Evaluating Treatment and Safety Outcomes of a Shorter Regimen for Drug-Resistant TB in Nigeria: An Implementation Research Study
Victor Babawale, Clement Adesigbin, Corinne S. Merle, Vanessa Veronese, Fatimata Bintou Sall, Benjamin Seydou Sombie, Eunice Nnaisa Jiya-Chitumu, Chizaram Onyeaghala, Adegboyega Moses Oyefabi, Rotimi Samuel Owolabi, Osman Eltaye, Olusoji Ige, Ogiri Sam, Obioma Akaniro

TL;DR
A shorter, all-oral regimen for drug-resistant tuberculosis in Nigeria shows promising results in improving patient outcomes and quality of life.
Contribution
This study evaluates the effectiveness and safety of a shorter, all-oral regimen for drug-resistant TB in a real-world Nigerian setting.
Findings
The intervention group had a higher, though non-significant, proportion of favorable outcomes compared to the standard of care group.
Intervention participants showed greater improvements in health-related quality of life compared to those receiving standard care.
About one-third of patients experienced serious adverse events, with no significant difference between the two groups.
Abstract
The introduction of significantly shorter, all-oral regimens has significantly shifted the management of drug-resistant tuberculosis (DR-TB) towards a more tolerable and patient-centred therapeutic approach that aims to enhance treatment adherence, clinical outcomes, and quality of life among patients. Nigeria has gradually adopted this all-oral, shorter regimen, but the impact of this regimen in programmatic settings has not yet been studied. In 2022, a longitudinal, two-armed cohort study was conducted to explore the effectiveness, safety, and feasibility of the all-oral shorter regimen in the programmatic management of RR/MDR-TB in Nigeria. Consenting and eligible RR/MDR-TB patients receiving the all-oral regimen (intervention group) in four states were consecutively enrolled and compared to those receiving the standard of care (SOC). Treatment effectiveness, proportion, and 95%…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
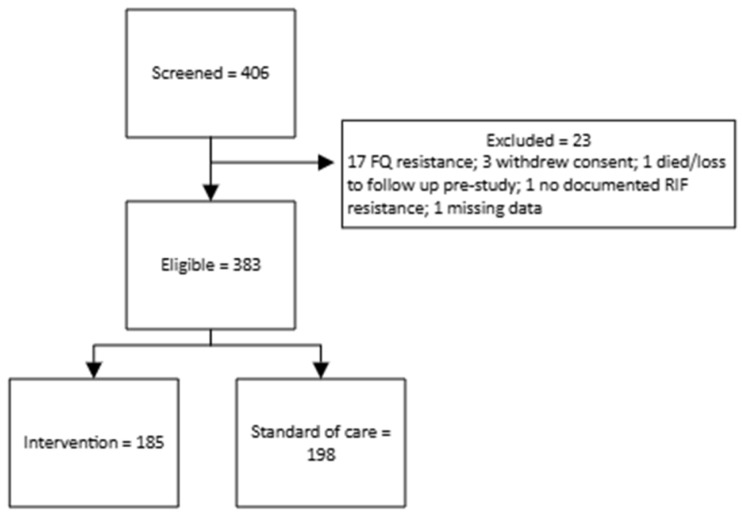 Figure 1
Figure 1- —United States Agency for International Development (USAID)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTuberculosis Research and Epidemiology · Healthcare Facilities Design and Sustainability · Advanced Data Processing Techniques
1. Introduction
The emergence of drug-resistant TB is a significant public health problem and an obstacle to achieving effective global TB control [1,2]. An estimated 400,000 people developed rifampicin-resistant or multidrug-resistant TB (RR/MDR-TB) in 2023, leading to an estimated 150,000 deaths [3,4,5,6]. Nigeria is among the 30 highest burden countries for MDR/RR-TB, and while the estimated number of incident RR/MDR-TB cases have almost halved over the past decade, challenges such as sub-optimal practice of and adherence to directly observed treatment (DOT), poor infection prevention and control measures, and increasing community transmission of drug-resistant TB contribute to ongoing transmission in Nigeria [7,8,9,10]. In line with the World Health Organization (WHO) guidance, Nigeria has recently scaled up the expansion of the rapid molecular diagnostic platforms to enhance diagnostic accuracy and timely TB diagnosis and the detection of drug resistance.
