Projected Health and Economic Impacts of Achieving the Recommended Dairy Intake in Japan: A Simulation Study of Increased Milk Consumption for Stroke Prevention
Ryota Wakayama, Michihiro Araki, Mieko Nakamura, Nayu Ikeda

TL;DR
Increasing milk consumption in Japan could reduce stroke cases and healthcare costs over 10 years.
Contribution
A simulation study evaluating health and economic impacts of increased milk consumption for stroke prevention in Japan.
Findings
Increasing milk intake to 180 g/day could reduce stroke incidence by 7.0% in an immediate increase scenario.
Healthcare expenditures for stroke could decrease by 5.1% under the immediate increase scenario.
A gradual increase in milk consumption could still reduce stroke-related deaths by 3.2%.
Abstract
Background/Objectives: Milk consumption is inversely associated with stroke risk. However, the average dairy consumption in Japan is below recommended guidelines. Therefore, we aimed to evaluate potential health and economic impacts of increased milk intake to achieve the recommended daily dairy intake for stroke prevention. Methods: A Markov model stratified by sex and age group simulated the effects of achieving the recommended dairy intake—by increasing milk consumption to 180 g/day—on stroke incidence, stroke-related deaths, and national healthcare expenditures among Japanese adults aged 30–79 years over 10 years. Two scenarios were defined; an immediate increase (Scenario 1) and a constant annual growth rate (Scenario 2) in milk intake, whereas the average dairy product consumption in 2023 was maintained in the base-case scenario. Results: Compared with the base-case scenario,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
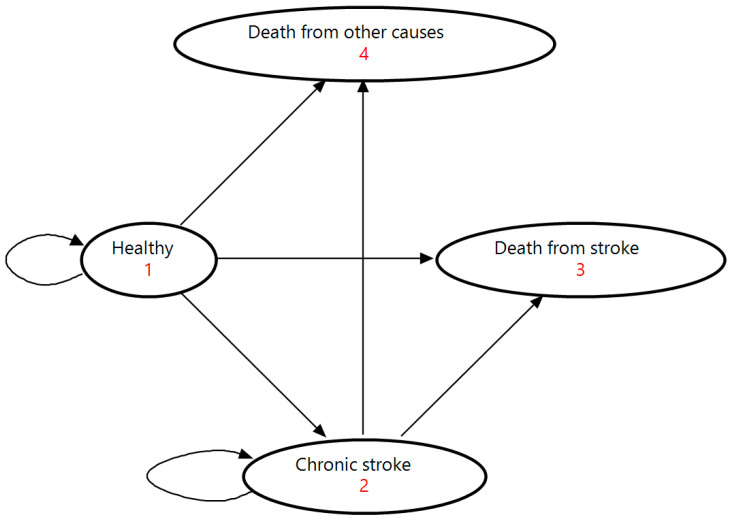 Figure 1
Figure 1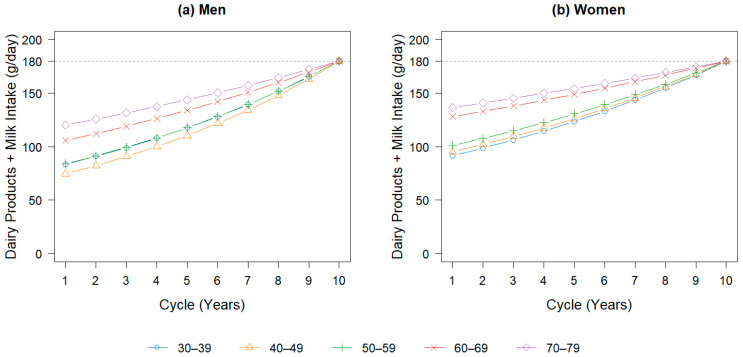 Figure 2
Figure 2- —Ministry of Health, Labour and Welfare
- —Ajinomoto Co., Inc.
- —Ezaki Glico Co., Ltd.
- —Kagome Co., Ltd.
- —Kikkoman Corporation
- —Zensho Holdings Co., Ltd.
- —Nissin Foods Holdings Co., Ltd.
