Ultra-Processed Foods and Mental Health in Children and Adolescents: Evidence from a Systematic Review
Antonia Georgiou, Stavri Chrysostomou, Maria Kantilafti

TL;DR
This paper reviews evidence linking high consumption of ultra-processed foods to mental health issues like anxiety and depression in children and adolescents.
Contribution
A systematic review of recent studies showing a link between ultra-processed food intake and mental health problems in young people.
Findings
High UPF consumption is positively associated with mental health problems such as anxiety and depression.
Variations in findings were observed based on country, sex, and assessment tools used.
The review supports UPFs as a potential risk factor for mental health issues in children and adolescents.
Abstract
Background/Objectives: The increasing consumption of ultra-processed foods (UPFs) has been associated in recent years with negative effects on both physical and mental health. Ultra-processed products have been increasingly linked with poorer mental health outcomes, with research suggesting associations with higher rates of depression, anxiety, and cognitive difficulties. The aim of this systematic review was to determine whether and to what extent UPF intake is linked to metal health in children and adolescents. Methods: The methodological approach involved a systematic review of 20 recent epidemiological studies, identified through the PubMed and EBSCO databases using MeSH and TIAB search terms. The selected articles were evaluated in terms of sample characteristics, assessment tools, results and methodological quality. Results: Most findings revealed a positive association between…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
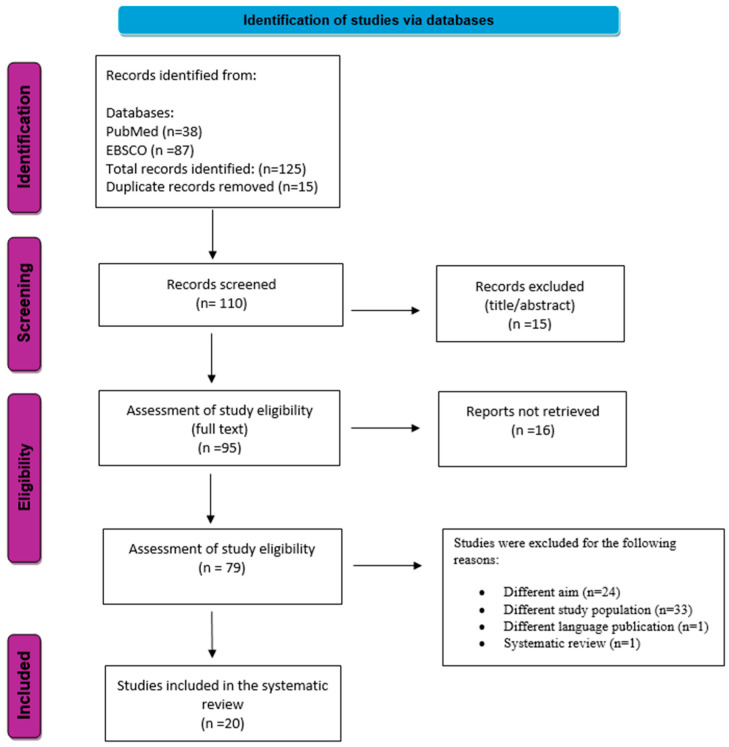 Figure 1
Figure 1| Author, Year | Country | Sample | Assessment/Tools | Exposure | Outcome | Main Findings |
|---|---|---|---|---|---|---|
| Vilija et al., 2014 [ | Lithuania | 13–14 years | Self-administered questionnaire assessing PTSSs, dietary habits and mental health indicators | Frequent consumption of unhealthy foods | PTSSs after traumatic life events | Higher consumption of unhealthy foods was significantly associated with increased PTSSs. |
| Zahra et al., 2014 [ | United Kingdom | 12–16 years | Self-reported mental and physical health dietary habits. | Fast food consumption | SDQ | Moderate consumption: OR = 1.31 (95% CI: 1.02–1.65, |
| Park et al., 2016 [ | South Korea | 12–18 years | Dietary behaviors and mental health | Energy drink consumption: | Sleep disturbance, anxiety, depressive mood, suicidal ideation, suicide planning, and suicide attempts | Frequent energy drink consumption (≥5 times/week) was associated with higher risk of mental health problems: |
| Parad et al., 2019 [ | India | 13–16 years | TAI, 24HR, and overall academic performance (school records and MCQ tests) | Fast food consumption | Academic performance and exam anxiety | In the sample from towns, frequent fast food consumption was not significantly associated with increased exam anxiety |
| Jacob et al., 2020 [ | 32 countries: | 12 years | Consumption of fast food, alcohol, sugary drinks, fruits and vegetables, as well as tobacco use and physical activity. | Fast food consumption | Suicide attempts in the past 12 months | Higher frequency of fast food consumption was associated with increased odds of suicide attempts. Across countries, 8.3% of adolescents reported suicide attempt. Poorer OR from meta-analysis across 32 countries: |
| Werneck et al., 2021 [ | Brazil | 14.3 years (mean age) | 7-day recall | Daily consumption of UPFs | Anxiety-related sleep disturbance | Daily UPF consumption was associated with increased likelihood of anxiety-induced sleep disturbance: |