In 2019, the WHO released new consolidated guidelines on the treatment of DR-TB, which recommended the transition to an all-oral, shorter regimen for patients with RR/MDR-TB, without resistance to fluoroquinolones [11]. The use of a shorter, all-oral regimen containing linezolid for those resistant to fluoroquinolones (BPaL regimen) was also advised under operational research conditions [12,13,14,15,16,17]. Consequently, these new regimens were adopted by the National Tuberculosis and Leprosy Control Programme (NTBLCP) of Nigeria. This implementation research study was conducted to evaluate the effectiveness, safety, and impact on the quality of life of the all-oral shorter regimens delivered under programmatic conditions in Nigeria.
2. Materials and Methods
2.1. Study Design
A prospective cohort study with two parallel arms was undertaken among MDR/RR-TB patients receiving the all-oral shorter MDR/RR-TB regimen compared to a comparison group receiving the standard of care (SOC). The study was conducted in eight selected states across Nigeria, with four randomly selected as the intervention group for the all-oral shorter regimen (Oyo, Plateau, Ebonyi, and Rivers) and the other four states as the control group for SOC (Ogun, Nasarawa, Abia, and Kaduna). The ShORRT research package, developed by The Special Programme for Research and Training in Tropical Diseases (TDR), was adapted to the Nigerian context for the development of the research protocol and data collection tools [18].
2.2. Participants
The study population comprised patients evaluated at selected TB clinics with bacteriologically confirmed rifampicin-resistant tuberculosis (RR-TB) or those clinically suspected of MDR/RR-TB, including children with a history of close contact with a confirmed MDR/RR-TB case. Children likely to be MDR/RR-TB based on a history of close contact with a confirmed MDR/RR-TB case were also considered. Eligibility criteria were defined as follows: willing and able to give informed consent (including signed or witnessed consent for illiterate patients and signed or witnessed consent from a parent or legal guardian for minors), and evidence of bacteriologically confirmed TB and resistance to at least rifampicin. Patients whose DST results identified resistance to fluoroquinolones, who were unable to take oral medication, had allergies or were taking other medications that contraindicated any of the medicines under investigation, and/or patients who had a corrected QT (QTc) interval of >500 msec were considered ineligible.
2.3. Treatment Regimens
Patients received either the modified all-oral shorter regimen (intervention) or the WHO-approved RR/MDR-TB regimen in use in Nigeria at the time (SOC), according to the regimen implemented in their state. The all-oral shorter regimen consisted of a 4–6-month intensive phase with bedaquiline (Bdq), high-dose levofloxacin (hLfx), linezolid (Lzd), and clofazimine (Cfz), followed by a 5-month continuation phase with Bdq (for the first two months), hLfx, Lzd, and Cfz.
The standard of care regimen consisted of 4–6 months of Bdq, moxifloxacin (Mfx), clofazimine (Cfz), high-dose isoniazid (Hh), prothionamide (Pto), ethambutol (E), and pyrazinamide (Z), followed by 5 months of Mfx, Cfz, E, and Z. Dosing was weight-based (Table 1).
Both regimens were fully oral and had a total duration of approximately 9–12 months. The main differences between regimens were the fluoroquinolone backbone (hLfx vs. Mfx) and the inclusion of linezolid with clofazimine in the all-oral shorter regimen versus high-dose isoniazid and prothionamide in the SOC regimen, reflecting efforts to improve tolerability and simplify treatment while maintaining efficacy.
2.4. Study Procedures
Patients presenting to any one of the eight study sites during the recruitment period and found to have evidence of resistance to rifampicin by either culture or molecular DST (i.e., Xpert MTB/RIF or Line Probe Assay) were assessed for enrollment and asked to provide informed consent. Consenting and eligible patients underwent the following baseline screening: collection of patient demographics and medical history; clinical evaluation, bacteriological and other laboratory testing; a chest X-ray and a 12-lead electrocardiogram (ECG) (or single-channel portable monitors). Chest X-ray (CXR) was used to determine the extent of pulmonary disease based on the proportion of lung fields involved. For ease of interpretation, we categorized radiographic extent into three ordered groups: category A (<25% of lung fields affected), category B (25–49% of lung fields affected), and category C (≥50% of lung fields affected or bilateral/multilobar disease). Higher categories therefore indicate more extensive lung damage.
