Clinical Manifestations of Lyme Borreliosis in Europe: Burden of Lyme Disease Study (BOLD), 2021–2022
Kate Halsby, Alexandra Loew-Baselli, Franc Strle, Anna Moniuszko-Malinowska, Johan Sanmartin Berglund, Viliam Cibik, Dagmar Zakova, Ye Tan, Frederick J. Angulo, Juanita Edwards, Andreas Pilz, Brad D. Gessner, Elizabeth Begier, James H. Stark

TL;DR
This study analyzed the clinical manifestations of Lyme disease across six European countries, finding significant variation in symptoms and treatment patterns.
Contribution
The study provides the first comprehensive, multi-country analysis of Lyme disease manifestations in Europe using standardized case definitions.
Findings
Erythema migrans was the most common manifestation in most countries, but Lyme arthritis dominated in Slovakia.
The proportion of disseminated disease varied widely, from 1.1% in Slovenia to 78.0% in Slovakia.
Doxycycline was the most commonly prescribed antibiotic across all countries.
Abstract
Lyme borreliosis (LB), the most common European tick-borne disease, can manifest as an erythema migrans (EM) rash or as disseminated LB. The prospective Burden of Lyme Disease (BOLD) study evaluated the frequency of LB clinical manifestations, including signs, symptoms, and treatment patterns in 14 healthcare practices in endemic regions of six European countries: the Czech Republic, Germany, Poland, Slovakia, Slovenia, and Sweden. Between April 2021 and December 2022, patients with suspected LB were evaluated using predefined case definitions that were applied by investigators to identify medically attended LB