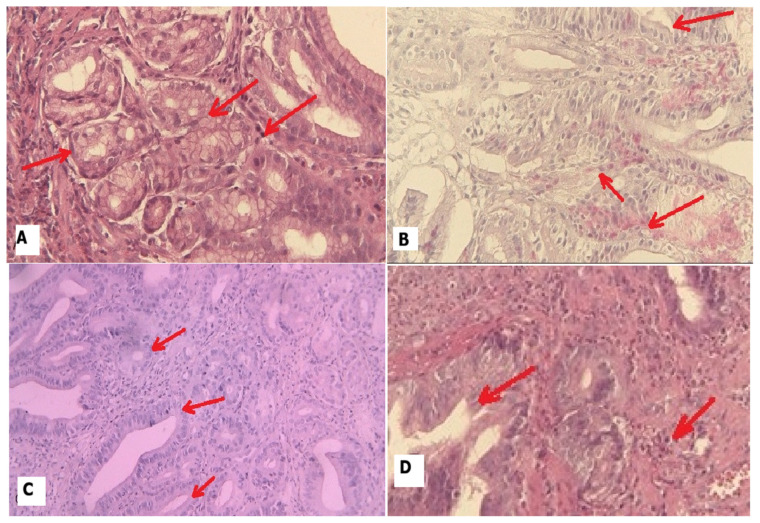 Figure 5
Figure 5- —University of Oradea, Romania
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsForeign Body Medical Cases · Esophageal and GI Pathology · Biliary and Gastrointestinal Fistulas
1. Introduction and Clinical Significance
Gastric polyps are a diverse group of lesions arising from the gastric mucosa or submucosa, encompassing hyperplastic, inflammatory, fundic gland, adenomatous, and serosal/foreign-body-associated variants [1]. Foreign bodies introduced into the stomach—whether iatrogenic, accidental, or intentional—can produce a spectrum of endoscopic appearances. Chronic irritation from a retained object may lead to reactive granulation tissue, inflammatory polyps, or focal mucosal hyperplasia. In some cases, the foreign material may be encapsulated or partially embedded within a polyp, necessitating careful histopathologic evaluation to differentiate benign reactive changes from dysplasia or neoplasia. The clinical significance lies not only in an accurate diagnosis but also in determining whether removal of the foreign body is indicated and how mucosal healing impacts polyp dynamics [2].
Clinically, patients may present with nonspecific epigastric discomfort, early satiety, anemia, or incidental findings on imaging or endoscopy performed for unrelated reasons. Endoscopic assessment is essential for characterizing the lesions, assessing the relationship to the foreign body, and determining the feasibility of endoscopic retrieval or need for surgical intervention. An endoscopic biopsy can help distinguish reactive polyps from neoplastic processes. The disadvantage consists in the likelyhood of limited access to biopsy with precision, especially if the lesion is fibrous or adherent to the foreign material. In select cases, imaging and endoscopic ultrasound may aid in assessing the depth of involvement and surrounding tissue reaction [3].
In the context of a gastric foreign body, the management focuses on two parallel goals: (1) safe and definitive removal or stabilization of the foreign object to prevent ongoing injury, migration, or perforation, and (2) appropriate treatment of the resulting mucosal lesion. If the foreign body is removable endoscopically and the polyp is purely reactive without dysplasia, removal plus a targeted biopsy may suffice, followed by surveillance to document mucosal recovery. If the polyp demonstrates dysplasia or neoplastic features, or if the foreign body cannot be safely retrieved endoscopically, multidisciplinary discussion regarding surgical options is warranted. Histopathology remains crucial to distinguish inflammatory or reparative polyps from neoplastic processes and to assess for complications such as ulceration or metaplasia [4].
Hypereosinophilia, defined as an elevated peripheral eosinophil count that is persistently above the expected reference range, reflects a spectrum of disorders ranging from allergic and parasitic processes to primary hematologic diseases and eosinophilic GI involvement. While eosinophilia is commonly discussed in the context of asthma, dermatologic conditions, or hypereosinophilic syndromes, its intersection with gastric foreign bodies is a less familiar but clinically meaningful topic [5]. This case-based discussion explores the potential link between gastric foreign bodies and eosinophilic gastric mucosal responses, highlighting diagnostic considerations, pathophysiologic mechanisms, and therapeutic implications.