- —Nissui Corporation
- —Meiji Co., Ltd.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNutritional Studies and Diet · Nutrition and Health in Aging · Dietary Effects on Health
1. Introduction
Stroke is a major public health concern in Japan, and the fourth leading cause of death [1]. The annual national healthcare expenditure (NHE) for stroke, including inpatient and outpatient costs, was estimated at approximately 11.6 billion US dollars (USD) in 2023 [2]. Among modifiable risk factors, diet plays a crucial role in stroke prevention. Excessive sodium intake is associated with hypertension, a major risk factor for stroke [3]. In addition, serum cholesterol levels are associated with ischemic and hemorrhagic stroke [4,5], highlighting the importance of a healthy diet.
A healthy diet helps prevent noncommunicable diseases, including stroke [6]. Dairy products are important components of a balanced diet and are recommended in many national dietary guidelines worldwide [7]. The Japanese Food Guide Spinning Top, Japan’s official dietary guideline, recommends two servings (2 SV) of dairy per day [8]. Dairy consumption is associated with reduced risks of type 2 diabetes [9], obesity [10], and hypertension [11]. Among dairy products, milk has been associated with a reduced stroke risk in several meta-analyses [12,13,14,15]. In Japan, daily milk consumption has also been associated with delayed onset and reduced mortality from stroke [16,17]. The recommendation of 2 SV corresponds to approximately 180 g of milk per day [8,18]. Milk is nutrient-dense food and provides multiple micronutrients that influence stroke risk. It is the main dietary source of calcium in Japan [19], which is inversely associated with hypertension [20] and stroke [21,22,23]. Milk also contains potassium and magnesium, which are associated with a lower stroke risk [18,22]. However, the mean milk and total dairy intake among Japanese adults is 61.8 g/day and 108.3 g/day, respectively [19], indicating that overall dairy consumption in Japan may be insufficient.
Given evidence that milk consumption is associated with reduced stroke risk, increasing milk consumption in Japan may be a practical approach to achieve the recommended dairy intake and reduce healthcare costs by reducing stroke incidence and mortality. However, the potential health and economic impacts of meeting the recommended dairy intake through increased milk consumption remain unclear. Therefore, we aimed to develop a simulation model to estimate the health and economic impacts of increased milk consumption to achieve the recommended daily dairy intake for stroke prevention in the Japanese population.
2. Materials and Methods
2.1. Modeling Framework
To evaluate the health and economic impacts of achieving the recommended dairy intake through increased milk consumption, we focused on stroke incidence, stroke-related deaths, and NHE in Japan. Based on data availability, the scope of this study was limited to total stroke, including subarachnoid hemorrhage, intracerebral hemorrhage, and cerebral infarction.
We developed a Markov cohort simulation model using TreeAge Pro Healthcare 2024 (TreeAge Software, Williamstown, MA, USA) to model transitions between multiple health states over time [24]. A closed cohort of Japanese individuals aged 30–79 years in 2023 was simulated over a 10-year period (2023–2032), with each cycle representing 1 year. We focused on adults aged ≥30 years because individuals in this age group account for >95% of stroke cases in Japan, whereas the incidence among those aged <30 years is relatively low [25,26]. This simulation period was set to 10 years to minimize the influence of long-term societal changes and ensure the robustness of the results.
In this study, a Markov model stratified by sex and 10-year age group (30–39, 40–49, 50–59, 60–69, and 70–79 years) was constructed. The model included four mutually exclusive health states: “Healthy” “Chronic stroke,” “Death from stroke,” and “Death from other causes” (Figure 1). The “Healthy” state represented individuals who had never experienced a stroke, while the “Chronic stroke” state included those who had survived a stroke. “Death from stroke” referred to individuals who died from stroke, and “Death from other causes” included deaths unrelated to stroke. The acute phase of stroke was not modeled as a separate state but was incorporated into transitions at stroke onset because its duration was shorter than the 1-year simulation cycle.
