Family Support in Healthy Dietary Behaviours Among Community-Dwelling Older Adults: A Scoping Review
Pui Ying Mak, Stefanos Tyrovolas, Justina Yat Wa Liu

TL;DR
This review explores how family support affects healthy eating in older adults living independently, highlighting the importance of shared meals and communication.
Contribution
The study provides a comprehensive synthesis of how family support influences dietary behaviors in older adults, emphasizing contextual and relational factors.
Findings
Family support, including shared meals and encouragement, is linked to better diet quality and adherence.
The impact of family support depends on relationship dynamics, communication, and cultural expectations.
Abstract
Background: Healthy dietary behaviours are essential for maintaining health, functional independence, and quality of life in later life. Family members are a key source of social support for community-dwelling older adults, yet the ways in which family support shapes older adults’ dietary behaviours, particularly among those who retain autonomy, remain insufficiently synthesized. Therefore, this review aims to map how family support influences dietary behaviours among community-dwelling older adults by examining the forms, roles, and contextual influences of family support within a Social Support Theory framework. Methods: Following Joanna Briggs Institute guidance and PRISMA-ScR reporting standards, we conducted a scoping review of empirical studies published in English or Chinese. Searches were conducted across PubMed, CINAHL, PsycINFO, Web of Science, and Scopus from inception to…
Click any figure to enlarge with its caption.
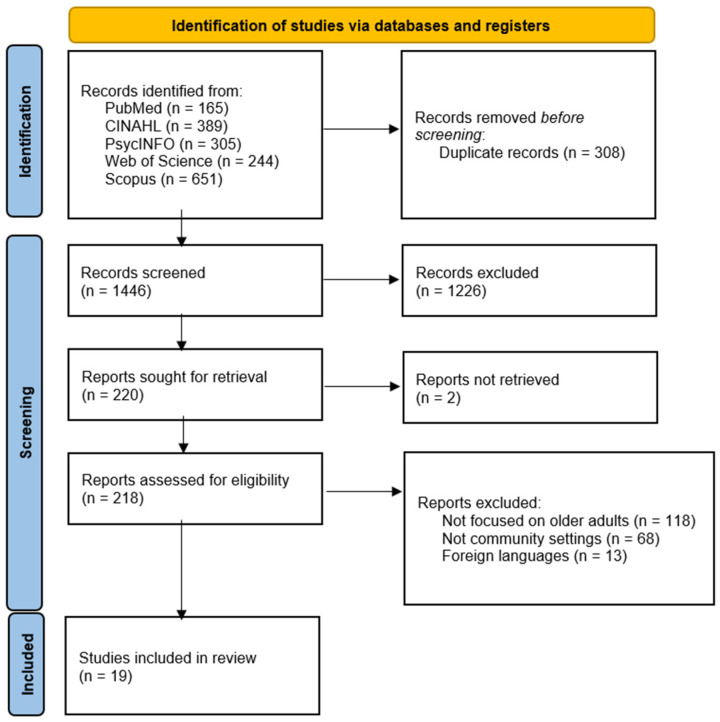 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNutritional Studies and Diet · Nutrition and Health in Aging · Health disparities and outcomes
1. Background
Globally, populations are ageing at an accelerating rate, resulting in a growing number of older adults living with chronic conditions and functional decline [1]. Healthy dietary behaviours, including balanced food choices, appropriate meal patterns, and quality diets, play a critical role in maintaining health, functional independence, and quality of life in later life [2,3]. Conversely, unhealthy dietary behaviours among older adults, such as inadequate protein intake and low consumption of fruits and vegetables, are associated with adverse outcomes, including malnutrition, cardiovascular disease, sarcopenia, frailty, diabetes mellitus, and increased healthcare utilization [4,5]. Maintaining healthy dietary behaviours is therefore essential for community-dwelling older adults to support healthy ageing and prevent nutrition-related morbidity [3,5].
Dietary behaviours in older adulthood are shaped by a complex interaction of individual, social, and environmental factors. Age-related physiological changes, declining appetite, chronic illness, and functional limitations may reduce dietary intake or compromise diet quality [2,6]. Age-related sensory decline, including reduced taste and smell sensitivity, may reduce appetite and food enjoyment, while oral health problems and swallowing difficulties may limit food variety and protein intake [7,8]. Polypharmacy and chronic disease management may further affect appetite, gastrointestinal comfort, and nutrient absorption [9]. Psychological factors such as depression, loneliness, and bereavement are also prevalent in later life and have been associated with irregular meal patterns and reduced dietary quality [10]. These multifaceted challenges of maintaining healthy dietary behaviours in older adulthood are closely tied to broader life transitions and contextual circumstances, making sustained healthy eating particularly complex. At the same time, social circumstances, such as living arrangements, social isolation, and inadequate social support networks, can further influence food choices, meal preparation, and eating patterns [11,12]. Among these social factors, the family represents a key source of support for many older adults living in the community [13].
Family involvement is increasingly recognized as an important determinant of health behaviours across the life course [13]. Drawing on Social Support Theory, family support can be conceptualized as encompassing emotional support (e.g., encouragement and reassurance), instrumental support (e.g., assistance with shopping, cooking, or meal preparation), informational support (e.g., advice or knowledge sharing), and appraisal support (e.g., feedback and reinforcement) [14,15]. Social Support theory was selected because it explicitly conceptualizes health behaviours as embedded within interpersonal relationships and distinguishes multiple functional types of support, making it particularly suitable for examining how family interactions shape everyday dietary practices. For community-dwelling older adults, family members may influence dietary behaviours directly through practical assistance or indirectly through shared beliefs, expectations, and social norms surrounding food and health.