After screening, treatment was initiated and patients were followed up monthly during the 9–12-month treatment phase. Monthly follow-up comprised clinical examination, collection of sputa for smear and culture, laboratory testing (hematology and serum liver enzymes, thyroid-stimulating hormone (TSH) at months three and six only, and ECG. DST was performed at baseline and after any reversion identified during treatment, and/or if any culture was found positive during the post-treatment follow-up or after conversion. At each visit, patients were asked about any adverse events experienced since the previous visit for monitoring and management.
At the end of the treatment phase, patients were followed for an additional 12 months and asked to return at six and 12 months post-treatment completion (or sooner in the event of TB clinical symptoms) for clinical assessment and sputum collection for smear and culture; culture-positive patients received follow-up DST examination (either culture or molecular), LPA, and CXR which was also performed among patients under suspicion of recurrent TB.
Disability assessment was conducted at baseline, end of treatment, and during follow-up using the Modified Medical Research Council Dyspnea Scale (mMRC), which is used to assess the degree of baseline functional disability due to dyspnoea by assigning a numerical score (0–4) to various statements reflecting the degree of breathlessness [19]. Health-related quality of life was also assessed at baseline, month four, end of treatment, and at 12-month follow-up using the EQ-5D-5L tool (Table 2).
2.5. Study Outcomes
The primary outcome was the effectiveness and safety of the intervention regimen compared to SOC. Effectiveness was defined as those with a favourable treatment outcome (patients who have completed treatment with no evidence of failure but who do not have bacteriological evidence of cure) or cure (patients who have completed treatment, have no evidence of failure, and at least two consecutive negative cultures at least 30 days apart at the end of treatment), and without recurrence at 12 months after the end of treatment. The primary safety outcome was defined as the proportion of patients reporting any occurrence of a serious adverse event (SAE) during treatment and up to six months after the end of the treatment.
Secondary outcomes assessed were as follows: treatment adherence (defined as patients missing less than 10% of treatment doses during the course of their therapy); proportion of patients self-reporting experiences of disability due to breathlessness using the mMRC Dyspnoea scale to measure the degree of disability that breathlessness poses on day-to-day activities on a scale from 0 to 4; [19]; proportion cured without permanent disability: a combined outcome, using the mMRC scale based on which patients with a score above 2 are considered permanently disabled in terms of their pneumological function, in addition to all serious adverse events by system organ class that are not resolved at the end of treatment, and; health-related quality of life: measured at baseline, month 4, end of treatment, and follow-up using the EuroQol visual analogue scale (EQ-VAS), a standardized tool that records patients’ self-rated health on a vertical scale from 0 (“the worst health you can imagine”) to 100 (“the best health you can imagine”). This tool was used to assess perceptions of health and functioning across five dimensions at baseline, month four, end of treatment, and at follow-up [19].
2.6. Recruitment and Sample Size
The target sample size of 400 participants (200 per arm) was determined based on the existing and projected case load and potential recruitment rate of bacteriologically confirmed DR-TB patients across each of the selected study sites. At each site, all consecutively presenting patients with bacteriologically confirmed RR/MDR-TB who met the eligibility criteria during the recruitment period were invited to participate until the overall sample size was reached. This approach reflects routine programmatic enrolment rather than random sampling of individuals.
2.7. Data Collection and Analysis
Socio-demographic, clinical, and laboratory data were collected from all participants using routine forms and registers and study-specific forms. Clinical data, including adverse events, laboratory data such as results of DST and other microbiological test results, were recorded onto the patient’s medical records and/or treatment cards and acted as the source documents. Individual patient case report forms (CRFs) were developed for the study and patient data was abstracted from source documents onto CRFs on at least a monthly basis by research assistants working at the study sites.
An electronic database, REDCap, was created and used to support data storage and management. Data was transposed from the CRFs to the REDCap database by a focal point at each of the study sites. Research staff at the national level had access to the database and were responsible for regular data review, management, and the identification of discrepancies. Any issues related to data quality or completeness were addressed directly with the relevant study team.
