Prognostic Impact of Nutritional Status in Patients with Candidemia
Nobuhiro Asai, Wataru Ohashi, Yuichi Shibata, Daisuke Sakanashi, Hideo Kato, Mao Hagihara, Hiroshige Mikamo

TL;DR
This study shows that the CONUT score is a better predictor of mortality in patients with candidemia compared to other nutritional assessment tools.
Contribution
The study identifies the CONUT score as a more reliable nutritional assessment tool for predicting mortality in candidemia patients.
Findings
The CONUT score had good prognostic performance for 30-day mortality with an optimal cut-off of 12.
Higher CONUT scores were associated with significantly shorter overall survival in candidemia patients.
CONUT score ≥ 12 was an independent predictor of 30-day mortality, unlike the GLIM criteria.
Abstract
Background: Candidemia remains a life-threatening infection with high mortality despite advances in antifungal therapy. Malnutrition has been suggested as an important contributor to poor outcomes; however, the prognostic value of different nutritional assessment tools in candidemia has not been fully clarified. This study aimed to evaluate the impact of nutritional status on prognosis in patients with candidemia and to identify the most reliable nutritional assessment tool. Method: We conducted a retrospective cohort study of adult patients diagnosed with candidemia at a tertiary teaching hospital in Japan between 2014 and 2024. A total of 170 patients were included, with a mean age of 73 years. Nutritional status was assessed using the Global Leadership Initiative on Malnutrition (GLIM) criteria and Controlling Nutritional Status (CONUT) score. The primary outcome was 30-day…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
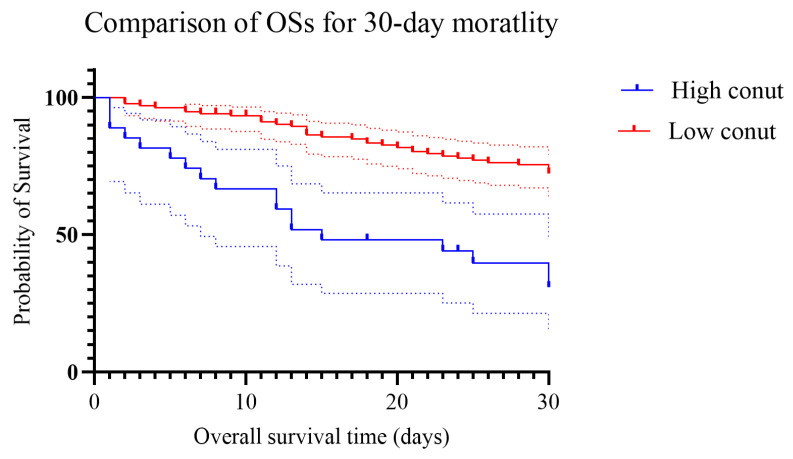 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Immunodeficiency and Autoimmune Disorders · Cystic Fibrosis Research Advances
1. Introduction
Despite significant advances in diagnostic methods and antifungal therapies, candidemia remains a major clinical challenge due to its persistently high mortality rate of 30–60% [1,2,3]. Candidemia, a bloodstream infection caused by Candida species, typically arises when the normal mucosal or skin barriers are breached, allowing the translocation of Candida from colonized sites into the bloodstream. This process is often facilitated by factors such as the presence of central venous catheters, use of broad-spectrum antibiotics that disrupt the normal microbiota, immunosuppression, surgical procedures, and prolonged hospitalization, particularly in intensive care units [4].
Under normal conditions, host defenses—including intact epithelial barriers, neutrophil function, and innate immune responses—are critical in preventing fungal invasion. However, when these defenses are compromised, Candida can enter the bloodstream and disseminate to various organs, leading to life-threatening systemic infection [4]. Malnutrition has been increasingly recognized as a significant risk factor that contributes to the development and progression of candidemia [5,6]. Protein–energy malnutrition impairs both innate and adaptive immunity, reducing phagocytic activity, cytokine production, and mucosal integrity. Additionally, low serum albumin levels, which are often used as markers of nutritional status, are associated with increased vascular permeability and poor wound healing, further facilitating microbial invasion and translocation. Furthermore, malnourished patients—especially those with chronic illnesses or frailty—often require invasive medical interventions such as feeding tubes or central venous catheters, which themselves are known risk factors for candidemia. Therefore, malnutrition may play both a direct and indirect role in the pathogenesis of candidemia by weakening host defenses and increasing exposure to procedural risks. Recently, several nutritional tools have been used to assess patients’ conditions in general medical settings, such as Global Leadership Initiative on Malnutrition (GLIM) criteria [7], Controlled Nutritional Status (CONUT) score [8], Prognostic Nutritional Index (PNI) [9], and Geriatric Nutritional Risk Index (GNRI) [10]. However, it remains unclear whether these nutritional tools can forecast outcomes in candidemia. While factors such as advanced age, immunosuppression, Acute Physiology, Age, Chronic Health Evaluation II (APACHE II), and Sequential Organ Failure Assessment (SOFA) scores have been well established as predictors of poor outcomes, the prognostic significance of malnutrition in candidemia has yet to be fully elucidated. Therefore, we conducted this retrospective study to investigate whether nutritional assessment tools can predict outcomes in candidemia patients, and to determine which tools most accurately reflect prognosis.