The role of family support in shaping dietary behaviours among children and adolescents’ chronic conditions has been extensively examined in previous studies. For example, a systematic review of 39 randomized controlled trials found that family-based nutrition interventions for children with obesity were associated with improvements in dietary behaviours, including reduced energy intake and healthier food choices, compared with interventions without family involvement [16]. In addition, a global systematic review of 48 qualitative studies identified key family-related mechanisms influencing the eating behaviours of adolescents, such as parental modelling, family motivation, food-related rules, and parenting styles that shaped knowledge, attitudes, and practices toward healthy eating [17]. However, the relevance and manifestation of family support may differ substantially in older adulthood. Older adults typically retain greater autonomy over food-related decisions compared with children, while also facing unique age-related challenges such as declining physical capacity, widowhood, and changes in household composition [18,19,20]. Consequently, the forms of family involvement that support healthy dietary behaviours in later life may differ in nature, intensity, and acceptability from those in earlier life [12,21].
Despite growing interest in family-centred approaches to promoting health, the role of family involvement in influencing dietary behaviours among community-dwelling older adults remains underexplored. Existing reviews have largely focused on caregiver-led nutritional interventions targeting malnutrition or frailty, often emphasizing education provided to informal caregivers rather than the dynamic interaction between older adults and their family members, such as negotiation around food choices, shared decision-making, everyday communication about eating, and adaptations to changing functional or social circumstances [22,23]. Moreover, many studies prioritize clinical outcomes rather than examining how family roles, support processes, and relational contexts shape everyday dietary behaviours [6,24]. There is also limited synthesis of the barriers and facilitators influencing family involvement, such as cultural expectations, older adults’ desire for independence, family availability, and interpersonal dynamics [25,26].
Given the heterogeneity of family structures, living arrangements, and cultural contexts, a comprehensive mapping of the existing evidence is needed to clarify how families influence dietary behaviours among community-dwelling older adults. A scoping review is particularly appropriate to examine the breadth of study designs, conceptual frameworks, and methodological approaches used in this field, and to identify gaps in current knowledge [27,28].
Therefore, the aim of this scoping review is to map how family support shapes dietary behaviours among community-dwelling older adults by examining the forms, roles, and contextual influences of family support within a Social Support Theory framework. The findings from a synthesis of the existing evidence can inform the development of family-inclusive strategies to support healthy dietary behaviours and promote healthy ageing in the community.
2. Methods
This scoping review follows the framework of Arksey and O’Malley [29] as advanced by Levac et al. [30] and the guidance for scoping reviews from the Joanna Briggs Institute (JBI). This review was also conducted and reported in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) [28]. Our protocol is available on the Open Science Framework (https://doi.org/10.17605/OSF.IO/7EPVQ).
2.1. Eligibility Criteria
The inclusion and exclusion criteria were established based on the PCC (participants, concept, context) framework.
2.1.1. Types of Participants
This scoping review includes studies involving community-dwelling older adults aged 60 years or above, as defined by the World Health Organization (WHO) as the threshold for an ageing population [1]. Older adults with diverse health profiles have been included, ranging from those in robust health to those with chronic conditions such as hypertension or diabetes but who retain autonomy in making daily dietary choices. Studies examining older adults and their family members, where family support is directly or indirectly related to dietary behaviours, have been included to capture the role of family support in promoting positive dietary habits. Studies focusing solely on caregivers without the direct involvement of older adults in the intervention have been excluded. No restrictions were applied to other demographic variables (e.g., gender, ethnicity, socioeconomic status) to ensure inclusivity of relevant studies.
2.1.2. Concept
The core concept of this scoping review is family support in influencing healthy dietary behaviours among community-dwelling older adults. Family support is broadly defined to encompass both the active engagement of family members, including in giving emotional, informational, or instrumental support such as offering encouragement, help with meal preparation and grocery shopping, or in participating in shared meal practices; and family-related contextual factors such as living arrangements, the presence of a spouse, or the frequency of family contact, which may influence the dietary behaviours or nutritional status of older adults [10]. Studies were eligible for inclusion if they investigated how family members support or influence older adults’ dietary behaviours, food choices, or nutritional outcomes; examined relationships between family-related factors (e.g., cohabitation, family communication, or spousal support) and older adults’ diet quality or nutritional health; or explored facilitators and barriers affecting the ability of family members to support healthy eating among older adults. For this review, healthy dietary behaviours refer to eating practices that promote health and prevent disease, as characterized by adequate nutrient intake, balanced food choices, and limited consumption of harmful substances [31]. Nutritional outcomes encompass measures of diet quality, nutritional status, and related health indicators among older adults [2].
2.1.3. Context
This scoping review includes studies conducted in community settings, where older adults have autonomy over their food choices, preparation, or consumption. Excluded were studies conducted in hospitals or long-term care facilities where dietary autonomy may be limited. Studies from any country were eligible, in order to provide a global perspective on family involvement in nutritional interventions for older adults. No restrictions were placed on cultural, socioeconomic, or geographic contexts to maximize the breadth of relevant findings.
2.1.4. Types of Studies
Both quantitative and qualitative studies, including observation studies, quasi-experimental studies, and experimental studies, were included. Studies published in English and Chinese were included, since there might be cultural differences in dietary behaviours [27]. No limitations were placed on the year of publication.
