Association Between Dietary Calcium or Dairy Product Intake and Metabolic Syndrome Risk: A Systematic Review and Meta-Analysis
Stefano Gonnelli, Antonella Al Refaie, Sara Gonnelli, Caterina Mondillo, Guido Cavati, Alessandra Cartocci, Carla Caffarelli

TL;DR
This study finds that higher dietary calcium and dairy intake are linked to a lower risk of metabolic syndrome in adults, but more research is needed to confirm if this is a cause-and-effect relationship.
Contribution
A systematic review and meta-analysis showing inverse associations between calcium/dairy intake and metabolic syndrome risk in adults.
Findings
Higher dietary calcium intake is associated with a 15% lower odds of metabolic syndrome.
Dairy product consumption is linked to a 22% lower odds of metabolic syndrome.
Calcium intake correlates with improved individual metabolic syndrome components like blood pressure and HDL cholesterol.
Abstract
Background: Dietary calcium and dairy products are hypothesized protective factors against metabolic syndrome (MetS), yet epidemiological evidence remains inconsistent. This systematic review and meta-analysis evaluated the association between total dietary calcium intake or dairy consumption and MetS prevalence in adults. Methods: Following PRISMA 2020 guidelines, PubMed, Cochrane Library, ClinicalTrials.gov, and SCOPUS were searched through to October 2025 for eligible cross-sectional studies assessing dietary calcium or dairy intake and MetS (NCEP ATP III, IDF, or JIS criteria). Longitudinal studies, non-English articles, and pediatric populations were excluded. Quality was assessed via an adapted Newcastle–Ottawa Scale. Random-effects meta-analyses pooled fully adjusted odds ratios (ORs) and 95% confidence intervals (CIs) comparing the highest versus lowest intake categories.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
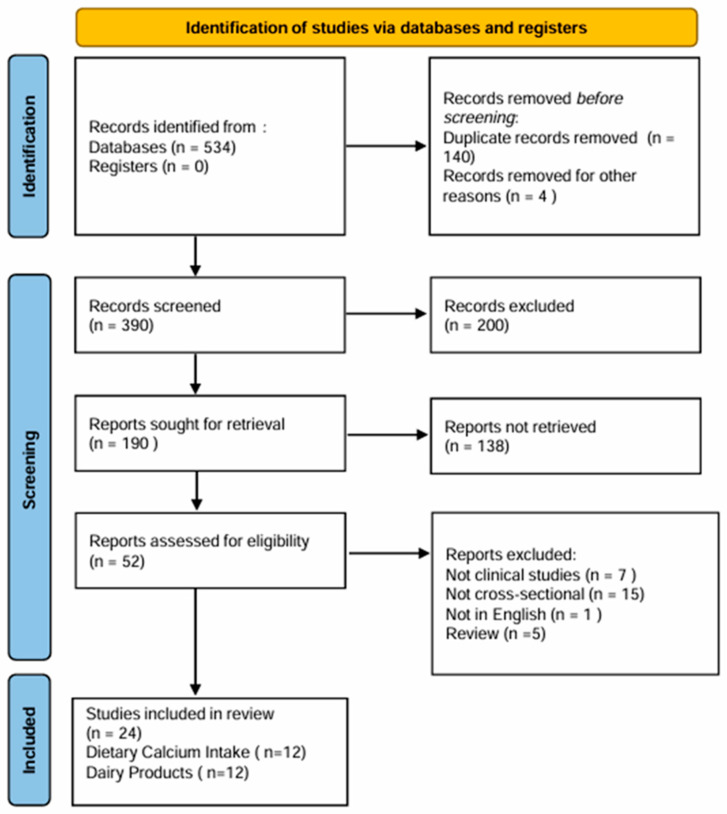 Figure 1
Figure 1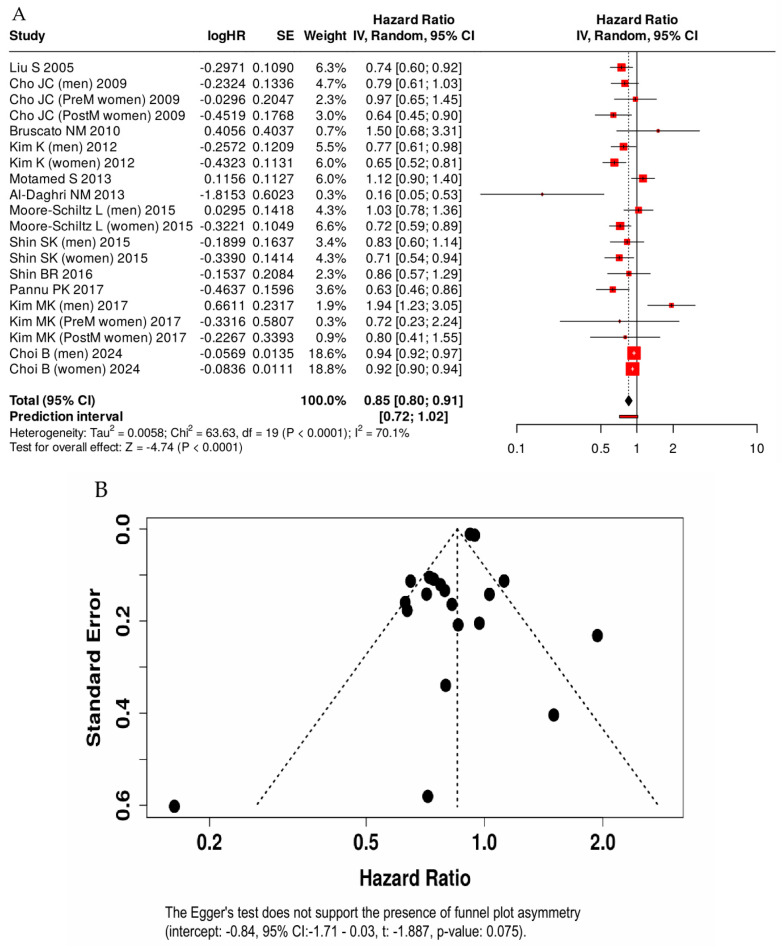 Figure 2
Figure 2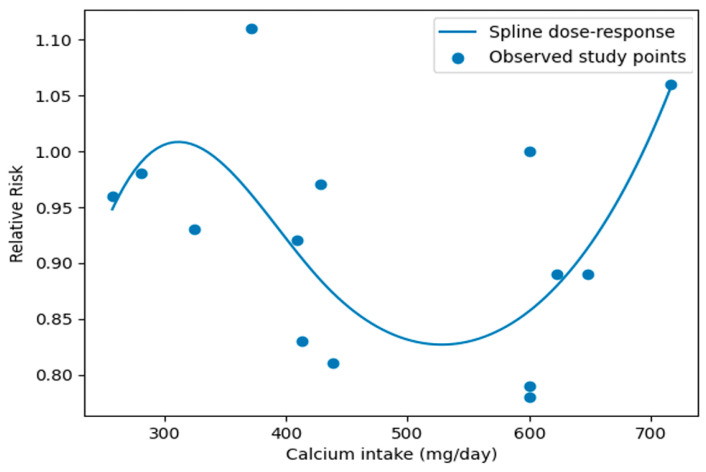 Figure 3
Figure 3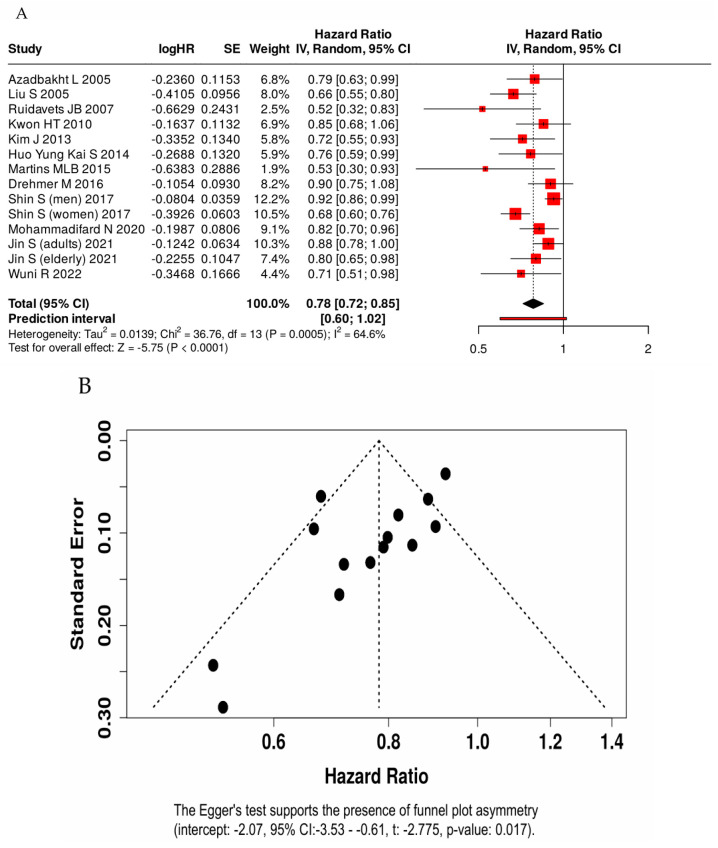 Figure 4
Figure 4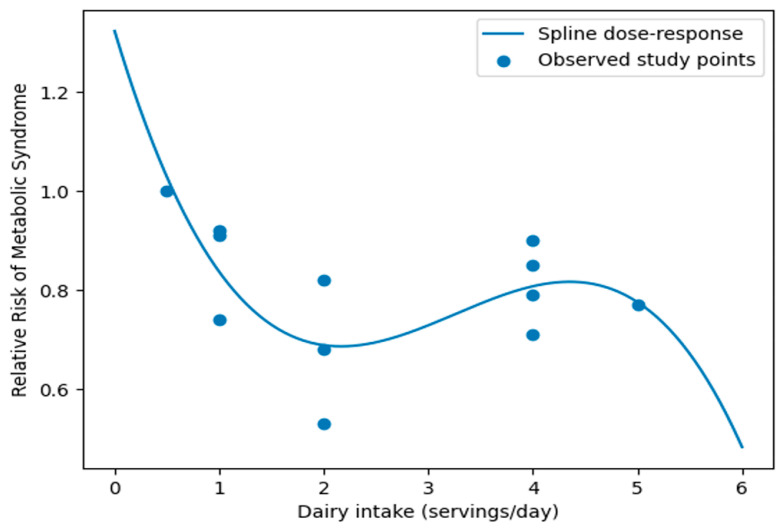 Figure 5
Figure 5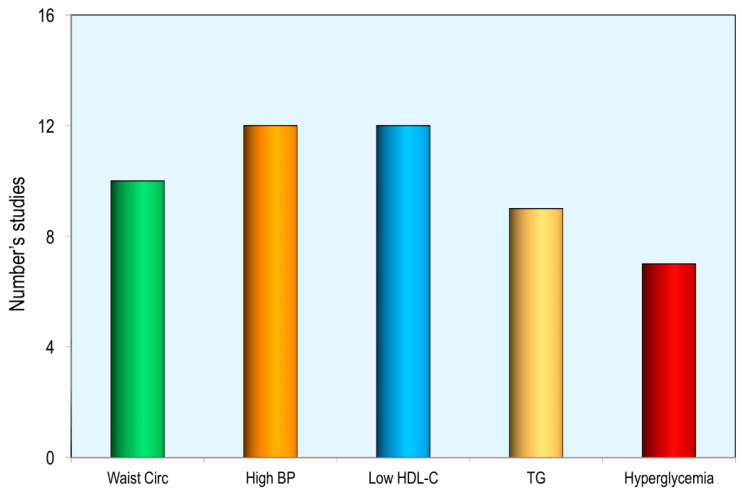 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNutritional Studies and Diet · Sodium Intake and Health · Vitamin D Research Studies
1. Introduction
Metabolic syndrome (MetS), first described by Reaven in 1988 as “Syndrome X,” is characterized by the clustering of metabolic risk factors that substantially increase the risk of cardiovascular disease and type 2 diabetes mellitus [1]. Diagnostic criteria included the presence of at least three of the following components: central obesity, arterial hypertension, fasting hyperglycemia, hypertriglyceridemia, and low HDL cholesterol levels [2]. MetS reflects a complex metabolic dysfunction, frequently associated with insulin resistance and chronic low-grade inflammation, and represents a major determinant of cardiovascular morbidity and mortality [3]. The prevalence of MetS is increasing worldwide, particularly in Western countries, the Americas, and the Eastern Mediterranean region, driven by sedentary lifestyles, rising obesity rates, and population aging [4]. In Western populations, MetS affects approximately 20–35% of adults; in the United States, about 34% of adults meet ATP III criteria, while Europe shows comparable prevalence with notable regional variability [4,5]. In Italy, epidemiological studies report prevalence rates between 25% and 30%, with higher rates among older individuals, men, and those with obesity, and a narrowing of sex differences after menopause [6].