| Álvarez-Villaseñor et al., 2020 [ | Mexico | 8–13 years | Questionnaires: | Fast food consumption | EAT | No significant association was found between fast food consumption and eating anxiety: |
| Silva et al., 2021 [ | Brazil | 12–17 years | GHQ-12 | Unhealthy dietary pattern with high UPF consumption and low- or non-processed foods | CMDs | The UPF-rich dietary pattern was associated with higher odds of CMDs: OR = 1.68, 95% CI: 1.51–1.87 |
| Horsager et al., 2022 [ | Denmark | 13–17 years | Online parent-reported questionnaire | UPF-dependence behaviors (food addiction symptoms) | Severity of food addiction symptoms | Higher UPF-dependence scores were observed among adolescents with mental disorders. Mean dependence score: 13.8 (95% CI: 12.6–14.9). |
| Faisal-Cury et al., 2022 [ | Brazil | 14–15 years | FFQ and | UPFs | Internalizing symptoms (anxiety, sadness, and isolation) | Higher UPF consumption was positively associated with internalizing symptoms in both crude (β = 0.14, |
| Mesas et al., 2022 [ | Brazil | 13–17 years | UPF intake, mental health and sociodemographic factors | UPF consumption | Mental health: depressing feelings, feelings that life is not worth living and that no one cares, and nervousness. Excessive worries about everyday matters. | Higher daily UPF consumption was associated with increased frequency of mental health symptoms: |
| Lane et al., 2022 [ | Iran | 12–18 years (girls) | UPF consumption and quality of life | UPF consumption | Quality of life, daytime sleepiness and insomnia | High UPF consumption was associated with increased odds of reduced quality of life |
| Gketsios et al., 2023 [ | Greece | 10–12 years | Dietary habits, consumption of UPFs and emotional/behavioral symptoms with emphasis on aggression and feelings of loneliness | Combined consumption of soda drinks and sweet/salty snacks, differentiated by intake level (low vs. at least moderate) | Emotional and behavioral symptoms (which worsen in aggression and loneliness) | Moderate consumption of sweets/salty snacks was associated with higher odds of aggressive behavior (OR = 1.50, 95% CI: 1.19–1.88) and feelings of loneliness (OR = 1.56, 95% CI: 1.20–2.01). |
| Gratão et al., 2024 [ | Brazil | 12–17 years | Dietary patterns, UPF consumption and mental health symptoms | UPF consumption | Mental health disorders: anxiety symptoms, depressive symptoms and somatic complaints | Higher UPF consumption was positively associated with increased risk of mental health disorders. Adolescents in the highest quartile of UPF consumption had higher odds of mental health problems (OR = 1.20; 95% CI:1.18–1.22). |
| Rurgo et al., 2024 [ | Italy | 9–18 years | CDI-2 | UPF consumption | Depressive symptoms, anxiety symptoms and sleep disturbance | Participants with high UPF consumption (≥2 times/day) were at higher risk of depressive symptoms CDI-2 ( |
| Huang et al., 2025 [ | China | 3–7 years: | SDQ, | UPF consumption | Emotional and behavioral problems: hyperactivity, difficulties in peer relationships and social withdrawal | Daily UPF consumption was associated with increased risk of psychological problems in young children (OR = 1.202, 95% CI: 1.051–1.376). |
| Yang et al., 2026 [ | China | 10–19 years, | Psychological distress: SCL-90 and | UPF consumption | PD | Νο PD: High UPF consumption increased danger of PD (OR = 1.710, 95% CI: 1.486–1.968, |
| Author/Year | Country | Sample | Assessment | Duration | Exposure | Outcome | Main Findings |
|---|---|---|---|---|---|---|---|
| Davison et al., 2021 [ | Ireland | 13–14 years | sWEMWBS, | 2 years | Frequency of consumption: junk food, fruits/vegetables, meat, bread/dairy, and protein | Mental well-being and HRQoL | Higher consumption of UPFs/junk food was negatively associated with quality of life (KS-10: Est = −0.165, |