2.2. Search Strategy
A three-step search strategy was employed. The search strategy was reviewed in consultation with a librarian. The first step was the initial search in PubMed and CINAHL. An analysis was conducted on the words included in the title, abstract, and keywords of the retrieved papers. Second, we searched through all of the selected databases for all words and keywords deemed to be relevant. Third, the reference lists of the selected papers were also screened for other possible related articles. The finalized search strategy is shown in Supplementary Material File S1. The search was conducted with Boolean operators (AND and OR). Free text and MeSH terms, whenever appropriate, were used. The selected electronic databases were: PubMed, CINAHL, PsycINFO, Web of Science, and Scopus. Databases were searched from inception to the year 2025.
2.3. Study Selection
Endnote 21 was used to manage the references, and duplications were removed. Study selection consisted of two phases. First, the two reviewers (PYM and JYWL) independently screened the titles, abstracts, and keywords of the paper to identify articles that seemed to meet the eligibility criteria. When there were disagreements over the results, the two reviewers engaged in a discussion to reach a consensus. The second phase involved retrieving and evaluating the full texts of those preliminarily selected studies in order to determine the final inclusion of articles. A flow chart was created according to the PRISMA guidelines to depict the selection process.
2.4. Data Extraction
Data extraction was conducted using a standardized extraction form developed by the review team to systematically capture pertinent information aligned with the aim of the review. Two independent reviewers (PYM and JYWL) extracted data from each included study, with discrepancies resolved through discussion or consultation with a third reviewer when necessary to ensure consistency and accuracy.
The extraction form captured core study details, including author(s), publication year, study design, aims and objectives, study setting, and population characteristics such as sample size and mean age, as well as family and social support variables. In addition, outcome data related to dietary behaviours and nutritional practices (e.g., food choices, meal patterns, diet quality, or dietary adherence) were collected for quantitative studies. For qualitative studies, data describing family roles, perceived facilitators and barriers to family involvement, and contextual influences on the dietary behaviours of older adults were extracted. Reported study limitations were also documented. This structured extraction process enabled a systematic comparison to be conducted across study designs and supported a subsequent quantitative summarization, qualitative thematic analysis, and integrative interpretation of the findings.
2.5. Critical Appraisal
The methodological quality of the included studies was assessed using the Joanna Briggs Institute (JBI) Critical Appraisal tools appropriate to each study design. Separate JBI checklists were applied for randomized controlled trials, quasi-experimental studies, cross-sectional studies, cohort studies, longitudinal studies, qualitative studies, and mixed-methods studies [32,33,34,35,36]. For the mixed-methods study, the qualitative and quantitative components were appraised independently using the corresponding JBI checklists. Two reviewers (PYM and JYWL) independently conducted the critical appraisal of all of the included studies. Any discrepancies in appraisal were resolved through discussion among the entire research team to achieve a consensus.
2.6. Reporting the Data
The reporting and synthesis of the data were undertaken by PYM. Data synthesis followed a convergent–segregated mixed-methods design, consistent with JBI guidance for integrating quantitative and qualitative evidence [37]. Quantitative data from observational, quasi-experimental, and randomized controlled trials, and the quantitative components of mixed-methods studies) were summarized descriptively according to study design, family support type, and outcome measures.
Qualitative data from qualitative studies and the qualitative components of mixed-methods studies were synthesized using a theory-informed deductive thematic approach guided by Social Support Theory [15]. Rather than conducting line-by-line coding, the qualitative findings were mapped against four domains of social support: instrumental, informational, emotional, and esteem support, to identify recurring patterns, facilitators, and barriers in family roles.
The quantitative and qualitative syntheses were then triangulated narratively to identify convergence and complementarity between quantitative outcomes and qualitative insights [38]. This integration provided a holistic understanding of how different forms and qualities of family support influence dietary behaviours among older adults across diverse cultural and contextual settings.
3. Results
3.1. Literature Selection Process
A PRISMA flow diagram of each stage of the literature search is given in Figure 1. The initial search of eight databases yielded a total of 1754 publications. After the removal of duplicates, 1446 publications remained. These were screened based on their titles and abstracts, and 1226 were excluded. Of the remaining 220 articles, the full texts of 218 articles were screened, while the full texts of 2 articles could not be retrieved. Of the 218 articles, 198 did not meet the eligibility criteria for the following reasons: (a) the focus was not on older adults (n = 118); (b) the study did not involve a community setting (n = 68); (c) the study was in a language other than English (n = 13). In the end, 19 publications met our eligibility criteria and were included for analysis.
3.2. Methodological Quality
All of the included studies (n = 19) underwent critical appraisal using the appropriate JBI tools according to the study design (Table 1, Table 2, Table 3, Table 4, Table 5 and Table 6). Overall, the methodological quality of the evidence was acceptable, with most studies meeting the majority of the appraisal criteria.
Among the cross-sectional studies, most clearly defined the inclusion criteria, described the study settings and participants in detail, and used appropriate methods of statistical analysis [12,40,42,44,45]. However, several studies showed limitations related to exposure measurements and confounding controls, with unclear or absent strategies to address confounders reported in the studies by Ong et al. [39], Watanabe et al. [43], Chung et al. [46], and Schoenberg [47].
The single cohort study demonstrated strong methodological quality, meeting nearly all appraisal criteria, including valid exposure and outcome measurements, the identification and management of confounders, and an appropriate method of statistical analysis [48]. The longitudinal study also met most criteria, although it was unclear whether the participants were consecutively included [24].