Gastric foreign bodies can provoke a localized inflammatory environment characterized by mucosal injury, chronic irritation, and regenerative changes. In susceptible individuals, this environment may recruit eosinophils to the gastric mucosa, contributing to endoscopic findings such as edema, friability, and polypoid changes, as well as histologic features including eosinophilic infiltration of the lamina propria and muscularis mucosae [6]. Eosinophil-dominated responses in the stomach may be driven by several pathways: direct tissue injury from the foreign body, mechanical stimulation, microbiome-epithelial interactions, and systemic or regional allergic or hypereosinophilic processes. Distinguishing a reactive, localized eosinophilic response from systemic eosinophilic gastroenteritis or other eosinophil-driven diseases is essential, as it guides both the management of the foreign body and any targeted anti-eosinophilic therapies [7].
The present case highlights educational themes applicable to gastroenterology practice: recognizing atypical etiologies of gastric polyps, integrating endoscopic and histopathologic data in the setting of a foreign body, and balancing the risks and benefits of foreign-body removal with lesion-directed therapy. It also illustrates decision-making frameworks for selecting surveillance intervals, determining indications for retrieval, and anticipating mucosal recovery after foreign-body removal.
The patient’s history of foreign-body ingestion, endoscopic findings, histopathologic results, imaging studies, and the therapeutic approach chosen provided the outline for the present case. We discuss the rationale for foreign-body management in conjunction with polyp treatment and review relevant guidelines on endoscopic removal and surveillance of reactive gastric lesions, reflecting on implications for prognosis and follow-up. Additionally, through a literature review, we aim to illuminate the pathophysiology of foreign-body-associated gastric polyps and provide a practical framework for evaluation and management of similar scenarios in clinical practice.
2. Case Presentation
2.1. General Data
This is the case of a male, 23 years old, who was admitted three times in our service (initial evaluation and two follow-ups), being diagnosed with infantile encephalopathy and intellectual disability, and also presenting trouble concerning his communication skills.
2.2. Clinical Data
Upon the first admission, the patient presented nausea and abdominal pain with 10 days prior onset. He was normal weight and had a slim abdomen, which presented tenderness upon palpation in the epigastric region. Mainly because of the communication limitations, multiple laboratory tests, imaging tests and endoscopies were performed on each admission.
2.3. Endoscopy Results
A total of three upper digestive tract endoscopies were performed (one during the initial admission and the others during the follow-ups). The endoscopy team was surprised to discover around 12 foreign plastic objects that were around 7–8 cm in length; most were blunt, but some had sharp edges, as depicted in Figure 1A,B. There was no data regarding when they were swallowed or whether they were swallowed at the same time.
The whole gastric body and antrum was covered with polypoid sessile lesions with an adenomatous appearance, measuring 1–3 cm, as illustrated in Figure 2A,B. Their texture was firm when biopsies were performed. Because of the risk of organ perforation, the sharp objects were immediately extracted. The blunt objects that did not present a risk of organ perforation or occlusion were extracted during the follow-up endoscopy. A rapid urease test was performed and showed the presence of an H. pylori infection, and hence, a regular regimen of eradication therapy was initiated and consisted of PPI, amoxicillin and levofloxacin [8].
The third and last follow-up endoscopy revealed chronic gastritis without any polyps, as seen in Figure 3, while the rapid urease test was negative.
2.4. CT Scan
Given the presence of multiple large-sized gastric polyps, a CT scan was performed, showing irregular thickening of the gastric walls with moderate contrast uptake and mild splenomegaly and without perigastric adenopathies (Figure 4).
2.5. Histopathology Results
During the first and second endoscopies, multiple biopsies were collected from the polyps and sent for histopathological examination. Hematoxylin–eosin staining was performed, showing both inflammatory and mild dysplasia lesions, as illustrated in Figure 5A–C. During the last follow-up endoscopy, a final set of biopsies were collected and the histopathologist concluded that only inflammatory lesions were present, as illustrated in Figure 5D. Giemsa staining was also performed and showed that H. pylori was no longer present [9].
2.6. Laboratory Results and Other Investigations
Baseline laboratory investigations indicated marked eosinophilia, where this abnormality was sustained and reached its zenith during the second assessment. The hematological findings were assessed in conjunction with the observed mild splenomegaly, and consequently, a hematologist performed a bone marrow biopsy, which was negative for malignancy.
Table 1 presents the evolution of the eosinophile count from the moment of diagnosis to the last follow-up. The spike point was recorded on September 2018, marking the final endoscopic extraction of the foreign bodies. The endoscopies were performed on April 2018, September 2018 and January 2022, each one on the same day as the admission. Subsequently, the eosinophile count began to decrease, reaching normal values by January 2025.
