Exploring the use of art interventions in challenging stigmas related to neurological disorders: A scoping review
Jack Lumsdon, Vivian Nyadimo, Shilla Dama Unda, Natasha Fothergill-Misbah, Mary A. Bitta, Loretta Giuliano, Loretta Giuliano, Loretta Giuliano

TL;DR
This study reviews how art can help reduce stigma around neurological disorders like epilepsy and dementia, finding that it can change attitudes and raise awareness.
Contribution
The novelty lies in systematically evaluating art-based interventions for stigma reduction in neurological disorders through a scoping review.
Findings
Art-based interventions effectively reduced stigma by addressing misinformation and encouraging supportive actions.
Interventions involving direct interactions with people with lived experience were particularly effective.
Digital media and theatre have potential to reach larger audiences but require further exploration.
Abstract
Stigma remains a major barrier to accessing healthcare for people with neurological disorders. The World Health Organization’s Intersectoral Global Action Plan on epilepsy and other neurological disorders urges all member countries to have at least one functioning awareness campaign for neurological disorders by 2031. Art has emerged as a valuable tool for social change with previous success in highly stigmatised disorders. This review aims to understand the effectiveness of art-based interventions in reducing stigma related to neurological disorders. A scoping review was conducted on three databases (PubMed, Web of Science, and Embase); from inception to October 2024. Data relevant to the study’s aims were extracted and underwent narrative synthesis to develop key themes and patterns across the included studies. After removing duplicates, 9,992 articles were screened with 24 articles…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
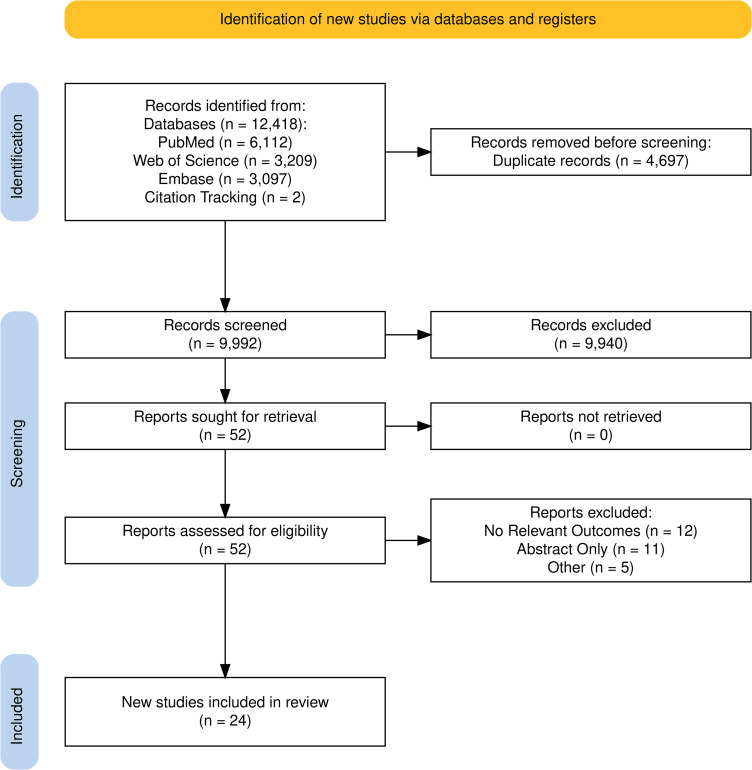 Fig 1
Fig 1- —http://dx.doi.org/10.13039/501100000286British Academy
- —http://dx.doi.org/10.13039/501100000286British Academy
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsArt Therapy and Mental Health · Mental Health and Patient Involvement · Empathy and Medical Education
Introduction
Neurological disorders affect over 1 in 3 people and are the leading cause of illness and disability worldwide [1]. This burden is felt the most in low- and middle-income countries (LMICs), where 70% of people with neurological disorders live [2]. Despite advancements in the diagnosis and treatment of neurological disorders, multiple barriers limit the accessibility of health services. One significant barrier to the diagnosis, treatment, and social integration of individuals with neurological disorders is stigma [3]. Stigma associated with neurological disorders is a widely recognised global health issue [4]. Stigma can have many cumulative downstream consequences which can have direct health implications, for example, delayed diagnosis and limited access to treatment, as well as social implications, including social isolation, thereby exacerbating the disease burden and hindering effective care [5]. Understanding and mitigating stigma surrounding neurological disorders is essential for improving the wellbeing of individuals and enhancing quality of life.
