Pleiotropic Bioactivity of Caterpillar Fungus, Orange Cordyceps, and Cordycepin: Insight from Integrated Network Pharmacology and Food and Drug Regulatory Framework
Alexander Panossian

TL;DR
This review explores the health benefits of two medicinal fungi and their compounds, suggesting they support resilience through multiple biological pathways and proposes new regulatory frameworks.
Contribution
The paper introduces a regulatory category for resilience-supporting physiological modulators based on systems biology insights.
Findings
Common adaptogenic mechanisms in O. sinensis, C. militaris, and cordycepin support cellular and system homeostasis.
Pharmacokinetic data suggest cordycepin's effects may be indirect or systems-level despite low systemic concentrations.
Network pharmacology identifies key pathways like PI3K–Akt and NF-κB linked to immune and metabolic regulation.
Abstract
Background/Objectives: The medical mushroom Ophiocordyceps sinensis (Caterpillar Fungus), known for its ability to enhance “vitality,” is one of the most popular medicines in Asian traditional medical systems. According to the Chinese Pharmacopeia, O. sinensis is standardized for its adenosine content, the precursor of ATP, which mediates numerous physiological and pathological processes in many diseases. The related fungus of order Hypocreales, Cordyceps militaris, and its major bioactive constituents, 3′-deoxyadenosine (cordycepin), also exhibit pleiotropic biological activities. This review aims to provide a rationale for the adaptogenic and resilience-supporting effects of these medicinal fungi and to align food and drug regulation in Western countries. Methods: In this narrative review, we integrated results from chemical, pharmacokinetic, network pharmacology, preclinical, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
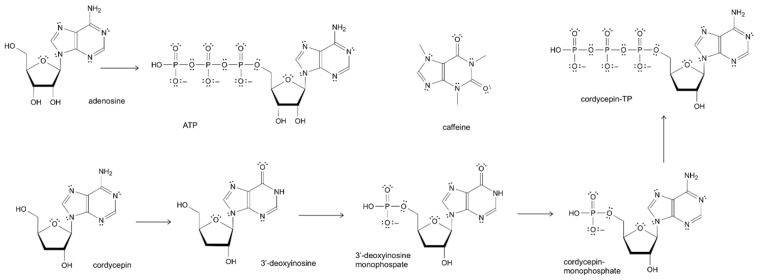 Figure 1
Figure 1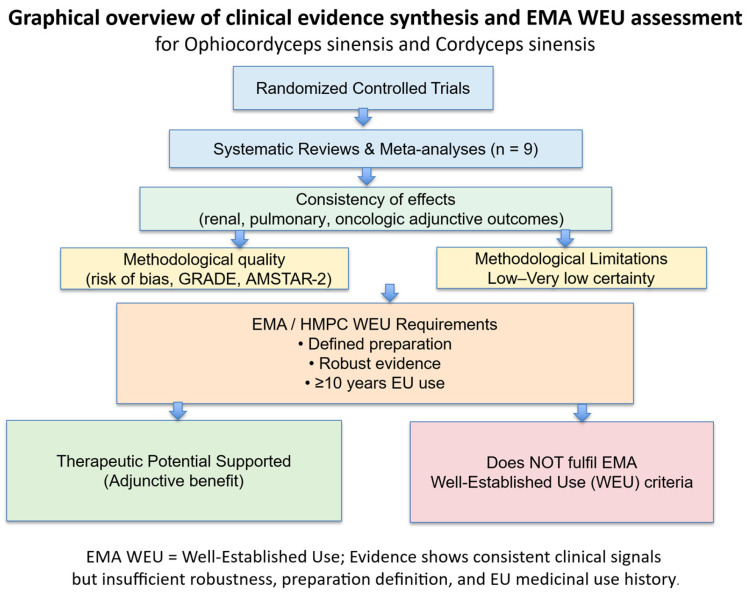 Figure 2
Figure 2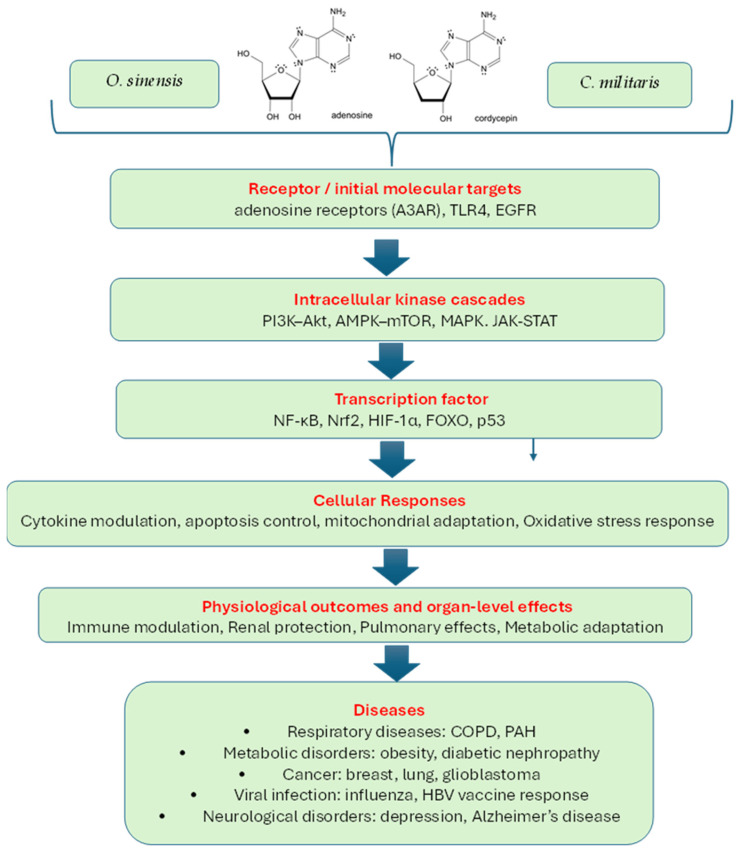 Figure 3
Figure 3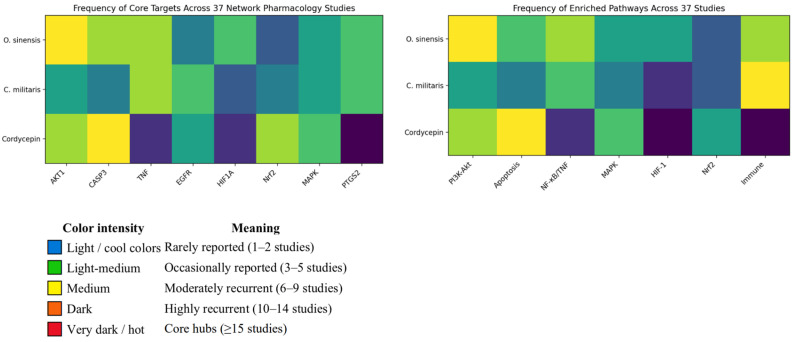 Figure 4
Figure 4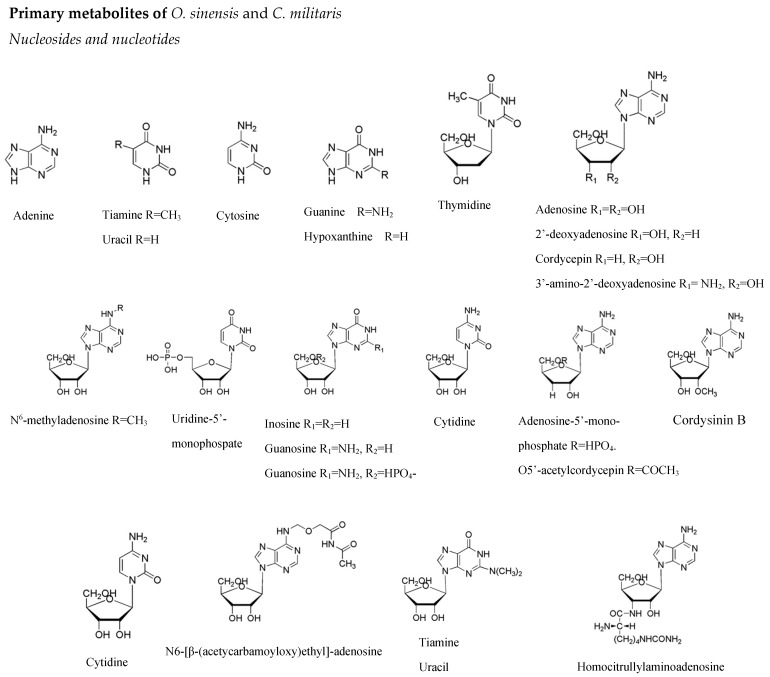 Figure 5
Figure 5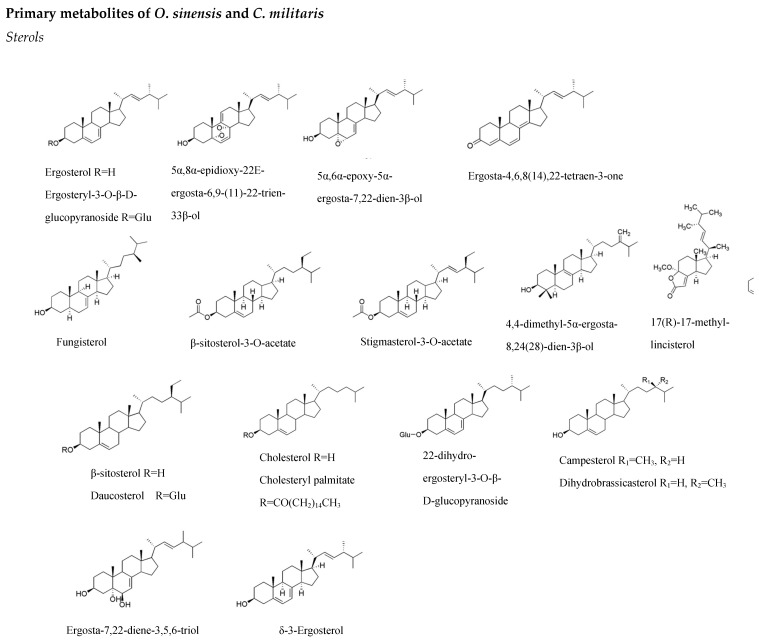 Figure 6
Figure 6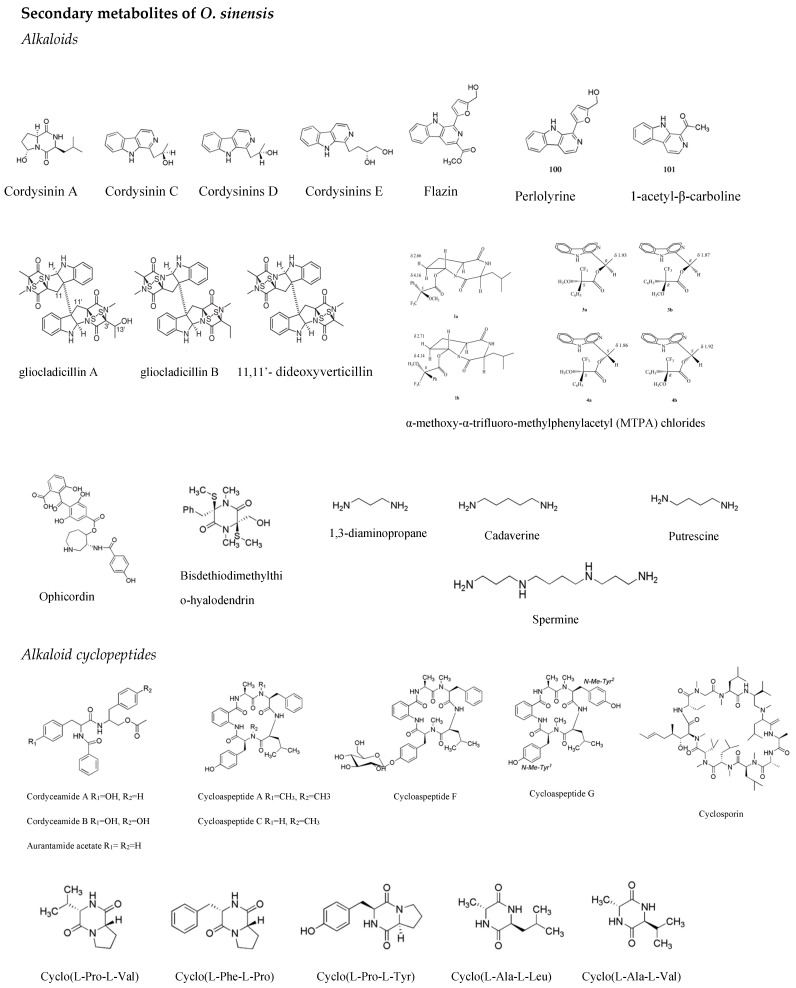 Figure 7
Figure 7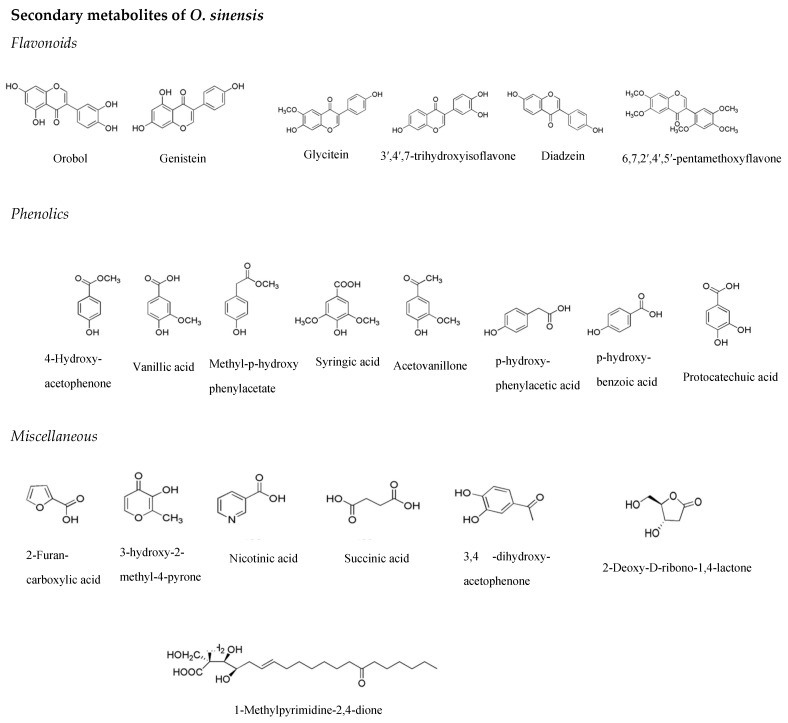 Figure 8
Figure 8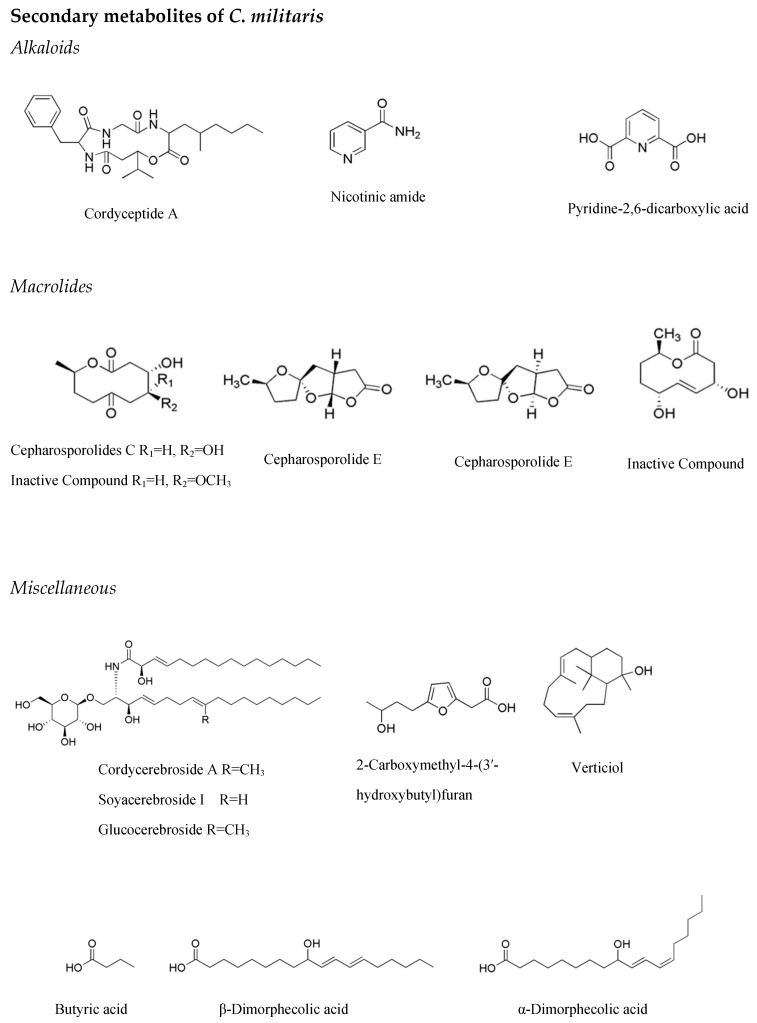 Figure 9
Figure 9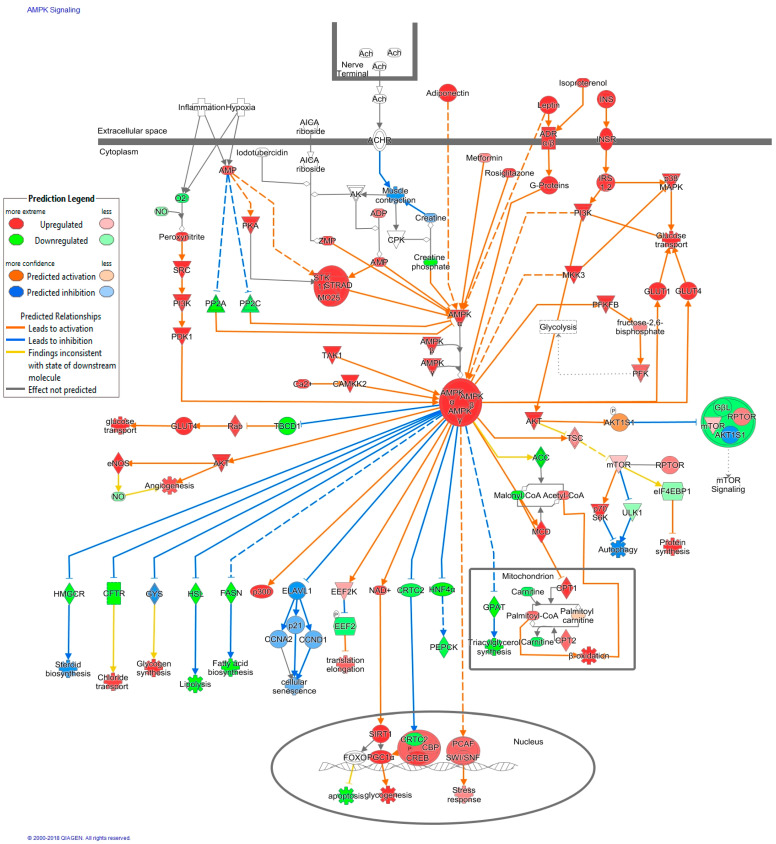 Figure 10
Figure 10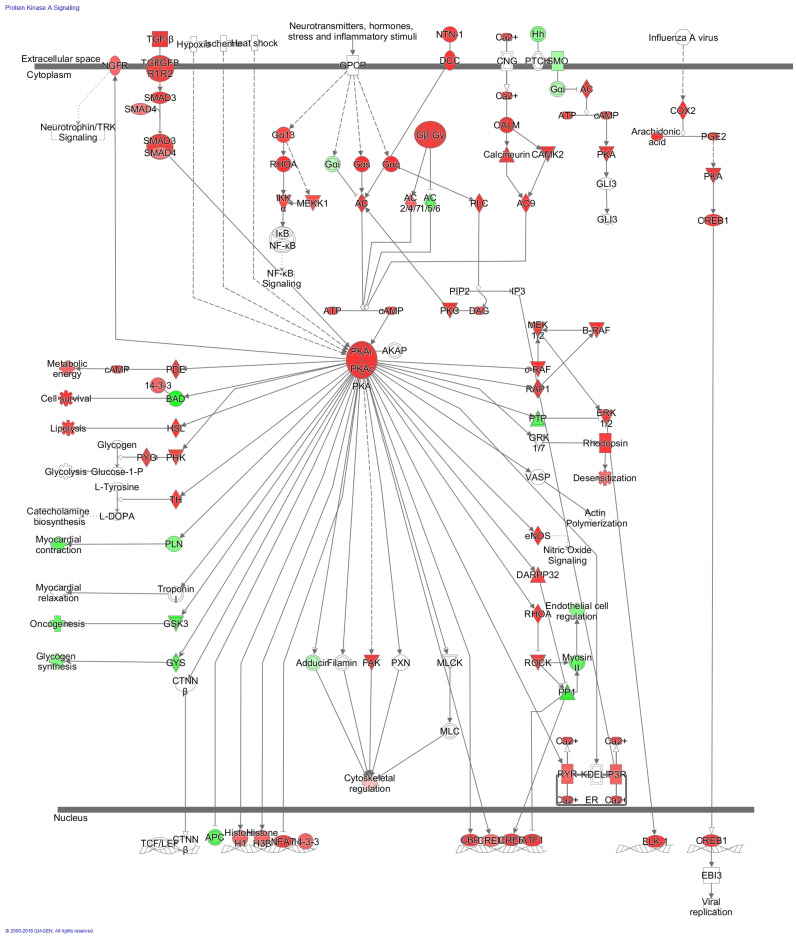 Figure 11
Figure 11 Figure 12
Figure 12Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFungal Biology and Applications · Flavonoids in Medical Research · Silymarin and Mushroom Poisoning
1. Introduction
Ophiocordyceps sinensis (Berk.) G.H. Sung, J.M. Sung, Hywel-Jones and Spatafora, 2007 (Caterpillar Fungus) [1] and Cordyceps militaris (L.) Fr., 1818 (Orange Cordyceps) [2] are botanicals [3] belonging to the fungi kingdom [4,5,6], traditionally valued across East Asia [7,8,9,10,11,12] for their tonic, energy-enhancing, aphrodisiac, and respiratory ailments, lung invigoration, and kidney-nourishing actions [13,14,15,16,17,18,19], Appendix A Table A1 and Table A2. Their therapeutic applications span inflammatory, respiratory disorders, fatigue, metabolic diseases (atherosclerosis, hyperlipidemia, glucose metabolism), kidney diseases, fertility, sexual-restorative functions, which are associated with immune, nervous, endocrine, cardiovascular, respiratory, renal, hepatic systems [14,20,21,22,23,24,25]. These attributes align with the modern concept of adaptogens as a therapeutic category of herbal medicines and nutritional products, characterized by increased human adaptability, survival, and resilience in response to stress by triggering intracellular and extracellular adaptive signaling pathways within cellular and organismal defense systems, including the neuroendocrine-immune complex [26]. In 1968, the term adaptogen (phytoadaptogen) was applied to medicinal plants, herbal medicines, and phytomedicines, reflecting their origin in the plant kingdom [27]. Phytoadaptogens are plant secondary metabolites, particularly tetracyclic terpenoids, and phenethyl- or phenylpropanoid derivatives of the defense system, chemically similar to steroidal and phenolic hormones of the human stress system [28].