cases. Enrolled cases were interviewed about their symptoms. Among the 797 LB cases, 615 (77.2%) had EM and 182 (22.8%) had disseminated disease; 154 of the disseminated cases had Lyme arthritis (LA), five had Lyme neuroborreliosis, and three had Lyme carditis. Geographically,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
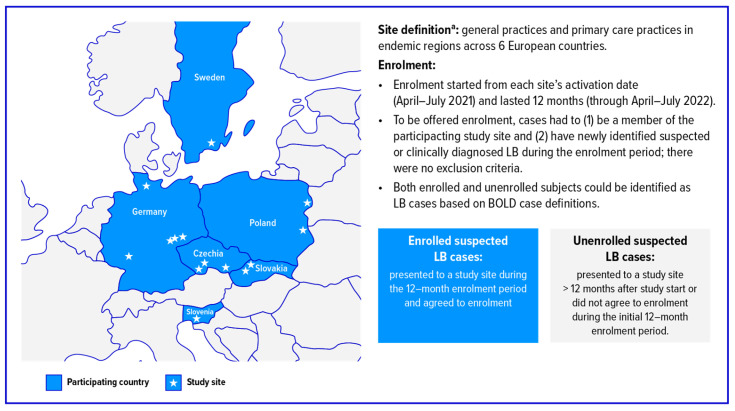 Figure 1
Figure 1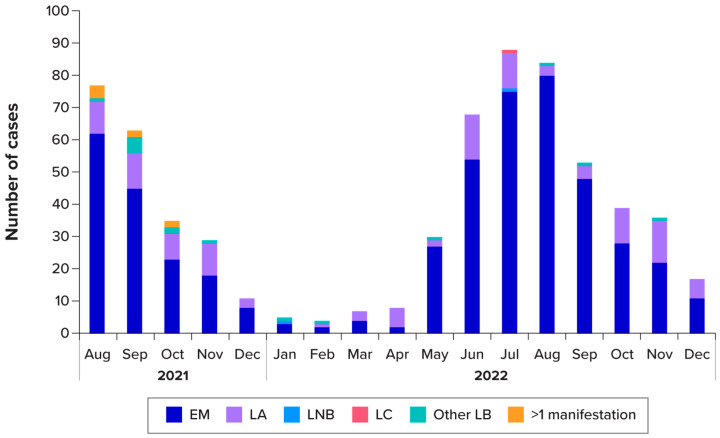 Figure 2
Figure 2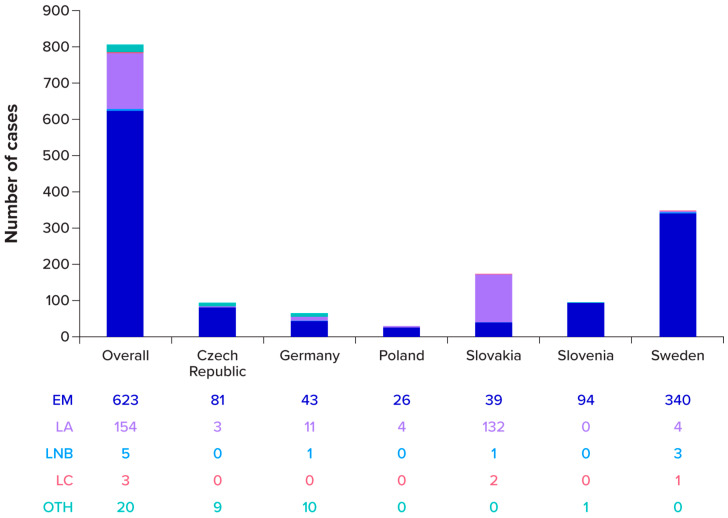 Figure 3
Figure 3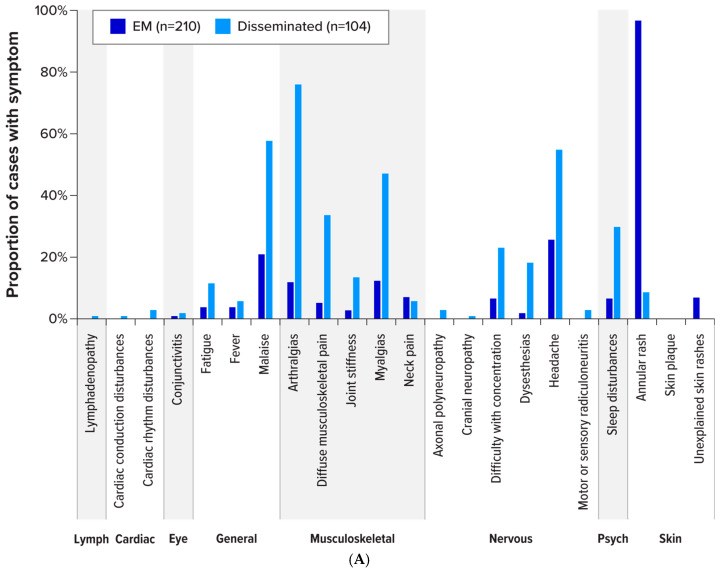 Figure 4
Figure 4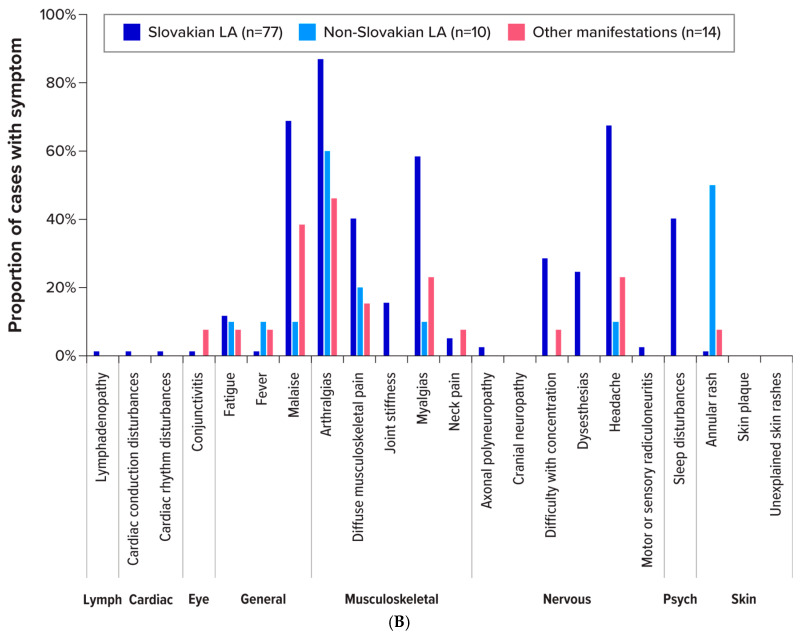 Figure 5
Figure 5 Figure 6
Figure 6- —Valneva
- —Pfizer
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVector-borne infectious diseases · Zoonotic diseases and public health · Parasitic Diseases Research and Treatment
1. Introduction
Tick-borne illnesses are a major health concern across Europe, and climate is likely changing the density and range of infection-carrying tick vectors [1]. The most common tick-borne illness in Europe is Lyme borreliosis (LB), which is caused by certain genospecies of Borrelia burgdorferi sensu lato [1]. The clinical presentation of LB varies; however, symptoms typically emerge within 30 days of infection. Erythema migrans (EM), a hallmark skin rash observed in most patients with LB, often serves as a key diagnostic factor for localised cases of infection [2,3,4]. Although the majority of LB cases can be effectively treated with an appropriate course of antibiotics [5], those with untreated infection may develop manifestations of disseminated disease [4].