Stigma related to neurological disorders takes multiple forms including social, self, and structural. Social stigma leads to exclusion and discrimination [6], self-stigma causes shame and deters care-seeking [5]., and structural stigma is embedded in policies, which can reduce access to treatment [7]. Stigma is often more pronounced in LMICs due to varying levels of awareness and medical education, which is largely a result of little funding, insufficient human resources and a lack of political support to invest in anti-stigma campaigns [8]. While some stigmatising factors such as fear, visibility, and unpredictability of symptoms may be globally experienced [9]. Some factors can be continent specific such as cultural beliefs around witchcraft and curses which are common in African countries such as Tanzania and Kenya for disorders like epilepsy and Parkinson’s [10–12]. Other continents, such as Asia, see a diagnosis as private and would prefer to be labelled drunk rather than divulge a diagnosis [13]. Both of which negatively influence health seeking behaviours and contribute towards isolation. Sudden or fluctuating symptoms such as seizures or stroke may provoke fear, misattribution, and isolation [14,15]. This complex stigma landscape hampers inclusion, care, and understanding for individuals living with neurological disorders, perpetuating cycles of fear and exclusion [16].
Tackling stigma is a key goal of the World Health Organization’s Intersectoral Global Action Plan on epilepsy and other neurological disorders 2022–2031 (IGAP) [2], which outlines a proposed action for Member States to “lead and coordinate intersectoral advocacy strategies for reducing stigma and discrimination” (p. 14). IGAP’s global target 1.2 states that 100% of countries will have at least one functioning awareness campaign of advocacy programme for neurological disorders by 2031. Although various awareness campaigns for neurological disorders have launched globally, public education remains inadequate, and stigma continues to limit access to healthcare, employment, and social inclusion for affected individuals [11,17]. It is unclear what these awareness campaigns should look like, particularly in LMICs, and how to measure their success. Creating a functional campaign requires innovative strategies and active engagement of stakeholders across sectors, ensuring the empowerment and involvement of people with lived experience of neurological disorders including their caregivers and members of the communities they live in. Given these challenges, it is critical to explore alternative, culturally relevant approaches that can help shift perceptions, reduce stigma, and promote inclusion.
Art has emerged as a valuable tool for social change, offering a platform to challenge stereotypes, foster empathy, and promote dialogue [18,19]. Within healthcare, artistic interventions serve both educational and therapeutic functions, enabling individuals to share their lived experiences and humanise stigmatised disorders [20]. The use of arts has also been successful in tackling the stigma of certain disorders such as mental illness [21]. Various art based initiatives are now branching into neurological disorders to provide compelling representations of the experiences of people with lived experience which serve to enhance public understanding and engagement [22]. These initiatives have been useful in challenging societal stigma and structural stigma by advocating for a holistic approach to care which values meaningful engagement. Performing arts offer interactive and immersive storytelling approaches that can highlight the struggles and resilience of people with lived experience, thereby counteracting prevailing misconceptions [23]. Similarly, literary arts and visual arts, serve as effective mediums for conveying the realities of people with lived experience [24], such as the use of photo-stories and fiction writing to address HIV stigma [25].