Descriptive statistics were used to summarize patient characteristics at baseline, and significance tests (Chi-square test, Fisher’s exact test, Mann–Whitney test, or Kruskal–Wallis tests as appropriate) were used to identify significant differences between the two treatment groups, including the occurrence of AEs of interest during the treatment phase. For treatment effectiveness, the proportion and 95% confidence intervals (CIs) of favourable and unfavourable treatment outcomes were measured at the end of treatment and during follow-up. Risk ratios were calculated to evaluate the differences in outcomes across the two groups and were adjusted by selected patient and clinical variables to account for possible confounding. Stata version 17 (StataCorp LLC, College Station, TX, USA) was used to perform all statistical analyses.
2.8. Ethics
This study received ethical approval from the WHO Research Ethics Review Committee (Protocol ID: ERC.0003305) and the National Health Research Ethics Committee (NHREC/01/01/2007 -01/06/2020). Written (or witnessed in the case of illiterate or minor participants) informed consent was obtained from all patients. All participant information was handled in accordance with applicable ethical and data protection standards. Personal identifiers were removed from study datasets and replaced with unique study identification numbers to ensure anonymity. Data were stored in password-protected electronic REDCap databases accessible only to authorized study personnel. Hard-copy CRF documents were kept in locked cabinets within secure offices. No identifiable patient information was included in the analysis or reporting.
3. Results
Between the 3rd of November 2020 and the 25th of May 2022, 406 patients were screened, of whom 17 were excluded on the basis of identified FQ resistance, three withdrew their consent, one died before treatment commenced, one did not have evidence of rifampicin resistance, and one had no data. Of the 383 remaining patients included in the analysis, 185 patients were enrolled at the intervention sites and received the all-oral shorter regimen and 198 patients were enrolled at the control sites and received the standard of care regimen (Figure 1).
Overall, patients had a median age of 35 (IQR: 25–45), were male (64.0%), new TB cases (77.8%), were previously treated with first-line drugs (92.9%), had a median BMI of 18.4, reported no existing neuropath (98.4%), returned a negative pregnancy test for female patients (87.6%), tested negative for HIV (90.1%), Hepatitis B and C (94.3 and 96.9%, respectively), and diabetes (94.3%). Measurements for the assessed clinical variables are presented in Table 3. The disability assessment identified that the majority of patients reported breathlessness with strenuous exercise (64.8%) and one-fifth reported breathlessness with moderate exertion, such as walking quickly or on an incline (23.9%). Patients in the two treatment groups differed significantly across the following variables: age group, patient type, Hepatitis B status, glucose, and creatinine values (Table 3).
The majority of patients were sputum smear-negative (48.6%) and culture-positive (59.5%). All patients were resistant to rifampicin, almost all had documented sensitivity to fluoroquinolone (84.9%), and roughly half were sensitive to isoniazid (48.0%). Just under half had evidence of cavitation on chest X-ray (45.7%) and two-fifths were classified as disease severity category B (41.5%). Patients in the two treatment groups differed significantly across the following clinical variables: sputum smear status, fluoroquinolone and isoniazid sensitivity status, cavitation on CXR, and extent of disease category (Table 4).
3.1. Effectiveness of Shorter All-Oral Regimen
At the end of the follow-up period, the intervention group had a higher but non-significant proportion of favourable treatment outcomes compared to the standard regimen (80.5% vs. 69.7%; p > 0.05). One episode of recurrent TB was noted in each group. Similar proportions in both arms were considered cured without permanent disability (Table 5).
Patients in the intervention group also had a higher proportion of favourable outcomes at the end of treatment: 81 vs. 76.8% among patients receiving the SOC. Five patients in the intervention group had treatment failure compared to three in the SOC regimen group (2.7 vs. 1.5%, respectively). Of the five failures in the intervention group, four were due to bacteriological reversion of sputum culture after conversion to negative, and one was due to a permanent change of at least two anti-TB drugs in the regimen because of adverse drug reactions (ADRs). All three failures in the SOC regimen were due to a lack of culture conversion after 4 months of treatment. Overall treatment adherence was high across both arms (Table 6).