| Peacock et al., 2011 [ | United Kingdom | FFQ and | 16 months | ‘Junk food’ consumption | Mental health: behavioral changes | No strong evidence of an association between junk food consumption and behavioral problems. The total difficulties score showed no significant association (OR = 1.05 (95% CI: 0.92–1.21, |
| Study | Country | Sample | Assessment/Instruments | Exposure | Outcome | Results |
|---|---|---|---|---|---|---|
| Kim et al., 2015 [ | Korea | 12–18 years (girls only), | K-BDI | Consumption of fast food and UPFs | Presence or absence of depression | Positive association between fast food consumption and depression (OR: 1.88, 95%CI: 1.13–3.14, |
| Author/Year | Selection * | Comparability ** | Outcome | Total Score | ||||
|---|---|---|---|---|---|---|---|---|
| (1) Representativeness of the Sample | (2) | (3) | (4) | (1) | (1) | (2) | ||
| Vilija et al., 2014 [ | ☆ | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆☆ | 9/10 |
| Zahra et al., 2014 [ | ☆ | ☆ | - | ☆ | ☆☆ | ☆ | ☆☆☆ | 9/10 |
| Park et al., 2016 [ | ☆ | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆ ☆ | 9/10 |
| Parad et al., 2019 [ | - | ☆ | ☆ | ☆ | ☆ ☆ | ☆ | ☆ ☆ | 8/10 |
| Jacob et al., 2020 [ | ☆ | ☆ | ☆ | ☆ | ☆ ☆ | ☆ | ☆ ☆ | 9/10 |
| Werneck et al., 2021 [ | ☆ | ☆ | - | ☆ | ☆ ☆ | ☆ | ☆ ☆ | 9/10 |
| Álvarez-Villaseñor et al., 2020 [ | - | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ ☆ | 7/10 |
| Silva et al., 2021 [ | ☆ | ☆ | - | ☆ | ☆ ☆ | ☆ | ☆ ☆ | 8/10 |
| Horsager et al., 2022 [ | - | ☆ | - | ☆ | ☆ ☆ | ☆ | ☆ ☆ | 7/10 |
| Faisal-Cury et al., 2022 [ | ☆ | ☆ | ☆ | ☆ | ☆ ☆ | ☆ | ☆ ☆ | 910 |
| Mesas et al., 2022 [ | ☆ | ☆ | ☆ | ☆ | ☆ ☆ | ☆ | ☆ ☆ | 9/10 |
| Lane et al., 2022 [ | - | ☆ | - | ☆ | ☆ ☆ | ☆ | ☆ ☆ ☆ | 8/10 |
| Gketsios et al., 2023 [ | ☆ | ☆ | - | ☆ | ☆ ☆ | ☆ | ☆ ☆ | 8/10 |
| Gratão et al., 2024 [ | ☆ | ☆ | - | ☆ | ☆ ☆ | ☆ | ☆ ☆ ☆ | 9/10 |
| Rurgo et al., 2024 [ | - | - | - | ☆ | ☆ ☆ | ☆ | ☆ ☆ ☆ | 7/10 |
| Huang et al., 2025 [ | ☆ | ☆ | - | ☆ | ☆ ☆ | ☆ | ☆ ☆ | 8/10 |
| Yang et al., 2026 [ | ☆ | ☆ | ☆ | ☆ | ☆ ☆ | ☆ | ☆ ☆ | 9/10 |
| Authors/Year | Selection | Comparability | Outcome | Total Score | |||||
|---|---|---|---|---|---|---|---|---|---|
| (1) | (2) | (3) | (4) Demostration That the Outcome of Interest Was Not Present at the Start of the Study | (1) | (1) | (2) | (3) | ||
| Davison et al., 2021 [ | ☆ | - | ☆ | - | ☆ ☆ | ☆ | ☆ | ☆ | 7/9 |
| Peacock et al., 2011 [ | ☆ | ☆ | ☆ | ☆ | ☆ ☆ | ☆ | ☆ | ☆ | 9/9 |
| Author/Year | Selection | Comparability | Exposure | Total Score | |||||
|---|---|---|---|---|---|---|---|---|---|
| (1) Adequate Case Definition | (2) | (3) | (4) | (1) | (1) | (2) | (3) | ||
| Kim et al., 2015 [ | ☆ | - | - | - | ☆ ☆ | ☆ | ☆ | ☆ | 6/9 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsConsumer Attitudes and Food Labeling · Global Public Health Policies and Epidemiology · Nutrition, Genetics, and Disease
1. Introduction
Ultra-processed foods (UPFs) are defined as industrial formulations composed mostly or entirely of substances derived from foods and additives, resulting from a series of industrial processes and typically containing little or no intact whole foods. These products often include ingredients of exclusive industrial use, such as flavorings, emulsifiers and other additives, and are designed to be convenient, highly palatable and long-lasting [1]. According to the NOVA food classification system, foods are categorized into four distinct groups based on the extent and purpose of industrial processing. Group 1 includes unprocessed or minimally processed foods, such as fruits and vegetables, which undergo little or no processing aimed primarily at preservation or minor modifications of texture without substantially altering their nutritional profile [2,3]. Group 2 consists of culinary ingredients extracted from whole foods or directly from nature and used mainly in food preparation and seasoning rather than consumed alone, such as sugar and salt [2,3]. Group 3 includes processed foods produced by combining foods from Group 1 with ingredients from Group 2, including examples such as canned vegetables and salted nuts [3]. Group 4 comprises UPFs, which are industrial formulations made from multiple ingredients and additives designed to enhance flavor, texture and shelf life, such as biscuits and sugar-sweetened beverages [3].