Disseminated LB can impact the musculoskeletal, nervous, and cardiovascular systems, potentially causing serious long-term health effects [2,3,4]. For example, Lyme arthritis (LA) makes up approximately 28% of all LB reported to the Centers for Disease Control and Prevention (CDC) in the United States of America [6,7]. In Europe, that proportion is lower, with a range of estimates varying by country; 0.6% in Slovenia [8], 2.1% in Germany [9], 13.6% in Norway [10], and 17% in Italy [11]. Lyme neuroborreliosis (LNB) can result in painful radiculitis, peripheral facial nerve palsy, and lymphocytic meningitis [12,13], whereas Lyme carditis (LC) usually manifests with heart block [14].
Information on the relative frequency of LB clinical manifestations is limited in Europe due to differences in diagnostic practices and surveillance approaches [8,9,10,15,16,17,18,19,20]. Thus, there is a need for clearer estimation of the frequency of LB manifestations across Europe. To address the challenges posed by differing case definitions and methodologies, the prospective Burden of Lyme Disease (BOLD) epidemiology study was conducted using a standardised surveillance approach and unified case definitions [21]. This methodology permitted comparison of data across endemic regions in 6 European countries: the Czech Republic, Germany, Poland, Slovakia, Slovenia, and Sweden [21]. Data from the BOLD study on the incidence of LB, the diagnostic testing, the patient-reported outcomes, and the cases with Post Treatment Lyme Disease Syndrome will be published elsewhere. Herein, we present the frequency of LB manifestations, including signs and symptoms in BOLD, as well as antibiotic treatment patterns by country. These insights aim to provide a more comprehensive understanding of LB disease burden in six European countries.
2. Materials and Methods
2.1. Study Design, Setting, and Participants
Detailed BOLD study methodology has been previously published [21], including site descriptions, surveillance period, and case definitions (Figure 1 and Table S1). In brief, this prospective, active surveillance, epidemiological study was conducted at 14 general practices/primary care practices located in Lyme-endemic areas in the Czech Republic, Germany, Poland, Slovakia, Slovenia, and Sweden. The study sought to identify medically attended LB cases, which include those subjects who sought medical care at their participating clinic and received a clinical diagnosis of EM or a clinical and standard of care laboratory diagnosis of disseminated disease (except multiple EM lesions or disseminated cases with an EM rash, which could be clinically diagnosed) according to the BOLD case definitions (Table S1). Study-site personnel received standardised training on screening and diagnosis of LB using these definitions. Active surveillance and study enrolment began on the activation date for each site, which ranged between April and July 2021, and continued for 12 months. Active surveillance (without enrolment) then continued until the end of 2022. During the initial 12-month period, all patients with suspected LB were offered informed consent before enrolment. Enrolled patients completed a questionnaire on medical history, signs and symptoms, and treatment, and were evaluated at up to five study visits. Visit 1 was at enrolment; visits 2 and 3 occurred 28 days and 10 months, respectively, after visit 1; and visits 4 and 5 were only for LB cases with ongoing symptoms and took place in months 16 to 24 after visit 1. The date of diagnosis was typically the date of visit 1 for newly presenting patients (or could precede the first study visit for cases seen outside the general practitioner’s practice), although it could occur at any time up to visit 2, depending on laboratory diagnostics.