Several studies claim that O. sinensis is an adaptogen [29,30,31,32] that triggers various adaptive stress–response signaling pathways [33,34,35,36,37,38]. However, the rationale for polyvalent action and the molecular mechanisms of O. sinensis have not been sufficiently studied or understood. Furthermore, clinical efficacy was not unambiguously demonstrated, and potential new indications for O. sinensis should be evaluated.
Unlike phytoadaptogens derived from the green plant kingdom Viridiplantae, O. sinensis [1,2,5,39,40], commonly known as Caterpillar Fungus or Winter Worm-Summer Grass, is an entomopathogenic fungus of the phylum Ascomycota, with a quite different biological nature compared to typical edible mushrooms (Basidiomycota). Initially described as Sphaeria sinensis by Berkeley in 1843, it was later named Cordyceps sinensis by Saccardo in 1878, and in 2007 it was renamed Ophiocordyceps sinensis, a member of the genus Ophiocordyceps (family Ophiocordycipitaceae, order Hypocreales), based on phylogenetic studies [3,4,10,25].
Caterpillar Fungus symbiotically parasitizes the larvae of ghost moths (Fam. Hepialidae, Hepialus spp./Thitarodes spp.) to survive, producing a characteristic club-shaped stroma that emerges from the mummified caterpillar [13,14,16,21,29,30,41,42]. As the larva’s self-defense mechanism weakens, the fungal cells spread throughout the body, forming the sexual stroma, which grows upward above the soil surface while remaining connected to the dead larva/host below, creating the unique insect/fungus combination [43,44,45,46].
This medicinal fungus is endemic to high-altitude regions of the Tibetan Plateau and the Himalayas [47,48] and has a long history in traditional medical systems of China, Nepal, India, Bhutan, Republic of Korea, Vietnam, Thailand, and Japan as a tonic to replenish bodily health [19,39]. Caterpillar Fungus is officially recognized as a medicinal fungus in the pharmacopeias of several countries, especially in East Asia, where it is highly valued for energy, immune, and respiratory support [49]. In Pharmacopeia of the People’s Republic of China, Chinese Caterpillar Fungus, Cordyceps (Dongchongxiacao) is classified as a Chinese Materia Medica crude drug, indicated for deficiency of kidney essence, impotence and seminal emission, limp aching in the lower back and knees, chronic cough and dyspnea of deficiency type, cough caused by consumptive diseases, and hemoptysis in daily dosage 3–9 g corresponding to ~1 mg of adenosine [50], Figure 1.
Related species, C. militaris [2], also known as the Scarlet Caterpillar Club and in Chinese as Northern Cordyceps, is cultivated on silkworm pupae and used for medicinal purposes, as a health supplement, and as a pharmaceutical drug on a large scale, especially in China [25,51]. Numerous studies on the chemical constituents and pharmacological activities of C. militaris [20,22,52,53,54] and its bioactive marker, cordycepin [53,54], reveal multiple effects on the neuroendocrine-immune complex [36,37,42,55,56,57,58,59,60,61,62], which is typical of adaptogens [22]. In the course of the search for new fungal antibiotics in 1950, Cunningham et al. found that the mold C. militaris secretes a substance called cordycepin, which inhibits the growth of several bacteria [63], increases the survival time of mice with Ehrlich ascites tumors, and inhibits the growth of human tumor cells in culture. In 1980, the chemical structure of cordycepin was elucidated as the nucleoside 3′-deoxyadenosine [64], a copy of adenosine with one oxygen atom removed from its structure (Figure 1).