At the start of the Markov simulation, the Japanese population was stratified into “Healthy” and “Chronic stroke” states based on the prevalence rates of stroke. The number of individuals initially assigned to the “Death from stroke” and “Death from other causes” states was set to zero. During each cycle, individuals in each cohort transitioned between the four health states according to the predefined transition probabilities. Individuals in the “Healthy” state could: (1) remain in the “Healthy” state; (2) experience the first incidence of stroke and survive, transitioning to the “Chronic stroke” state; (3) experience the first incidence of stroke and die during the acute phase (within 28 days), transitioning to the “Death from stroke” state; or (4) die from other causes, transitioning to the “Death from other causes” state. Individuals in the “Chronic stroke” state could: (1) remain in the “Chronic stroke” state without recurrence; (2) experience a recurrent stroke and survive, remaining in the “Chronic stroke” state; (3) experience a recurrent stroke and die during the acute phase, transitioning to the “Death from stroke” state; or (4) die from other causes, transitioning to the “Death from other causes” state. All transitions between the health states were assumed to be irreversible.
2.2. Scenarios
In this study, we modeled intervention scenarios in which the recommended dairy intake of 2 SV per day was achieved solely through increased milk consumption. In the guideline, a 180 mL milk bottle was used as a practical example. One serving of dairy contains approximately 100 mg of calcium from milk or dairy products. According to the Standard Tables of Food Composition in Japan (2020 edition), 100 g of milk contains 110 mg of calcium [18]; therefore, 180 g of milk provides approximately 200 mg of calcium, equivalent to the recommended intake of 2 SV. In addition, milk contains other micronutrients relevant to stroke prevention, including potassium and magnesium. Therefore, the target milk intake was set at 180 g/day.
To reach the target milk intake, two intervention scenarios were defined. In Scenario 1, milk consumption increased immediately to 180 g/day for all age-sex groups. In Scenario 2, milk intake increased gradually over 10 years, reaching 180 g/day by the end of the simulation period for each age-sex group (Figure 2). The base-case scenario assumed that the average dairy consumption by sex and age remained at the 2023 level throughout the simulation period.
Health and economic impacts were evaluated by comparing the projected stroke incidence, stroke-related mortality, and NHE across the base-case and intervention scenarios. In both intervention scenarios, the milk-specific dose-response relative risk for stroke was applied only to the group with incremental milk intake above the baseline average dairy consumption. Net impacts were calculated as the difference between base-case and intervention estimates. Therefore, the estimates reflect only the impacts of increased milk intake and vary according to the baseline gap between current and target dairy intake for each age-sex group.
2.3. Input Parameters
For all input parameters, the most recent data available from public databases and peer-reviewed literature as of July 2025 were used as baseline data (Table 1). Age- and sex-specific input parameters are presented in Table 2. For baseline data not available by age group, the 28-day acute fatality rates of stroke were set at 14.9% and 15.7% for men and women, respectively, and recurrence rates were set at 28.2% for men and 24.8% for women [27,28]. The relative risk of stroke per 200 g of milk intake among Asian population was 0.82 (95% confidence interval [CI]: 0.75–0.90) for both sexes [13].
The probability of transitioning between health states was determined using stroke prevalence and incidence rates, stroke-specific and all-cause mortality rates, 28-day acute fatality rates, recurrence rates, and the relative risk of stroke associated with milk intake. The probability of transitioning from the “Healthy” to “Chronic stroke” state was calculated as the product of stroke incidence rates and relative risk associated with milk intake. For individuals in the “Chronic stroke” state, the recurrence rate of stroke was assumed to be constant, regardless of the number of prior events. Similarly, the probability of transitioning from the “Chronic stroke” to “Death from stroke” state was based on a uniform 28-day acute fatality rate, regardless of whether the stroke was an initial or recurrent event. The probability of transitioning from the “Healthy” to “Death from other causes” state was calculated by subtracting stroke mortality rates from all-cause mortality rates.
Stroke-related medical costs included inpatient care, outpatient care, and prescription drug costs (Table 3). Inpatient care costs were assigned to stroke onset events, regardless of whether the stroke was initial or recurrent. Outpatient care and prescription drug costs were assigned to individuals remaining in the “Chronic stroke” state. Prescription drug costs related to stroke were estimated by multiplying the total cardiovascular-related prescription drug costs by the ratio of stroke prevalence to cardiovascular disease prevalence.
NHEs were converted from Japanese yen (JPY) to USD using the average annual exchange rate for 2024 published by the International Monetary Fund (1 USD = 156.65 JPY) [33]. In accordance with economic evaluation guidelines in Japan, 2% annual discount rate was applied to the NHE [34].