Despite extensive research, the pathogenesis of MetS remains only partially understood. Both genetic and environmental factors contribute, with diet playing a central role. Diets rich in simple sugars and saturated or trans fats and poor in fiber and micronutrients promote insulin resistance, inflammation, and endothelial dysfunction [7]. Conversely, healthy dietary patterns such as the Mediterranean and Dietary Approaches to Stop Hypertension (DASH) diets have been shown to improve glucose and lipid metabolism and favorably influence individual MetS components, including waist circumference, triglycerides, HDL cholesterol, and fasting glucose [7,8,9,10].
Growing epidemiological evidence suggests that higher consumption of dairy products—particularly low-fat and fermented types—is associated with a lower risk of MetS and improvements in its individual components [11,12,13]. Although dairy foods contain multiple nutrients that may affect metabolic health, calcium has been proposed as a key contributor. Observational studies have consistently reported inverse associations between dietary calcium intake and MetS prevalence, particularly in women [14,15]. Higher calcium intake has been linked to reduced obesity risk, possibly through effects on lipogenesis and fat oxidation [16], as well as improvements in insulin secretion, blood pressure regulation, and lipid metabolism [17,18]. However, other studies have failed to confirm these associations, yielding inconsistent findings [19,20]. In summary, while evidence suggests a potential link between dietary calcium intake and MetS, current data remain inconclusive.
Therefore, this systematic review and dose–response meta-analysis aims to examine evidence from cross-sectional studies on the association between dietary calcium intake or dairy products and metabolic syndrome, to better clarify the nature of this relationship.
2. Materials and Methods
2.1. Search and Assessment of Studies
For this review we considered all relevant articles published up to October 2025. The PubMed/Medline, Cochrane Library, ClinicalTrials.gov, and SCOPUS databases were searched using the following search terms: “calcium intake” or “dietary calcium”, “dairy foods/products consumption” and “metabolic syndrome” or “MetS”. The process of selecting the studies for review in adherence to the PRISMA 2020 (Preferred Reporting Items for Systematic reviews and Meta Analyses) [21] is shown in Figure 1. Moreover, the protocol was registered in PROSPERO with code CRD420261328992. After excluding irrelevant articles, duplicates, case–control, cohort, reviews, and meta-analyses, 24 studies were deemed eligible for inclusion in the review. Of these, 12 examined the relationship between total dietary calcium intake and metabolic syndrome, while 12 investigated the association between dairy products consumption and metabolic syndrome, thereby forming two distinct groups that were analyzed separately. All included studies had a cross-sectional design. In all cases, daily dairy food consumption and total dietary calcium intake were assessed using dietary questionnaires. The exclusion criteria were as follows: (i) cohort and longitudinal studies; (ii) studies written in languages other than English; (iii) studies assessing the association between dietary calcium intake or dairy consumption and one or only some components of metabolic syndrome, rather than metabolic syndrome as a whole; and (iv) studies including participants under 18 years of age or with specific pathologies.
2.2. Methodological Quality and Risk of Bias of Studies
Methodological quality and risk of bias of the included cross-sectional studies were assessed using an adapted version of the Newcastle–Ottawa Scale (NOS). This tool evaluates studies across three domains: Selection (maximum 4 stars), Comparability (maximum 2 stars), and Outcome (maximum 3 stars), with a total possible score of 9 stars. Overall study quality was categorized as low (0–4 stars), moderate (5–6 stars), or high (7–9 stars). Two investigators (A.A. and G.S.) independently reviewed all identified studies and performed quality assessment; any disagreements regarding study eligibility were resolved through discussion and consensus (Table S1A,B of the Supplementary Material).
In all the selected studies, metabolic syndrome was defined exclusively according to one of the following criteria: (1) the Third Report of the National Cholesterol Education Program Adult Treatment Panel (NCEP ATP III) [22], (2) the International Diabetes Federation definition (IDF) [23], or (3) the Joint Interim Statement of the International Diabetes Federation (JIS) [24].
To assess the certainty of evidence, we applied the GRADE (Grading of Recommendations, Assessment, Development, and Evaluations) approach, separately evaluating the studies that considered dietary calcium intake and those that assessed dairy product consumption (Table S2A,B of the Supplementary Material) [25].