Both fungi contain diverse bioactive metabolites, including nucleosides, sterols, peptides, polysaccharides, and secondary metabolites (Appendix A Figure A1 and Table A3, Table A4, Table A5 and Table A6).
The pharmacological breadth of both species suggests multi-target effects rather than classical single-receptor drug actions (Appendix A Table A4 and Table A5). Network pharmacology has become a significant framework for elucidating the complex, multi-target actions of such herbal and fungal preparations, providing a systematic approach to deciphering these interactions by integrating predicted targets, signaling pathways, molecular docking, and multi-omics data. However, most reports remain scattered, disease-specific, or lacking integration with wet-lab validation. A unified synthesis is needed to understand the core pharmacological principles of O. sinensis and C. militaris.
Despite numerous studies, no comprehensive synthesis has unified the mechanistic insights across species, compounds, and disease contexts. This narrative study integrates 37 network pharmacology investigations and 10 experimental validation studies to define the adaptogenic potential and systems-level pharmacology of these fungi and their active constituent, 3-deoxyadenosine (cordycepin).
Network pharmacology provides a valuable framework for understanding these multi-component, multi-target interactions. Nevertheless, existing studies are often disease-specific and fragmented, lacking an integrated mechanistic synthesis. This work consolidates findings from 37 network pharmacology studies, including 22 experimentally validated investigations, to establish a unified systems-level model for the adaptogenic activity of Caterpillar Fungus, Orange Cordyceps, and 3-deoxy-adenosine.
The adaptogenic concept represents a systems-level interpretation of complex physiological responses characteristic of holistic Traditional Chinese Medicine (TCM) and Ayurvedic concepts, whereas European Food Safety Authority (EFSA) regulatory frameworks lack concepts for resilience and adaptive capacity and operate at the level of single, well-defined functional outcomes, which raises regulatory issues for food and drugs in Western countries.
The implementation of European standards by EMA drug regulatory authorities for traditional herbal medicines and other botanicals developed under regulatory conditions in Asian countries creates problems for their regulation in Europe. This is mainly due to the core conceptual differences between reductionistic, mechanistic, and Systems-based, integrative, and holistic approaches to medicine in Western and Oriental countries, as well as to insufficient clinical evidence and limited well-established use. Another limitation in EU countries is that the EFSA does not accept the definitions of stress, fatigue, and adaptogens as dietary supplements or food additives, despite their worldwide scientific recognition. The reason is that EFSA considers these products for use only in healthy subjects, whereas medicines are used to treat or prevent defined diseases. However, the same products are used in China, India, Japan, and other Asian countries to restore balance and resilience. In this review, we sought to harmonize these complementary paradigms to address the gap and reach consensus.
Overall, this literature review primarily aims to justify a rationale for the pleiotropic adaptogenic potential of two traditionally used botanicals from the fungal species, Caterpillar Fungus and Orange Cordyceps, and its active constituent, 3-deoxyadenosine (cordycepin), using a network pharmacology approach The secondary aim was to establish a regulatory category for resilience-supporting physiological modulators that could align food and drug regulation in the EU with contemporary systems biology, and regulatory acceptance of adaptogenic botanicals across the European Union (EU), United States (US), and selected Asian jurisdictions.
2. Results
2.1. Bioactive Compounds of O. sinensis and C. militaris Fungi and Their Pharmacological Activity
Overall, 90 primary and secondary metabolites in O. sinensis and 26 constituents in C. militaris were identified in an extensive review, covering its traditional uses, chemistry, and pharmacology [19], as shown in Appendix A Table A3 and Table A4 and Figure A1.
Studies of chemical compositions of O. sinensis [21,29,65] and C. militaris [23,29,66,67] show the presence of host–parasite symbiotic interactions, four types of primary metabolites: (i)—amino acids and peptides, (ii)—nucleotides/nucleosides, (iii)—lipids, including sterols and fatty acids, and (iv)—carbohydrates, including polysaccharides. All of them are essential for the parasite’s growth and development, as well as for the host’s adaptive stress response (Appendix A Table A4, Table A5 and Table A6). Some secondary metabolites that function in defense responses include cytotoxic alkaloids and antioxidant phenolic compounds. These compounds were isolated and identified in O. sinensis growing under wild conditions, but not in cultivated O. sinensis and C. militaris (Appendix A Figure A1).
Many primary metabolites of mushrooms, including nucleosides, sterols, and polysaccharides, have been specified as physiologically active markers of O. synensis in both in vitro and in vivo studies [68]. Meanwhile, several novel compounds characteristic of O. sinensis have been identified, including epipolythiodioxopiperazines, gliocladicillins A, B, and 11,11′-dideoxyverticillin, which are capable of inhibiting the growth of tumor cells [16,69,70]. Exclusive to O. sinensis, five anti-inflammatory alkaloids, named cordysinin (A–E), have also been reported for the first time [16,19,71].
At present, cordycepin, adenosine, total nucleosides, ergosterol, and polysaccharides are commonly used quality control markers for O. sinensis and C. militaris products (Table 1 and Table A5) [18,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97]. However, they are not regarded as efficacy markers for therapeutic or nutritional purposes for several reasons, including poor oral bioavailability, instability, nonspecific (cordycepin, adenosine) or inconsistent actions (polysaccharides, ergosterol), and a lack of direct correlation between marker levels and clinical effects in humans [84,85].
O. sinensis exhibits broad biological and pharmacological actions in hepatic, renal, cardiovascular, and immunological systems, and has anticancer activity as well [15,97]. Over 30 different bioactivities have been reported for O. sinensis, including anti-inflammatory, immunomodulatory, antioxidant, antibacterial, hepatoprotective, antifatigue, antiaging, steroid hormones production, antidepressant, sedative, and the ability to promote endurance capacity, improve learning-memory in vitro, in vivo, or ex vivo studies, as shown in Appendix A Table A4 [97].
In the course of the search for new fungal antibiotics in 1950, Cunningham et al. found that the mold C. militaris secretes a substance called cordycepin, which inhibits the growth of several bacteria [63], increases the survival time of mice with Ehrlich ascites tumors, and inhibits the growth of human tumor cells in culture. In 1980, the chemical structure of cordycepin was elucidated as the nucleoside 3′-deoxyadenosine [64] (Figure 1). One of its modes of action is by inhibition of RNA synthesis. It is incorporated as 3′-deoxyadenosine triphosphate at the 3′ end of the RNA molecule, thereby preventing further elongation [98]. Phosphorylated adenosine, adenosinetriphosphate (ATP), is known as an “energy currency” in the metabolism of the organism. A cellular energy sensor, AMPK (AMP-activated protein kinase (PRKAA1/2/PRKAG1) is one of the key mediators of adaptive stress–response signaling pathways. Phosphorylated cordycepin (cordycepin triphosphate, COR-tp) competes with ATP, resulting in its incorporation into enzymatic processes where it acts as a substitute for ATP [99,100]. This molecular mimicry may underlie the diverse biological activities of cordycepin, leading to abnormal purine metabolism and inhibiting or aberrantly activating ATP-targeted protein kinases [35,62]. Consequently, it is not surprising that cordycepin may have beneficial health effects in stress-induced metabolic diseases and aging disorders, showing anticancer, antiviral, antioxidant, anti-aging, and anti-inflammatory activities [33,34,35,36,37,38,42,55,61,101,102,103,104].
Overall, the pharmacological activity of O. sinensis and C. militaris product preparations is unlikely to be attributable to a single active constituent, as compounds such as cordycepin and adenosine suffer from poor oral bioavailability and limited pharmacokinetic stability. Instead, it is reasonable to hypothesize that the overall therapeutic profile arises from the synergistic action of multiple metabolites—including nucleosides, polysaccharides, sterols, and peptides—that interact with diverse molecular targets. At present, the validity of this hypothesis rests primarily on the outcomes of randomized controlled clinical trials, rather than on any single chemical marker. In this context, network pharmacology approaches combined with gene expression analyses may be suitable tools for elucidating the complex, multi-target interactions underlying the putative synergistic effects of O. sinensis and C. militaris ingredients.
2.2. Nucleosides Adenosine and Cordycepin as Mediators of Adaptive Stress Response Andanti-Fatigue Activity of O. sinensis, and C. militaris
The choice of adenosine as an active marker for the standardization of Cordyceps (Dongchongxiacao), Chinese Caterpillar Fungus [50] and Patented Traditional Chinese Medicines (TCM) Bailing capsule [105], containing fermented O. sinensis powder standardized for 0.4 mg of adenosine, is presumably due to: (i) its high content in O. sinensis and (ii) its physiological functions.
Adenosine functions as an energy metabolite (part of the ATP/AMP balance) and as a signaling molecule via cell-surface receptors and intracellular actions in the nervous, cardiovascular, immune, respiratory, and renal systems [106,107,108,109,110,111]. Adenosine is a byproduct of the “energy fuel”, adenosine triphosphate (ATP) breakdown during stress (hypoxia, ischemia, exercise), matching oxygen supply with demand as a local, short-lived homeostatic regulator, and coordinating energy balance, vascular tone, neuronal excitability, and immune activity [112,113,114,115,116,117,118]. During low-energy states, adenosine acts as a local signal to increase energy supply. Adenosine indirectly regulates AMP-activated protein kinase (AMPK) activity through AMP/adenosine balance. High AMP/ATP ratios activate AMP-activated protein kinase (AMPK), promoting energy-conserving processes. Adenosine can also directly activate receptors, and its balance with AMP is maintained by enzymes such as adenosine kinase (ADK), as shown in Figure 1. Its primary molecular targets are the four adenosine GPCRs (A1, A2A, A2B, A3), as well as metabolic enzymes and transporters that control its levels [117,119,120,121,122].
Adenosine is the endogenous agonist of GPCR adenosine receptors (A1, A2A, A2B, A3, high affinity; EC50 in the low-nanomolar range), producing inhibitory neuromodulation that promotes sleep, decreases neuronal firing, and increases the subjective sensation of fatigue [101,123], Table 2. In contrast, caffeine acts as a competitive antagonist at A1 and A2A receptors (non-selective; micromolar affinities, Ki ~2–50 µM), thereby blocking adenosine’s inhibitory signaling and producing stimulatory effects on arousal, mood, reduced fatigue, and physical performance [124,125,126], Table 2. Cordycepin (3′-deoxyadenosine), despite structural similarity to adenosine, can act as an agonist in vitro (at A3 in many cell studies and A1/A2A in some reports), and has minimal functional interaction with adenosine receptors in vivo because it is rapidly deaminated to 3′-deoxyinosine, exhibits very low plasma nano-molar levels after oral ingestion [127,128], and demonstrates poor blood–brain barrier penetration, meanwhile in cell/animal models cordycepin’s effects (anti-inflammatory, antiproliferative) are often attributed to A3 agonism or other intracellular actions (AMPK activation, PI3K/mTOR inhibition) [101,129,130]. Consequently, cordycepin does not meaningfully modulate adenosine receptor activity and cannot reproduce either the inhibitory effects of adenosine or the stimulatory effects of caffeine. The net result is that adenosine is fatigue-promoting, caffeine is fatigue-reducing, and cordycepin is functionally neutral in the context of central fatigue regulation (Table 2).
Cordycepin cannot meaningfully act as a CNS adenosine receptor ligand, yet O. sinensis and C. militaris extracts and purified cordycepin repeatedly show anti-fatigue effects in animals and humans. This appears contradictory only if one assumes that fatigue modulation must occur via central adenosinergic signaling. Apparently, the anti-fatigue effects of O. sinensis and C. militaris are mediated by non-adenosinergic, non-CNS mechanisms, though somewhat peripheral.
Cordycepin has poor intestinal permeability and low bioavailability due to rapid hepatic degradation by the enzyme adenosine deaminase, which converts it to the inactive 3′-deoxyinosine. However, 3′-deoxyinosine has significant bioavailability following oral administration of cordycepin, when absorbed into the systemic circulation, and can be phosphorylated to the active cordycepin 5′-triphosphate, an analog of ATP [131], Figure 1, and therefore could be responsible for the therapeutic effects of cordycepin when administered orally. These findings offer important insights into the mechanisms underlying the therapeutic effects of cordycepin. Moreover, this metabolic pathway could play an important role in the activity of adenosine and other adenosine analog drugs. The metabolized products (i.e., the inactive metabolite of cordycepin, 3′-deoxyinosine) are available in the systemic circulation instead. They can return to the phosphorylation pathway of their parent form, as shown in this study [131].
The bioavailability of cordycepin is very low; a 10 mg/kg intravenous dose in rats yields a peak concentration of 2.1 ± 0.9 μg/mL (8366 nM). However, when cordycepin is administered orally to rats at a 10-fold higher dose of 100 mg/kg, it results in a relatively low peak plasma concentration, averaging approximately 0.004 ± 0.001 μg/mL (16 nM) [127]. The Cmax values of cordycepin in the rat blood and brain after exposure (10 mg/kg, i.p.) were 7.8 ng/mL (31 nM) and 5.4 ng/mL (21 nM), respectively [128]. Pharmacokinetic and brain research studies [127,128,131,132] reveal that the concentration of cordicepin in blood, kidney > liver > heart > lung > spleen > brain is dramatically lower than observed in vitro studies [127]. After systemic dosing with 10 mg cordycepin, its concentration in rat brain tissue is on the order of ~10–50 nM [127,128], while most published microglia/astrocyte studies use 10–50 μM cordycepin, which is 1000-fold higher than the presumed brain levels from a 9 g/day O. sinensis crude dose. These μM levels are clearly supra-physiological compared with the nM brain levels observed in PK studies; they are more like “pharmacological screening” than strict dose translation.