3. Discussion
This case describes a unique constellation of gastric pathology following ingestion of multiple foreign bodies, concurrent Helicobacter pylori infection, and marked hypereosinophilia. The clinical intervention consisted of removal of intragastric foreign bodies with subsequent eradication of H. pylori, leading to full remission despite the high dysplasia. This context offers several points of discussion regarding pathogenesis, diagnostic strategy, management, and prognostic implications.
The attempt to establish the determining cause of the gastric polyps from a morphological and histopathological perspective is difficult. They could be primarily caused by chronic irritation from the foreign bodies or by H. pylori infection. Histopathology results in this case can find characteristics that occur both in chronic H. pylori infection and persistent mucosal injury. These findings may include foveolar hyperplasia, glandular distorsion or inflammatory cell infiltration.
The idea that the H. pylori infection served as the main cause of mucosal proliferation and possibly produced a synergistic inflammatory impact in addition to the mechanical irritation from the foreign bodies is strongly supported by the significant regression of the patient’s polypoid lesions.
Table 2 summarizes literature case reports regarding the relationship between foreign bodies and gastric polyps and lesions, along with the main features and outcomes.
The development of multiple gastric polyps secondary to chronic foreign body ingestion is an exceptionally rare phenomenon, with limited reports in the literature.
Our patient presented with multiple polypoid lesions visualized using endoscopy, which resolved completely following the removal of the foreign bodies and appropriate medication. These findings suggest a sinergic causal relationship between the chronic presence of foreign objects in the stomach, Helicobacter pylori infection and polyps formation.
The literature on foreign-body-related gastric polyps is largely limited to case reports describing polypoid lesions or mass-like granulomas resulting from chronic mucosal irritation. Daneshbod et al. (2011) reported a case of a peach kernel lodged in the duodenum that mimicked a polypoid tumor endoscopically and was initially misdiagnosed as malignancy before histological analysis revealed no neoplasia but foreign-body-induced inflammation [10]. Okasha et al. (2024) also documented a fishbone-induced gastric granuloma masquerading as malignancy [11]. These cases highlight the potential for foreign bodies to induce chronic inflammatory reactions that mimic polypoid lesions or tumors, though they do not represent true epithelial polyps.
In contrast, the coexistence of a true gastric polyp in association with a foreign body is rare and not well established as causative. Behzad et al. (2020) reported a case of a gastric inflammatory fibroid polyp alongside a foreign-body-induced liver abscess, concluding that the occurrence was coincidental rather than causative [12].
The mechanism by which foreign bodies may induce polypoid lesions likely involves chronic mechanical irritation leading to localized mucosal inflammation, hyperplasia, and regenerative changes. These inflammatory changes can give rise to polypoid appearances, granulomas, or pseudotumoral lesions on endoscopy. Our case presented unique features, with multiple polyps that resolved entirely following the foreign body removal and medical treatment, suggesting these lesions were reactive and reversible rather than true neoplastic polyps.
On the other hand, Helicobacter pylori infection has been implicated in the pathogenesis and persistence of gastric hyperplastic polyps, with multiple studies reporting regression of polyps following eradication therapy [16,17]. The current literature suggests that H. pylori induce a hyperproliferative state via inflammatory cytokines; thus, the mechanism of polyp remission following eradication therapy is likely attributable to the cessation of this inflammatory cascade [18]. Ohkusa et al. demonstrated the disappearance of hyperplastic polyps after successful eradication [19], suggesting a causal role for infection. Subsequent observational work consistently linked H. pylori eradication with polyp regression [20,21]. Several studies pointed out that eradication reduces the recurrence risk after endoscopic resection [22,23], reporting lower recurrence rates post-eradication; drug therapy targeting H. pylori in infected polyps also favorably affected outcomes [24]. Collectively, these data support incorporating H. pylori testing and eradication as part of the management strategy for patients with gastric hyperplastic polyps, especially in the context of endoscopic resection, with a follow-up endoscopy to document regression and monitor recurrence. Table 3 summarize the most relevant publications regarding gastric polyps regression after H. pylori eradication.
Data on the regressions of low- and high-grade dysplasias after eradication of H. pylori infection are very scarce.