2.3. Statistical Analysis
Two separate random-effects meta-analyses were conducted to calculate the overall association between the prevalence of metabolic syndrome in studies that evaluated total dietary calcium intake and in those that evaluated dairy product intake, respectively. For each study, the most fully adjusted odds ratio (ORs) and 95% confidence intervals (CIs) comparing the highest versus the lowest categories of intake were extracted and pooled. Random-effects models were applied to account for between-study variability. Statistical heterogeneity was assessed using Cochran’s Q-test and quantified with the I^2^ statistic, calculated as
where Q represents Cochran’s heterogeneity statistic and df the degrees of freedom. I^2^ values of <50%, 50–75%, and >75% were considered indicative of low, moderate, and high heterogeneity, respectively. A Q-test p-value < 0.05 was considered statistically significant. The between-study variance (τ^2^) was estimated within the random-effects framework. Potential publication bias was evaluated by visual inspection of Begg’s funnel plots and statistically assessed using Begg’s rank correlation test and Egger’s regression test. A p-value < 0.05 was considered statistically significant. The Greenland and Longnecker method was used to evaluate the dose response meta-analysis [26].
3. Results
According to our search strategy, twenty-four cross-sectional articles were selected and included in this review. Of these, 12 articles focused on the association between total dietary calcium intake and metabolic syndrome, while the remaining 12 explored the possible association between daily consumption of dairy foods and metabolic syndrome.
3.1. Total Dietary Calcium Intake and Metabolic Syndrome
Table 1 presents the main characteristics of the eligible cross-sectional studies included in the systematic review and meta-analysis examining the association between dietary calcium intake and metabolic syndrome in adults [19,20,27,28,29,30,31,32,33,34,35,36]. Overall, the included studies comprised a total of 73,652 men and 128,058 women. With regard to study location, eight studies were conducted in Asia, two in the United States, one in Brazil, and one in Australia. Dietary calcium intake was assessed using food frequency questionnaires (FFQs) and/or 24–48 h dietary recalls. Study quality was rated as high in eight studies, moderate in three, and low in one [Table S1A in Supplementary Materials].
Moreover, all studies were conducted in apparently healthy participants. Across studies, higher dietary calcium intake was associated with lower odds of metabolic syndrome, with a pooled odds ratio of 0.85 (95% CI: 0.80–0.91) [Figure 2]. Thus, the highest level of dietary calcium intake, compared with the lowest, was associated with a statistically significant 15% reduction in the odds of metabolic syndrome. Substantial relative heterogeneity was observed (I^2^ = 70.1%); however, the estimated between-study variance was small (τ^2^ = 0.005; τ ≈ 0.07), indicating limited absolute variability in effect sizes on the log-odds scale. Visual inspection of the funnel plot of log (OR) versus standard error did not indicate substantial asymmetry. This observation was supported by Egger’s regression test (p = 0.075) and Begg’s test (Kendall’s τ = −0.02, p = 0.92), suggesting no strong evidence of publication bias among the included studies.
Meta-regression analyses were conducted to explore potential sources of heterogeneity, including geographic region, sex group, and dietary assessment method. The analysis showed that sex significantly moderated the association between dietary calcium intake and metabolic syndrome (β = −0.275, p = 0.038), indicating an inverse association in women compared with men. Geographic region and dietary assessment method were not significantly associated with Mets. Dose–response relationships were examined using a two-stage random-effects dose–response meta-analysis based on the method of Greenland and Longnecker. A linear dose–response analysis including 10 studies showed that each 100 mg/day increment in dietary calcium intake was associated with an approximately 2% lower odds of metabolic syndrome (OR = 0.98). Accordingly, a 300 mg/day increment corresponded to an estimated 6% lower odds of MetS (OR = 0.94) (Table S3A of the Supplementary Material). Potential nonlinear dose–response relationships were evaluated using restricted cubic splines with three knots placed at the 10th, 50th, and 90th percentiles of the exposure distribution. The nonlinear analysis indicated a significant association between dietary calcium intake and MetS, with the greatest reduction in MetS odds observed at approximately 500 mg/day of dietary calcium intake. Beyond this level, further increases in calcium intake were not associated with additional reductions in MetS odds [Figure 3]. This pattern suggests a potential threshold effect, whereby moderate dietary calcium intake may be sufficient to achieve the maximal reduction in MetS odds.