Over recent decades, UPFs have become increasingly prevalent not only in adult diets but also among children and adolescents, while the consumption of unprocessed or minimally processed foods has declined [4]. Evidence from population-based studies indicates that UPFs contribute a substantial proportion of daily energy intake from an early age [1,5,6]. In the United Kingdom, consumption of UPFs at the age of seven accounts for approximately 59.4% of total energy intake [7]. Similarly, in the United States, UPFs contribute approximately 66.2% and 66.4% of total energy intake among children and adolescents, respectively [8].
High consumption of UPFs has been consistently associated with adverse health outcomes and an increased risk of non-communicable diseases in both adults and children [3,9]. Research suggests that UPFs negatively affect glycemic response [10] alter gut microbiota composition [11], reduce overall dietary nutritional quality [12] and are associated with higher prevalence of obesity [13], hypertension [14], cardiovascular diseases and metabolic syndrome [15]. Importantly, the impact of UPFs extends beyond physical health and may also influence mental health outcomes. The World Health Organization (WHO) defines mental health as a state of well-being in which individuals realize their abilities, can cope with the normal stresses of life, work productively and contribute to their community. Mental health encompasses not only the absence of mental disorders but also emotional regulation, resilience and the ability to maintain healthy interpersonal relationships. Common mental disorders include anxiety disorders (such as generalized anxiety disorder, phobias, panic disorder and social anxiety disorder) and depressive disorders (including major depressive disorder and dysthymia), as well as mood disorders (e.g., dipolar disorder), eating disorders (e.g., anorexia nervosa and bulimia nervosa), psychotic disorders (e.g., schizophrenia) and post-traumatic stress disorder (PTSD) [16].
According to the WHO, approximately one in seven adolescents aged 10–19 years experience a mental disorder, accounting for nearly 15% of the global burden of disease within this age group. Depression, anxiety and behavioral disorders are among the most prevalent mental health conditions in youth. Moreover, suicide represents the third leading cause of death among individuals aged 15–29 years worldwide, highlighting the critical importance of identifying modifiable risk factors during childhood and adolescence [16].
Current evidence from two meta-analyses suggests a significant association between UPF consumption and mental health outcomes. Two recent meta-analyses published in 2022 highlight this relationship across different population groups [17,18]. The meta-analysis by Lane et al. (2022), which included 17 observational studies (15 cross-sectional and 2 prospective studies) comprising a total of 385,541 participants (the mean age of the sample was 35 years old), demonstrated that higher consumption of UPFs was associated with an increased likelihood of depressive and anxiety symptoms [18]. Similarly, the meta-analysis conducted by Malmir et al. (2023), focusing exclusively on children and adolescents, analyzed 17 observational studies and reported significant associations among anxiety, sleep disturbances and reduced psychological well-being [17].