Patients with suspected LB were identified through routine patient tracking or medical records during the active surveillance period. All patients with suspected LB received a final diagnosis of LB (i.e., cases) or “Not LB” based on unified case definitions (Table S1). LB cases were further classified as having disseminated disease if they had LA, LNB, LC, ocular manifestations, acrodermatitis chronica atrophicans, or more than one manifestation. The classification of manifestation was a clinical decision based on the case definitions outlined in the protocol (Table S1), and the final decision was made by primary site investigators. LB diagnoses without established LB clinical manifestations (as defined in Table S1) were also recorded if the subject had a laboratory confirmation. The BOLD study aimed to capture and describe non-traditional presentations of LB and therefore allowed clinical judgement in this more loosely defined group of patients. These cases were given a manifestation classification of “other” and included subjects with, e.g., systemic symptoms or multiple EM.
Local ethics committees for each participating site approved this study, and enrolled participants provided written informed consent [21]. The study complied with legal and regulatory requirements, the International Ethical Guidelines for Biomedical Research Involving Human Participants, the International Council for Harmonisation Good Clinical Practice Guideline, and the Declaration of Helsinki.
2.2. Analyses
Analyses were conducted using available data, and subjects with missing data were excluded from the affected analyses. One asymptomatic subject was identified following a routine blood draw for non-study–related purposes and was given an LB diagnosis by site investigators. This subject was excluded from the manifestations, as well as the signs and symptoms analysis. All analyses were descriptive, and no formal statistical hypothesis testing was performed. The analyses were performed using Statistical Analysis System (SAS) software (version 9.4).
3. Results
The BOLD study identified 797 medically attended LB cases: 342 in Sweden, 173 in Slovakia, 95 in Slovenia, 94 in the Czech Republic, 63 in Germany, and 30 in Poland (Table S2). Over half (n = 436 [54.7%]) of cases were female, and 331 cases (41.5%) were aged 45–64 years. A total of 315 medically attended LB cases agreed to enrol in the study, with the majority coming from Slovakia (n = 107/315 [34.0%]) and Sweden (n = 104/315 [33.0%]). More females enrolled than males (enrolled: female = 179/315 [56.8%], male = 136/315 [43.2%]; unenrolled: female = 257/482 [53.3%], male = 225/482 [46.7%]), a slightly higher proportion of the enrolled cases fell into the ≥45-year age groups (enrolled 45–64 years = 137/315 [43.5%], ≥65 years = 100/315 [31.7%]; unenrolled 45–64 years = 194/482 [40.2%], ≥65 years = 147/482 [30.5%]), and 33.3% (105/315) of enrolled cases had disseminated disease compared with 16.0% (77/482) of unenrolled cases.
3.1. Key Medical History
Medical history was available for each of the 315 enrolled medically attended LB cases, of whom 182 (57.8%) reported a history of tick bites in the years prior to the current LB diagnosis. Of those reporting a history of prior tick bites (lifetime), the median number of tick bite episodes was 10 (interquartile range, 2 to 90). Forty-five subjects reported ≥100 tick bites (44 from Sweden and 1 from Slovenia).
Over a third of enrolled cases had a previous history of LB (n = 112 [35.6%]). Eighty-three cases reported a total of 137 previous EM episodes; of these, 30 were medically confirmed (including 10 laboratory confirmed) and 107 were self-reported. Similarly, 39 enrolled cases reported 46 total previous episodes of disseminated disease; of these, 37 were medically recorded (including 28 laboratory confirmed) and nine were self-reported.
3.2. Cases with EM and Disseminated LB
Among the 797 medically attended LB cases, 615 (77.2%) had EM manifestations, 181 (22.7%) had disseminated disease, and one presented asymptomatically (Table S2). More females presented with EM (females = 352/436 [80.7%] and males = 263/360 [73.1%]), whereas more males had disseminated LB (females = 84/436 [19.3%] and males = 97/360 [26.9%]). Most cases of EM and disseminated disease occurred among participants aged ≥45 years (EM: ≥45 years = 437, 0–44 years = 178; disseminated: ≥45 years = 140, 0–44 years = 41). Geographically, over half of the EM cases were reported in Sweden (n = 334), followed by Slovenia (n = 94), the Czech Republic (n = 81), Germany (n = 42), Slovakia (n = 38), and Poland (n = 26). Nearly 75% of the disseminated cases were reported in Slovakia (n = 135), whereas other countries reported far fewer: 21 cases in Germany, 12 in the Czech Republic, eight in Sweden, four in Poland, and one in Slovenia.