3.2. Total Daily Consumption of Dairy Foods and Metabolic Syndrome
Table 2 presents the main characteristics of the studies that evaluated the association between dairy products consumption and metabolic syndrome in adults [37,38,39,40,41,42,43,44,45,46,47]. Overall, the included studies comprised a total of 70,985 men and 129,952 women. With regard to study location, seven studies were conducted in Asia, two in Europe and in Brasil and one in the USA. Dietary calcium intake was assessed using FFQs and/or 24–48 h dietary recalls. Study quality was rated as high in nine studies, moderate in two, and low in one.
Using a random-effects model, higher total calcium intake was associated with lower odds of metabolic syndrome, with a pooled odds ratio of 0.78 (95% CI: 0.72–0.85) for the highest compared with the lowest intake category. Thus, the highest level of dairy products consumption, compared with the lowest, was associated with a 22% reduced odds of metabolic syndrome [Figure 4]. Moderate-to-substantial heterogeneity was observed across studies (I^2^ = 64.6%). The estimated between-study variance was modest (τ^2^ = 0.013; τ ≈ 0.11), indicating limited absolute variability in effect sizes across studies. Egger’s regression test showed significant funnel plot asymmetry (p = 0.016), which was confirmed by Begg rank correlation test (Kendall’s τ = −0.56, p = 0.005). Although both Egger’s and Begg’s tests indicated the presence of small-study effects, the trim-and-fill analysis showed an attenuation of the pooled effect after imputing potentially missing studies, while the association remained statistically significant. This suggests that publication bias may have inflated the magnitude of the effect, but it is unlikely to fully account for the observed association.
We conducted additional meta-regression analyses to explore potential sources of heterogeneity. The models included geographic region, sex group, and dietary assessment method as study-level moderators. The results indicated that sex significantly moderated the association between dairy products and metabolic syndrome, with a stronger inverse association observed in women compared with men (β = −0.302, p = 0.003). In contrast, geographic region and dietary assessment method were not significantly associated with the effect size. These findings suggest that sex differences may partly explain the between-study heterogeneity observed in the analysis (Table S3B of the Supplementary Material). Dose–response relationships were examined in nine studies where dairy product intake could be evaluated in terms of servings per day, using a two-stage random-effects dose–response meta-analysis based on the Greenland and Longnecker method. A linear dose–response analysis showed that 1-serving/day increment in dairy intake was associated with an 8% lower risk of metabolic syndrome (OR 0.92, 95% CI 0.90–0.95). A restricted cubic spline dose–response meta-analysis showed a nonlinear inverse association between dairy intake and metabolic syndrome. The steepest reduction in risk was observed up to approximately 2 servings/day, after which the association plateaued [Figure 5].
Sixteen studies examined the association between dietary calcium intake and the odds of individual components of metabolic syndrome. Higher calcium intake, from either total dietary sources or dairy products, was associated with significantly lower odds of elevated blood pressure and low HDL cholesterol in 12 studies, increased waist circumference in 10 studies, elevated triglycerides in 9 studies, and fasting hyperglycemia in 7 studies [Figure 6].
4. Discussion
The majority of cross-sectional studies included in this meta-analysis indicate that dietary calcium intake is inversely associated with the odds of metabolic syndrome in adults. This association was not observed only in the studies by Bruscato and Motamed [29,31]. In particular, in the study by Bruscato et al., the lack of association may be explained by the characteristics of the study population, which consisted exclusively of postmenopausal women older than 65 years, suggesting that nutritional factors may exert a stronger influence on MetS development at younger ages [29]. Moreover, estrogen deficiency may contribute to these age-related differences, as estrogens enhance calcium absorption and exert beneficial metabolic effects, including improvements in insulin sensitivity, reductions in inflammation, and limitation of abdominal fat accumulation [48,49]. Supporting this evidence, studies that analyzed men and women separately consistently reported a stronger protective effect of calcium intake in women than in men [28,30,32,33,35]. Similarly, in the study by Shin S. et al. [44], higher milk consumption was associated with lower odds of MetS, with a more pronounced inverse association in females. Numerous studies have demonstrated an association between dairy products with MetS [37,50]. However, this association often loses statistical significance after adjustment for calcium intake, highlighting the central role of this mineral [42]. Milk is a rich source of bioactive compounds that may improve