Based on the existing literature, an increasing body of evidence suggests a positive association between the consumption of UPFs and adverse mental health outcomes among children and adolescents at a global level. Research interest in this field has grown substantially in recent years. However, the specific impact of UPF consumption on the mental health of younger populations remains insufficiently explored and highly fragmented. Most available studies are observational in nature, vary considerably in their methodological approaches, and differ in terms of mental health outcomes assessed, age groups examined, and definitions of UPF exposure. To date, only a limited number of meta-analyses have examined this association, with only two meta-analyses published so far, both in 2022 [17,18]. However, the meta-analysis by Lane et al. (2022) [18] included predominantly adult populations, while the meta-analysis by Malmir et al. (2023) [17], although focusing on children and adolescents, was based on studies published up to four years prior to its publication. Given the rapid expansion of the literature, the public health relevance of childhood dietary patterns, and the vulnerability of mental health during early life stages, a comprehensive and up-to-date systematic review is warranted to synthesize current evidence, identify research gaps, and inform future research, policy, and intervention strategies.
Therefore, this study aims to examine the association between UPF consumption and mental health outcomes in children and adolescents through a systematic review of the current scientific evidence.
2. Materials and Methods
2.1. Search Strategy and Eligibility Criteria
A systematic literature search was conducted using PubMed and EBSCOhost databases between November 2026 and January 2026, in order to identify studies examining the association between UPF consumption and mental health outcomes in children and adolescents. The final search was completed on 31 January 2026. Boolean operators (AND, OR) were used to combine keywords and enhance the precision of the search by reducing non-relevant records. In PubMed, the search strategy was refined using both MeSH (Medical Subject Headings) terms and TIAB (title/abstract) field tags to ensure the retrieval of both indexed and recently published studies. In EBSCOhost, the same search terms and Boolean operators were applied, without the use of MeSH or TIAB field tags.
Study selection and data extraction were conducted according to predefined inclusion and exclusion criteria. Eligible studies examined the association between UPF consumption and mental health outcomes and involved children and adolescents aged 3–19 years. Only studies published in English and employing an observational study design, specifically cross-sectional, cohort, and case–control studies, were included. Studies were excluded if they involved animal models, were published in languages other than English, were case reports, or included adults or infants. A summary of the search strategy is presented in Table 1. The full strategy can be found in Supplementary Material Table S1.
2.2. Study Selection and Data Extraction
The titles and abstracts identified through the electronic searches were independently screened by two researchers, and full-text articles of studies deemed potentially eligible were retrieved and assessed according to the predefined inclusion criteria. Conflicting assessments were resolved via discussion until a consensus was achieved. From each included study, data were systematically extracted using a standardized form. The extracted information included: author(s), year of publication and country; study design (cross-sectional, cohort or case–control) and follow-up duration (where applicable); sample size and age range of participants; dietary assessment methods and classification of UPFs according to the NOVA system; type and frequency of UPF exposure; mental health outcomes assessed and corresponding measurement instruments; key statistical estimates (e.g., odds ratios, beta coefficients, and confidence intervals); and the main findings of each study.
2.3. Quality Assessment
The methodological quality of the included studies was assessed using the Newcastle–Ottawa Scale (NOS), with adaptations according to study design. For cross-sectional studies, scores of 9–10 stars were classified as very high quality, 7–8 stars as high quality, 5–6 stars as satisfactory quality, and 4 stars or fewer as unsatisfactory quality. For cohort studies, methodological quality was categorized as good, moderate, or poor based on domain-specific star allocation. Similarly, case–control studies were classified as having good or poor methodological quality according to predefined star thresholds across the NOS domains [19].
3. Results
3.1. Main Findings of the Included Studies
The systematic search identified a total of 125 studies (PubMed = 38 and EBSCO = 87). After removing duplicates and screening titles and abstracts, 110 studies proceeded to full-text assessment. Following eligibility assessment, 20 studies met all inclusion criteria and were incorporated into the systematic review (Figure 1).
Most of the studies were cross-sectional designs (n = 17), followed by two prospective cohort studies and one case–control study. Sample sizes ranged from 56 to 105,061 participants. The target population comprised children and adolescents aged 3–19 years, with adolescents aged 12–18 years representing the predominant age group. Most studies utilized self-reported questionnaires to assess both dietary intake and mental health status. The primary exposures included consumption of UPFs, junk food and sugar-sweetened beverages. Mental health outcomes encompassed a wide range of indicators, such as depressive and anxiety symptoms, sleep disturbances, suicidal ideation and behavioral problems. More detailed information on the main characteristics of the included studies is presented in Table 2, Table 3 and Table 4.