3.3. Manifestations of LB
LB manifestations by subject are summarised in Table 1. Of the 796 LB cases (excluding 1 asymptomatic Borrelia infection), 615 (77.3%) had EM, 147 (18.5%) had LA, four (0.5%) had LNB, two (0.3%) had LC, 19 (2.4%) had no established LB clinical manifestations (“other”), and 9 (1.1%) reported more than one manifestation: EM and LA (n = 6); EM and LC (n = 1); EM and LNB (n = 1); and LA and unspecific general symptoms (n = 1). The proportion of subjects presenting with an EM (including those with more than one manifestation) outside Slovakia was 584/623 (93.7%). Both disseminated and EM cases occurred year-round, with most cases diagnosed in the spring and summer months before gradually tapering through the autumn and winter (Figure 2).
When individual manifestations are counted (so that subjects with >1 manifestation are counted more than once), there were a total of 805 manifestations among the 796 cases: EM, n = 623 (78.3%); LA, n = 154 (19.3%); LNB, n = 5 (0.6%); LC, n = 3 (0.4%); and no established LB clinical manifestations (“other”), n = 20 (2.5%) (Table 1). These manifestation counts are depicted in Figure 3 by country. For the two most prevalent manifestations, EM and LA, the majority of occurrences were reported in Sweden (n = 340) and in Slovakia (n = 132), respectively.
3.4. Signs and Symptoms of LB
There were 314 enrolled LB cases with information on signs and symptoms (excluding the single asymptomatic infection). Among enrolled cases with a manifestation of EM (n = 210), 203 (96.7%) presented with an annular rash, 15 reported an “unexplained skin rash,” and one reported a “skin plaque.” Other symptoms reported by a large proportion of EM cases included headache (n = 54 [25.7%]) and malaise (n = 44 [21.0%]) (Figure 4A and Table S3). Of enrolled cases with disseminated LB (n = 104), the most commonly reported symptoms were arthralgias (n = 79 [76.0%]), malaise (n = 60 [57.8%]), headache (n = 57 [54.8%]), myalgias (n = 49 [47.1%]), diffuse musculoskeletal pain (n = 35 [33.7%]), sleep disturbances (n = 31 [29.8%]), and difficulty with concentration (n = 24 [23.1%]). Symptoms varied by manifestation (Table S3). Signs and symptoms were recorded for the 12 enrolled cases with no established LB clinical manifestations (“other”); the “other” cases comprised one case with multiple EMs and 11 cases with musculoskeletal and/or general symptoms (Table S3).
LA was the most reported disseminated manifestation among LB cases, and Slovakia had more LA cases than any other country. The signs and symptoms of enrolled LA cases in Slovakia (n = 77) were compared with those of enrolled LA cases outside Slovakia (n = 10) (Figure 4B). Notably, malaise was reported in 68.8% (n = 53) of LA cases in Slovakia (and 10.0% [n = 1] of LA cases outside Slovakia). There were 58 LA cases in Slovakia that presented with nervous system symptoms, including difficulty with concentration (28.6% [n = 22]), dysesthesia (24.7% [n = 19]), and headache (67.5% [n = 52]). The only nervous system symptom reported by LA cases outside Slovakia was headache (10% [n = 1]). One LA case (1.3%) in Slovakia and five LA cases (50%) outside Slovakia reported a rash (all six cases were classified as having more than one manifestation). Cases with LB clinical manifestations that did not fall within pre-specified categories (“other”) reported predominantly generalised and musculoskeletal symptoms with some nervous system symptoms, and one case reported a multiple EM rash (which is considered a disseminated LB manifestation).
The mean time from symptom onset to LB diagnosis was 16.5 days (13.4 days for those with EM and 24.9 days for disseminated disease). Those with “other” manifestations had the longest time from onset to diagnosis (mean, 38.5 days), followed by those with more than one manifestation (mean, 23.8 days) and those with LA (mean, 23.6 days) (Table S4).