The randomized controlled trial showed appropriate randomization and statistical analysis; however, it was unclear whether or not the participants, intervention providers, and outcome assessors were blinded, reflecting common challenges in behavioural and dietary interventions [49]. Among the quasi-experimental and pretest–posttest studies, most demonstrated a clear causal direction, consistent outcome measurements, and appropriate analyses, although one study lacked a control group [50], and the reliability of the outcome measurements was unclear in others [51,52].
The qualitative studies generally demonstrated strong congruity between the methodology, data collection, analysis, and interpretation; and the participants’ voices were well represented across the studies [47,53,54,55]. Nonetheless, reflexivity was limited, with none of the studies explicitly addressing researcher influence, and statements locating the researchers culturally or theoretically were unclear across all of the qualitative studies. Ethical approval was reported in Beverly et al. [54] and Choi et al. [55], while it was unclear whether such approval had been obtained in the studies of Gallant et al. [53] and Schoenberg [47].
3.3. Characteristics of the Included Studies
We identified 19 empirical studies that met our inclusion criteria and examined family roles in influencing dietary behaviours among community-dwelling older people. The evidence base comprised heterogeneous study designs, including twelve quantitative observational studies, three quasi-experimental or pretest–posttest interventions, one randomized controlled trial, three qualitative studies, and one mixed-methods study. Most studies were conducted in Asia (South Korea, Japan, Thailand, Singapore, and Indonesia) and North America (United States), with one that involved rural African American communities. Sample sizes ranged from small qualitative groups (~30–100 participants) to large observational samples (e.g., community national dataset analyses and samples comprising >300–400 participants) [39,42,46]. Populations included both healthy older adults [12,39] and older adults with chronic conditions including type 2 diabetes [24,40,43,50,53,54,55], heart failure [46], colorectal cancer [44,45], and hypertension [47,49].
Table 7, Table 8, Table 9 and Table 10 summarize the characteristics and key findings of the quantitative studies (n = 15), and Table 11 and Table 12 present information from the qualitative and mixed-methods studies (n = 4).
3.4. Narrative Synthesis of Quantitative Findings
Across the 15 quantitative studies that were included, diverse forms of family support were identified and mapped under the domains of the Social Support Theory: instrumental, emotional, informational, and esteem support. These studies collectively examined how family members influenced older adults’ dietary adherence, nutritional knowledge, and dietary-related behaviours in community settings or outpatient contexts. The majority of the evidence demonstrated that family support, particularly instrumental and emotional support, was positively associated with improved diet quality and better nutritional outcomes. However, the results were not consistent across the studies, as the strength and direction of these effects varied by gender, cultural norms, and the quality of support.
3.4.1. Outcome Measures
Dietary and nutrition-related outcomes were measured using a wide range of self-reported and objective tools, including the Nutrition Knowledge Index [39], Diet Quality Index [44,45], Health-Promoting Lifestyle Profile—Nutrition Subscale [41], Elder Healthy Eating Scale [51], and 3-day food records [50]. Across the included studies, these tools assessed both specific targeted dietary behaviours and broader dietary practices. Specific behaviours included changes in nutrient intake and food choices, such as sodium reduction (measured by 24h urinary sodium excretion [46,49]), increased fruit and vegetable intake (reflected by serum carotenoids [48]), and protein intake (assessed via food records [50]). Broader practices encompassed adherence to healthy eating guidelines and overall diet quality (measured by diet quality indices [44,45] and the Elder Healthy Eating Scale [51]). Additional objective and biochemical measures included metabolic or clinical indicators such as HbA1c, triglycerides, BMI, cholesterol, and cardiac risk scores [40,43]. Broader health-related outcomes such as quality of life, depression, and self-esteem were also reported [41,52]. The outcome measured in the included studies captured multiple dimensions of diet-related behaviour and well-being among older adults.
3.4.2. Instrumental Support: Shared Meal Preparation, Cooking, and Co-Adherence
Instrumental support, which refers to the tangible actions that family members took to help with food-related behaviours, was the most consistently reported domain. Across studies, family members engaged in meal planning, grocery shopping, cooking, and shared adherence to dietary restrictions [43,51]. Older adults who received such support generally demonstrated higher diet quality and adherence. For instance, when family members jointly followed a low-sodium diet, patients with heart failure or hypertension exhibited significantly lower 24 h urinary sodium excretion and were up to four times more likely to adhere to dietary recommendations than those without shared adherence [46,49]. Similarly, caregivers’ own healthy eating practices, such as increasing the consumption of vegetables and cutting down on foods high in sugar or fat, were associated with better diet quality and nutrient intake among colorectal cancer survivors [44]. A study conducted in rural Thailand, which involved family members in meal preparation and education sessions, led to significant improvements in the healthy eating scores of older people both one week and 12 weeks after the programme [51]. In a study conducted in Indonesia, a family-inclusive programme combining joint education and cooking sessions improved compliance to a low-salt diet and reduced levels of urinary sodium [49]. These findings suggest that the active engagement of family members in shared food-related tasks is a key facilitator of sustained dietary change.
3.4.3. Emotional and Esteem Support: Encouragement, Autonomy, and Motivation
Emotional and esteem support, such as giving encouragement, showing empathy, and building confidence, emerged as another crucial influence on dietary behaviour. A study conducted by Lee et al. [40] found that older adults who perceived autonomy-supportive behaviours from their family or friends showed higher adherence to healthy diets and exercise. Similarly, older adults living with family members reported better nutrition behaviours, self-esteem, and overall health-promoting practices compared with those living alone [41].
However, the quality and tone of the emotional support that was provided determined whether its influence was positive or negative. In a study involving couples who were managing type 2 diabetes, supportive and collaborative spousal behaviours were associated with improved dietary adherence, whereas critical or controlling interactions led to lower adherence and higher levels of distress [24]. This indicates that emotional support functions effectively when autonomy and partnership are respected, but can become a barrier when it manifests as coercion or pressure.