The potential use of art in addressing stigma related to neurological disorders remains largely unexplored [26]. This review seeks to assess the effectiveness of art-based interventions in reducing stigma related to neurological disorders, identify the most impactful artistic approaches and their mechanisms of influence, examine how demographic and cultural factors shape intervention effectiveness, and evaluate the challenges, barriers, and long-term sustainability of art-based stigma reduction initiatives.
Methods
This review aims to provide a general overview of the literature, as opposed to answering a specific question. As such, a scoping review was deemed the most appropriate methodology [27]. This scoping review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines [28]. A completed PRISMA checklist is provided as supplementary S1 File. The aim of the review is to systematically map existing literature on the use of art-based interventions for stigma reduction in neurological disorders, a protocol was not published for this.
Eligibility criteria
This review of peer-reviewed original publications included studies that evaluated interventions incorporating visual arts theatre, film, storytelling, or music as a means of addressing stigma. Studies were eligible if they assessed the impact of these interventions on stigma-related outcomes (conceptualised as changes in knowledge, attitudes and behaviour) and provided information on intervention characteristics, target populations and geographic distribution. Published reviews were excluded, although reference lists were searched for any relevant articles. No restrictions were imposed on study design, publishing date or geographic location to ensure a comprehensive synthesis of the available evidence.
Information sources
Systematic searches were conducted across three key databases: PubMed, Web of Science, and Embase. These databases were chosen as they provide a comprehensive and multi-disciplinary overview of available literature. PubMed highlights medical research while Web of Science and Embase provide access to social science literature. Searches yielded relevant peer-reviewed literature published from inception until October 2024 when the search was carried out.
Search strategy
The search strategy identified articles using art-based interventions in the context of neurological disorders targeting stigma and efforts to raise awareness. The search strategy can be found in S2 File.
Selection process
All search results were imported into Rayyan, a web-based application designed to assist in systematic reviews [29]. Duplicate records were identified using Rayyan then manually checked and removed. Two independent reviewers (VN & SD) conducted the title and abstract screening process for relevance, followed by a full-text review by VN & JL for eligible studies. Citation tracking was used to identify additional relevant articles which were not identified within the initial search. Discrepancies in study selection were resolved through discussion or consultation with a third reviewer (NFM & MB).
Data extraction
A data extraction form was developed to include relevant data items to address the review’s aims. To ensure rigor and reduce bias, data extraction was performed by two reviewers (VN & JL) to collect information on intervention type, study design, target population, geographic distribution, and stigma-related outcomes; any discrepancies were discussed and resolved through consensus.
Data interpretation
Using the Patterns, Advances, Gaps, Evidence for practice and Research recommendations framework, the key findings of the review were visualised using a patterning chart [30]. Extracted data were analysed using a narrative synthesis approach to identify key themes and patterns across studies [31]. Given the expected heterogeneity in study methodologies and outcome measures, no formal meta-analysis was conducted. Instead, findings were summarised descriptively, with tabulated data where applicable, to provide a structured overview of intervention characteristics and effects.
Results
Study characteristics
As indicated in Fig 1, three databases were searched for articles published prior to October 2024. A total of 12,420 articles were identified. After removing duplicates, 9,992 titles and abstracts were screened. Fifty-two articles were retrieved for a full text review, with 24 articles identified for inclusion within this review. Extracted study characteristics (Table 1) and an overview of extracted data (Table 2) enabled patterns within the data to be summarised. The final extracted dataset is available as supplementary S3 File.
Table 1: Study characteristics of included studies.
Table 2: Patterning chart of included studies.
PRISMA flow diagram of included studies.
Included studies predominantly occurred in high-income countries in North America, Europe, and Australasia (63%) [34,35,39–48,51–53] with fewer studies conducted across the South Americas (13%) [36,50,54], Asia (17%) [32,33,38,49], and Africa (13%) [37,49,55]. Art interventions aimed at reducing stigma addressed three neurological disorders: dementia (38%) [41–45,48,51–53], epilepsy (42%) [32,33,36,37,39,40,46,47,54,55], and stroke (21%) [34,35,38,49,50]. Interestingly, no articles were included tackling other common neurological disorders such as Parkinson’s disease and Multiple Sclerosis.