2.4. Sensitivity Analysis
We performed deterministic one-way sensitivity analyses to examine the impact of parameter uncertainty on the simulation results. The parameters examined included stroke incidence, prevalence, and mortality rates, all-cause mortality rates, the relative risk of stroke associated with milk intake, and the discount rate. Uncertainty in stroke-related parameters was assessed using their respective 95% CIs around the baseline values (Table 2). The discount rate was varied from 0–4%, in accordance with the Japanese economic evaluation guidelines [34].
3. Results
3.1. Projected Stroke Incidence, Mortality, and NHE Under the Base-Case Scenario
Table 4 presents the projected 10-year cumulative stroke incidence, stroke-related deaths, and NHE under the base-case scenario, assuming the 2023 average daily dairy product intake remained constant. In this scenario, a cumulative total of 1,759,971 stroke cases (2.2% of the total population: 1,096,425 cases among men and 663,546 among women) were projected. Stroke-related deaths were estimated at 267,544 (0.3% of the total population: 163,367 among men and 104,177 among women). The cumulative NHE for stroke was projected to reach USD 51,107,100,072 (USD 30,488,722,609 among men and USD 20,618,377,463 among women). Men exhibited a higher stroke incidence, stroke-related mortality, and NHE than women across all age groups. Projections for stroke cases, stroke-related deaths, and NHE for stroke were highest for the 70–79-year age group for both men and women.
3.2. Projected Stroke Cases and Mortality Under Scenarios of Increased Milk Intake to Achieve the Recommended Dairy Intake
Table 5 presents the projected 10-year cumulative numbers of stroke cases and stroke-related deaths preventable by achieving the recommended dairy intake through increased milk consumption, compared with those for the base-case scenario. In Scenario 1, in which milk consumption increased immediately to the target level, 123,618 stroke cases were projected to be prevented over 10 years (a 7.0% reduction; 85,864 among men and 37,754 among women), along with 18,721 stroke-related deaths (a 7.0% reduction; 12,794 among men and 5927 among women). In Scenario 2, in which milk consumption increased gradually each year to reach the target level over 10 years for each age-sex group, 56,480 cases were projected to be prevented (a 3.2% reduction; 38,788 among men and 17,692 among women), along with 8557 stroke-related deaths (a 3.2% reduction; 5779 among men and 2778 among women). In both scenarios, the numbers of prevented stroke cases and deaths were consistently higher for men than for women across all age groups. The highest numbers of prevented stroke cases and deaths were projected in the 70–79-year age group for both sexes, with the largest percentage reductions in the 40–49-year age group among men and the 30–39-year age group among women.
3.3. Projected NHE Under Scenarios of Increased Milk Intake to Achieve the Recommended Dairy Intake
Table 6 presents the projected cumulative NHE for stroke that could be saved over 10 years by achieving the recommended dairy intake through increased milk consumption, compared with the base-case scenario. In Scenario 1, the cumulative reduction in NHE was estimated at USD 2,598,230,462, corresponding to a 5.1% reduction (USD 1,742,238,244 for men and USD 855,992,218 for women). In Scenario 2, the cumulative reduction was estimated at USD 1,120,633,534, a 2.2% reduction (USD 741,423,469 for men and USD 379,210,065 for women). In both scenarios, the reduction in NHE was consistently greater among men than among women across all age groups. The largest absolute reduction in NHE was projected in the 70–79-year age group for both sexes, with the highest percentage decrease in the 40–49-year age group.
3.4. Sensitivity Analyses
The results of the one-way sensitivity analyses are presented in Table 7. In both scenarios, the largest source of uncertainty in the simulation results was the relative risk of stroke associated with milk intake. The range of cumulative NHE savings due to uncertainty in the relative risk was USD 2,300,333,792 and USD 1,005,552,453 in Scenarios 1 and 2. Conversely, in both scenarios, the smallest sources of uncertainty differed by sex: stroke mortality rates for men and all-cause mortality rates for women.