3.2. Safety Outcomes
During the treatment phase, 344 patients overall (90.0%), with similar proportions across the two groups (87 vs. 92% intervention vs. SOC), experienced AEs. Overall, 1277 individual AEs were reported or an average of four per patient (IQR 2–5) and two per patient for AEs of interest among patients experiencing at least one AE during the treatment phase (IQR 2–3; Table 7).
The most frequently reported events were elevated liver enzymes (37.7%), QTc prolongation (27.6%), and anemia (21.1%), followed by thrombocytopenia (11.4%). Other events were uncommon, each accounting for less than 2% of reported events. Regarding severity, most AEs were grade 1 (45.9%) or grade 2 (38.2%), while grade 3 and grade 4 events represented 12.4% and 3.5% of events, respectively. The distribution of AE types and severity grades was broadly similar between treatment groups (Supplementary Data, see Appendix A Table A1).
When considering the proportion of participants experiencing at least one AE of interest, 279 participants (73.4%) experienced elevated liver enzymes, 211 (55.5%) experienced QTC prolongation, and 184 (48.4%) experienced anemia. The proportion of participants with elevated liver enzymes was significantly higher in the standard regimen group compared with the all-oral shorter regimen group (79.4% vs. 66.9%, p = 0.008). Conversely, peripheral neuropathy occurred only in the all-oral shorter regimen group (3.9% vs. 0.0%, p = 0.005). No statistically significant differences were observed between treatment groups for the other adverse events, including anemia, thrombocytopenia, leukopenia, QTc prolongation, anxiety, depression, optic neuritis, and ototoxicity (Supplementary Data, see Appendix A Table A2).
Serious Adverse Events
In total, there were 32 patients who experienced at least one SAE with a non-significant difference in the proportion of SAE patients between the two groups. The majority of SAEs were deaths, which occurred among 11 patients in the all-oral group and 17 in SOC (85.7% and 81.0%, respectively). None of the SAEs were determined as related to the medication, 69.7% were deemed unrelated, and 30.3% were unable to be attributed due to insufficient data (Table 8).
3.3. Health-Related Quality of Life
Between baseline and 4 months, participants receiving the all-oral shorter regimen showed significantly greater improvement in self-assessed median health-related quality of life compared with those on the standard regimen (β 3.2, 95% CI 0.59–5.8; p = 0.017); however, there were no significant differences observed at the other timepoints (Table 9).
4. Discussion
This study provides important evidence supporting the effectiveness and safety of an all-oral shorter regimen for the treatment of rifampicin-resistant and multidrug-resistant tuberculosis (RR/MDR-TB) in Nigeria, compared to the standard of care (SOC) regimen. Although differences in treatment success between the two regimens did not reach statistical significance, the all-oral shorter regimen consistently demonstrated favourable trends, including higher proportions of treatment success and lower rates of death and loss to follow-up. These findings reinforce the potential of this regimen to improve RR/MDR-TB outcomes in programmatic settings and point to a regimen that is well tolerated by patients in Nigeria.
Our findings demonstrated that the all-oral shorter regimen achieved a higher treatment success rate at the end of treatment (81.1% vs. 76.8% for SOC), with a notably higher cure rate (80.7% vs. 68.8%). While these findings were not significant, the results are consistent with recent clinical trials and observational studies that have reported improved efficacy, tolerability, and adherence associated with shorter, fully oral regimens [20,21,22]. The advantages of this all-oral approach include shorter treatment duration, elimination of injectable toxicities, and greater convenience, all of which likely contribute to enhanced treatment adherence and patient satisfaction [23].
Despite high initial success rates, treatment outcomes declined slightly over longer follow-up due to increasing non-assessable patients, underscoring the critical need for strengthened post-treatment surveillance and support. The occurrence of treatment failures, primarily due to bacteriological reversion in the all-oral group and lack of culture conversion in the SOC group, warrants further investigation to elucidate potential contributing factors such as drug pharmacokinetics, adherence patterns, or comorbid conditions [24].
Safety profiles were broadly comparable between regimens, with no drug-related serious adverse events reported. Notably, one-third of patients experienced elevated liver enzymes and a significant proportion developed prolonged QT intervals, highlighting the importance of close clinical and laboratory monitoring to promptly identify and manage potential toxicities [25,26]. The low incidence of other adverse effects such as neuropsychiatric symptoms, anemia, and ototoxicity affirms the relative safety and tolerability of these regimens [27,28].