Targeted populations and types of stigmas explored
The target population of the art intervention varied between the general population (50%) [32–34,36,38,41,47–52], children (33%) [32,35,37,39,40,53–55], and university students (25%) [42–47]. Additionally, some papers explored internal stigma among people with lived experience (13%) [36,41,52]. 71% articles reported the age of participants with a range of 7–65+ [32,34,35,37,39,40,43,45–51,53–55] while 67% reported the sex of participants, with the participation of females ranging from 27–85.3% with an average of 56% females per study [33,34,37,39–43,45–51,54,55]. Due to the broad methods of data collection, some studies did not report demographics.
While all studies explored the use of arts to address stigma, hence their inclusion, these could be broken down further into studies exploring the effectiveness of educational materials (46%) [32,33,35,37,39,40,46,49,50,54,55], focusing on leveraging the lived experience to reduce stigma (38%) [36,41–45,51–53], and a mix of the two aims (17%) [34,38,47,48].
Types of art employed
The most common form of art employed was videos (38%) [32–35,40,41,46,49,50]. These were predominantly short educational videos conveying disorder specific information such as risks, symptoms, and how to respond to a stroke or seizure. All studies using videos aimed to assess the effectiveness of educational materials. Of the 54% of studies leveraging lived experience to tackle stigma, a more diverse range of arts were used, such as visual media (54%) [34,38,44,45,47,48,53] (e.g., short films, adverts, and use of images such as comic books or posters), dance and theatre (38%) [34,36,41,51,52], auditory means (23%) [42–44] such as music, storytelling, and poetry, and painting (15%) [41,45]. Regarding the evaluation of interventions, 63% used quantitative methods [32–35,37,39,40,45–47,49–51,54,55], 21% used qualitative methods [36,38,41,44,52,56], and 17% used mixed methods [42,43,48,53].
Impact of art interventions in reducing stigma and mechanisms of change
Only 21% [34,43–45,53] of studies involved multiple sessions of an intervention with most studies being a one off intervention which limits the conclusions which can be drawn from the effect of intervention length. 96% of included studies found positive impacts on stigma following an art intervention. These studies included a pre- and post- comparison or comparison to ‘naïve’ controls. The one study without a significant positive impact may be due to the control group receiving a non-art based intervention [47]. This indicates that future studies should explore the comparison between art and non-art-based interventions to fully investigate how art itself may mediate outcomes. Additionally, another study resulted in overall positive effects, however, some outcomes worsened which indicates the need to quality control the knowledge being shared during art interventions [54].
Included studies showcased diverse mechanisms of change, with 71% studies focusing on the change in attitudes and perceptions [32–34,37,39,40,42–48,51,52,54,55], 54% on raising awareness and enhancing knowledge [32–35,37–40,46,47,49,50,54,55], and 42% on the influence of emotional engagement, empathy, and social inclusion [33,36,38,41–46,51]. Studies also captured how the intervention influenced behaviours and practices (21%) [34,44,52,54,55], the use of a follow-up to demonstrate the long-term effects of art-based interventions (13%) [35,40,54], and the value of cultural adaptation (5%) [48]. This highlights the broad and dynamic ways in which arts-based interventions can tackle stigma. In the subsequent sections of the results, we use the three domains of stigma (knowledge, attitudes, behaviours) to expound on mechanisms which brought about stigma reduction. Within the theme of behaviour, we also describe the impact of the intervention on emotions,
Shifting attitudes.