4. Discussion
We investigated the health and economic impacts of achieving the recommended dairy intake—through milk consumption—on stroke in the Japanese population aged 30–79 years. Attaining the recommended dairy intake of 2 SV by increasing milk consumption to 180 g/day was projected to reduce stroke incidence by 2.1–10.6%, stroke-related mortality by 2.1–10.6%, and stroke-related NHE by 1.5–8.5% over a 10-year period compared with the status quo of consumption levels in 2023.
In two intervention scenarios, the largest absolute reduction in NHE for stroke was projected in the 70–79-year age group. However, the percentage reduction in stroke-related NHE was higher in the 30–59-year age groups than in the 60–79-year age groups for both men and women. This pattern may reflect a low baseline dairy product consumption among younger adults, leading to a larger relative impact of increased intake. In contrast, the absolute reduction in NHE was smaller in younger age groups than in older age groups because NHE for stroke increases with age. In addition, in both intervention scenarios, men consistently had higher cumulative incidences of stroke, stroke-related deaths, and NHE than women across all age groups. This difference may be attributable to the higher baseline dairy product intake among women.
Although the Japanese Food Guide Spinning Top recommends 2 SV of total dairy products per day, we focused specifically on milk as the intervention approach. We modeled the achievement of the recommended dairy intake solely through increased milk consumption for two reasons. First, dose-response meta-analyses show that milk is the only dairy subtype with a clear and statistically significant inverse association with stroke risk, particularly in East Asian populations, whereas total dairy, yogurt, and butter show no significant associations and cheese shows only marginal effects [13]. Second, milk accounts for the majority of dairy intake in Japan, making it the most appropriate component for modelling increases in total dairy intake [19]. Therefore, milk was used as the primary approach to achieve the recommended dairy intake in the intervention scenarios.
The beneficial effects of increased milk consumption on stroke can be explained by several mechanisms. Hypertension is a major risk factor for stroke, and a reduction in systolic blood pressure (SBP) of 5 mmHg is associated with a 29% lower risk of stroke [35]. Dairy intake reduces SBP (−0.11 mmHg per 55 g of dairy) [36] and the risk of hypertension (relative risk, 0.96 per 200 g of milk) [37]. In the Japanese population, characterized by relatively high sodium intake and low dairy consumption, dairy intake has been inversely associated with SBP and hypertension risk [38]. Milk is rich in calcium (110 mg per 100 g) [18]. Calcium intake is associated with reduced SBP [39] and hypertension risk (relative risk, 0.93/500 mg) [20] through mechanisms involving parathyroid hormone regulation [40] and vascular structure [41]. Moreover, calcium intake, particularly from dairy products, is inversely associated with stroke risk [21,22,23], including in Asian populations [23]. In addition to calcium, milk contains potassium (150 mg/100 g) and magnesium (10 mg/100 g) [18], which reduce blood pressure [42,43] and are associated with decreased stroke risk [22]. Milk proteins and bioactive peptides also exert antihypertensive effects [44,45], suggesting that these micronutrients jointly contribute to a lower stroke risk.
In addition to blood pressure control, which is mediated by minerals and proteins, saturated fatty acids (SFAs) in milk may also affect stroke risk. Milk contains 2.33 g of SFAs per 100 g [18]. SFAs can increase serum cholesterol levels [46,47], a risk factor for stroke [5], leading the World Health Organization to recommend limiting SFA intake to <10% of total energy intake [48]. Accordingly, the Dietary Reference Intake for Japanese includes dietary goals for SFAs [3], and several Japanese nutrient profiling systems for processed foods classify SFAs as nutrients to limit [49,50,51,52]. However, mean SFA intake among the Japanese population remains <10% of total energy intake [3]; even with milk consumption increased to 180 g/day, SFA intake would not exceed this threshold. Notably, low serum cholesterol levels are inversely associated with stroke risk in Japan [53], and some studies have reported an inverse association between SFA intake and stroke incidence [54,55,56]. Therefore, while excessive milk consumption could increase the intake of nutrients to limit, moderate milk consumption is likely to confer favorable impacts on stroke.