Mortality rates, although relatively low, remain concerning and were not attributable to treatment-related adverse events. Contributing factors such as comorbidities, treatment delays, and social determinants must be addressed to further reduce mortality in this vulnerable population [29,30,31]. The absence of prolonged hospitalizations with the all-oral regimen suggests potential benefits for decentralizing care and reducing healthcare system burdens, enhancing accessibility and patient-centred care.
While this study has generated important evidence on the effectiveness, safety, and health-related quality of life of the new shorter regimen for DR-TB in real-world, programmatic settings, it must be considered with the following limitations in mind: (1) the use of a non-randomized study design is inherently susceptible to selection bias; however, we attempted to mitigate this through cluster-level allocation and systematic enrollment of all eligible DR-TB patients; (2) we did not conduct certain exploratory analyses, such as assessing associations between disease extent, cavitation, and treatment outcomes, which were beyond the pre-specified analysis plan yet could present a more nuanced understanding of treatment effectiveness, nor did we conduct stratified analyses by age or resistance profile due to the small number of children and patients with isoniazid resistance included in the study; and (3) this study was not sufficiently powered to detect differences in rare adverse events.
In conclusion, our study substantiates the World Health Organization’s recommendation and supports the Nigerian National Tuberculosis and Leprosy Control Programme’s transition to all-oral shorter regimens for RR/MDR-TB management. The all-oral shorter regimen showed comparable effectiveness to the standard of care, with favorable trends in outcomes and a generally acceptable safety profile, supporting its continued programmatic implementation. Future efforts should prioritize robust follow-up systems, ongoing pharmacovigilance, and research into factors influencing treatment failure to optimize clinical outcomes and curb the RR/MDR-TB epidemic in Nigeria and similar settings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tiberi S. Utjesanovic N. Galvin J. Centis R. D’Ambrosio L. van den Boom M. Zumla A. Migliori G.B. Drug resistant TB–latest developments in epidemiology, diagnostics and management Int. J. Infect. Dis.2022124 S 20S 2510.1016/j.ijid.2022.03.02635342000 · doi ↗ · pubmed ↗
- 2Xi Y. Zhang W. Qiao R.J. Tang J. Risk factors for multidrug-resistant tuberculosis: A worldwide systematic review and meta-analysis P Lo S ONE 202217 e 027000310.1371/journal.pone.027000335709161 PMC 9202901 · doi ↗ · pubmed ↗
- 3Kumari S.L. Kongara S. Bhaskar K. Srikanti R. Rao C.R. Sanjana P.H. Outcomes and adherence of shorter MDR TB regimen in patients with multidrug resistant tuberculosis Indian J. Tuberc.20237010310610.1016/j.ijtb.2022.03.02136740304 · doi ↗ · pubmed ↗
- 4Koirala S. Shah N.P. Pyakurel P. Khanal M. Rajbhandari S.K. Pun T. Shrestha B. Maharjan B. Karki S. Tamang K.B. High success and low recurrence with shorter treatment regimen for multidrug-resistant TB in Nepal Public Health Action 202111384510.5588/pha.21.004134778014 PMC 8575385 · doi ↗ · pubmed ↗
- 5WHO Global Tuberculosis Report WHO Geneva, Switzerland 2023
- 6Shibabaw A. Gelaw B. Gebreyes W. Robinson R. Wang S.H. Tessema B. The burden of pre-extensively and extensively drug-resistant tuberculosis among MDR-TB patients in the Amhara region, Ethiopia P Lo S ONE 202015 e 022904010.1371/journal.pone.022904032053661 PMC 7018133 · doi ↗ · pubmed ↗
- 7Prasad R. Singh A. Gupta N. Adverse drug reactions with first-line and second-line drugs in treatment of tuberculosis Ann. Natl. Acad. Med. Sci.202157153510.1055/s-0040-1722535 · doi ↗
- 8Silva D.R. Mello F.C. Migliori G.B. Shortened tuberculosis treatment regimens: What is new?J. Bras. Pneumol.202046 e 2020000910.36416/1806-3756/e 2020000932215450 PMC 7462706 · doi ↗ · pubmed ↗