A shift in in attitudes was primarily tackled in two ways, either by educational means in which participants learnt about a disorder (79%) or by working directly alongside people with lived experience while creating art, which allows for biases and misconceptions to be rewritten (21%). This was primarily achieved through emotional engagement and fostering empathy. Theatre-based interventions helped transform negative biases into more positive perceptions, with participants reporting more relaxed and excited emotions following the performance [51]. Similarly, a 10-minute first aid informational video on epilepsy shown to psychology undergraduate students in Australia addressed stigma with significant improvements to a questionnaire around being afraid (r = .53) or nervous (r = .38) around a person with epilepsy, and led to students suggesting they would not avoid someone with frequent seizures (r = .43) [46]. Despite no direct contact with people with lived experience, there was a sense of increased understanding and appreciation of lived experience. Following an educational video and drama aimed at improving knowledge and reducing stigma towards epilepsy in children aged 9–11 years old in Czechia, the intervention group were more likely to say they would be friends with a person with epilepsy compared to the control group (81–84% vs 59%) [40]. Additionally, one study explored the utility of a live performance to tackle stigma against people with dementia and was performed at several care homes, conferences, and public theatres in Canada [52]. After the performance, one care home staff said “we’re not just caring for bodies but for people, institutions can become very mechanical” (p. 97) and another indicated dedication to behavioural change following the performance saying “I’m going to try living these ideas” (p. 97), which demonstrates the power of the arts to reduce stigma [52].
Of the 21% of studies that involved the co-production of art alongside a person with lived experience, the experience of participants was positive [41–45]. Interestingly, all co-production occurred alongside people with dementia. Co-production activities ranged from 1–12 sessions depending on the study and 80% of co-production studies focused the intervention towards university students. In a creative story telling intervention with medical students and people with dementia in the USA, after four sessions, there were significant improvements in feeling relaxed around people with dementia, no longer feeling afraid of people with dementia, and being familiar with dementia [43]. The students discussed how “None of the worries I had previous to our first day manifested themselves, it was a very fun experience.” (p. 325) and “I think seeing the patients here humanised them… it’s not just slapping a label on a person.” (p. 326) [43]. These findings were similar among another study which involved a single art workshop with medical students and people with dementia where they co-created poetry and compared descriptions of dementia pre- and post- workshop, being “Quiet, reserved, frightened, moody” to “Kind lively, happy, and funny” respectively (p. 5) [42]. One study focussed on the artist’s experience following the co-production of paintings and a dance routine in a single session alongside people with dementia [41]. The artists reported feeling “more comfortable being around people with dementia” (p. 366) and “felt surprised that it was such a positive experience” (p. 366) [41]. Although it can be difficult to untangle whether art or the act of working alongside a person with lived experience drove these findings.
A handful of studies explored the experiences of persons with lived experience in participating in the art intervention, whether they were the audience or were involved in the co-production. In an arial silk performance in Brazil, people with epilepsy felt valued and represented when viewing the performance and related to several scenes [36]. In the co-production of paintings and a dance routine in Canada, people with dementia were able to see dementia in a different light which brought a sense of comfort and reduced internalised stigma [41].
Raising awareness and enhancing knowledge.
Participation in art interventions allows participants to become more familiar with the disorder, whether through watching videos or through creating art alongside with people with lived experience. Enhancing knowledge stood out as a prominent mechanism, particularly using visual and narrative art forms. For example, one study used educational videos and quizzes with students aged 13–19 years old and teachers in Malaysia which led to substantial improvements in knowledge of epilepsy, with knowledge scores increasing from low and moderate respectively to very high [32]. Another study which used comic books to tackle stigma of epilepsy in Ethiopia not only boosted understanding of causes and whether the disorder was contagious, but also improved practical skills, with accurate first-aid responses for seizures rising from 30% to 68% in the questionnaire [37].