Obviously, the active concentrations of cordicepin, O. sinensis, and C. militaris preparations used in vitro studies are 1000-fold higher than those used in animal studies and do not match the effective therapeutic human daily dose of 9 g of O. sinensis and C. militaris crude drugs [50], which are traditionally used.
2.3. Efficacy and Safety of Ophiocordyceps sinensis and Cordyceps militaris in Human Subjects
2.3.1. Traditional Use
Oriental medical systems, TCM and Ayurveda, are based on a holistic approach, multi-target and polyvalent actions, but rely on archaic theories. In contrast, Western conventional medicine is based on a reductional approach, selective targeting, and specific action in the treatment of diseases, relying on another archaic theory of galenic preparations that ignores interactions and overlaps among regulatory systems and the effects of other constituents in multi-component plant extracts. In fact, both approaches are complementary, particularly in the treatment of diseases of complex pathology associated with the stress system interacting with other regulatory systems. The concomitant administration of several Western conventional medicines that selectively act on various receptors provides more effective treatment in hypertension, post-stroke rehabilitation, viral infections, etc. The “ready for use” of complex botanicals and botanical hybrid products used in the Eastern world acts similarly. The challenge is to understand the mechanisms of action and scientifically validate their efficacy, quality, and safety.
According to traditional Chinese medicine (TCM) theory, the organ functions concepts differ from Western physiology and pathology, suggesting that Caterpillar Fungus goes to the “Lung” and the “Kidney” meridians, supporting “lung protection,” “kidney improvement,” and so-called “YinYang double invigoration” [133]. Since the kidneys are considered “the root of life” in TCM, they store “Jing,” a substance described as an undifferentiated, prime organic material that is “the source of reproduction, development, and maturation” [133]. Conception is made possible by the power of Jing; growth to maturity is the blossoming of Jing; and the decline into old age reflects the weakening of Jing. Over time, the Jing decreases in both vitality and quantity. Consequently, according to TCM, reproductive problems such as sterility or impotence and developmental disorders like retarded growth or lack of sexual maturation are seen as a dysfunction of the kidney’s storing of Jing [133]. Moreover, according to TCM theory, the kidneys enable the fundamental “energy of life, so-called the Natural Air”, Qi/chi, to penetrate deeply, completing the inhalation process by what is called “grasping the Qi.” The kidneys are thus the root of Qi, while the lungs are the “foundation of Qi.” Proper breathing thus depends on the kidneys, and kidney disharmonies may result in respiratory problems, especially chronic asthma. In a “disharmony of the Lungs,” a deficient Qi can result in any area of the body, and the power of resistance of the “protective Qi will be poor” [13,133]. Both TCM and Ayurveda have a notion of “life vital energy” and activating the body and mind: the qi in TCM and the prana in Ayurveda. Herbalists refer to adaptogens as restoratives, qi-tonics, rasayanas, or rejuvenating herbs [134].
According to TCM, Caterpillar Fungus goes to the “Lung” and the “Kidney” meridians, supporting “lung protection,” “kidney improvement,” and so-called “YinYang double invigoration” [133] and therefor was used to treat “lung” and “kidney” asthenia syndromes describing groups of symptoms associated with respiratory and renal diseases and other disease conditions such as fatigue, asthenia after severe illness, night sweating, male and female hyposexualities, including impotence, hyperglycemia, hyperlipidemia, respiratory diseases, renal dysfunction and renal failure, liver diseases, arrhythmias and other heart diseases [13]. They have been included as a dietary supplement to maintain health and prevent disease (Appendix A Table A7) [13,135].
It has been found that most local folk/traditional healers use Caterpillar Fungus to treat 21 ailments, including erectile dysfunction, female aphrodisia, malignant tumors, bronchial asthma, bronchitis, diabetes, cough and cold, jaundice, alcoholic hepatitis, and others [21,97].
2.3.2. Clinical Studies
2.3.2.1. Systematic Reviews and Meta-Analyses of Randomized Clinical Trials
Several systematic reviews and meta-analyses of randomized clinical trials of O. sinensis in dialysis patients [136,137] with renal dysfunction [137], acute kidney injury [138], chronic kidney disease [139], diabetic kidney disease [140], lung cancer [141], chronic obstructive pulmonary disease [142,143] and in healthy human subjects [144,145] were conducted, Table 3. These meta-analyses support the efficacy and safety of O. sinensis for immune and respiratory health, making it a promising adjunct in both healthy and clinical populations.
An umbrella-level synthesis of these systematic reviews and meta-analyses of randomized controlled trials (RCTs) evaluating O. sinensis was conducted by AI assistance. The objective was to assess the strength and consistency of the clinical evidence, stratified by species and preparation type, and to grade the overall level of evidence in accordance with the European Medicines Agency (EMA) criteria for well-established use (WEU) herbal medicinal products. Evidence was synthesized narratively and comparatively, without re-pooling individual trial data, in line with accepted methodology for overviews of systematic reviews [146].
Table 3 summarizes the totality of clinical evidence from nine systematic reviews, stratified by species and indication, and maps the findings against the key elements required for well-established use according to EMA/HMPC principles. Figure 2 illustrates the conceptual pathway from individual randomized trials to regulatory-relevant evidence grading, highlighting the points at which the current evidence base fails to meet WEU requirements despite consistent efficacy signals.
Figure 2 summarizes the progression from randomized controlled trials through systematic reviews to regulatory-relevant evidence grading. Although consistent adjunctive clinical benefits are observed across renal, pulmonary, and oncologic indications, limitations in methodological quality, preparation heterogeneity, and lack of documented long-term EU medicinal use prevent fulfillment of EMA criteria for well-established use (WEU), which requires: (i) recognized therapeutic efficacy, (ii) acceptable safety, (iii) sufficient clinical evidence, (iv) use for at least 10 years within the European Union, and (v) a well-defined herbal substance or preparation.
Across these reviews, consistent improvements were reported in surrogate renal and inflammatory outcomes, including reductions in serum creatinine, blood urea nitrogen, C-reactive protein, and proteinuria, as well as improvements in albumin and hemoglobin levels in dialysis populations. Preventive use before contrast exposure was associated with a reduced incidence of contrast-associated acute kidney injury in several trials. However, all reviews identified substantial methodological limitations, including: (i) predominantly open-label RCTs, (ii) inadequate reporting of allocation concealment and blinding, (iii) short treatment duration and follow-up, and (iv) reliance on surrogate rather than hard clinical endpoints (e.g., mortality, progression to end-stage kidney disease). Certainty of evidence was graded as low to very low using the grading of recommendations assessment, development and evaluation (GRADE) methodology [147] in the original reviews, primarily due to risk of bias, indirectness, and imprecision.
A critical limitation for O. sinensis is the heterogeneity of preparations. Most clinical trials investigated fermented mycelial products (e.g., Bailing, Jinshuibao, Zhiling) rather than the wild fungus, and variability in fungal strains, manufacturing processes, and dosing regimens was observed. This heterogeneity limits the extrapolation of findings to a single, well-defined herbal substance or preparation.
Systematic reviews of O. sinensis evaluated its adjunctive use in COPD, lung cancer, and renal dysfunction. Across COPD studies, adjunctive use was associated with improvements in lung function parameters (e.g., FEV_1_), exercise tolerance, and quality-of-life scores. In lung cancer, meta-analyses reported improved tumor response rates, immune markers, and reduced treatment-related adverse reactions when O. sinensis was added to chemo- or radiotherapy. In renal dysfunction, consistent improvements in biochemical markers were observed.
Despite these positive signals, the evidence base shared several limitations:
- Trials were almost exclusively conducted in China;
- Most studies were small and short-term;
- Blinding and placebo control were largely absent;
- Outcomes were frequently surrogate or supportive rather than definitive clinical endpoints.
Accordingly, the certainty of evidence ranged from low to moderate, with significant downgrading for risk of bias and indirectness.
Many reviews used the name O. sinensis to describe commercial mycelial preparations that are taxonomically closer to O. sinensis or other related fungi. This taxonomic and pharmaceutical ambiguity represents a major obstacle for regulatory classification and evidence consolidation.
Overall, across nine systematic reviews, both O. sinensis preparations demonstrate biologically plausible and clinically consistent adjunctive benefits, particularly in renal disease and chronic pulmonary conditions. However, when assessed against the EMA criteria relevant to well-established herbal medicinal products, the current body of evidence does not meet the requirements for WEU, as outlined in Table 3.
This conclusion is driven not by lack of efficacy signals, but by:
- Insufficient methodological robustness;
- Absence of EU-based medicinal use documentation;
- Lack of a single, standardized herbal substance or preparation;
- Predominant reliance on surrogate outcomes.
From a scientific perspective, the evidence supports potential therapeutic value and justifies further high-quality clinical research. From an EMA regulatory perspective, the findings are more consistent with traditional herbal medicinal products rather than well-established use.
2.3.2.2. Clinical Evidence for Anti-Fatigue Effects of O. sinensis and C. militaris: Implications for EMA Well-Established Use
Early placebo-controlled clinical studies examined the effects of O. sinensis (cordymax™ Cs-4) therapy in elderly patients with fatigue and other aging-related symptoms [148,149,150]. Compared with placebo-treated patients who showed no improvement in symptoms, most O. sinensis (Cs-4)-treated patients reported overall clinical improvement [149]. The subjective improvements included promotion to endurance capacity [150] and alleviation of fatigue, cold intolerance, dizziness, frequent nocturia, tinnitus, hyposexuality, and amnesia [13,149].
The results of some studies of O. sinensis in a limited number of healthy subject athletes suggest that it can increase exercise performance [151,152], tolerance to high-intensity exercise [153], and alleviate muscle injury [154], maintain the hemoglobin and hematocrit levels [154], while the results of a few other placebo-controlled randomized studies were not reproducible and do not show health benefits [154,155].
Two review articles summarized the effects of O. sinensis on aerobic performance and fitness in human studies [144,145].
Supplementation with O. sinensis was expected to exhibit a potential physical performance-enhancing (ergogenic) effect by increasing time to exhaustion when administered regularly for 2 to 16 weeks before exercise, although its effects on improving aerobic fitness remain inconsistent [145]. Most studies involved active, young participants; however, the ergogenic potential of O. sinensis in aging and sedentary populations remains poorly understood, as few studies have examined it [145].
In summary, the potential benefits of O. sinensis supplementation are supposed to: (i) improve aerobic performance, (ii) enhance oxygen utilization, (iii) increase maximal oxygen consumption (VO_2_max, a key indicator of aerobic fitness), and (iv) delay fatigue. However, the problems and challenges are: (i) some studies do not exhibit improvements, and the effects are inconsistent, (ii) the benefits may depend on the dosage used. Overall, while promising, more high-quality human studies are needed to fully understand its effects, especially across different populations such as older adults and sedentary individuals.
Welch et al., (2023) [144] reviewed 29 full texts of the 4308 potentially relevant articles selecting seven randomized trials of O. sinensis conducted with a total of 286 healthy human subjects [150,154,155,156,157,158,159,160] and applying PRISMA, the Cochrane risk-of-bias tool, the Jadad’s quality scale, and the Checklist score of Items for Reporting Trials of Chinese Herbal Medicine Formulas from CONSORT extension for Chinese herbal medicine. Formulas were applied to the data with the purpose of critically assessing the current evidence for or against the effectiveness or efficacy of O. sinensis. Their evaluation highlights the need to conduct high-quality, low-bias clinical trials [144]. The authors conclude that supplementation with O. sinensis may affect aerobic performance and could have implications for various athletic events; however, insufficient reporting of the details of the O. sinensis preparation used was a common issue across the included studies. Of the included studies, five reported significant pre- and post-intergroup differences in the effect of O. sinensis supplementation on aerobic performance [144].
Importantly, between-group analysis showed no significant changes in VO_2_max, work rate at the metabolic threshold, or work rate at the ventilatory threshold between the treatment and placebo groups [144].
In some studies, baseline (before treatment) primary outcome measures differ significantly between the placebo and O. sinensis groups [150], suggesting a lack of randomisation. A fatal methodological flaw in other studies was that between-group changes from baseline over time (before and after treatment) were not assessed to exclude the placebo effect. The products and their method of preparation were insufficiently characterized to demonstrate reproducibility and consistency in the results of various clinical trials.
Table A8 summarizes results of meta-analysis of randomized placebo-controlled clinical trials of O. sinensis in athletes [152,153,154] and healthy adults [150,158,161,162], as well as in other human subjects with symptoms of long COVID [163], mild COVID-19 [164], asthma [165], exercise fatigue [152], and C. militaris in mild liver dysfunction [166], depression with insomnia [167] and fatigue [153,154,161,162].
Clinical trials of O. sinensis include traditional extracts and cultivated mycelial products. The majority of fatigue-related trials of O. sinensis investigated fermented mycelial preparations, most commonly Cs-4^®^. Randomized, double-blind, placebo-controlled trials in healthy older adults demonstrated improvements in exercise tolerance, VO_2_max, ventilatory threshold, and perceived exertion, outcomes that are directly relevant to physical fatigue. Early Japanese double-blind trials demonstrated reductions in subjective fatigue scores and improved tolerance during graded exercise tests in healthy adults. Additional studies in athletes and physically active individuals reported improved exercise tolerance and oxygen-related biomarkers, although findings were inconsistent across studies. Null results were frequently observed in highly trained populations, suggesting a limited ergogenic ceiling effect and reinforcing the notion that fatigue-modulating effects may be most relevant in sub-optimally conditioned or aging individuals.