3.4.4. Informational Support: Guidance and Knowledge Sharing
Informational support, which includes providing knowledge, reminders, or practical advice, was a common but variably effective form of family involvement. In a study conducted in Singapore, older adults with access to help from family or friends showed higher scores in nutrition knowledge and were more likely to report that they understood nutritional information [39]. Two studies showed that family-based education and cooking programmes enhanced dietary knowledge among both older adults and their relatives [49,51]. However, one study indicated that passive or unsolicited advice [43] did not always translate into behavioural adherence, particularly when it was perceived as intrusive. This distinction suggests that informational support is most effective when family members are engaged as collaborative learners rather than as instructors.
3.4.5. Family-Inclusive Interventions and Broader Family Context
Several quasi-experimental and intervention studies demonstrated that structured family support directly contributed to improved dietary adherence and nutrition-related outcomes among community-dwelling older adults [49,50,51,52]. In Thailand, a family-involved nutrition education programme that trained older adults and their family members in healthy meal planning, preparation, and goal setting led to significant improvements in healthy eating scores at both the short-term and 12-week follow-ups [51]. Likewise, a community-based cooking programme that encouraged spouses or caregivers to participate alongside older adults with diabetes produced reductions in total energy, fat, and sodium intake and improvements in nutrient balance [50]. A randomized controlled trial in Indonesia further supported these findings, showing that joint education and cooking sessions with family members improved compliance with a low-salt diet and reduced salt concentration in food and urine compared to standard care [49].
Living arrangements and family proximity also influenced nutritional outcomes. Older adults living with family members, particularly spouses or adult children, reported higher levels of engagement in health-promoting dietary behaviours and a lower risk of malnutrition compared with those living alone [41,42]. Frequent contact with family members was also protective against poor nutritional status, whereas isolation or limited family interaction was associated with greater vulnerability to malnutrition. These findings suggest that beyond active caregiving or shared meal practices, the presence and accessibility of family members create a supportive social environment that enables sustained healthy dietary behaviours among older adults.
3.5. Thematic Synthesis of Qualitative Findings
Studies with qualitative and mixed-methods findings (n = 4) [47,53,54,55] provided depth to the qualitative data, illuminating the mechanisms and context through which family influence operates. Family support in older adults’ dietary behaviours manifested through all four domains of the Social Support Theory. Table 13 shows a thematic synthesis of family support domains mapped to the Social Support Theory framework.
3.5.1. Instrumental Support
Instrumental support encompassed practical involvement in food-related and health-related activities, including control over food preparation, shared food practices, dietary monitoring, and household assistance. Spouses, most often wives, frequently assumed responsibility for cooking and portion control, which facilitated dietary adherence but sometimes generated tension when older adults perceived a loss of autonomy or the presence of excessive control [53,54]. Collaborative practices such as joint grocery shopping, shared meal preparation, and the adoption of similar diets fostered mutual responsibility and cooperation within households [54,55].
However, instrumental support was not uniformly present. Some older adults, particularly African American participants, continued to prepare meals independently despite living with family members, reflecting limited reliance on household assistance [47]. Beyond food preparation, spouses also provided encouragement to exercise and accompaniment to medical appointments, reinforcing dietary adherence through broader health-related support [55].
3.5.2. Informational Support
Informational support involved dietary competence, exchanges of health information, and health awareness. Couples actively sought dietary information from healthcare professionals, books, and the media, which enhanced their knowledge and confidence in managing dietary changes [54]. Family members with health-related backgrounds often acted as informal advisors; however, unsolicited or conflicting advice sometimes undermined adherence [53,55].
In some cases, older adults demonstrated general awareness of dietary guidelines but relied primarily on self-initiated moderation and personal responsibility, rather than on ongoing family guidance [47].
3.5.3. Emotional Support
Emotional support was reflected in encouragement, empathy, emotional understanding, and emotional independence. Supportive communication, reassurance, and a sense of teamwork, particularly among couples managing chronic conditions, strengthened motivation and sustained dietary changes [54,55].
At the same time, emotional support was not always reciprocated or effective. Some participants, especially women, reported that their dietary concerns were not taken seriously by spouses, which reduced perceived support [55]. Others emphasized self-reliance and emotional independence, preferring to manage dietary behaviours without family involvement [47].
3.5.4. Esteem and Appraisal Support
Esteem and appraisal support operated through patterns of communication, recognition of competence, and inclusion in decision-making. Open communication and mutual problem-solving enhanced marital relationships and dietary adherence, whereas controlling language or avoidance undermined cooperation [54,55]. Older adults valued understanding and validation, particularly from peers or family members with similar health experiences; conversely, a lack of empathy from healthy relatives contributed to feelings of isolation [53].
3.5.5. Coping, Psychological Support, and Cultural Factors
Coping processes and cultural contexts further shaped family involvement in dietary behaviours. Couples often viewed chronic disease management as a shared challenge, with collaborative coping enhancing resilience and adherence [54,55]. However, overprotection, which manifested through excessive control, criticism, or nagging, sometimes undermined autonomy and self-efficacy, prompting older adults to rely instead on self-regulation and moderation strategies [47,53]. Cultural norms also influenced how support was enacted and interpreted. For example, Korean immigrant families experienced emotional and cultural strain when modifying traditional rice-based diets, whereas African American elders described culturally embedded beliefs around ageing and gradual dietary moderation [47,55].