The arts were not just effective at improving knowledge but also facilitating an understanding of lived experience. For example, an arts program involving the co-development of visual art projects with undergraduate students and people with dementia in the USA reported positive effects in understanding that people with dementia can enjoy life (r = −.4) and can feel when others are kind to them (r = −.37) [45]. In a movie review of a short film exploring an older couple’s lived experience of dementia tailored for Chinese Americans, one comment read “now I know dementia is not about going crazy” [48]. In another study, Australian children aged 8–10 years old attended three lessons, one to create a painting of a memory, then to learn about dementia, and lastly to recreate the original art through the lens of someone with dementia [53]. The latter artworks were noticeably darker in mood and more abstract in shape which demonstrated an increased awareness and understanding of dementia. These studies exemplify that the arts can be used as a medium to raise awareness of disorders, not just of their existence but also to reframe representations.
Behavioural and emotional impact.
Behavioural and emotional changes were achieved through interventions that developed practical skills and encouraged cognitive reframing. In some studies, the value of art as a tool to tackle stigma lay in its ability to elicit emotional reactions. A range of studies report participants feeling emotional reactions to the art, such as the review of a short film aimed at raising stroke awareness: “the film is very profound, moving, and beautiful.” (Supplementary S3 File) [38]. Storytelling and creative expression initiatives which involved four sessions enabled medical students to adopt a more person-centred approach, with many noting an improved ability to see beyond the diagnosis in clinical environments “Every person is different. So just by saying you have AD that shouldn’t mean you are the same as other people” (p. 326) [43]. Direct engagement with people with lived experience was found to be fun, engaging, exciting, and heartfelt [42,43]. In one study, 6 or 7 art sessions alongside people with dementia led to 56% of participants continuing engagement in some way beyond the initial course either through continuing volunteering post course completion, shifting toward a geriatric focus in clinical work, or integrating the skills learnt into the care of people with dementia in their own families [44]. Quantitative data from another study which involved a county wide awareness campaign in France spanning two months led to a 15% increase in emergency calls for stroke symptoms, demonstrating enhanced public responsiveness [34]. This demonstrated the behavioural and emotional influences of art in addressing stigma, particularly in reference to working directly alongside people with lived experience and in watching short films and performances.
Benefits and challenges to art-based interventions
Some of the reviewed articles indicated facilitators and barriers to the sustainability of arts-based interventions for neurological disorders. A key facilitator was the adaptability of art forms, allowing interventions to accommodate diverse participant needs. For instance, offering varied artistic mediums such as educational videos and storytelling enabled individuals with different learning preferences to engage effectively, promoting sustained interest and reducing stigma [39]. Emotional and social support also played a crucial role, with collaborative art projects helping participants build social connections and reduce feelings of isolation. Involving people with dementia in shared artistic experiences fostered a sense of belonging and mutual understanding [41]. Additionally, interventions that resonated personally with participants enhanced motivation and long-term engagement, where participants expressed feeling valued when their emotions were artistically represented [36]. Only one article explored culturally tailored interventions and found this effectively reduced stigma in specific cultural contexts, with 89% of Chinese American participants reporting shifts in their perceptions of dementia [48]. However, minimal details were reported on what constituted tailoring this intervention for a different culture.
Utilising the arts can provide a vehicle to spread awareness of a disorder. In a study using a short film to promote stroke awareness, one of the movie reviews noted “The very first thing I did after seeing the movie was forward it to my father!” (Supplementary S3 File) [38]. However, certain barriers also impacted the sustainability of these interventions. Physical and cognitive limitations among participants sometimes hindered consistent engagement, particularly in programs with high physical demands [35]. Resource availability emerged as a significant challenge, with limited funding affecting the reach and effectiveness of a stroke awareness campaign in France which used visual arts [34]. The burden on caregivers was another obstacle, where caregivers often struggled to balance their responsibilities, potentially affecting the continuity of interventions [36]. Moreover, measuring the long-term impact of arts-based interventions proved difficult. One study showed that while short films could modify stigma effectively, quantifying their lasting influence on community attitudes remained challenging [48].