metabolic efficiency and target multiple components of MetS; nevertheless, calcium appears to represent a key mediator of these beneficial effects. Importantly, the source of calcium seems to be a critical determinant. In a study by Shin BR et al., a paradoxical finding was reported, whereby obese males with the highest calcium intake who did not consume dairy products showed an increased incidence of MetS [34]. This observation suggests that both the dietary source of calcium and obesity status may significantly modify the association between calcium intake and MetS risk. This factor should therefore be carefully considered when interpreting associations between calcium intake and metabolic outcomes. Whether calcium supplementation can replicate the beneficial effects observed with dietary calcium remains unclear, and the optimal supplemental dose has yet to be established. Moreover, although higher dietary calcium intake has been associated with a reduced risk of metabolic syndrome in several studies, elevated serum calcium concentrations have conversely been linked to an increased likelihood of developing metabolic syndrome [51]. This apparent discrepancy suggests that the metabolic effects of calcium may depend on its dietary source and physiological regulation rather than on total systemic calcium levels alone. Collectively, these findings underscore the importance of promoting an overall healthy dietary pattern rather than reliance on isolated nutrient supplementation. Consistent with the previous literature, the present meta-analysis confirms that higher total dietary calcium intake and dairy consumption are inversely associated with the risk of individual components of metabolic syndrome [13,15]. Furthermore, the protective effect of dietary calcium appears to be more pronounced for blood pressure and lipid profiles. Several studies have reported that dairy foods may exert beneficial effects on blood pressure [17]. The beneficial effects of dairy foods on metabolic syndrome may extend beyond their calcium content and may be attributed to the complex dairy matrix, likely reflecting the combined action of bioactive peptides, whey proteins, specific fatty acids, vitamins, and fermentation-derived compounds that can favorably modulate insulin sensitivity, blood pressure, inflammation, and gut microbiota composition [52]. In particular, adequate calcium intake has been shown to modulate the renin–angiotensin–aldosterone system and improve the sodium–potassium balance, thereby contributing to blood pressure reduction [53]. Blood pressure is tightly regulated by intracellular calcium concentrations in vascular smooth muscle cells, which influence vasoconstriction and vascular tone. Low dietary calcium intake appears to activate multiple hypertensive mechanisms, including increased secretion of the parathyroid hormone, which elevates intracellular calcium directly and via calcitriol activation, and stimulation of the renin–angiotensin–aldosterone system, leading to enhanced sodium and water reabsorption and subsequent expansion of vascular volume [54]. Increased dietary calcium reduces intracellular Ca^2+^ influx in adipocytes, thereby decreasing fatty acid synthesis and enhancing lipolysis, which results in reduced triglyceride storage. Moreover, calcium, which is abundant in milk and yogurt, can bind fatty acids and bile acids in the intestine, increasing fecal fat excretion and inhibiting lipid reabsorption [16]. Consequently, higher calcium intake may contribute to an improvement in the HDL-cholesterol to LDL-cholesterol ratio [16,18] and a reduction in fat mass, particularly in females [55]. However, despite the aforementioned positive effects of dietary calcium intake on the various components of the metabolic syndrome, studies that have evaluated the relationship between calcium intake and cardiovascular diseases such as stroke and coronary syndromes have reported inconclusive results [56]. Beyond lipid metabolism, calcium may exert additional benefits through its effects on oxidative stress and inflammation. Both oxidative stress and chronic low-grade inflammation are recognized as key contributors to the development and progression of metabolic syndrome [57]. Evidence suggests that adherence to a Mediterranean dietary pattern and higher dietary calcium intake may exert antioxidant effects, providing an additional layer of protection against MetS [58]. From a nutrigenomic perspective, the role of calcium appears particularly relevant. Nutrigenomics, which investigates interactions between nutrients and genetic variants, has shown that dietary patterns, such as high-fat diets, can modulate genetic susceptibility to MetS [59]. In a study conducted in a Korean population, Kim et al. reported that higher calcium intake attenuated the risk of MetS among carriers of the minor alleles of rs6445834 in the ARHGEF3 gene, rs10850335 in the TBX5 gene, and rs180349 in the BUD13 gene [30]. These findings suggest that calcium intake may interact with specific genetic profiles to influence metabolic health outcomes, highlighting its potential role in personalized nutrition strategies.