2. Materials and Methods
2.1. Study Design and Patient Enrollment
This retrospective study was conducted at our institute, a tertiary teaching hospital with 800 beds located in a rural area of Aichi Prefecture, Japan. The objective was to identify which nutritional assessment tools best predict the prognosis of candidemia between 2014 and 2024.
We included patients aged ≥16 years who were diagnosed with candidemia at our institution. Candidemia was defined as the presence of at least one positive blood culture for Candida species, in accordance with previous studies [11]. Patients were excluded if clinical data were insufficient or if follow-up was not possible due to transfer to another medical facility.
This study was approved by the Institutional Review Board of Aichi Medical University Hospital (Approval No. 2025-040).
2.2. Patient Characteristics and Disease Severity
A total of 170 patients with candidemia were enrolled in the study. We evaluated patients’ characteristics including age, sex, underlying diseases, and nutritional status. Clinical outcomes such as initial antifungal therapy, duration of hospitalization, and treatment regimens were also assessed.
Disease severity was evaluated using the Systemic Inflammatory Response Syndrome (SIRS), quick Sequential Organ Failure Assessment (qSOFA), and SOFA scores. Adherence to the candidemia management bundle was assessed using the European Confederation of Medical Mycology Quality of Clinical Candidemia Management (EQUAL) Candida score [11,12]. The EQUAL Candida Score is a quality-of-care scoring system developed by the European Confederation of Medical Mycology. It measures adherence to guideline-recommended management of candidemia and invasive candidiasis. The score assigns points to key diagnostic, therapeutic, and follow-up interventions. In patients with a central venous catheter (CVC), the maximum score is 22 points, whereas in patients without a CVC, the maximum score is 19 points, because catheter removal cannot be assessed. Higher scores indicate better adherence to recommended management strategies. The score is primarily used for quality assessment and antifungal stewardship rather than for individual risk prediction [11,12].
Nutritional status was evaluated based on the GLIM criteria [7], CONUT score [8], PNI [9], and Geriatric Nutritional Risk Index (GNRI). A comparison of these nutritional indices is presented in Supplemental Table S1. Underlying comorbidities were assessed using the Charlson Comorbidity Index (CCI). Disseminated intravascular coagulation (DIC) was diagnosed using the Japanese Association for Acute Medicine (JAAM) DIC criteria [13]. Septic shock was defined as a systolic blood pressure <90 mmHg or the requirement for vasopressor support, in line with previous definitions [11].
2.3. Data Collection
We collected demographic and clinical data, including age, sex, underlying conditions, use of immunosuppressive agents, known risk factors for candidemia [14,15,16,17], and the infection source. Laboratory data were obtained on the day a positive blood culture was collected. Additionally, 30-day mortality, in-hospital mortality, and the date of last follow-up were recorded to calculate overall survival (OS). The EQUAL Candida score was assessed for each patient throughout the study period.
2.4. Microbiological Evaluation
Candida species were identified using the VITEK-MS system (bioMérieux, Marcy-l’Étoile, France). Antifungal susceptibility testing for amphotericin B, caspofungin, fluconazole, itraconazole, and voriconazole was conducted using the VITEK-2 AST-YS07 card (bioMérieux). Minimum inhibitory concentrations (MICs) were interpreted according to Clinical and Laboratory Standards Institute (CLSI) guidelines [18,19], using species-specific breakpoints for caspofungin (CPFG), fluconazole (FLCZ), itraconazole (ITCZ; for C. albicans), and voriconazole (VRCZ) [19]. Susceptibility to amphotericin B (AMB) and liposomal amphotericin B (L-AMB) was interpreted based on species-specific breakpoints established by the European Committee on Antimicrobial Susceptibility Testing (EUCAST), in accordance with prior studies [18].
2.5. Statistical Analyses
Categorical variables are presented as percentages, and continuous variables as mean ± standard deviation (SD). The Chi-square or Fisher’s exact test (two-tailed) was used for categorical variables, while the unpaired Student’s t-test or the Mann–Whitney U test was applied for continuous variables. Variables with a p-value < 0.10 in univariate analysis were included in multivariate models. Multivariate analysis was adjusted for potential confounders previously reported [14,15,16,17]. All statistical analyses were performed using SPSS version 26 for Windows (SPSS Inc., Chicago, IL, USA). Kaplan–Meier survival curves were generated using GraphPad Prism version 10. Overall survival (OS) was defined as the time from diagnosis to death from any cause. Comparisons of OS between groups were conducted using the log-rank test. A p-value < 0.05 was considered statistically significant.