Discussions
Key findings
The review found that arts-based interventions effectively contributed to stigma reduction in neurological disorders through three primary mechanisms: shifting attitudes, raising awareness thus enhancing knowledge, and influencing behaviours. Additionally, some studies illustrated that through evoking emotional responses, desirable changes such as improvement of discriminatory attitudes was observed. Knowledge, attitudes and behaviours are widely used constructs of stigma in mental and brain health, but emotions are a less explored construct, yet the findings suggest that they might mediate stigma reduction in some participants. Future studies should explore the role of emotions in imparting change alongside other established constructs of stigma.
Included studies explored art-interventions for reducing stigma in epilepsy, stroke, and dementia. While these are important disorders to address, it is important to consider additional neurological disorders such as Parkinson’s disease and multiple sclerosis that are both highly prevalent and stigmatised [1,17,57]. These disorders can be managed well through appropriate treatment, yet, especially for those living in LMICs countries, stigma acts as a barrier to accessing healthcare [10,58]. This highlights the lack of attention within the current literature and suggests an important gap. Art-based interventions provide a unique opportunity to tackle stigma through fostering public understanding and empathy which may promote early diagnosis and management [5].
The finding on the utility of visual and narrative arts (such as the use of comic books) highlighted potential artistic approaches for tackling stigma among young populations such as school going children, university students and crucial demographics like medical students who eventually become part of healthcare systems. Early intervention has a high potential of bringing sustained positive change but the mechanism through which this change is sustained in unclear [59]. One possible explanation is that early exposure to visual and narrative arts creates an immersive experience delivered through experiential learning which fosters greater empathy than didactic approaches alone [60]. However more robust testing is required across multiple neurological disorders and multiple settings. Secondly, considerations such as cost-effectiveness and potential for scaling up should be made. Digital media, while not providing direct interactions with the public may be a potential platform for scaling up such interventions as they allow for an accessible, cost-effectiveness, and large reaching strategy which can facilitate quick comprehension and retention of critical information [61].
Regarding evaluation of effectiveness of these interventions, most studies used one-off, cross-sectional questionnaires or interviews. Behaviour change is difficult, takes time and can may not be sustained long-term. While a small number of studies followed up participants post-intervention and/or investigated changes to behaviours (primarily through self-reported behaviour questions), overall, the depth of data collected limits the understanding of the influence interventions may have on stigma, and the particular components of the intervention that contributed to reducing stigma. Self-reported responses encourage a social desirability bias leading to responses which may not accurately reflect the behaviours and attitudes of a participant [62]. To capture changes in stigma on a deeper level, methods such as a reflective diary may be more appropriate, as well as longitudinal follow-up.
There was a significant gap in the use of art-based interventions for neurological awareness in LMICs with only two countries in sub-Saharan Africa being represented(Ethiopia and Madagascar). Most of the reviewed studies were conducted in high-income Western countries, with limited representation from South America, Asia, and the Middle East. This is of issue as the need for anti-stigma interventions is higher in these regions [12,13] with LMICs containing the majority of burden from disease within the world [2]. Yet the amount of funding and human resources needed to adequately address healthcare issues brought about by stigma is consistently unmet and undervalued within LMICs. Additionally, this geographical and cultural paucity limits our understanding of contextual factors which could influence the effectiveness of art-based interventions while also highlighting a critical need for expanding art-based interventions to underrepresented regions. For example, a scoping review of art projects in sub-Saharan Africa found a primary focus on HIV and AIDS which has successfully raised awareness and empowered individuals to take control of their own health [63] and these approaches can be extended to brain health. Additionally, limited efforts have been made in tailoring interventions for different cultures with minimal details around how best to ensure the relevancy of art based interventions to different cultural and religious backgrounds.