Several limitations of this study should be acknowledged. First, all included studies were cross-sectional, which precludes causal inference and allows for potential residual confounding and reverse causation. Second, moderate-to-substantial heterogeneity was observed, likely reflecting differences in study populations, dietary assessment methods, and confounder adjustment. Third, calcium intake was primarily assessed using self-reported dietary instruments, which are inherently prone to measurement error. Fourth, evidence of small-study effects was detected in the analysis of dairy consumption, which may have led to an overestimation of effect sizes. Fifth, since the study did not report results based on identical covariate models, standardizing the adjustment across studies was not feasible. Finally, the predominance of studies conducted in Asian and Western populations may limit the generalizability of the findings to other ethnic and geographic groups. This systematic review and meta-analysis also has several notable strengths. First, it is based on a large overall sample size, providing high statistical power and precise effect estimates. The inclusion of studies assessing both total dietary calcium intake and calcium derived from dairy products allowed evaluation of different dietary sources of calcium. Most included studies were of moderate-to-high methodological quality and involved apparently healthy adults, reducing the likelihood of disease-related reverse causation. The consistency of inverse associations across several components of metabolic syndrome, particularly blood pressure and HDL cholesterol, supports the biological plausibility of the findings. Additionally, the use of random-effects models and multiple approaches to assess publication bias enhanced the robustness and generalizability of the results.
5. Conclusions
In conclusion, this systematic review and meta-analysis provides robust evidence of an inverse association between dietary calcium intake and metabolic syndrome in adults, with a more pronounced protective effect in women. Evidence suggests that calcium is a key mediator of the beneficial effects of dairy products on metabolic health, particularly on blood pressure and lipid profiles. Biological plausibility is supported by mechanisms involving lipid metabolism, blood pressure regulation, inflammation, and gene–diet interactions. However, the cross-sectional nature of the included studies precludes any inference of causality between calcium intake and MetS. Well-designed prospective and interventional studies are warranted to clarify whether this relationship is causal and to define optimal dietary recommendations. Overall, these findings support recommendations promoting adequate calcium intake from foods within healthy dietary patterns, given its potential contribution to a lower risk of metabolic syndrome and better cardiometabolic health.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Reaven G.M. Banting Lecture 1988. Role of insulin-resistance in human disease Diabetes 1988371595160710.2337/diab.37.12.15953056758 · doi ↗ · pubmed ↗
- 2Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults Executive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III)J. Am. Med. Assoc.20012852486249710.1001/jama.285.19.248611368702 · doi ↗ · pubmed ↗
- 3Obunai K. Jani S. Dangas G.D. Cardiovascular morbidity and mortality of the metabolic syndrome Med. Clin. N. Am.2007911169118410.1016/j.mcna.2007.06.00317964915 · doi ↗ · pubmed ↗
- 4Noubiap J.J. Nansseu J.R. Lontchi-Yimagou E. Nkeck J.R. Nyaga U.F. Ngouo A.T. Tounouga D.N. Tianyi F.L. Foka A.J. Ndoadoumgue A.L. Geographic distribution of metabolic syndrome and its components in the general adult population: A meta-analysis of global data from 28 million individuals Diabetes Res. Clin. Pract.202218810992410.1016/j.diabres.2022.10992435584716 · doi ↗ · pubmed ↗
- 5Hirode G. Wong R.J. Trends in the prevalence of metabolic syndrome in the United States, 2011–2016 J. Am. Med. Assoc.20203232526252810.1001/jama.2020.4501 PMC 731241332573660 · doi ↗ · pubmed ↗
- 6Cicero A.F. Dormi A. D’Addato S. Gaddi A.V. Borghi C. Long-term effect of a dietary education program on postmenopausal cardiovascular risk and metabolic syndrome: The Brisighella Heart Study J. Womens Health 20101913313710.1089/jwh.2008.126820088669 · doi ↗ · pubmed ↗
- 7Esposito K. Marfella R. Ciotola M. Di Palo C. Giugliano F. Giugliano G. Armiento P. Giugliano D. Effect of a Mediterranean-style diet on endothelial dysfunction and markers of vascular inflammation in the metabolic syndrome: A randomized trial J. Am. Med. Assoc.20042921440144610.1001/jama.292.12.144015383514 · doi ↗ · pubmed ↗
- 8Kastorini C.M. Milionis H.J. Esposito K. Giugliano D. Goudevenos J.A. Panagiotakos D.B. The effect of Mediterranean diet on metabolic syndrome and its components: A meta-analysis of 50 studies and 534,906 individuals J. Am. Coll. Cardiol.2011571299131310.1016/j.jacc.2010.09.07321392646 · doi ↗ · pubmed ↗