According to the 2023 National Health and Nutrition Survey of Japan, the mean dairy product intake among individuals aged 30–79 years ranged 74.5–136.7 g/day (Table 2), while the mean milk intake ranged 34.8–82.6 g/day [19]. Consistent with these estimates, the milk shipment volume in 2023 totaled 3,211,400 kL, corresponding to an estimated per capita consumption of 71.1 mL/day (73.2 g/day, assuming a milk density of 1.03 g/mL) [57]. The median dairy product intake reported in the same survey ranged 13.5–106.0 g/day for individuals aged 30–79 years, indicating a highly skewed distribution of dairy consumption in Japan, with a substantial proportion of the population consuming little or no milk. When the simulation was conducted under the assumption of median dairy product intake, the maximum potential reduction in stroke-related NHE was estimated to be USD 4,052,321,603, corresponding to a 7.9% reduction compared with the base-case scenario, with reductions of USD 2,693,458,208 and USD 1,358,863,395 for men and women, respectively.
Long-term caregiving costs could not be incorporated into the simulation model owing to insufficient data. Including these costs would likely reveal greater health and economic impacts than those estimated in this study. Stroke is the second leading reason for long-term caregiving in Japan, accounting for 16.1% of all cases requiring caregiving [58]. Stroke onset often limits in activities of daily living and reduces patients’ quality of life [59,60]. Therefore, reducing the risk of stroke among community-dwelling individuals could lower the risk of requiring long-term care and improve quality of life and life satisfaction across the life course. Increased milk consumption is associated with improved cognitive outcomes following stroke-related cognitive decline [61,62], representing another mechanism through which reducing stroke incidence by increasing milk intake may contribute to lowering long-term caregiving expenditures and alleviating the burden on healthcare resources. Milk shipment volumes in Japan have declined over the past decade [57]; however, promoting milk consumption could be a cost-effective strategy for improving public health and curbing NHE in Japan.
Support from policymakers and food manufacturers may be necessary to increase milk consumption among the Japanese population. Based on the shipment volume and total sales (USD 3.86 billion) in 2023 [57], the average retail price of milk is estimated at approximately USD 0.12 per 100 g. Applying this price to the gap between current consumption and the recommended level, the additional cost corresponds to approximately USD 0.05–0.12 per person per day, depending on sex and age group. In this context, promoting higher milk consumption may require a combination of subsidies, nutrition education, and improvements in the food environment.
Incorporating dairy products into the Japanese diet as part of diverse foods may have important implications for improving dietary quality and health economics in Japan [63,64,65]. For instance, adequate yogurt intake has been projected to provide health economic benefits through the prevention of type 2 diabetes [66]. Blood pressure control through dietary salt reduction has been actively promoted as a strategy to prevent cardiovascular diseases under “Health Japan 21 (the third term)” [67]; however, average salt intake has remained stable over the past 10 years [19]. Including milk, which provides potassium, in the diet could reduce the sodium-to-potassium ratio and potentially attenuate the unfavorable effects of high sodium intake. The Japanese Food Guide Spinning Top recommends dairy intake as part of a balanced diet [8], and adherence to this guideline has been associated with improved dietary quality and a lower risk of cerebrovascular disease [68]. Moreover, a new dietary approach, “New Washoku,” which incorporates the umami of dairy products into traditional Japanese diets, has been proposed to promote sodium reduction without compromising taste [69]. Collectively, these approaches suggest that integrating dairy products, particularly milk, into traditional Japanese diets could enhance dietary health while offering potential economic savings in healthcare without sacrificing dietary preferences.