This section critically reviews fatigue-specific clinical trials of O. sinensis in healthy adults, older adults, and individuals with post-COVID-19 conditions. It assesses the strength of the evidence against the European Medicines Agency (EMA) criteria for well-established use (WEU). EMA WEU requirements include recognized efficacy, acceptable safety, consistent clinical evidence, a well-defined herbal preparation, and at least 10 years of medicinal use within the European Union. Species are analyzed separately due to regulatory and pharmacognostic relevance.
Appendix A Table A9 is focused exclusively on long COVID/post-COVID fatigue. As summarized in the table, direct clinical evidence for the use of O. sinensis in long COVID-related fatigue is currently limited but emerging. A recent randomized, waitlist-controlled trial in patients with long COVID demonstrated that Cs-4^®^ significantly improved fatigue severity, functional capacity, and health-related quality of life compared with usual care [163]. This study represents the most direct clinical evidence for an anti-fatigue effect of O. sinensis in a post-viral population. However, the trial was limited by regional recruitment, short follow-up, and reliance on patient-reported outcomes. Evidence on COVID-19-related fatigue is emerging but remains limited. An industry-sponsored randomized study reported improvements in fatigue and recovery time during acute COVID-19 when O. sinensis capsules were used as add-on therapy. However, the lack of peer review and methodological transparency substantially reduces the evidentiary weight.
Fatigue-specific clinical trials of O. sinensis demonstrate biologically plausible and clinically observable benefits, particularly in aging and post-viral populations. However, when evaluated against EMA/HMPC standards, the evidence base remains insufficient for WEU designation, primarily due to methodological limitations and heterogeneity in preparation.
Overall, across healthy, aging, and post-infectious populations, O. sinensis demonstrates biologically plausible and clinically observable anti-fatigue effects, with the strongest signals seen in older adults and long COVID patients. However, under EMA/HMPC standards, the current evidence base is insufficient to support well-established use due to methodological limitations, evidence quality (most trials are small, short-term, and use heterogeneous or surrogate fatigue endpoints); GRADE certainty would be low to moderate: downgrading was primarily due to risk of bias (blinding, allocation concealment), inconsistency across populations, indirectness (exercise performance vs. validated fatigue scales), and imprecision (small sample sizes), preparation heterogeneity (fermented mycelium, different strains, combination products), preventing the definition of a single herbal preparation, and a lack of documented long-term EU medicinal use. From a scientific perspective, the evidence justifies further high-quality trials using validated fatigue endpoints. From a regulatory perspective, the data align more closely with traditional use of herbal medicinal products than with well-established use (WEU) status, and emerging clinical signals warrant further confirmatory trials using validated fatigue instruments. Future studies should prioritize validated fatigue scales, longer follow-up, and standardized preparations to strengthen both scientific and regulatory credibility.
2.4. Systems-Level Mechanisms of O. sinensis, C. militaris, and Cordycepin: An Integrative Network Pharmacology and Experimental Evidence Review
Caterpillar Fungus and Orange Cordyceps are medicinal fungi traditionally valued for their restorative, endurance-enhancing, and homeostasis-supporting properties. These attributes align with the modern concept of adaptogenic activity, characterized by improved resistance to physical, chemical, and biological stressors [26,28,134].
Both fungi contain diverse bioactive metabolites, including nucleosides (adenosine, 3-deoxy-adenosine/cordycepin), sterols, peptides, and polysaccharides. The pharmacological breadth of O. sinensis suggests multi-target effects rather than classical single-receptor drug actions. Network pharmacology provides a systematic approach to deciphering these complex interactions, integrating predicted targets, signaling pathways, molecular docking, and multi-omics data.
Network pharmacology, combining computational target prediction, pathway enrichment, and systems biology, has become a significant framework for elucidating the complex multi-target actions of such herbal [168,169,170,171,172,173], including O. sinensis, C. militaris, and cordicepin and other fungi preparations [68,174,175]. Many network pharmacology studies of O. sinensis employ a so-called “reverse pharmacology” approach [176], based on plants described in ancient texts or on the empirical knowledge of traditional healers, and are focused on elucidating their mechanisms of action, which is typical of TCM. However, most reports remain scattered, disease-specific, or lacking integration with wet-lab validation. Despite numerous studies [57,60,103,140,144,174,175,177,178,179,180,181,182,183,184,185,186,187,188,189,190,191,192,193,194,195,196,197,198,199,200,201,202,203,204,205,206,207,208], no comprehensive synthesis has unified the mechanistic insights across species, compounds, and disease contexts. A unified synthesis is needed to understand the core pharmacological principles of O. sinensis and C. militaris.
This section provides the most comprehensive overview to date of network pharmacology analyses of O. sinensis, C. militaris, and cordycepin, integrating computational predictions and experimental evidence to derive a consolidated mechanistic model. This study integrates 37 network pharmacology investigations, including 22 experimental validation studies, along with Appendix A Table A10 and Table A11 [177,178,179,180,181,182,183,184,185,186,187,188,189,190,191,192,193,194,195,196,197,198,199,200,201,202,203,204,205,206], to define the adaptogenic potential and systems-level pharmacology of Caterpillar Fungus, Orange Cordyceps, and cordycepin.
Across the studies, the workflow is similar: selection of active constituents of Cordyceps → predict molecular targets → build protein–protein interaction/pathway networks → dock key compounds to target proteins → sometimes validate in cells/animals. Importantly, these are hypothesis-generating in silico, so their strength depends on follow-up experiments (Appendix A Table A10 and Table A11).
Across fungal species and study designs, highly consistent mechanistic hubs emerged: inflammatory cytokines (TNF, IL-6, IL-1β), stress-activated kinases (MAPK1/3/8), survival pathways (AKT1), mitochondrial regulators (FOXO3, HIF-1), apoptotic mediators (CASP3, BAX/BCL2), transcriptional co-regulators (CREBBP, EP300, FOXO3), and metabolic enzymes (IDH1, CYP19A1), Figure 3, Table A12 and Table A13.
The most frequently enriched recurrent pathways included PI3K–Akt, MAPK, NF-κB, apoptosis, oxidative-stress regulation, and AMPK–SIRT1–PGC-1α, the latter closely linked to metabolic and mitochondrial adaptation, Appendix A Table A12. This convergence indicates that O. sinensis and C. militaris metabolites act not through a single canonical receptor but through a broad network modulation that affects immunity, metabolism, mitochondrial function, and cell-survival signaling—consistent with the systems-level pharmacology expected of adaptogenic botanicals.
Experimental evidence validated predicted mechanisms in obesity, COPD, pulmonary hypertension, cancer, influenza, and vaccine immunogenicity (Appendix A Table A10), Figure 3.
Experimental validation studies evidence confirmed network predictions in:
- Immune modulation via TLR4/TNF-α [182];
- Cancer apoptosis via PI3K–Akt and caspase regulation [187];
- Apoptotic pathway activation in cancer [178,187];
- Cytokine normalization and lung restoration in COPD [174];
- PAH through apoptosis and vascular remodeling repair [191];
- Obesity/metabolic syndrome via AKT1/MAPK14/GSK3B [192];
- HBV vaccine response enhancement [177].
The integrative analysis of network pharmacology data combined with experimentally validated studies demonstrates that O. sinensis, C. militaris, and cordycepin share a convergent mechanistic architecture centered on immune modulation, stress-kinase regulation, metabolic adaptation, mitochondrial support, and apoptosis control. The repeated identification and validation of PI3K–Akt, MAPK, NF-κB, and AMPK–SIRT1–PGC-1α pathways indicate that O. sinensis, C. militaris, and cordycepin are systems-level adaptogenic agents capable of normalizing physiological functions across multiple organ systems. These findings support the therapeutic potential of standardized preparations and justify further translational research, particularly in immunometabolic and chronic inflammatory diseases.
Table 4 presents the key findings of network pharmacology studies and the characteristic differences between O. sinensis [139,197,198,208] and C. militaris preparations [182,183,185,206] (Appendix A Table A10 and Table A11).
The implications and predictions for health claims inferred from the network pharmacology studies, Table 4, can be summarized as follows:
- O. sinensis exhibits broad-spectrum organ support and multi-pathway modulation, especially in chronic diseases and viral infections. The most defensible, network-anchored claims are around kidney support/adjunct in chronic kidney disease, inflammation/oxidative stress, and respiratory immune modulation—with some clinical meta-analytic support but still needing higher-quality trials [136,139].
- C. militaris shows targeted cytotoxicity and immune activation, making it more suitable for oncology and immunotherapy applications. C. militaris preparations, explicitly characterized by high content of cordycepin, have the strongest network-mechanistic case for anticancer mechanisms, immune modulation (TLR4–TNF, macrophage polarization), and metabolic/urate axes. The evidence is growing, but disease-specific clinical endpoints remain limited [182,183,185].
Pathways are stratified according to an evidence-tier framework:
- Tier 1 (Prediction Only): Identified through in silico network modeling and enrichment analysis without biological confirmation.
- Tier 2 (Experimental Validation): Supported by in vitro or in vivo mechanistic studies.
- Tier 3 (Clinical Alignment): Mechanistic pathways supported by human clinical biomarker modulation or RCT endpoints.
This structured presentation reduces target inflation bias and visually distinguishes hypothesis-generating predictions from experimentally or clinically supported mechanisms.
Convergent evidence from network pharmacology, experimental studies, and multi-omics analyses demonstrates that O. sinensis, C. militaris, and cordycepin share a unified mechanistic architecture centered on immune modulation, stress-kinase regulation, mitochondrial adaptation, and metabolic homeostasis. This integrated systems pharmacology supports their classification as adaptogenic natural products with relevance to chronic inflammatory, metabolic, and immunological diseases. Future work prioritizing standardized preparations and mechanistically powered clinical studies will be essential for therapeutic translation.
Table A14 presents an evidence-tier framework that distinguishes Tier 1 (in silico prediction), Tier 2 (experimental validation), and Tier 3 (clinical alignment). Figure 4 and Table 4 reflect validation levels and reduce potential target inflation bias.
Figure 4 presents frequency heatmaps summarizing the recurrence of predicted and validated targets and enriched pathways across 37 independent network pharmacology studies involving O. sinensis, C. militaris, and cordycepin. Heatmaps were generated using AI to visualize the frequency of reported targets and enriched pathways across 37 network pharmacology studies. For each entity (O. sinensis, C. militaris, cordycepin), the number of independent publications reporting a given target or pathway was counted. Color intensity represents recurrence frequency, with warmer colors indicating higher convergence across studies.
Table 5 shows the effects of cordycepin on adaptive stress–response signaling pathways and physiological roles [36,209,210,211,212,213,214,215,216,217]. Appendix A Table A13 presents the major adaptive stress response pathways modulated by cordycepin, highlighting key genes, their biological roles, and the primary supporting studies.
Caterpillar Fungus, Orange Cordyceps, and 3-deoxyadenosine exhibit a unified adaptogenic pharmacology that involves immune modulation, mitochondrial enhancement, stress-signal regulation, and metabolic homeostasis. These effects arise through multi-target synergy across PI3K–Akt, MAPK, NF-κB, apoptosis, and AMPK–SIRT1–PGC-1α pathways. The strong convergence of network and experimental evidence supports their potential in immunometabolic and stress-related disorders.
Our findings align with a recent review providing evidence-based rationale for Chinese traditional medicinal mushrooms, which demonstrate multi-target anti-inflammatory activity by modulating key cellular mediators (macrophages, regulatory T cells, natural killer cells) and signaling pathways (NF-κB, MAPK, NLRP3 inflammasome, Nrf2/HO-1) of mushrooms for chronic inflammation management [68].
Table 6 summarizes key genes involved in cordycepin-induced adaptive stress–response signaling pathways and their physiological roles [33,34,35,36,37,38].
2.5. Food and Drug Regulation of O. sinensis and C. militaris in Western and Oriental Worlds
Wild O. sinensis has medicinal rather than culinary use in TCM, traditionally as a tonic, and is not classified as an edible mushroom in food codes. Cultured mycelium of O. sinensis can be food-grade or supplement-grade, depending on the strain and national registration (Appendix A Table A15). C. militaris, by contrast, is generally recognized as edible and is widely cultivated as a functional food mushroom. Table 7 summarizes the regulatory/edible/novel-food status of O. sinensis vs. C. militaris across major regions, with key references to support claims. Data derived from peer-reviewed studies [16,218], official food and drug regulatory websites, and Rapid Alert System for Food and Feed (RASFF) notifications [219,220,221,222,223,224,225,226,227,228].
In China, C. militaris has a new resource-food status (since 2009) [218], so it is widely used in domestic foods/health foods. In the Republic of Korea and Japan, C. militaris is regarded as edible/medicinal under functional food or Kampo frameworks, whereas O. sinensis is used as a medicinal fungus rather than a culinary mushroom. In the USA, both are typically sold as dietary supplements, avoiding disease claims to stay out of the “new drug” category. Overall, in the EU, O. sinensis (mycelium and fruiting body) is used as a food supplement without a novel food authorisation (other food uses may still be novel). C. militaris (mycelium and fruiting body) is novel and not yet authorized; placing supplements with C. militaris on the EU market requires a successful novel food authorisation or an exemption that does not currently exist and can be expected at the Rapid Alert System for Food and Feed (RASFF) alerts portal, see Appendix A [225,226,227,228], Table A15. The Appendix A Table A16, Table A17, Table A18, Table A19 and Table A20 show characteristic features of O. sinensis and C. militaris across key pharmacopeias and regulatory frameworks, including health claims and medicinal uses.