3.2. Methodological Quality
Table 5, Table 6 and Table 7 present the results of the methodological quality assessment of the included cross-sectional, cohort and case–control studies, respectively, using the NOS. Overall, most of the included studies were rated high and very high methodological quality. Most cross-sectional studies demonstrated high [21,22,23,24,25,26,27] and very high methodological quality [28,29,30,31,32,33,34,35,36,37]. The cohort studies were generally assessed as being of good [38] and medium [39] methodological quality. The case–control study [40] was rated as being of moderate methodological quality.
3.3. UPFs and Mental Health—Cross-Sectional Studies
Most of the included cross-sectional studies consistently reported positive associations between UPF consumption and adverse mental health outcomes among children and adolescents. Higher intake of energy drinks, soft drinks, fast food and junk food was associated with increased odds of psychological distress, depressive symptoms, anxiety, suicidal ideation and suicide attempts across diverse populations [27,28,29,30,31,32,33,34,35,36]. These associations were largely consistent across countries, age groups, and specific mental health outcomes.
Several large national studies conducted in Lithuania [36], the United Kingdom [35], South Korea [34], China [28] and Brazil [29,30] demonstrated dose–response relationships, with more frequent consumption linked to progressively higher risks of mental health problems. Particularly strong associations were observed between suicidal behaviors among adolescents and frequent energy drink consumption, especially when combined with junk food intake [34].
Multinational data from the Global School-based Student Health Survey across 32 countries further supported these findings, showing elevated odds of suicide attempts among fast food consumers, with stronger associations in low-income countries [33]. Similar patterns were observed in younger children and specific populations, including preschool-aged children in China [22], adolescent girls in Iran [24], and adolescents with anorexia nervosa in a clinical sample [21].
These findings were consistent across the large majority of cross-sectional studies included in the review, irrespective of country, age group, or the specific mental health outcomes assessed (Table 2).
3.4. UPFs and Mental Health—Cohort Studies
Only two cohort studies have examined the longitudinal association between UPFs or junk food consumption and mental health or behavioral outcomes among children and adolescents. The Wellbeing in Schools (WISE) study conducted in Northern Ireland reported a negative longitudinal association between junk food consumption and mental well-being over a two-year follow-up period, with evidence of stability in dietary patterns over time [38]. Higher junk food intake was also associated with poorer overall dietary quality at baseline. In contrast, findings from the Avon Longitudinal Study of Parents and Children (ALSPAC) suggested that although initial analyses indicated positive associations between junk food intake in early childhood and later behavioral difficulties, these associations were attenuated and became non-significant after adjustment for key confounders [39]. Results from the cohort studies are summarized in Table 3.
3.5. UPFs and Mental Health—Case–Control Study
Only one case–control study met the inclusion criteria of the present review (Table 4). In this study, higher consumption of UPFs and fast food was positively associated with depressive symptoms among adolescent girls, even after adjustment for potential confounders [40]. Adolescents with greater UPF intake had substantially higher odds of depression, whereas higher consumption of minimally processed plant foods, including vegetables and legumes, was inversely associated with depressive symptoms.
4. Discussion
The present systematic review identified reported associations between high UPF consumption and various mental health indicators in children and adolescents across several studies. The most consistent and recurrent associations were observed for anxiety-related symptoms, depressive symptoms and sleep disturbances, which were reported across multiple studies and diverse populations [21,28,29,32,34]. In addition, higher UPF intake was associated with other internalizing and externalizing psychological symptoms, including post-traumatic stress, irritability, nervousness, hyperactivity and emotional detachment [22,30,35,37]. Associations were also reported with suicidal ideation and suicide attempts [33,34], as well as with poorer psychosocial well-being and reduced perceived quality of life [24,38].