This study had some limitations. First, milk type was not considered in the simulation model because the National Health and Nutrition Survey of Japan does not provide consumption data by type. Based on shipment volume data, 76.6% of milk products in Japan are regular (unmodified) milk [57]. Previous research has indicated that the relative risk of stroke differs by milk type (0.96/200 g for low-fat milk and 1.03/200 g for high-fat milk) [13]. Thus, the estimated health and economic impacts may vary depending on the type of milk consumed. Future research utilizing milk-type-specific data or stratified relative risks will help generate more robust and scientifically detailed estimates. Second, the simulation model did not differentiate between stroke subtypes and applied a uniform relative risk across all subtypes. Previous studies have reported subtype-specific relative risks per 200 g for stroke in global populations: 0.95 (95% CI, 0.89–1.01) for ischemic stroke, 0.90 (95% CI, 0.74–1.09) for hemorrhagic stroke, and 0.88 (95% CI, 0.81–0.96) for fatal stroke [13]. However, subtype-specific data for East Asian populations are limited, and assuming a uniform relative risk may over- or underestimate impacts for specific subtypes. In addition, it may not extend to strokes attributable to specific etiologies that are more common at younger ages in Japan, such as moyamoya disease. Subtype-specific analyses could enhance the precision of future health and economic impact estimates. Third, because our Markov model used population-level relative risks that were not stratified by menopausal or hormonal status, we could not assess whether the protective association of milk consumption with stroke differs in post-menopausal women. Given that hormonal status influences calcium metabolism and vascular physiology, subgroup-specific analyses may provide more precise estimates in future research. Fourth, the simulation did not include the costs required to achieve increased milk consumption. Although the current analysis reflects only potential healthcare savings and does not constitute a full cost-effectiveness evaluation, increasing population-level milk consumption would require programmatic and structural investments, such as policy support and collaboration with policymakers and food manufacturers. These implementation costs could partially offset the savings estimated in our model. Fifth, this study focused on Japanese individuals aged 30–79 years and assumed a 10-year time horizon without accounting for changes in population structure. Therefore, the findings are specific to the assumptions and scope of the analysis. Finally, long-term care expenditures, which are substantial in aging societies, could not be included due to the lack of appropriate data. Incorporating long-term care expenditures in future analyses would allow for a more comprehensive assessment of the societal and economic impacts by achieving the recommended dairy intake through increased milk consumption.
5. Conclusions
In this 10-year Markov cohort simulation of Japanese adults aged 30–79 years, increasing milk intake to 180 g/day, corresponding to the recommended dairy intake in Japan, was associated with 7.0% reductions in both stroke incidence and stroke-related mortality, as well as a 5.1% reduction in NHE. Public health institutions may facilitate this through nutrition education, subsidies, and improvements in the food environment. These findings suggest that promoting the recommended dairy intake through milk consumption may help prevent stroke while alleviating the economic burden on the healthcare system. The study provides evidence to inform future public health strategies that emphasize the health and economic advantages of adhering to dietary recommendations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ministry of Health, Labour and Welfare Vital Statistics 2024 Available online: https://www.mhlw.go.jp/toukei/list/81-1.html(accessed on 30 September 2025)
- 2Ministry of Health, Labour and Welfare Estimates of National Medical Care Expenditure 2023 Available online: https://www.mhlw.go.jp/toukei/saikin/hw/k-iryohi/23/dl/R 05data.pdf(accessed on 24 December 2025)
- 3Ministry of Health, Labour and Welfare, Japan The Dietary Reference Intakes for Japanese 2025 Available online: https://www.mhlw.go.jp/stf/newpage_44138.html(accessed on 24 September 2025)
- 4Xie L. Wu W. Chen J. Tu J. Zhou J. Qi X. Yin X. Cholesterol levels and hemorrhagic stroke risk in East Asian versus non-East Asian populations: A systematic review and meta-analysis Neurologist 20172210711510.1097/NRL.000000000000012628644250 · doi ↗ · pubmed ↗
- 5Gong X. Chen L. Song B. Han X. Xu W. Wu B. Sheng F. Lou M. Associations of lipid profiles with the risk of ischemic and hemorrhagic stroke: A systematic review and meta-analysis of pro-spective cohort studies Front. Cardiovasc. Med.2022989324810.3389/fcvm.2022.89324836407431 PMC 9668898 · doi ↗ · pubmed ↗
- 6World Health Organization Healthy Diet Available online: https://www.who.int/news-room/fact-sheets/detail/healthy-diet(accessed on 30 September 2025)
- 7Cámara M. Giner R.M. González-Fandos E. López-García E. Mañes J. Portillo M.P. Rafecas M. Domínguez L. Martínez J.A. Food-based dietary guidelines around the world: A comparative analysis to update AESAN Scientific Committee dietary recommendations Nutrients 202113313110.3390/nu 1309313134579007 PMC 8471688 · doi ↗ · pubmed ↗
- 8Ministry of Health, Labour and Welfare Japanese Food Guide Spinning Top Available online: https://www.mhlw.go.jp/bunya/kenkou/eiyou-syokuji.html(accessed on 17 September 2025)