Mapping these findings to the Social Support Theory framework reveals that while families are powerful enablers of healthy dietary behaviours, they can also inadvertently become barriers when practical or emotional support compromises autonomy or cultural identity.
These studies show that family support in dietary behaviour is complex, relational, and context-dependent rather than uniformly beneficial. Its effectiveness depends on the quality of interactions and the extent to which supportive behaviours align with the preferences, autonomy, and emotional needs of older adults. Supportive behaviours foster positive outcomes when they promote cooperation, mutual respect, and shared responsibility within families. Conversely, when family involvement becomes overly controlling, critical, or intrusive, it can undermine motivation and dietary adherence. The meaning and effect of support are also shaped by household relationships, communication patterns, and generational expectations within families.
3.6. Integrated Triangulation
The integrated synthesis of quantitative and qualitative evidence indicates that instrumental, emotional, and esteem support from family are most consistently associated with improved dietary behaviours in community-dwelling older adults, whereas informational support and overall family involvement show more context-dependent effects.
Quantitatively, instrumental support, such as shared meal preparation, assistance with grocery shopping, and family co-adherence to dietary recommendations, was linked to higher diet quality, better objective biomarkers (e.g., lower 24 h urinary sodium) [46,49], and improved dietary indices in family-engaged interventions [50,51]. Qualitative findings complemented the quantitative findings by showing that practical assistance facilitates healthy eating and fosters shared responsibility, although it can feel controlling when it undermines autonomy [53,54,55].
Emotional and esteem support emerged as central motivational mechanisms that facilitate sustained changes in behaviour. Quantitative studies showed that perceived autonomy-supportive behaviours from family or informal supporters were associated with higher adherence to healthy diets and greater patient activation [40,44], whereas observational studies documented poorer adherence when support took the form of pressure or criticism [24]. The qualitative findings further indicated that encouragement and respectful communication strengthened confidence and adherence, while nagging or patronizing behaviours reduced self-efficacy and sometimes led to covert non-adherence [47,53,54]. Together, these findings suggest that emotional tone and respect for autonomy shape whether family involvement supports or undermines dietary behaviours [24,43].
Informational support produced mixed outcomes across trials and observational studies. Family-inclusive education and hands-on cooking programmes increased nutrition knowledge and, in some cases, improved diet indicators [49,50,51], whereas passive advice or unsolicited tips did not reliably translate into behavioural adherence [43,47]. The qualitative findings indicate that information is more effective when shared collaboratively (e.g., learning or cooking together) rather than delivered as top-down instruction [54,55].
Contextual moderators, including living arrangement, frequency of family contact, and social participation, were supported by both quantitative and qualitative evidence. Large-sample analyses reported more active engagement in health-promoting behaviours and a lower risk of malnutrition among older adults with regular family contact or supportive co-residence arrangements [41,42], while longitudinal work linked social participation to better objective markers of diet quality [48]. The qualitative studies suggest that while proximity increases opportunities for shared meals and monitoring, it may also generate conflict when shaped by family norms, gender roles, or intergenerational tensions.
4. Discussion
4.1. Summary of the Findings
This mixed-methods scoping review mapped the nature and scope of family involvement in shaping healthy dietary behaviours among community-dwelling older adults, using a Social Support Theory framework. Across 19 empirical studies, family involvement was consistently associated with older adults’ dietary behaviours, although its effects were not uniformly positive. Instrumental and emotional/esteem support emerged as the most influential forms of family involvement, while informational support showed more variable effects. Importantly, findings drawn from both quantitative and qualitative studies converged to show that the quality of family support, particularly its respect for autonomy and collaboration, moderated whether family involvement facilitated or hindered dietary adherence. These findings suggest that family members function not merely as sources of assistance, but as key actors shaping the dietary environment, motivation, and sustainability of healthy eating in later life.
4.2. Interpretation of Findings and Comparison with Existing Literature
4.2.1. Instrumental Support and the Role of Co-Adherence
The importance of instrumental support observed in this review is consistent with the findings from the body of research on chronic illness and ageing, which highlights the role of family members in lowering practical obstacles to healthy behaviours. Previous studies have shown that family involvement facilitates health literacy, self-care engagement, and healthier behavioural patterns among older adults, thereby shaping the broader household environment in which dietary behaviours occur [56,57]. However, this review extends prior work by differentiating between passive assistance and active co-adherence. Evidence from the quantitative studies demonstrated that when family members adopted the same dietary practices, such as following a low-sodium or balanced diet alongside the older adult—dietary adherence and objective biomarkers improved. These findings suggest that “doing with” rather than “doing for” older adults normalizes dietary change within the household and reduces environmental temptations. This is consistent with broader evidence indicating that collaborative family engagement and shared decision-making enhance adherence and satisfaction with care among older adults [58]. Earlier reviews have largely focused on education-based interventions targeting individuals [59,60]; in contrast, the present synthesis highlights that shared household practices and co-adherence may be critical for sustaining changes in dietary behaviour, particularly in the context of the long-term self-management of chronic conditions.
4.2.2. Emotional and Esteem Support: Support Versus Social Control
This review has identified the boundary between supportive encouragement and counterproductive social control. While emotional involvement is frequently promoted in self-management interventions, the findings from both the quantitative and qualitative studies indicated that emotional support facilitated dietary adherence only when it respected autonomy. Studies measuring autonomy-supportive behaviours showed positive associations with diet adherence, patient activation, and reduced health risks [40], whereas another study reported poorer adherence when support took the form of pressure, criticism, or monitoring [24]. These findings resonate with previous studies suggesting that directive or coercive support may provoke behavioural reactance [61]. The qualitative findings further explained this mechanism, describing how nagging, overprotection, or patronizing communication diminished confidence and sometimes resulted in covert non-adherence [53,54]. Thus, emotional and esteem support appear to act as moderators that determine whether instrumental support is experienced as empowering or undermining.