3. Results
Table 1 shows patient characteristics and clinical outcomes. The mean age was 73 years old [(±standard deviation (SD) 13.7]. They were 108 males (64%) and 62 females (36%). The most frequent infection site was CRBSI in 91 (53%), followed by unknown in 71 (42%). As for nutritional status, the mean body mass index (BMI) and CONUT score were 19.2 (±3.9) and 9.5 (±2.1), respectively. One hundred twenty-three (72%) and 100 (59%) of the patients were assessed as having moderate and severe malnutrition by the GLIM criteria.
In terms of underlying diseases, malignancy was the most commonly seen in 90 (53%), followed by diabetes mellitus in 50 (29%). The mean CCI score was 3.7 ± 2.5. Candida spp. Isolated was 176 isolates from 170 patients. Candida albicans was most frequently seen in 78 (46%), followed by C. parapsilosis in 43 (25%). The mean EQUAR Candida scores in the patients with and without CVC were 13.7 and 11.7, respectively.
Regarding clinical course and outcomes, the median duration from hospital admission to the diagnosis of candidemia was 22 days (range 0–197). Echinocandin was the most frequently used in 118 (69%) as the initial antifungal therapy. The 30-day and in-hospital mortality were 35% and 44%, respectively.
3.1. Receiver Operating Characteristic (ROC) Curves of CONUT Score for 30-Day
Area under the Receiver operating characteristic (AUROC) of CONUT score for 30-day mortality was 0.723 [95% confidence interval (CI) 0.645–0.801, p < 0.001].
3.2. Prognostic Accuracy of CONUT Score for 30-Day Mortality
Table 2 shows the prognostic accuracy of CONUT score for predicting 30-day mortality. The appropriate cut-off for the CONUT score was 12 and was chosen based on the Youden Index [20].
3.3. Comparison of Overall Survival Time Between CONUT Score ≥12 and <12
We compared the OSs between those with the CONUT score ≥12 and <12. Patients with the CONUT score ≥12 had shorter OSs than those with the CONUT score <12 as shown in Figure 1 (Log-Rank test p < 0.001).
3.4. Univariate and Multivariate Analyses of 30-Day Mortality Among Candidemia Patients
Compared with the survival group, the death group had higher CONUT scores (>12), SOFA scores (>5), Charlson Comorbidity Index (CCI) scores (>3), and EQUAL Candida scores (>10), all of which were associated with 30-day mortality in patients with candidemia (Table 1). Among these variables, multivariate Cox proportional hazards analysis identified a higher CONUT score (≥12) and a higher SOFA score (≥5) as independent poor prognostic factors for 30-day mortality, whereas a higher EQUAL Candida score (≥10) was identified as an independent favorable prognostic factor (Table 3).
4. Discussion
In the present study, 72% of patients were classified as malnourished according to the GLIM criteria. It is reasonable that candidemia frequently develops in immunocompromised patients, regardless of the underlying cause. We found that malnutrition defined by the GLIM criteria failed to predict the 30-day mortality rate in patients with candidemia, whereas the CONUT score did so successfully. This discrepancy between the two nutritional assessment tools may be attributed to their distinct characteristics. The CONUT score includes acute inflammatory markers such as serum albumin levels and lymphocyte counts, whereas the GLIM criteria primarily reflect chronic nutritional status rather than inflammation-related changes. Because candidemia is a critical infection with a high mortality rate, chronic indicators like the GLIM criteria may not accurately assess short-term outcomes in these patients. Previous studies have also reported that the CONUT score predicted outcomes in patients with infective endocarditis [21,22] and pleural infections [23]. As these conditions similarly carry poor prognoses, the ability of CONUT to reflect inflammation-related physiological deterioration may explain its superior prognostic performance in severe infections.
The lack of prognostic significance of malnutrition defined by the GLIM criteria may be explained by several pathophysiological mechanisms specific to acute, life-threatening infections such as candidemia. The GLIM criteria were developed to diagnose malnutrition based on relatively stable phenotypic indicators (e.g., weight loss, low body mass index, and reduced muscle mass) combined with etiologic factors such as reduced intake or chronic inflammation. These components are well suited to identifying long-term nutritional deficits but are less sensitive to rapid physiological changes driven by acute systemic inflammation [24,25].