The current literature presents meta-analyses on the regression of precancerous lesions (such as atrophic gastritis, along with focal or complete type of intestinal metaplasia) and gastric polyps with eradication of Helicobacter pylori infection, but there is no evidence of moderate dysplasia without resection of lesions [28,29,30]. Piazuelo and collaborators demonstrated that after at least six years without infection, a preneoplastic lesion such multifocal atrophic gastritis is reversible to a non-atrophic state, while the protective effect of anti-H. pylori therapy (ITT) against progression of precancerous lesions remains after 20 years. In the initial years of follow-up, bacterial clearance did not result in any discernible histological changes, according to analysis of the cumulative effect of H. pylori status from baseline to 20 years. However, as the number of years without infection increased, more significant consequences were observed [31].
Several authors reported that eradication of Helicobacter pylori infection decreases the risk of metachronous gastric cancer after removal of dysplastic lesions [32,33].
Two cases of low and moderate gastric epithelial dysplasia with H. pylori infection have been reported in the literature. Following H. pylori eradication, there is evidence of both significant endoscopic expression and regression of histological lesions, after one, two and three years follow-up, while gastric dysplasia was observed at the 3-month follow-up [34].
Given the unique features of the present case, our findings underscore the importance of considering foreign body ingestion in the differential diagnosis of multiple gastric polyps, particularly when the clinical history is suggestive and when other common etiologies are excluded. Endoscopic surveillance following foreign body extraction is recommended to confirm resolution of mucosal abnormalities.
Future studies comprising large number of cases are necessary to be documented to further characterize the pathophysiological mechanisms linking chronic foreign body presence to gastric mucosal proliferation and polyp formation. Until then, clinicians should maintain a high index of suspicion for foreign-body-induced mucosal lesions in atypical cases.
Ultimately, our report provides proof that eliminating the mechanical irritant and the antigenic stimulation, H. pylori can result in the full restoration of the stomach architecture, providing young patients with complicated comorbidities with an organ-sparing prognosis.
4. Conclusions
The development of inflammatory-driven dysplastic gastric lesions is an example of the synergistic pathogenic interaction between persistent Helicobacter pylori infection and prolonged mechanical irritation from retained foreign materials. A case of H. pylori infection and diffuse gastric lesions has been illustrated in this report as a rare association. The gastric lesions significantly regressed after the endoscopic removal of foreign bodies combined with H. pylori eradication. This case suggests that gastric mucosal pathology may be aggravated by the simultaneous presence of chronic mechanical irritation and infection.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Arteaga C.D. Wadhwa R. Gastric Polyp Stat Pearls Stat Pearls Publishing Treasure Island, FL, USA 2025 Available online: http://www.ncbi.nlm.nih.gov/books/NBK 560704/(accessed on 17 February 2026)32809539 · pubmed ↗
- 2Ambe P. Weber S.A. Schauer M. Knoefel W.T. Swallowed foreign bodies in adults Dtsch. Arzteblatt Int.201210986987510.3238/arztebl.2012.0869 PMC 353604023293675 · doi ↗ · pubmed ↗
- 3Oh Y.E. Moon H.S. Upper Gastrointestinal Tract Foreign Bodies Korean J. Helicobacter Up. Gastrointest. Res.202424243010.7704/kjhugr.2024.000240503279 PMC 11967526 · doi ↗ · pubmed ↗
- 4Demiroren K. Management of Gastrointestinal Foreign Bodies with Brief Review of the Guidelines Pediatr. Gastroenterol. Hepatol. Nutr.20232611410.5223/pghn.2023.26.1.136816435 PMC 9911172 · doi ↗ · pubmed ↗
- 5Mikhail E.S. Ghatol A. Hypereosinophilic Syndrome Stat Pearls Stat Pearls Publishing Treasure Island, FL, USA 2025 Available online: http://www.ncbi.nlm.nih.gov/books/NBK 599558/(accessed on 17 February 2026)38261702 · pubmed ↗
- 6Hrabar D. Duvnjak M. Lerotic I. Tomasic V. Supanc V. Bilic B. Gastric foreign body Gastrointest. Endosc.200663498499; discussion 49910.1016/j.gie.2005.06.06816500405 · doi ↗ · pubmed ↗
- 7Ridolo E. Melli V. De’ Angelis G. Martignago I. Eosinophilic disorders of the gastro-intestinal tract: An update Clin. Mol. Allergy 2016141710.1186/s 12948-016-0055-y 27956893 PMC 5131414 · doi ↗ · pubmed ↗
- 8Malfertheiner P. Megraud F. Rokkas T. Gisbert J.P. Liou J.-M. Schulz C. Gasbarrini A. Hunt R.H. Leja M. O’Morain C. Management of Helicobacter pylori infection: The Maastricht VI/Florence consensus report Gut 2022 gutjnl-2022-32774510.1136/gutjnl-2022-327745 · doi ↗