4.2.3. Informational Support and Collaborative Learning
Informational support demonstrated more diverse effects across studies. Family-inclusive education and cooking programmes improved nutrition knowledge and, in some cases, dietary indicators in the included studies [49,51]. However, passive or unsolicited advice did not reliably translate into behavioural change in another included study [43]. These findings align with prior evidence suggesting that knowledge alone is insufficient to alter entrenched dietary habits [62]. The qualitative evidence in this review clarifies this inconsistency by showing that older adults are more receptive to information when it is shared collaboratively, through joint learning, shared meal preparation, or collective goal-setting, rather than delivered in a top-down or corrective manner [55]. Informational support appears to be most useful when shared within supportive family relationships and combined with practical food-related activities, rather than provided on its own.
4.2.4. Contextual Influences
The influence of family support on the dietary behaviours of older adults observed in this review is shaped by broader household and cultural contexts, and is largely consistent with research emphasizing that health behaviours are socially embedded rather than individually determined [63]. The population-based studies included in this review indicate that co-residence with family members or frequent family contact is associated with higher levels of engagement in health-promoting dietary behaviours and a lower risk of malnutrition [41,42], while greater social participation is linked to favourable objective dietary markers such as serum carotenoids [48]. These patterns can be understood in light of existing research showing that family roles and gendered divisions of food-related labour structure daily eating practices in later life, shaping both access to food and the social expectations surrounding eating [64,65,66]. In such contexts, family members often function as organizers of meals, gatekeepers of food choices, or monitors of dietary behaviour. This helps to explain why living arrangements and family proximity emerged as important correlates of dietary outcomes in this review. The findings from the qualitative studies add nuance by illustrating how contextual influences shape everyday dietary practices, rather than operating only at the level of caregiving norms. For example, shared living arrangements can increase opportunities for meal sharing and support, but they may also intensify tensions when cultural food norms or intergenerational expectations conflict with dietary recommendations [53,55]. Such tensions represent an important social challenge in multigenerational households and warrant greater attention in both research and practice [67]. The existing literature suggests that these conflicts are best managed through open communication, negotiation, and flexible meal practices that preserve older adults’ autonomy while accommodating household preferences [68]. Meal sharing does not necessarily require that all family members consume identical foods; rather, it may involve eating together while allowing variation in meal components [69]. For instance, in households where dietary preferences differ, families may prepare shared base dishes with optional additions, offer alternative protein sources, or rotate meal planning responsibilities to ensure that different preferences are respected over time. Research on autonomy-supportive family interactions indicates that collaborative decision-making and mutual respect are associated with better adherence and reduced relational strain, compared with rigid or controlling approaches [40].
Beyond these practical adaptations, a substantial body of family research demonstrates that successful navigation of dietary conflict depends on negotiation processes such as identifying and reconciling underlying interests, perspective-taking, shared problem-solving, and role flexibility within the household [70]. Studies of chronic illness management and intergenerational households have shown that families who engage in collaborative planning and explicitly discuss expectations are better able to align dietary goals with cultural traditions and personal preferences [71,72]. In contrast, unresolved tensions often arise when dietary changes are framed as unilateral prescriptions rather than shared adjustments [67]. By situating the present findings within this broader literature, it becomes clear that family-inclusive strategies must address relational dynamics directly rather than assuming that involvement alone will produce positive dietary outcomes.
Taken together, these findings suggest that the influence of family support on dietary behaviours is contingent on household dynamics and cultural context, which shape how support is enacted, interpreted, and translated into changes in dietary behaviour.
The findings of this review align conceptually with broader life-course research showing that family relationships influence dietary behaviours through relational quality, communication, and shared food practices. While most existing evidence comes from studying children and adolescents, the present review suggests that similar relational mechanisms remain relevant in later life, even when older adults retain autonomy over dietary decisions [73,74].
4.3. Strengths and Limitations
This scoping review has several strengths. First, it systematically mapped a diverse body of evidence from evidence drawn from quantitative and qualitative studies on family involvement in dietary behaviours among community-dwelling older adults. The inclusion of multiple study designs allowed for a comprehensive overview of how family roles, forms of support, and relational processes influence dietary behaviours across different contexts. Second, the review was guided by Social Support Theory, providing a theory-informed framework to categorize forms of family support and interpret findings in a structured and conceptually coherent manner. Third, a methodological appraisal of quality was undertaken using appropriate JBI critical appraisal tools, enabling transparent reporting of the strengths and limitations of the included evidence and supporting a cautious interpretation of the findings.
Several limitations should also be considered. As a scoping review, the primary aim was to map the breadth and nature of the existing evidence rather than to synthesize effect sizes or determine the effectiveness of interventions; therefore, conclusions regarding causality or comparative effectiveness cannot be drawn. Substantial heterogeneity across study designs, populations, outcome measures, and conceptualizations of family involvement limited direct comparison across studies and precluded the conducting of a meta-analysis. In addition, family involvement was variably defined and operationalized across studies, which may have influenced the consistency of the findings and limited the ability to draw unified conclusions on specific family roles. Finally, many of the included studies relied on self-reported dietary behaviours and family support measures, which may be subject to recall and social desirability bias. Moreover, dietary recommendations evolve over time as scientific evidence accumulates. As a result, the meaning of “healthy” dietary practices and the nature of family support aligned with these recommendations may vary across study periods and contexts. This dynamic may influence the interpretation and long-term applicability of the findings.