2.6. Resilience Biology, Inflammation, and Adaptogens: An Umbrella Review of Biological Evidence and Regulatory Frameworks Across Europe, the United States, and Asia
Stress responses and inflammation are evolutionarily conserved adaptive processes essential for survival and recovery, restoring homeostasis following injury or challenge [229,230,231,232,233,234,235,236], as shown in Appendix A Table A21. While inflammation is firmly established as a pathological and regulatory target in Western medicine [237,238], stress adaptation and resilience biology remain poorly integrated into regulatory frameworks, particularly within the European Union [239,240,241]. Adaptogens are proposed to enhance adaptive capacity and nonspecific recovery in various diseases and disorders [26,28,134,242]. Despite accumulating biological evidence, adaptogens lack regulatory recognition in the EU [241], while receiving broader acceptance in the United States [237,243], and Asia [244].
This umbrella review section synthesizes evidence from systematic reviews, narrative reviews, and regulatory documents to compare (i) biological definitions of inflammation, stress, and adaptive stress responses; (ii) their physiological roles and resolution mechanisms; and (iii) regulatory acceptance of adaptogenic botanicals across the European Union (EU), United States (US), and selected Asian jurisdictions. A structured umbrella review approach was applied to peer-reviewed reviews (2000–2024) addressing inflammation, stress physiology, adaptogens, and regulatory science. Regulatory guidance from EFSA, EMA, FDA, and Asian authorities was examined. Findings were narratively synthesized.
Stress and inflammation share common adaptive purposes and resolution dynamics (Table 8). Both stress and inflammation are beneficial in acute settings and harmful in chronic settings (Appendix A Table A20). Chronic stress drives chronic inflammation, and chronic inflammation feeds back into stress circuits.
Unfortunately, terms such as stress, fatigue, and adaptation have not been formally recognized as a regulatable pathological entity in the EU. The reason lies in the basic concepts of health and fatigue in Western and Oriental medical paradigms, as reflected in the food and drug regulatory authorities in Europe, the USA, China, India, and Japan. Key conflict: traditional systems intervene upstream of disease, whereas EU drug regulators say “no disease exists yet” (Table 9 and Table 10).
Why is the “anti-inflammatory” effect a recognized regulatory term, but “antistress”, “anti-fatigue”, and “stress-protective” are not recognized in Europe? Regulatory reasoning is that: inflammation is a defined pathological process, established clinical biomarkers exist, precise pharmacological mechanisms are known, and historical drug precedents exist (NSAIDs, corticosteroids). Consequently, the European Medicines Agency accepts anti-inflammatory mechanism-based claims and botanical medicines with demonstrated effects on inflammatory mediators.
Meanwhile, the terms “antistress”, “anti-fatigue”, and “stress-protective” are not accepted by EMA because of regulatory concerns, including: (i) “Stress” is considered a normal life experience, not a disease, (ii) claims imply psychological or psychiatric effects, and (iii) risk of unsubstantiated or exaggerated health claims. Scientific challenges include: (i) stress is considered contextual and subjective, (ii) no single, validated disease definition, and (iii) biomarkers are indirect, variable, and situation-dependent. Thus, authorities avoid approving terms that: (i) lack precise physiological targets, (ii) cannot be consistently quantified, and (iii) blur boundaries between food, supplements, and medicines.
A core regulatory paradox is that vitamins and antioxidants are recognized, but adaptogens are not. The reason is that EU Regulation favors selected target, single-pathway, disease-linked, measurable mechanisms, while adaptogenic effects are systems-level and contextual. While adaptogens aim to normalize stress responses rather than inhibit a specific pathological pathway, this does not fit the reductionist regulatory model.
EU drug authorities consider stress as an adaptive life process, but not a disease target, and adaptogens as a regulatory misfit, but not a scientific invalidity. Adaptogens fail not scientifically, but structurally. EU drugs regulators lack a legal category for resilience enhancers. Adaptogens challenge regulatory frameworks because they support resilience rather than treat disease.
In 2007, EMEA’s “Reflection paper on the adaptogens concept” clarified that the term “adaptogen” is applied to different herbal medicinal products (including preparations derived from Eleutherococcus, Ginseng, and Rhodiola) that have the capacity to normalize bodily functions and strengthen systems compromised by stress [241]. They are reported to have a protective effect on health against a wide variety of environmental assaults and emotional conditions [241]. EMA approved EU Community Monographs for Rhodiola, Eleutherococcus, and Ginseng as traditional herbal medicinal products for the relief of stress-related symptoms, such as fatigue and exhaustion [245]. EMEA “Reflection paper on the adaptogens concept” concluded “The concept of adaptogens is sufficient to be considered in the assessment of traditional herbal medicinal products (e.g., monograph on Eleutherococcus root). As the term “adaptogen” is considered not appropriate for a marketing authorisation, more clinical studies, and data on the efficacy in a well-defined clinical condition would be necessary” [241]. When the second sentence is taken out of context from the EMA conclusion, e.g., on Wikipedia, it creates a misleading impression of the scientific validity of the adaptogenic concept. Over the last two decades, our understanding of the mechanisms of action and clinical conditions of adaptogens has been substantially enriched through network pharmacology and molecular biology studies [26,28,134,171,173,246,247], whereas the clinical evidence of their efficacy remains insufficient due to various methodological shortcomings and limited characterization of study products [241].
Adaptogens are rejected in the EU not because they lack biological validity, but because European regulation has no legal concept of resilience. In contrast, Asia is built on it, and the US pragmatically tolerates it (Table 10).
Adaptogens demonstrate modulatory effects on immune, inflammatory, neuroendocrine, and metabolic pathways consistent with resilience biology [26,28,134,242,246] yet lack a regulatory category in Europe. The US adopts a permissive structure–function approach, while Asian systems explicitly integrate adaptogens within traditional and functional medicine paradigms.
This review clarifies conceptual and regulatory barriers to recognizing resilience-supporting interventions and informs future regulatory innovation. Adaptogens are not rejected due to insufficient biology, but because current regulatory frameworks lack concepts for resilience and adaptive capacity. Establishing a regulatory category for resilience-supporting physiological modulators could align regulation with contemporary systems biology.
3. Discussion
3.1. An Integrative Network Pharmacology and Systems-Level Mechanisms of Ophiocordyceps sinensis, Cordyceps militaris, and Cordycepin
The quantitative synthesis of 37 network pharmacology studies reveals a highly convergent and biologically coherent systems-level pharmacological architecture underlying the activities of O. sinensis, C. militaris, and cordycepin. Rather than supporting isolated, disease-specific mechanisms, aggregated networks consistently converge on a limited set of high-centrality molecular hubs and signaling modules that govern cellular stress adaptation, immunometabolic homeostasis, inflammatory tone, and survival–death decisions.
3.1.1. Convergence on a Conserved Stress-Adaptive Signaling Core
Across species and preparations, the most frequently identified hubs—including AKT1, CASP3, TNF/NF-κB, MAPKs, HIF-1α, and Nrf2—define a conserved stress-adaptation core network. These nodes integrate metabolic sensing (PI3K–Akt, AMPK–mTOR), redox regulation (Nrf2), inflammatory control (TNF/NF-κB, TLR signaling), and apoptotic regulation (caspase cascades), Appendix A Table A20. The repeated emergence of this hub constellation across heterogeneous disease models indicates that O. sinensis and C. militaris-derived products function as coordinated regulators of cellular resilience systems rather than as single-target agents.
This convergence provides a mechanistic foundation for the traditional classification of Cordyceps mushroom as tonic or adaptogenic medicines and is consistent with contemporary network-medicine models, in which therapeutic benefit arises from distributed modulation of interacting stress-response circuits rather than maximal perturbation of isolated molecular targets.
3.1.2. Species-Level Pharmacology Reflects Network Breadth, Not Redundancy
Although O. sinensis and C. militaris share substantial overlaps in their predicted and validated networks, their frequency profiles reveal distinct pharmacological emphases. O. sinensis shows preferential enrichment in immune–pulmonary–renal metabolic networks, with frequent involvement of HIF-1, AGE–RAGE, VEGF, chemokine, and inflammatory lipid pathways. This pattern suggests dominant engagement of hypoxia adaptation, vascular regulation, tissue microenvironment remodeling, and chronic inflammatory control, aligning closely with its traditional and contemporary investigation in respiratory, renal, ischemic, and fatigue-associated disorders.
In contrast, C. militaris demonstrates stronger relative representation of immune receptor signaling, oxidative-stress pathways, and metabolic enzymes, consistent with a mechanistic orientation toward immune modulation, antiviral and anticancer responses, and metabolic regulation. The prominence of TLR-associated and lipid-inflammatory pathways supports its emerging positioning as an immune-functional and anticancer medicinal fungus.
Thus, while the two species occupy overlapping regions of pharmacological network space, they exhibit distinct systems-level biases rather than functional redundancy.
3.1.3. Cordycepin Acts as a Dominant Molecular Effector Within Broader Fungal Networks
Cordycepin-centered networks display a distinct topological signature, characterized by high-centrality intracellular signaling hubs that control apoptosis, kinase cascades, and metabolic checkpoints. Compared with whole-fungus preparations, cordycepin exhibits a disproportionately strong action of caspase signaling, AMPK–mTOR, PI3K–Akt, Wnt/β-catenin, and Nrf2 pathways, indicating a more targeted regulation of intracellular stress integration, metabolic reprogramming, and survival–death switching.
These patterns support a model in which cordycepin acts as a dominant molecular effector that drives a subset of C. militaris pharmacology. However, the broader immunological, vascular, and lipid–steroid signaling observed for whole-fungus preparations likely reflects synergistic contributions from additional nucleosides, polysaccharides, sterols, peptides, and secondary metabolites. Consequently, cordycepin recapitulates but does not fully reproduce the systems-level pharmacology of C. militaris.
3.1.4. Validated Versus Predicted Networks Define Evidence Tiers
Stratification of validated and prediction-only studies demonstrates that the most frequently recurring hubs and pathways—PI3K–Akt, NF-κB/TNF, apoptosis, MAPKs, HIF-1, Nrf2, and immune signaling—are robust to evidence filtering and consistently supported by experimental data. In contrast, lower-frequency pathways are concentrated in prediction-only studies, representing hypothesis-generating extensions rather than confirmed pharmacological cores.
This separation establishes an evidence-tier framework that may guide translational prioritization: validated networks provide mechanistic foundations suitable for biomarker development and clinical positioning, whereas prediction-only networks identify directions for targeted experimental expansion.
3.1.5. Implications for Natural-Product Systems Pharmacology
Collectively, these findings position Caterpillar Fungus, Orange Cordyceps-derived products as archetypal systems-level natural therapeutics whose biological activities arise from coordinated regulation of adaptive stress-response networks. The consistent involvement of immunometabolic, redox, hypoxia, and apoptosis modules underscores their potential relevance not only for disease intervention but also for functional resilience, recovery support, and maintenance of physiological function during aging.
Moreover, the alignment between traditional tonic indications and modern network-level convergence highlights network pharmacology as a translational bridge between ethnopharmacology and molecular systems medicine, enabling rational development, standardization, and positioning of medicinal fungi.
The integrative analysis of network pharmacology data, combined with experimentally validated studies, demonstrates that Caterpillar Fungus, Orange Cordyceps, and cordycepin share a convergent mechanistic architecture centered on immune modulation, stress-kinase regulation, metabolic adaptation, mitochondrial support, and apoptosis control. The repeated identification and validation of PI3K–Akt, MAPK, NF-κB, and AMPK–SIRT1–PGC-1α pathways indicate that Orange Cordyceps acts as a systems-level adaptogenic agent, capable of normalizing physiological functions across multiple organ systems. These findings support the therapeutic potential of standardized preparations of Caterpillar Fungus and Orange Cordyceps and justify further translational research, particularly in immunometabolic and chronic inflammatory diseases.
The striking convergence across species, compounds, and diseases indicates that Caterpillar Fungus, Orange Cordyceps, and cordicepin operate as network-level adaptogens. Their actions modulate: immune homeostasis, mitochondrial resilience, redox balance, stress-kinase signaling, and metabolic efficiency. These domains correspond to the core characteristics of adaptogenic botanicals.
Although 3-deoxyadenosine undergoes rapid metabolism and has low plasma concentrations, these levels are compatible with hormetic activation of AMPK, SIRT1, and FOXO pathways—mechanisms central to metabolic and mitochondrial adaptation.
Alignment of network predictions with experimental data across diverse disease models strongly supports the robustness of the mechanistic model.
3.1.6. Limitations
Limitations of these studies include heterogeneity of extracts, target inflation bias, uneven experimental validation, and overrepresentation of cancer/inflammation models. Variability in fungal strains, extraction methods, and analytical techniques remains a challenge. More standardized preparations and human mechanistic trials are required.
As a matter of fact, all the network pharmacology studies of O. sinensis were conducted on a limited number of one (cordicepin) to 13 bioactive constituents/compounds (Table A10 and Table A11) in the total of 84 compounds identified in O. sinensis, Figure A1, Figure A2, Figure A3, Figure A4 and Figure A5, and Table A3. Many other bioactive fungi secondary metabolites (Table A3, Table A4, Table A5 and Table A6), specifically alkaloids, flavonoids, sterols, cyclodipeptides, and other bioactive O. sinensis secondary metabolites, were not included in the network analysis. That is an essential omission that may affect the outcomes of these studies, and the overall evidence supporting health claims, and medical use in drug authorities’ assessments. Most network pharmacology studies analyze only a subset of fungal metabolites because compound selection is typically based on overlap between known molecular targets and disease-associated targets. Consequently, many primary and secondary metabolites listed in Section 2.1 remain outside current network analyses because their targets are unknown. The proposed core network in these studies reflects the subset of metabolites currently under study rather than responses to the full chemical diversity of O. sinensis and C. militaris. The lack of knowledge can be overcome in future studies using various molecular biology methodologies, including transcriptome-wide microarray profiling of gene expression experiments on extracts containing all extractive constituents of O. sinensis or C. militaris, in a non-targeted study design discussed in Section 3.1.7.