3.5. Treatment
Among the 315 enrolled LB cases, most were attended by a primary care physician (n = 251 [79.7%]), by a general practitioner (n = 58 [18.4%]), or via telephone consultations with a healthcare provider (n = 40 [12.7%]) when seeking care. Among the other healthcare providers seen were specialists (undefined) (n = 10), rheumatologists (n = 5), dermatologists (n = 4), and neurologists (n = 3) (Table S5). Four cases (1.3%) of 315 enrolled cases were hospitalised (one EM case and three disseminated cases [two with LA and one with LNB]): two cases for one night, and one case each for two nights and three nights.
Of the 315 enrolled cases, 306 (97.1%) received an antibiotic (three patients refused antibiotics, and six did not receive antibiotic therapy, with no explanation given by the site). The most common types of prescriptions were doxycycline (n = 123 [40.2%]), phenoxymethylpenicillin (n = 86 [28.1%]), and azithromycin (n = 79 [25.8%]). Antibiotic use varied significantly by country, although every country prescribed doxycycline, and it was the most prescribed type of antibiotic in the Czech Republic (57.6%), Germany (95.0%), Poland (88.9%), and Slovenia (47.6%) (Figure 5). In Slovakia, azithromycin was the type of antibiotic most commonly prescribed (64.4%), and in Sweden, phenoxymethylpenicillin was the most common (77.4%). Prescribing patterns for EM cases and disseminated manifestations were similar for all countries, except for Sweden. In Sweden, phenoxymethylpenicillin was most prescribed for EM disease (82.5%), but doxycycline was most prescribed for disseminated disease (66.7%).
Seventeen cases (5.4%) that were prescribed an antibiotic received more than one antibiotic (Slovakia, n = 13; Sweden, n = 2; Czech Republic, n = 1; Poland, n = 1). The most common first-line antibiotic was azithromycin (n = 7), and doxycycline was the most frequently used second-line antibiotic (n = 9). The most frequent combination was azithromycin and doxycycline (n = 6, of whom two received the doxycycline first). The duration of antibiotic use varied by country and by EM or disseminated disease presentation (Table 2). Poland had the longest duration of antibiotic treatment (median, 23.5 days: EM, 22 days; disseminated, 30 days), whereas Slovakia had the shortest (median, 9 days: EM, 9 days; disseminated, 10 days) (Table 2).
4. Discussion
The BOLD study is the first prospective epidemiological study for medically attended LB in multiple European countries, evaluating the signs and symptoms and manifestations of LB using standardised case definitions. Overall, over 75% of cases in BOLD had an EM manifestation; when Slovakia is excluded, this increased to 93.7% (584/623). LA was the most common disseminated manifestation, occurring in 19.3% (154/796) of cases (or 3.5% [22/623] excluding Slovakia), whereas LNB (n = 5) and LC (n = 3) case numbers were both very low. The distribution of manifestations in Slovakia was different from that in the other five countries, with LA comprising 76% of total cases. Most patients in the study received at least one course of antibiotic, varying substantially between countries but generally aligned with respective national guidelines.
With the exception of Slovakia, the distribution of manifestations in the BOLD data is similar to that seen in Brestrich et al.’s meta-analysis [18], which combined data from eight studies in France, the Netherlands, Germany, and Slovenia to give the following proportions: EM = 96.9%, LA = 1.3%, LNB = 1.7%, and Other = 0.1%. BOLD (non-Slovakian) data showed a higher proportion of cases without established LB clinical manifestations (“other” manifestations) (3.2%; range, 0% [Poland, Sweden]–15.9% [Germany]), likely due to the study allowing the inclusion of cases with a non-specific symptom presentation that other studies might have excluded. BOLD data also showed a higher proportion of LA cases (3.5%; range, 0% [Slovenia]–17.5% [Germany]) than the 1.3% reported by Brestrich et al. This may have been because final decisions on manifestation classification were made by primary site investigators, and subjects with more generalised systemic symptoms could be inconsistently allocated to either LA or to “other” manifestations. Finally, our LNB data was similar to countries with comprehensive LB surveillance systems, where approximately 2–4% of surveillance-reported LB cases are LNB [20,22,23]. Because the European Centre for Disease Prevention and Control (ECDC) began LNB surveillance in 2018, data on the proportion of LNB cases in Europe have been of good quality.