Despite these limitations, this review provides a comprehensive synthesis of the current evidence and highlights important gaps to inform future research and the development of family-inclusive dietary interventions for older adults in community settings.
4.4. Implications for Practice and Research
Globally, vertical households are becoming more prevalent, meaning that more older adults now share their living spaces with adult children or grandchildren [75]. In these shared family environments, family members play an increasingly important role in shaping everyday dietary practices [10]. The findings of this review are therefore particularly timely, as they provide insight into how family dynamics within these evolving household structures may influence healthy eating.
The findings of this review can inform the development of family-inclusive strategies to support healthy dietary behaviours and promote healthy ageing in community settings. Across the included studies, family involvement influenced dietary behaviours through practical assistance, encouragement, shared food-related practices, and communication patterns [43,45,47,54,55]. However, the review also shows that family involvement alone does not guarantee positive outcomes. Instead, the manner in which support is provided determines whether it facilitates or undermines dietary adherence. Approaches that actively engage family members while preserving the autonomy and decision-making capacity of older adults may enhance motivation, confidence, and the sustainability of dietary change.
These findings are consistent with prior interventional studies demonstrating that family-based programmes are most effective when they involve structured communication training, shared goal-setting exercises, and strategies for negotiating differences in food preferences [76,77,78]. The broader literature emphasizes that family members function not only as supporters or monitors but also as active participants in behavioural change [79,80]. Accordingly, family-inclusive strategies should include components that explicitly teach families how to manage disagreement constructively, adapt meals flexibly, and balance collective routines with individual dietary needs.
Practitioners designing family-inclusive dietary programmes should therefore consider strategies that help family members engage in ways that foster collaboration, mutual respect, and supportive communication instead of controlling or overprotective approaches. This relational perspective is particularly important in households where differing food preferences, cultural traditions, or health needs may create tensions around dietary change [81]. Supporting families to negotiate these differences constructively may help maintain both adherence and relational harmony [82].
Future research should go beyond documenting whether family support is present to examining how different family roles, interaction styles, and support processes shape dietary behaviours over time. Longitudinal and intervention studies conducted at the family or household level are needed to capture relational dynamics, negotiation of autonomy, and changes in support patterns as dietary practices evolve. By mapping how these relational processes operate specifically in the context of older adults’ dietary behaviours, the present review provides a conceptual foundation to guide future intervention design and policy development. Rather than proposing a specific programme, this synthesis highlights key relational mechanisms that should be considered when developing family-inclusive approaches to promote healthy dietary behaviours among older adults.
5. Conclusions
In conclusion, this scoping review demonstrates that family involvement exerts a central influence on dietary behaviours among community-dwelling older adults. Consistent with the broader literature on family and nutrition across the life course, instrumental support shapes the practical food environment, while emotional and relational support influences motivation and adherence. Family involvement is most effective when it transforms dietary management into a collaborative, respectful practice. These findings highlight the importance of designing family-engaged, autonomy-supportive strategies to promote healthy eating and well-being in later life.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1WHO Ageing and Health Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health(accessed on 15 November 2025)
- 2Ahmed T. Haboubi N. Assessment and management of nutrition in older people and its importance to health Clin. Interv. Aging 2010520721610.2147/cia.s 966420711440 PMC 2920201 · doi ↗ · pubmed ↗
- 3Clegg M.E. Williams E.A. Optimizing nutrition in older people Maturitas 2018112343810.1016/j.maturitas.2018.04.00129704915 · doi ↗ · pubmed ↗
- 4Mithal A. Bonjour J.P. Boonen S. Burckhardt P. Degens H. El Hajj Fuleihan G. Josse R. Lips P. Morales Torres J. Rizzoli R. Impact of nutrition on muscle mass, strength, and performance in older adults Osteoporos. Int.2013241555156610.1007/s 00198-012-2236-y 23247327 · doi ↗ · pubmed ↗
- 5Shlisky J. Bloom D.E. Beaudreault A.R. Tucker K.L. Keller H.H. Freund-Levi Y. Fielding R.A. Cheng F.W. Jensen G.L. Wu D. Nutritional considerations for healthy aging and reduction in age-related chronic disease Adv. Nutr.20178172610.3945/an.116.01347428096124 PMC 5227979 · doi ↗ · pubmed ↗
- 6Suominen M.H. Puranen T. Jyväkorpi S. Eloniemi-Sulkava U. Kautiainen H. Siljamäki-Ojansuu U. PitkaläK. Nutritional guidance improves nutrient intake and quality of life, and may prevent falls in aged persons with Alzheimer disease living with a spouse (Nu AD trial)J. Nutr. Health Aging 20151990190710.1007/s 12603-015-0558-026482691 PMC 12878907 · doi ↗ · pubmed ↗
- 7Li Y. Wang S. Zhang L. Dong Q. Hu X. Yang Y. Liu T. Wu B. Shan B. Yin C. Sensory insights in aging: Exploring the impact on improving dietary through sensory enhancement Food Sci. Nutr.202513 e 7007410.1002/fsn 3.7007440041711 PMC 11876084 · doi ↗ · pubmed ↗
- 8Spence C. Youssef J. Aging and the (chemical) senses: Implications for food behaviour amongst elderly consumers Foods 20211016810.3390/foods 1001016833467624 PMC 7830801 · doi ↗ · pubmed ↗