3.1.7. Future Perspectives
Network pharmacology is a relatively new, biology-based interdisciplinary field that combines principles of pharmacology and systems biology to study the complex interactions between drugs, their targets (e.g., receptors or enzymes), pathological processes, and diseases within integrated, holistic systems, exploring the polypharmacology and toxicology of drugs by utilizing the computational tools and network analysis algorithms.
Depending on the aims, the design and methodology of NP studies can be specific disease-targeted or non-targeted studies, where
Disease-targeted bioinformatic-based network analysis reveals the molecular mechanisms of action, common molecular targets of active compounds, and stimulus-response coupling signaling pathways [57,60,103,140,144,174,175,177,178,179,180,181,182,183,184,185,186,187,188,189,190,191,192,193,194,195,196,197,198,199,200,201,202,203,204,205,206,207,208]. Such study design and methodology do not account for synergistic and antagonistic interactions in networks induced by various constituents of the complex, multi-component extracts, which can lead to unexpected outcomes, e.g., [246,247].Non-targeted transcriptome-wide microarray profiling of gene expression-based experiments following integrated metabolomics and network analysis, revealing all molecular targets of active compounds and their response, coupling signaling pathways. The results of these studies can predict unknown physiological functions, health consequences, and therapeutic indications due to synergistic and antagonistic interactions [171,173,246,247].Currently, all conducted network pharmacology studies on Caterpillar Fungus, Orange Cordyceps, and cordicepin are limited to disease-targeted investigations of Chinese TCM prescriptions for the treatment of kidney diseases and related disorders. Non-targeted transcriptome-wide microarray profiling of gene expression-based experiments can lead to the discovery of new therapeutic indications and functional claims.
All published network pharmacology studies of O. sinensis have a targeted design focused on a specific disease. The search for unknown therapeutic uses can be pursued by exploring alternative study designs based on gene expression, and by using transcriptomics, proteomics, and metabolomics (omics-wide array) methodologies to discover new targets associated with potential pathologies and diseases.
Further perspectives include integration of multi-omics, AI-driven causal inference, pharmacokinetic–network modeling, and biomarker-guided trials.
3.2. Nucleosides Adenosine and Cordycepin as Mediators of Adaptive Stress Response and Anti-Fatigue Activity of O. sinensis, and C. militaris
Published pharmacokinetic studies of cordycepin and adenosine show remarkable variability, with rapid metabolism, low oral bioavailability, and plasma concentrations often in the low nanomolar range [127,128,131,132]. These levels are insufficient to activate classical high-affinity adenosine receptors or produce direct pharmacological effects via receptor agonism or antagonism (Section 2.2). Purinergic receptors are important for regulating inflammation, muscle contraction, neurotransmission, and nociception. Extracellular ATP and its metabolites are the main ligands for these receptors. ATP supplementation in healthy subjects for 4 weeks did not change blood or plasma ATP concentrations. Of all ATP metabolites, only plasma uric acid levels increased significantly after the administration of 5000 mg of ATP [85]. A single oral dose of ATP is not bioavailable in healthy human subjects, which may explain why several studies failed to detect ergogenic effects of oral ATP supplementation. On the other hand, increases in uric acid after release of ATP in the proximal part of the small intestine suggest that ATP or one of its metabolites is absorbed and metabolized [84]. This implies that extensive metabolism has no effect on the bioactivity of accumulated ATP in intracellular processes, and particularly on the AMPK-mediated signaling pathway, which plays an essential role in stress response, cellular senescence, apoptosis, autophagy, angiogenesis, protein and glycogen synthesis, steroids biosynthesis, mTOR signaling, etc. [59,248] (Appendix A Figure A6, Figure A7 and Figure A8). Similarly, 3-deoxyadenosine (cordycepin), even at physiological concentrations, may compete with adenosine for receptors, thereby triggering AMPK- and AKT (protein kinase B)-mediated intracellular signaling pathways. Some predicted kinase interactions may not be directly achievable at physiological concentrations, and indirect or systems-level mechanisms may contribute to biological activity. Further studies are required, as physiological concentrations of cordycepin are essential for experimental evidence supporting our hypothesis. For comparison, Ginsenoside Rg5 in physiological concentrations (nM-pM-fM) significantly deregulates gene expressions in brain cell culture [173].
These nucleosides fall within the range where hormetic activation of metabolic stress-response pathways, such as AMPK, SIRT1, TIGAR, and PGC-1α, occurs. Thus, the inconsistencies in pharmacokinetic and pharmacodynamic characteristics of cordycepin are not contradictory but relatively entirely consistent with the concept that cordycepin functions as a metabolic adaptogen with a biphasic hormetic dose–response. Cordycepin may act as a driver, triggering the organism’s adaptive stress response in stress-induced and aging-related diseases.
The lack of correlation between plasma cordycepin concentration and biological outcomes indicates that it does not act through linear, dose-dependent pharmacology but rather through multi-target metabolic adaptation, characteristic of adaptogenic botanicals. In this context, even low, transient, and variable systemic exposures can induce stable improvements in transcription and mitochondrial function.
Cordycepin exhibits a genuine adaptogenic profile driven by low-dose hormetic activation of metabolic resilience pathways, particularly AMPK, SIRT1, PGC-1α, and TIGAR. Although it lacks CNS stimulant effects and does not act via adenosine receptors, cordycepin enhances mitochondrial efficiency, improves ATP production, and increases resistance to physical and metabolic stress. Within C. militaris or O. sinensis extracts, synergistic interactions among multiple constituents amplify these effects, providing a biologically plausible explanation for the anti-fatigue and performance-enhancing outcomes observed in animal and human studies.
Cordycepin exerts effects through peripheral metabolic enhancement, mitochondrial biogenesis, and hormetic stress adaptation rather than through central adenosinergic stimulation. Cordycepin acts as a low-dose metabolic hormetic agent, while Orange Cordyceps and Caterpillar Fungus extracts display multi-target synergy that cannot be explained by nucleosides alone. This framework resolves the apparent contradictions between cordycepin’s limited CNS pharmacology and the robust anti-fatigue outcomes observed in animals and humans.
3.3. Western Regulatory vs. Traditional Medical Paradigms
TCM and Ayurveda are based on a holistic and integrative approach, multi-target and polyvalent action [134], but they rely on archaic theories. In contrast, Western conventional medicine, based on a reductional approach, selective targeting, and specific action in the treatment of diseases, relies on another archaic theory of galenic preparations that ignores interactions and overlaps among regulatory systems and the effects of other constituents in multi-component plant extracts. In fact, both approaches are complementary, particularly in the treatment of diseases of complex pathology associated with the stress system interacting with other regulatory systems. The concomitant administration of several Western conventional medicines that selectively act on various receptors provides more effective treatment in hypertension, post-stroke rehabilitation, viral infections, etc. The “ready for use” of complex botanicals and botanical hybrid products used in the Eastern world acts similarly. The challenge is to understand the mechanisms of action and scientifically validate their efficacy, quality, and safety by strengthening the integration of TCM into European health systems, improving quality control, conducting randomized clinical trials, and improving regulatory standards [249].
The concept of adaptogens originated in Eastern medical and pharmacological traditions and describes natural products that increase an organism’s capacity to maintain physiological homeostasis under conditions of stress [28,135]. In this framework, stress is understood as a multisystem challenge that affects neuroendocrine regulation, energy metabolism, immune competence, and cognitive and physical performance, particularly in aging and stress-exposed populations [229,230,250,251,252,253,254,255,256].
While adaptogens are commonly recognized as a pharmacological category in several non-European regulatory and medical systems [256,257,258,259,260,261,262,263,264], they are not formally acknowledged within EFSA or EMA frameworks. The term “adaptogen” is considered not appropriate for a marketing authorization within EFSA or EMA frameworks [241], which require substantiation of discrete, well-defined physiological endpoints and do not evaluate systems-level concepts such as adaptation or stress resilience [238,239,240]. As a consequence, holistic or systems-level constructs such as “adaptation”, “stress resilience”, or “anti-fatigue” cannot be evaluated as such under current EU food or medicinal product legislation.
Importantly, the lack of regulatory recognition does not imply scientific invalidity of the adaptogen concept but rather reflects methodological constraints of existing regulatory paradigms.
In summary, the adaptogen concept represents a systems-level interpretation of complex physiological responses, whereas EFSA evaluation operates at the level of single, well-defined functional outcomes. By translating adaptive effects into EFSA-recognized physiological functions—such as physical performance or perceived exertion—it is possible to preserve scientific validity while remaining compliant with regulatory requirements.
This translational framework enables constructive dialogue between scientific innovation and regulatory practice, without forcing premature or inappropriate reclassification of complex biological concepts.
3.4. Resilience Biology as the Missing Regulatory Construct
The findings of this review indicate that the regulatory marginalization of adaptogens in Europe does not arise from a lack of biological plausibility, but from a structural gap in regulatory concepts. Inflammation and stress responses are both evolutionarily conserved adaptive systems with active resolution mechanisms [229,230,231,232,233,234,235,236]; however, only inflammation is formally recognized as a regulatable pathological entity within European frameworks [238].
Adaptogenic botanicals consistently demonstrate modulatory effects across immune, inflammatory, neuroendocrine, and metabolic systems [26,28,134]. These effects are bidirectional, context-dependent, and primarily aimed at restoring homeostasis rather than suppressing specific pathways. Such characteristics align poorly with disease-centric regulatory logic but are fully consistent with contemporary systems biology, allostasis, and resilience theory [232,265].
Asian medical systems have long operationalized this concept by framing health as adaptive capacity rather than the absence of disease [244]. In contrast, European regulation—despite recognizing allostasis, inflammation resolution, and psychoneuroimmunology at the scientific level—lacks a functional category that allows these principles to be translated into health claims or product classifications [238,239,240]
3.4.1. Why a Hybrid EU–Asia Model Is Scientifically Justified
A hybrid EU–Asia regulatory model reconciles two complementary strengths: the European emphasis on safety, standardization, and evidentiary rigor, and the Asian emphasis on functional balance, recovery, and resilience embedded in traditional medical systems [26,28,134,244,264,265].
This review demonstrates that adaptogens act upstream of pathology by supporting recovery kinetics, physiological flexibility, and stress-response resolution—features increasingly recognized as determinants of long-term health outcomes [232,265]. These effects are not adequately captured by current EU categories, such as vitamins, antioxidants, or anti-inflammatory agents, which are anchored in deficiency-correction or pathway-inhibition models [238,239,240]. Nevertheless, adaptogenic effects can be measured using non-disease endpoints, including return-to-baseline time, performance maintenance under load, and immune homeostasis markers [26,28].
Importantly, the proposed hybrid model does not dilute regulatory rigor. Rather, it reallocates evidentiary focus from disease endpoints to functional adaptation metrics, maintaining consumer protection while enabling scientific innovation consistent with systems biology.
3.4.1.1. Resilience-Supporting Physiological Modulators as a Regulatory Bridge
The proposed category of resilience-supporting physiological modulators (RSPMs) offers a legally conservative yet biologically modern solution. By explicitly excluding disease prevention or treatment claims, this category preserves the boundary between food supplements and medicines while legitimizing claims related to recovery, homeostasis, and adaptive capacity. Such a category would be compatible with the existing institutional roles of the European Food Safety Authority—responsible for safety evaluation and health-claim substantiation—and the European Medicines Agency, which oversees the boundary between functional and pharmacological activity [238,239,240,241]. Asian regulatory frameworks would serve as functional reference models rather than direct validation pathways, allowing integration without undermining EU legal coherence.
Further expert consensus guidelines can be developed to focus on the selection and justification of outcome measures and endpoints across various stress-induced and aging-related health conditions, and to propose measurable resilience-related biomarkers as candidate endpoints to operationalize the proposed resilience-supporting physiological modulator (RSPM) framework. The criteria for resilience and the biomarker set are similar to those summarized in a recent review on adaptogens [26], including recovery indices in chronic unpredictable stress (CUS) animal models, which induce affective behaviors in mice and, once established, measure stress-related alterations in the intrinsic excitability and synaptic regulation of the medial prefrontal cortex layer pyramidal neurons, cortisol recovery kinetics, cytokine balance ratios, and adaptive stress–response signaling pathways markers, e.g., G-protein coupled (GPCR), tyrosine, toll-like receptors, and I3PK-AKT, AMPK-mediated pathways known to promote survival in response to stress, suggesting neuroprotective activity and the potential benefits of adaptogens in neurodegenerative diseases.
3.4.1.2. Regulatory Language as a Determinant of Scientific Visibility
One of the essential points of this review is that language—not evidence—is the principal barrier to adaptogen acceptance for marketing authorization in Europe. Terms such as anti-stress or adaptogenic for marketing authorization are rejected not because stress biology is unrecognized, but because stress is classified as a normal life condition rather than a regulatable physiological domain [238,239,240,241]. The hybrid model resolves this tension by shifting the claim architecture toward supporting normal physiological function during periods of increased demand, a formulation already consistent with European health-claim jurisprudence. This reframing allows resilience biology to be communicated without encroaching on medical or psychological claims, thereby increasing regulatory acceptability while preserving scientific meaning.