In contrast, the cross-sectional study by Álvarez-Villaseñor et al. (2020) [26] and the cohort study by Peacock et al. (2011) [39] found no significant associations. In the study by Álvarez-Villaseñor et al. (2020) [26], no statistically significant association was found between junk food consumption and anxiety. This lack of association is likely due to the exceptionally high prevalence of junk food intake within the sample (94%). Such high prevalence substantially limited exposure and reduced the statistical power of the analysis. Although the assessment of disordered eating-related anxiety using the EAT questionnaire is considered valid and widely applied in adolescent populations, the cross-sectional design precludes causal inference. This limitation arises from the lack of temporal sequencing between exposure and outcome [26]. These findings highlight the need for additional longitudinal research to more accurately evaluate the relationship between junk food consumption and anxiety symptoms in youth. Similarly, the cohort study by Peacock et al. (2011) [39] found no evidence of an association between junk food consumption at 81 months of age and behavioral problems over the following 16 months. Any initial associations were largely attenuated after adjustment for baseline behavioral difficulties and key confounders, including socioeconomic status, child IQ, and maternal mental health. This suggests that the observed relationship may have been influenced by confounding rather than reflecting a direct dietary effect. Age at assessment and methodological factors may also have contributed to the reduced likelihood of detecting diet-related behavioral outcomes [26].
The findings of the present review are consistent with previous systematic reviews and meta-analyses examining the association between ultra-processed food consumption and mental health outcomes. The meta-analysis by Lane et al. (2022), which predominantly included adult populations, reported significant associations between higher UPF intake and increased depressive and anxiety symptoms, findings that align with those observed in the present review [18]. More directly comparable are the results of the meta-analysis by Malmir et al. (2023), which focused on children and adolescents and identified significant associations between junk food consumption, psychological distress and sleep-related outcomes [17]. The present review supports these findings and extends the existing evidence by incorporating more recent studies and examining a broader range of mental health outcomes.
High consumption of UPFs has been associated with poorer mental health outcomes through a rage of biological and psychological mechanisms. UPFs are rich in added sugars, trans fatty acids and other compounds associated with chronic inflammatory processes and gut microbiome dysbiosis, leading to increased intestinal permeability and neuroinflammation [18]. Elevated inflammatory markers such as C-reactive protein (CRP) and cytokines (IL-6, TNF-a) have been repeatedly linked to depressive and anxiety symptoms [41]. Inflammatory processes can disrupt serotonin and dopamine production, affecting mood, sleep and behavior [18]. UPFs may also influence neurotransmission [42]. Chronic consumption may result in deficiencies in essential micronutrients (e.g., magnesium, zinc, and B vitamins) that are required for neurotransmitter synthesis [43]. Excessive sugar intake is associated with dopaminergic dysregulation, characterized by overstimulation of reward pathways, which over time may lead to dependency, emotional instability and mood fluctuations [44]. Evidence from human and animal studies indicates that chronic UPF intake disrupts dopaminergic signaling, increasing cravings and promoting persistent consumption [45]. UPF consumption is also associated with body image disturbances and challenges in weight management, including increased obesity risk and psychological distress related to eating behaviors [45]. Additionally, UPFs are implicated in gut microbiome dysbiosis [46]. Their low fiber content and high levels of processed sugars negatively affect gut microbial composition. Gut dysbiosis may impair gut–brain communication via the vagus nerve, influencing neurotransmitters such as serotonin and dopamine [47]. UPFs also affect psychosocial mechanisms, including emotional eating. Adolescents frequently report using UPFs to cope with stress or loneliness. Social isolation, low self-esteem and the need for immediate gratification increase the preference for ‘comfort foods’, which are often ultra-processed [48].
The current review presents both strengths and limitations. A key strength is that this review specifically focuses on the pediatric population, addressing a critical gap in the literature. To date, only one meta-analysis published in 2022 has examined the association between UPF consumption and mental health in children and adolescents [17]. Additionally, this systematic review incorporates the most recent studies on the topic, providing an up-to-date synthesis of current evidence. By including only studies conducted in children and adolescents, the review allows for a more precise understanding of age-specific associations and developmental considerations that may not be captured in adult-focused research. Unlike earlier meta-analyses, which predominantly focused on adults or relied on older studies, the present review synthesizes a highly fragmented and methodologically diverse body of literature, where mental health outcomes, exposure definitions, and assessment tools vary considerably. By integrating these heterogeneous findings, it offers a coherent and developmentally sensitive perspective on the relationship between UPFs and mental health during critical early life stages. Furthermore, it highlights issues that received limited attention in previous work, such as the overrepresentation of adolescent girls in several studies and the implications for interpretation and generalizability. This age-focused synthesis thus advances the field beyond merely updating available evidence. However, several limitations must be acknowledged. First, the predominance of cross-sectional studies restricts the ability to draw causal conclusions. Only two cohort studies and one case–control study were included, the latter presenting methodological limitations that further constrain causal inference. The heterogeneity of mental health and dietary assessment tools also complicates comparability across studies, despite common use of instruments such as GHQ, SDQ, NOVA classification, FFQs and 24 h recalls. Notably, several of the included studies focused exclusively or predominantly on adolescent girls [21,23,24,40]. This is not incidental, as international data consistently show that adolescent girls report higher rates of anxiety and depression compared with boys after puberty and the WHO highlights that eating disorders and internalized psychological distress are more common in females [49]. However, the overrepresentation of female participants limits the generalizability of the findings to the broader adolescent male population, underscoring the need for balanced gender representation in future studies. Finally, the primary studies did not conduct analyses of macro- or micronutrient profiles, nor did they distinguish between potential ‘toxic’ effects of industrial food processing (e.g., additives and chemical neoformations) and the ‘deficiency’ effects arising from displacement of essential nutrients such as zinc, magnesium, or omega-3 fatty acids. As a result, the mechanisms underlying the observed associations cannot be attributed specifically to nutrient insufficiencies or to processing-related components, and future studies incorporating biochemical markers and detailed nutrient analyses are needed to elucidate these pathways.