An unusually high proportion of LA cases were reported in Slovakia, where 76% of cases had LA compared with an average of 3.5% in the other BOLD countries. Although Slovakian LA cases presented with the traditional musculoskeletal symptoms, a large number also presented with general or nervous system symptoms. Additionally, only a few Slovakian LA cases reported an EM rash compared with 50% of the LA cases outside Slovakia. Multiple factors could have played a role in the unusual presentation of LB in Slovakia. There could be differences in the predominant subspecies of Borrelia burgdorferi s.l. or a more complex co-infection occurring, or the different presentation may reflect differences in healthcare-seeking behaviour, diagnostic practices, medical adherence, and site-specific clinical focus among different populations. The COVID-19 pandemic may have delayed EM diagnoses, leading to more patients presenting with a disseminated manifestation (including LA). Additionally, the two BOLD study sites in Slovakia were situated in very rural areas, with a local population who may be less likely to attend their primary physician for a skin rash. BOLD is not the first dataset to report a high proportion of LA cases among identified LB cases; a previous Slovakian study (1999–2000) reported 25% of cases were LA [24], and Slovakian public health surveillance data in 2021–2022 reported 8.2% to 17.0% of cases as LA [25,26]. At this time, there is no clear explanation for the higher rate of LA cases reported in Slovakia in this study, and B. burgdorferi s.l. isolates from LA cases were not available. It remains possible that there could have been differential classification of disseminated cases by manifestation between countries despite standardised case definitions. With the unusual presentation of LB observed in Slovakia, the laboratory diagnostic practices underpinning the diagnosis are of importance. The BOLD case definition required standard of care laboratory testing for disseminated cases, with Slovakia using a higher proportion of one-tier testing than other countries. The BOLD study also undertook standardised study laboratory testing using a modified two-tier test (MTTT) across all countries, where disseminated cases from the Czech Republic and Slovakia had a lower proportion of positive MTTTs. Laboratory testing in BOLD will be explored more fully in a separate manuscript.
The proportion of subjects presenting with an annular rash in this study was higher than the proportion in the literature [27,28]. This likely reflects a limitation of the data collection methods in BOLD, with no validation performed on these reports to ensure annular rashes were truly ring-shaped. Decisions on signs and symptom reporting were made by local clinical staff, and clinical judgement was accepted. Clinicians may have preferentially considered annular rashes as diagnostic of EM, while homogeneous rashes may have been less frequently recognised or classified as such. The large number of tick bites reported in some subjects’ medical histories was also unexpected; the maximum reported was 999. Data entry was capped at the value 999, and other high values were entered (e.g., 800, 600), so the large values are plausible. All but one of the values above 100 were reported by the Swedish cases, indicating that the Swedish study site was situated in an area with frequent tick exposure.
Almost all patients in the study received at least one course of an antibiotic. The types of antibiotics prescribed generally aligned with respective national guidelines (Appendix B), with minor variations that may be due to physician decisions based on patients’ medical history and needs. The variation in the type of antibiotic used by each country shows that there are multiple antibiotics still effective against LB, and only 17/306 (6%) cases required >1 antibiotic. Most of the study sites had mean and median antibiotic treatment times that were within their country recommendations and were based on prescribing guidelines (e.g., azithromycin has a shorter prescription length than most other antibiotics recommended for LB). For EM cases, the mean and median treatment times were slightly longer than their respective country guidelines for the Czech Republic, Germany, Poland, and Sweden. However, some antibiotic prescriptions require doses more than once per day, and if the first dose was given late in the day, a 14-day course could have been spread across 15 days. Some patients received a very high number of days of antibiotics to treat their LB, which can come with adverse effects, such as antibiotic resistance, microbiome disruption, and Clostridioides difficile infection [29,30]. The three longest courses of antibiotics were 48, 53, and 93 days. All three were disseminated cases, two qualified for a classification of PTLDS, and the third reported symptoms of disease lasting 16 months. The persistent symptoms and PTLDS cases will be described in a separate manuscript. An effective Lyme vaccine could have an important impact in reducing this antibiotic exposure.