3.4.2. Outlook and Future Directions
3.4.2.1. From Disease Regulation to Health Maintenance
European regulatory systems are approaching a conceptual inflection point. As chronic, lifestyle-associated conditions increasingly dominate healthcare burden, the inability to regulate interventions that support recovery and adaptive capacity represents a growing limitation (Furman et al., 2019) [265]. Resilience biology provides a scientifically grounded framework to address this gap.
The hybrid EU–Asia model outlined here offers a pathway to transition from a purely disease-reactive paradigm toward health-maintenance regulation, without compromising evidentiary standards or public safety.
3.4.2.2. Implications for Regulatory Science
Future regulatory development should prioritize:
- Formal recognition of homeostasis and recovery as legitimate physiological outcomes;
- Acceptance of systems-level functional endpoints alongside classical biomarkers;
- Development of claim guidance specific to resilience-supporting functions.
Pilot implementation through emerging-science claim pathways, limited botanical lists, and post-market monitoring would allow regulatory learning while maintaining risk control [238,239,240].
3.4.2.3. Implications for Research and Industry
Adoption of a resilience-focused regulatory category would incentivize improved human study designs using load-and-recovery paradigms, better standardization of complex botanical preparations, and closer integration of traditional knowledge with modern clinical research [26,244]. This would reduce the current disconnect between scientific evidence, regulatory acceptance, and consumer communication.
3.4.2.4. Concluding Perspective
The regulatory challenge posed by adaptogens is not an anomaly but a signal: modern biology has outgrown purely disease-centric regulation. A hybrid EU–Asia regulatory model integrating resilience biology would align policy with science, recognize health as a dynamic adaptive process, and provide a coherent framework for interventions that maintain function rather than treat pathology.
Resilience is not an alternative to medicine; it is the biological foundation upon which medicine succeeds.
4. Materials and Methods
This mixed-methods review explores evidence from 9 systematic clinical and 37 network pharmacology studies on O. sinensis, C. militaris, and cordycepin, extracting active compounds, disease indications, predicted targets, enriched signaling pathways, and mechanistic conclusions to elucidate their molecular actions in diseases treated in TCM. A systematic review of meta-analyses of randomized controlled trials (RCTs) was conducted to evaluate the efficacy, safety, quality control practices, and compliance with EMA criteria for well-established herbal medicinal products. Data synthesis included pooled effect-size estimation and risk-of-bias assessment using Cochrane methods. A structured umbrella review approach was applied to peer-reviewed reviews addressing inflammation, stress physiology, adaptogens, and regulatory science. Regulatory guidance from EFSA, EMA, FDA, and Asian authorities was examined, and findings were narratively synthesized.
4.1. Literature Search
This review thoroughly explores the current evidence on the network pharmacology studies of O. synensis, C. militaris, and cordycepin, covering publications from 2010 to 2025 and addressing inflammation, stress physiology, adaptogens, and regulatory science. Regulatory guidance from EFSA, EMA, FDA, and Asian authorities was examined. Findings were narratively synthesized. A search was conducted using several major databases and platforms, including PubMed, Google Scholar, ScienceDirect, Scopus, CNKI, and Web of Science, as well as the Google search engine, the National Library of Medicine, regulatory documents from EFSA, EMA, FDA, and Asian health authorities, and the ChatGPT AI technology.
The search strategy involved targeted use of keywords such as “Ophiocordyceps sinensis”, “Cordyceps militaris” (L.), “network pharmacology,” “randomized” AND “health claims”, “indications” AND “pharmacopeia”, AND “dietary supplements”. The search was limited to English-language publications within the specified period. The review process adhered to EMA guidelines, and the quality of the studies was evaluated using CONSORT and Cochrane standards.
4.2. Inclusion and Exclusion Criteria
4.2.1. Inclusion Criteria
For network pharmacology synthesis:
- Studies explicitly performing target prediction and pathway enrichment analyses.
- Studies identifying protein–protein interaction (PPI) networks.
- Studies reporting enriched KEGG/GO pathways.
- Studies involving O. sinensis, C. militaris, or cordycepin as primary exposure.
For experimental validation:
- In vitro or in vivo confirmation of predicted targets/pathways.
- Clear reporting of biological endpoints.
- Mechanistic linkage to predicted signaling hubs.
For clinical evaluation:
- Randomized controlled trials (RCTs).
- Systematic reviews or meta-analyses.
- Clearly defined preparation type.
4.2.2. Exclusion Criteria
Reviews without primary mechanistic data.Studies lacking explicit pathway enrichment methods.Case reports without mechanistic evaluation.
4.3. Data Extraction
Data extraction covered: major active compounds/ligands, disease indications, predicted molecular targets, enriched signaling pathways, docking scores, and presence of experimental validation. Target convergence and pathway frequency analyses were performed to identify core mechanistic hubs.
Included studies employed network pharmacology tools such as target prediction algorithms, KEGG/GO pathway enrichment, molecular docking, transcriptomics, metabolomics, or integrated multi-omics. Ten studies with experimental validation—including cellular assays, animal disease models, and clinical observations—were also included.
Reviews addressing inflammation resolution, stress biology, adaptogens, or regulatory frameworks were also included. Findings were narratively integrated across biological, clinical, and regulatory domains.
4.4. Data Integration and Evidence Integration Strategy
All AI-assisted frequency aggregation was manually verified against original publications to prevent duplication or misclassification.
Thirty-seven network pharmacology studies were identified. For each study:
- Predicted targets were extracted.
- Enriched pathways were recorded.
- Frequency of pathway recurrence across independent studies was counted.
To reduce “target inflation bias,” predicted targets were stratified according to validation level:
- In silico prediction only;
- Experimentally validated (cellular or animal models);
- Clinically supported endpoints.
Targets and pathways were aggregated across studies. Mechanistic convergence was assessed by frequency. Experimental studies were cross-mapped onto predicted networks. Heatmaps (Figure 4) represent recurrence frequency across independent publications, not gene expression magnitude.
AI-assisted tools were used exclusively for structured aggregation and visualization of manually extracted data. Literature identification, study selection, and data extraction were performed manually from full-text publications. Extracted variables (intervention, targets, enriched pathways, validation status, and study identifiers) were compiled into standardized tables (Table A10 and Table A11) prior to AI processing. AI was subsequently used only to compute recurrence frequencies, stratify findings by evidence tier, and generate graphical heatmaps (Figure 4). No automated literature screening, target prediction, or mechanistic interpretation was performed by AI. All aggregated outputs were manually cross-verified against the original dataset to prevent duplication or misclassification.
5. Conclusions
Many reviews on various aspects of the medical mushroom O. sinensis, which has historically been recognized in Asian traditional medical systems for its ability to enhance vitality, describe pleiotropic therapeutic applications. However, the polyvalent adaptogenic potential of O. sinensis has not been systematically proven, and a consolidated mechanistic synthesis integrating both network predictions and experimental validation is lacking. This review, for the first time, shows that:
- O. sinensis, C. militaris, and cordycepin share a common adaptogenic mechanism of maintenance of cellular and integrated biology system functions homeostasis.
- The systems-level adaptogenic mechanism of these fungi is characterized by their ability to modulate multiple interconnected biological networks rather than acting on a single target.
- This is in line with TCM and Ayurveda holistic concepts and the modern concept of pleiotropic therapeutic activity of adaptogens and particularly of O. sinensis.
- The review reveals controversy regarding the bioavailability of cordycepin in vivo and its concentration in vitro studies, raising the hypothesis that cordycepin may act as a driver, triggering the organism’s adaptive stress response in stress-induced and aging-related diseases.
- Nucleosides, adenosine and cordycepin, along with other adaptogenic botanical metabolites (steroids and phenolics), contribute to the maintenance of cellular and integrated biology system functions homeostasis.
- Network pharmacology studies identify multi-target pathways, including convergent hubs, such as PI3K-Akt, AMPK–mTOR, MAPK, apoptosis, Nrf2 and AMPK–SIRT1–PGC-1α pathways.
- By influencing pathways associated with immune regulation, mitochondrial function, and metabolic adaptation, they orchestrate a holistic response that enhances the organism’s resilience to various stressors.
- This integrative effect is especially significant in the context of complex disorders, where multifactorial interventions are necessary for effective therapeutic outcomes.
- This is the first comparative meta-analysis of validated vs. predicted effects of O. sinensis, C. militaris and species-level versus cordycepin-driven mechanisms.
- Validation studies confirm predictions across chronic obstructive pulmonary disease, pulmonary arterial hypertension, cancer, obesity, influenza, and immunogenicity.
Caterpillar Fungus, Orange Cordyceps, and 3-deoxyadenosine exhibit a unified adaptogenic pharmacology that involves immune modulation, mitochondrial enhancement, stress-signal regulation, and metabolic homeostasis. These effects arise through multi-target synergy across PI3K–Akt, MAPK, NF-κB, apoptosis, and AMPK–SIRT1–PGC-1α pathways. The meta-analysis of network pharmacology studies suggests that O. sinensis and C. militaris act as multi-compound immunometabolic regulators, while cordycepin functions as a dominant molecular effector controlling apoptosis, metabolism, and adaptive stress signaling. The strong convergence of network and experimental evidence supports their potential in immunometabolic and stress-related disorders. Distinguishing validated from predicted networks is essential for translational reliability.
Results of network pharmacological studies of OS, CM, and CC that demonstrate activation of adaptive extracellular and intracellular signaling pathways, key mediators, and physiological functions are associated with pleiotropic health effects.
Clinical efficacy of OS, CM, and CC is noticed in stress-induced physical and cognitive fatigue, mental and immune disorders; these studies are limited to physical fatigue in healthy individuals, chronic kidney disease, respiratory conditions, and cancer adjunct therapy.
The effects of cordycepin were demonstrated in micromolar concentrations in vitro cell models. Clinical and pharmacokinetic studies show that high concentrations of cordycepin, adenosine, and their bioactive metabolites, ATP and CTP, in blood circulation cannot be achieved with therapeutic doses of O. sinensis and C. militaris due to intensive enzymatic metabolism and renal clearance. However, since ATP, adenosine, cordycepin, and other purine metabolites are involved in numerous physiological processes and exert pharmacological effects, we can hypothesize that they trigger these effects at physiological nanomolar concentrations. Cordycepin may function as a systems-level metabolic trigger rather than as a classical high-affinity receptor ligand.
The adaptogenic concept represents a systems-level interpretation of complex physiological responses characteristic of holistic TCM and Ayurvedic concepts, whereas European Food Safety Authority regulatory frameworks lack concepts for resilience and adaptive capacity and operate at the level of single, well-defined functional outcomes, which raises regulatory issues for food and drugs in Western countries.
This review clarifies conceptual and regulatory barriers to recognizing resilience-supporting interventions and informs future regulatory innovation. The review for the first time suggests establishing a regulatory category for resilience-supporting physiological modulators that could align food and drug regulation in the EU with contemporary systems biology, thereby complementing EFSA, EMA, FDA, and Asian authorities.
Numerous critical appraisals and limitations were discussed above in detail across the sections on clinical and network pharmacology, as well as in the regulatory framework. Future perspectives of primary importance include integrating TCM into European health systems, improving quality control, conducting randomized clinical trials effectively, strengthening regulatory standards, and the wide implementation of network pharmacology study design and methodology, which account for synergistic and antagonistic interactions by various constituents of the complex, multi-component extracts, which can lead to unexpected outcomes. They include transcriptome-wide microarray profiling of gene-expression-based experiments, integrated with metabolomics and network analyses, revealing all molecular targets of active compounds and coupling signaling pathways to final outcomes. The results of these studies can reveal unknown health consequences and therapeutic indications, leading to new drug discoveries.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Taxonomy Browser: Ophiocordyceps sinensis NCBI, National Library of Medicine Bethesda, MD, USA Available online: https://www.ncbi.nlm.nih.gov/Taxonomy/Browser/wwwtax.cgi?mode=Info&id=72228(accessed on 21 January 2026)
- 2Taxonomy Browser: Cordyceps militaris NCBI, National Library of Medicine Bethesda, MD, USA Available online: https://www.ncbi.nlm.nih.gov/Taxonomy/Browser/wwwtax.cgi?command=show&mode=node&id=73501&lvl=(accessed on 21 January 2026)
- 3Botanical Drug Development Guidance for Industry FDA Silver Spring, MD, USA 2016 Available online: https://www.fda.gov/files/drugs/published/Botanical-Drug-Development--Guidance-for-Industry.pdf(accessed on 21 January 2026)
- 4Ahmadjian V. Alexopoulos C.J. Moore D. Fungus. Encyclopaedia Britannica 2025 Available online: https://www.britannica.com/science/fungus(accessed on 21 January 2026)
- 5Moore D. Encyclopaedia Britannica Outline of Classification of Fungi 2025 Available online: https://www.britannica.com/science/fungus/Outline-of-classification-of-fungi(accessed on 21 January 2026)
- 6Petruzzello M. Encyclopaedia Britannica Cordyceps 2025 Available online: https://www.britannica.com/science/cordyceps(accessed on 21 January 2026)
- 7Winkler D. Cordyceps sinensis (Berk.) Sacc.: Economy, Ecology, and Ethno-Mycology of Yartsa Gunbu, a Medicinal Fungus Endemic for the Tibetan Plateau Int. J. Med. Mashrooms 2005748148210.1615/Int J Med Mushr.v 7.i 3.1100 · doi ↗
- 8Winkler D. Caterpillar Fungus production and sustainability on the Tibetan Plateau and in the Himalayas Asian Med.2009529131610.1163/157342109 X 568829 · doi ↗