Candidemia induces a profound inflammatory response characterized by cytokine release, endothelial dysfunction, capillary leakage, and metabolic dysregulation. During this acute phase, serum protein levels, immune cell counts, and metabolic markers change rapidly, often independent of baseline nutritional reserves. For example, acute-phase reactions suppress albumin synthesis and promote lymphocyte apoptosis or redistribution, leading to transient hypoalbuminemia and lymphopenia. These alterations are strongly associated with disease severity and short-term mortality but are not captured by the GLIM framework, which intentionally excludes laboratory biomarkers to avoid confounding by inflammation [26,27]. Moreover, body weight and body mass index—key phenotypic components of GLIM—may be misleading in critically ill patients. Fluid resuscitation, edema, ascites, or third spacing frequently observed in candidemia can mask true body composition and result in inaccurate assessment of nutritional status. Similarly, the evaluation of muscle mass is often impractical or unavailable in the acute care setting, further limiting the applicability of GLIM in critically ill patients. In contrast, the CONUT score incorporates laboratory parameters that dynamically reflect acute inflammatory burden, immune competence, and metabolic reserve. Hypoalbuminemia reflects both nutritional depletion and systemic inflammation, lymphopenia indicates impaired cell-mediated immunity against Candida species, and hypocholesterolemia has been associated with adverse outcomes in sepsis due to altered lipid metabolism and impaired endotoxin neutralization. Collectively, these factors may explain why the CONUT score more accurately predicts short-term mortality in candidemia than GLIM-defined malnutrition.
There are several limitations in the study. First, this is a retrospective study in a small population. Second, those without nutritional status were excluded in this study. Then, the population never can reflect all candidemia patients’ results in the real world. There might have been a selection bias. Third, nutritional status was assessed at the time of candidemia diagnosis. Some patients may already have been affected by infection at the time of assessment. Fourth, detailed information regarding the number and duration of prior antibiotic treatments was not consistently available due to the retrospective design of this study, which may have influenced the results.
5. Conclusions
In conclusion, we found that CONUT score could predict the 30-day mortality in candidemia patients, while the GLIM criteria failed. The CONUT score is useful for predicting the 30-day mortality among patients with candidemia.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Toda M. Williams S.R. Berkow E.L. Farley M.M. Harrison L.H. Bonner L. Marceaux K.M. Hollick R. Zhang A.Y. Schaffner W. Population-Based Active Surveillance for Culture-Confirmed Candidemia—Four Sites, United States, 2012–2016 MWR Surveill. Summ.20196811510.15585/mmwr.ss 6808 a 1PMC 677218931557145 · doi ↗ · pubmed ↗
- 2Asai N. Sakanashi D. Suematsu H. Kato H. Hagihara M. Shiota A. Koizumi Y. Yamagishi Y. Mikamo H. To what degree could clinical trials in evidence based medicine reflect reality in the treatment of candidemia?J. Microbiol. Immunol. Infect.20225514715310.1016/j.jmii.2020.11.00333339744 · doi ↗ · pubmed ↗
- 3Bassetti M. Taramasso L. Nicco E. Molinari M.P. Mussap M. Viscoli C. Epidemiology, species distribution, antifungal susceptibility and outcome of nosocomial candidemia in a tertiary care hospital in Italy P Lo S ONE 20116 e 2419810.1371/journal.pone.002419821935385 PMC 3174155 · doi ↗ · pubmed ↗
- 4Song J. Yang X. Liu X. Li J. Gut bacteria: Protective mediators, pathogenic contributors and novel therapeutic targets in Candida albicans infections Gut Pathog.2025177710.1186/s 13099-025-00755-841039491 PMC 12490052 · doi ↗ · pubmed ↗
- 5Lee Y.C. Chen Y.C. Wang J.T. Wang F.D. Hsieh M.H. Hii I.M. Lee Y.L. Ho M.W. Liu C.E. Chen Y.H. Impact of Nutritional Assessment on the Clinical Outcomes of Patients with Non-albicans Candidemia: A Multicenter Study Nutrients 202113321810.3390/nu 1309321834579094 PMC 8465954 · doi ↗ · pubmed ↗
- 6Piazza O. Boccia M.C. Iasiello A. Storti M.P. Tufano R. Triassi M. Candidemia in Intensive Care patients. Risk factors and mortality Minerva Anestesiol.200470636914765046 · pubmed ↗
- 7Cederholm T. Jensen G.L. Correia M. Gonzalez M.C. Fukushima R. Higashiguchi T. Baptista G. Barazzoni R. Blaauw R. Coats A. GLIM criteria for the diagnosis of malnutrition—A consensus report from the global clinical nutrition community Clin. Nutr.2019381910.1016/j.clnu.2018.08.00230181091 · doi ↗ · pubmed ↗
- 8Ignacio de Ulibarri J. Gonzalez-Madrono A. de Villar N.G. Gonzalez P. Gonzalez B. Mancha A. Rodriguez F. Fernandez G. CONUT: A tool for controlling nutritional status. First validation in a hospital population Nutr. Hosp.200520384515762418 · pubmed ↗