This study has limitations. The results reported here for sites selected among high LB incidence regions in Europe may not be generalisable to other locations. Generalised conclusions were also limited by the uneven contribution of cases across countries, limiting cross-national comparability. Clinicians at the BOLD sites may be more experienced at identifying and diagnosing LB, potentially identifying more unusual cases with higher accuracy than clinicians would elsewhere. Similarly, antibiotic prescribing practices for the treatment of LB cases in the BOLD sites may not be representative of nationwide prescribing practices in each country. The clinical manifestations of LB may vary geographically based on the local prevalence of different Borrelia genospecies. Diagnostic and treatment practices vary across countries, which may also influence how and when manifestations are reported. Laboratory confirmation for the case definition was based on standard-of-care testing, which varied between sites and countries. There was potential for misdiagnosis, especially of EM cases where a laboratory confirmation was not required. In particular, the high proportion of annular rash presentations compared with prior literature suggests some misclassification. The presentation of LB cases to healthcare clinics in 2021 may have been affected, and healthcare-seeking behaviour may have been delayed as a result of the coronavirus disease (COVID-19) pandemic in 2020. Not all LB cases were willing to enrol in the study, or presented during a period when enrolment was no longer open, so signs and symptom descriptions and medical history are available only for the enrolled subset, which was slightly older, more likely to be female, and more likely to have disseminated disease. This may have affected the signs and symptoms reported in the dataset (with potentially more systemic and fewer localised cases in older age groups) and may have led to more use of antibiotics for disseminated disease. All analyses were descriptive, which limits the strength of inferences. There was an uneven contribution of cases by country, limiting the possibility of cross-country comparisons.
5. Conclusions
These findings show that the frequency of LB manifestations varies substantially between countries, with the distribution differing markedly in Slovakia. This study also improves understanding of treatment patterns across Europe and highlights the need for prevention measures, such as vaccination. To continue supporting clinical trials and public health needs, additional studies are needed to further characterise LB clinical manifestations across Europe and to understand drivers for between-country variation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lindgren E. Jaenson T.G.T. Lyme Borreliosis in Europe: Influences of Climate and Climate Change, Epidemiology, Ecology and Adaptation Measures World Health Organization Geneva, Switzerland 2006
- 2Steere A.C. Strle F. Wormser G.P. Hu L.T. Branda J.A. Hovius J.W. Li X. Mead P.S. Lyme borreliosis Nat. Rev. Dis. Primers 2016216090 Erratum in Nat. Rev. Dis. Primers 2017, 3, 17062. https://doi.org/10.1038/nrdp.2017.6210.1038/nrdp.2016.9027976670 PMC 5539539 · doi ↗ · pubmed ↗
- 3Sykes R.A. Makiello P. An estimate of Lyme borreliosis incidence in Western Europe J. Public Health 201739748110.1093/pubmed/fdw 01726966194 · doi ↗ · pubmed ↗
- 4Khanna S. Goebel L.J. Atypical Lyme disease rash: A case report Cureus 202416 e 5477910.7759/cureus.5477938529463 PMC 10961653 · doi ↗ · pubmed ↗
- 5National Institute of Allergy and Infectious Diseases Lyme Disease Antibiotic Treatment Research National Institute of Allergy and Infectious Diseases Rockville, MD, USA 2018 Available online: https://www.niaid.nih.gov/diseases-conditions/lyme-disease-antibiotic-treatment-research(accessed on 4 December 2025)
- 6Udziela S. Biesiada G. Osiewicz M. Michalak M. Stażyk K. Garlicki A. Czepiel J. Musculoskeletal manifestations of Lyme borreliosis—A review Arch. Med. Sci.20221872673110.5114/aoms.2020.9645835591816 PMC 9102650 · doi ↗ · pubmed ↗
- 7Marques A.R. Strle F. Wormser G.P. Comparison of Lyme disease in the United States and Europe Emerg. Infect. Dis.2021272017202410.3201/eid 2708.20476334286689 PMC 8314816 · doi ↗ · pubmed ↗
- 8Strle F. Wormser G.P. Mead P. Dhaduvai K. Longo M.V. Adenikinju O. Soman S. Tefera Y. Maraspin V. Lotrič-Furlan S. Gender disparity between cutaneous and non-cutaneous manifestations of Lyme borreliosis P Lo S ONE 20138 e 6411010.1371/journal.pone.006411023737968 PMC 3667797 · doi ↗ · pubmed ↗