Strengths and limitations
We used the PRISMA-SR guidelines to undertake this review which ensured methodological rigour and minimised bias. By involving at least two reviewers at both the screening and data extraction stage, the risk of bias was reduced [64,65]. By screening 9,990 articles, this review provides a thorough overview of available literature, however, we acknowledge key information may have been missed from conference abstracts and activities to raise awareness and tackle stigma occurring outside of academic research [66]. Hence, while this review provides a strong overview of available literature, we acknowledge the limitation of being unable to include non-academic art interventions and those without explicit evaluations, such as short films and creative art workshops within communities [67–70]. This review includes studies that possess both a participatory nature, as well as the dissemination of knowledge and experiences through the arts and media. Due to the varying elements within these two approaches, there may be differences in results, however, we have accounted for this by distinguishing between the two during the synthesis of results.
Reporting how gender, intervention length, and cultural context influence the effectiveness of art-based interventions was limited during this review due to the scarcity of literature exploring these topics. Additionally, questions around how stigma interventions interact within the wider context of an individual, such as family members, would provide an opportunity to better understand the spread of awareness raising efforts. To better understand how best to deliver and who best to deliver art interventions to, future art-based interventions tackling stigma should explore different audiences and delivery lengths to improve upon current knowledge.
Conclusion
This review provided a methodologically rigorous overview on the role of art in tackling stigma in neurological disorders. It demonstrated that art-based interventions can be a powerful tool in reducing stigma around neurological disorders, both in terms of raising awareness and shifting attitudes towards neurological disorders. Interventions prioritising the direct interactions between a small number of the public and people with lived experience seems particularly effective at driving meaningful and lasting changes in attitudes.
More robust evidence of effectiveness of these approaches across diverse settings and a diverse range of highly stigmatised disorders such as Parkinson’s disease and multiple sclerosis is required. Lastly, robust and enduring mechanisms of measuring effectiveness of these interventions using mixed methods data and models of how these interventions bring change should be explored.
Supporting information
S1 FileCompleted PRISMA Checklist for the systematic review.(DOCX)
S2 FileSearch Strategy.(DOCX)
S3 FileStandardized data extraction template applied to included studies.(XLSX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Steinmetz JD, Seeher KM, Schiess N, Nichols E, Cao B, Servili C. Global, regional, and national burden of disorders affecting the nervous system, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. The Lancet Neurology. 2024;23(4):344–81.38493795 10.1016/S 1474-4422(24)00038-3PMC 10949203 · doi ↗ · pubmed ↗
- 2World Health Organization. Intersectoral global action plan on epilepsy and other neurological disorders 2022-2031 Geneva. 2023. Available from: https://www.who.int/publications/i/item/978924007662410.1227/neu.000000000000197635383690 · doi ↗ · pubmed ↗
- 3Earnshaw VA, Quinn DM. The impact of stigma in healthcare on people living with chronic illnesses. J Health Psychol. 2012;17(2):157–68. doi: 10.1177/1359105311414952 21799078 PMC 8919040 · doi ↗ · pubmed ↗
- 4Corrigan PW, Watson AC. Understanding the impact of stigma on people with mental illness. World Psychiatry. 2002;1(1):16–20. 16946807 PMC 1489832 · pubmed ↗
- 5Scambler G. Health-related stigma. Sociol Health Illn. 2009;31(3):441–55. doi: 10.1111/j.1467-9566.2009.01161.x 19366430 · doi ↗ · pubmed ↗
- 6Hatzenbuehler ML, Link BG. Introduction to the special issue on structural stigma and health. Soc Sci Med. 2014;103:1–6. doi: 10.1016/j.socscimed.2013.12.017 24445152 · doi ↗ · pubmed ↗
- 7Majeed T, Hopkin G, Wang K, Nepal S, Votruba N, Gronholm P, et al. Anti-stigma interventions in low-income and middle-income countries: a systematic review. E Clinical Medicine. 2024;72:102612. doi: 10.1016/j.eclinm.2024.102612 38707913 PMC 11066569 · doi ↗ · pubmed ↗
- 8Ju HJ, Harley D, Miller-Rankin J. Manifestations of public and self-stigma of physical disability: A scoping review in rehabilitation and disability research. Sgrjarc. 3:178–99.