5. Conclusions
Τhe current evidence indicates a clear association between high consumption of ultra-processed foods and adverse mental health outcomes in children and adolescents. These findings highlight the urgent need for additional prospective studies that can provide stronger causal evidence. Future research should focus on the development and consistent application of age- and culture-specific psychosocial and dietary assessment tools and include diverse socio-cultural populations to enhance validity and generalizability. Beyond research, school- and family-based interventions, along with nutrition education programs, are essential to reducing UPF consumption from an early age and promoting healthier dietary habits. These interventions may contribute to healthier dietary patterns in childhood and potentially support mental well-being. However, further research is needed to clarify causal pathways.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Monteiro C.A. Cannon G. Levy R.B. Moubarac J.C. Louzada M.L. Rauber F. Khandpur N. Cediel G. Neri D. Martinez-Steele E. Ultra-processed foods: What they are and how to identify them Public Health Nutr.20192293694110.1017/S 136898001800376230744710 PMC 10260459 · doi ↗ · pubmed ↗
- 2Monteiro C.A. Cannon G. Levy R. Moubarac J.C. Jaime P. Martins A.P. Canella D. Louzada M. Parra D. NOVA. The star shines bright World Nutr.201672838
- 3Gibney M.J. Ultra-processed foods: Definitions and policy issues Curr. Dev. Nutr.20193 nzy 07710.1093/cdn/nzy 07730820487 PMC 6389637 · doi ↗ · pubmed ↗
- 4Wang L. Martínez Steele E. Du M. Pomeranz J.L. O’Connor L.E. Herrick K.A. Luo H. Zhang X. Mozaffarian D. Zhang F.F. Trends in Consumption of Ultraprocessed Foods Among US Youths Aged 2–19 Years, 1999–2018 JAMA 202132651953010.1001/jama.2021.1023834374722 PMC 8356071 · doi ↗ · pubmed ↗
- 5Poti J.M. Braga B. Qin B. Ultra-processed Food Intake and Obesity: What Really Matters for Health-Processing or Nutrient Content?Curr. Obes. Rep.2017642043110.1007/s 13679-017-0285-429071481 PMC 5787353 · doi ↗ · pubmed ↗
- 6Neri D. Steele E.M. Khandpur N. Cediel G. Zapata M.E. Rauber F. Marrón-Ponce J.A. Machado P. da Costa Louzada M.L. Andrade G.C. Ultraprocessed food consumption and dietary nutrient profiles associated with obesity: A multicountry study of children and adolescents Obes. Rev.202223 e 1338710.1111/obr.1338734889015 · doi ↗ · pubmed ↗
- 7Conway R.E. Heuchan G.N. Heggie L. Rauber F. Lowry N. Hallen H. Llewellyn C.H. Ultra-processed food intake in toddlerhood and mid-childhood in the UK: Cross sectional and longitudinal perspectives Eur. J. Nutr.2024633149316010.1007/s 00394-024-03496-739363048 PMC 11519182 · doi ↗ · pubmed ↗
- 8Khandpur N. Neri D.A. Monteiro C. Mazur A. Frelut M.L. Boyland E. Weghuber D. Thivel D. Ultra-Processed Food Consumption among the Paediatric Population: An Overview and Call to Action from the European Childhood Obesity Group Ann. Nutr. Metab.20207610911310.1159/00050784032344405 · doi ↗ · pubmed ↗