Changes in Eating Behavior Among Children with Overweight or Obesity: Results of a Nutritional Intervention
Luana de Paula Ivnuk, Ádelin Olivia Lopes Joly Rodrigues, Isabela Cristina Santos Freire de Paula, Carlos Henrique Pereira, Marina Amaro da Rocha Matuguma, Gustavo Hermes Soares, Renata Iani Werneck, Juliana Schaia Rocha Orsi

TL;DR
A nutritional intervention helped children with overweight or obesity and their families change eating habits and increase awareness of food choices.
Contribution
The study highlights how family involvement in workshops can lead to positive shifts in children's eating behaviors.
Findings
Families reported reduced consumption of ultra-processed foods and reorganized eating routines.
Children showed increased critical awareness of food-related media and appreciation for body diversity.
Improved homemade school snacks indicated meaningful family engagement in the intervention.
Abstract
Background/Objectives: This study aimed to explore perceived changes in the eating behavior of children with overweight and obesity following a nutritional intervention, considering the perspectives of children and their families participating in a specialized health promotion program. Methods: This qualitative study included five children aged 7 to 12 years and four family members enrolled in the ProSaúde Kids Program in southern Brazil. The study comprised three stages: initial semi-structured interviews; nine interactive nutritional workshops conducted from July to November 2024 with active family participation; and final interviews after the intervention. Recordings were transcribed and analyzed in ATLAS.TI® using the collective subject discourse approach, guided by Bronfenbrenner’s Ecological Systems Theory. Results: The intervention was associated with reported changes in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
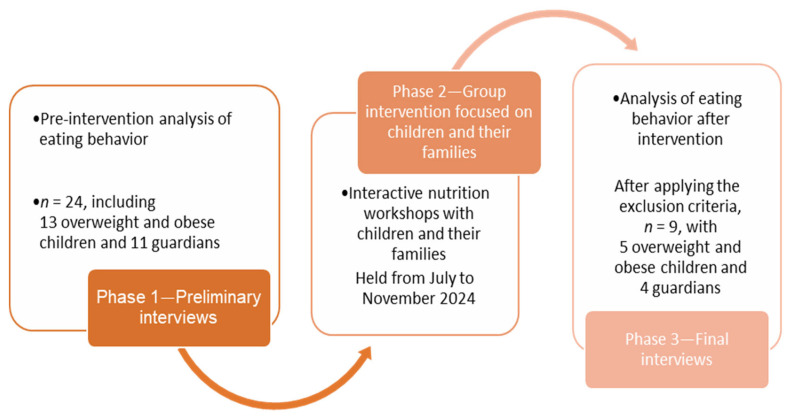 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsObesity, Physical Activity, Diet · Health, Education, and Aging · Health Education and Validation
1. Introduction
Childhood obesity is recognized as one of the major health burdens in Brazil, affecting 13% of children aged 0–5 years and 31.65% of those aged 6–10 years, according to BMI-for-age criteria [1]. This situation is particularly concerning due to its strong association with the early onset of metabolic syndrome—a cluster of interrelated metabolic disorders that include insulin resistance, dyslipidemia, hypertension, and central obesity—all of which significantly increase the risk of cardiovascular diseases, type 2 diabetes, and other chronic complications throughout life [2]. Among the factors considered globally essential for the prevention and control of this condition are physical activity and dietary habits [3,4].
Eating behavior is defined as a set of individual reactions to the environment and circumstances in which individuals are embedded [5]. Numerous factors influence eating behavior and may contribute to the increasing rates of overweight and obesity. These include external factors—such as social and family units, social and cultural values, media, food availability, and nutrition knowledge—as well as internal factors—such as psychological development and characteristics, body image, values and personal experiences, self-esteem, food preferences, and health [3,6,7].
Despite the complex interplay involved in eating behavior, educational strategies that focus solely on the individual sphere of the child remain common in nutrition. However, behavioral changes are challenging, especially when they involve eating habits established since childhood [8]. Such changes require not only knowledge but also emotional support, consistency in the environment, and continuous reinforcement [9]. In this context, interventions involving the family unit appear to be favorable for maintaining healthy eating behaviors [10]. Studies indicate that positive parental practices—such as having family meals and involving children in food preparation—are associated with healthier diets, while negative approaches—such as pressuring children to eat or using food as a reward—may lead to unhealthy eating patterns [11,12,13].
Therefore, nutritional actions must be in the family context to promote lasting behavioral changes [13]. Furthermore, successful changes in eating behavior involve multicomponent approaches that combine nutrition education, family support, motivational strategies, and modifications in the food environment [14]. Active participation of parents and caregivers, as well as coherence between what is taught and what is practiced in the family environment, are determining factors for the success of these strategies [9,13,15].
Based on this premise, the evaluation of eating behaviors among children with overweight or obesity is important not only to describe dietary patterns but also to explore how behavioral changes are perceived, negotiated, and incorporated into everyday family contexts. While the relevance of family-based interventions is well documented, qualitative evidence on how children and families experience these interventions across different ecological contexts remains relatively limited. Anchored in Bronfenbrenner’s Ecological Systems Theory [10], this study seeks to understand the perceived transformations associated with a nutritional intervention within a health program, examining changes in eating behavior and in autonomy, critical awareness, body perception, and lifestyle, from the perspectives of the children and their families.
2. Material and Methods
This study employed a qualitative approach and was conducted in three stages: 1. A preliminary semi-structured interview to assess eating behaviors before the intervention. 2. A group-based intervention involving children and their families. 3. A final semi-structured interview to evaluate eating behaviors after the intervention. The research stages are described in Figure 1.
This study was structured in accordance with the COREQ checklist [16], which aims to consolidate criteria for reporting qualitative research.
A pilot study was conducted to train the research team and test the applicability and clarity of the questionnaires, allowing for adjustments to procedures and ensuring higher data quality in the main study. Participants included children from the same target age group enrolled in the program, but with eutrophic BMI, and their families. During data collection, researchers recorded field notes, and after each session, they met to discuss challenges and propose adjustments. The revisions were incorporated into the final versions of the questionnaires and the operational protocol. Given the research team’s involvement in the design and implementation of the intervention, reflexive discussions were also undertaken throughout data collection and analysis to examine potential influences on interpretation.
2.1. Ethical Considerations
This research was approved by the Research Ethics Committee (CEP) of the Pontifical Catholic University of Paraná (PUCPR) under CAAE number 78754224.8.0000.0020 and opinion number 6.861.110. All investigations were conducted in accordance with the ethical principles of the Declaration of Helsinki of 1975, as revised in 2013.
All participating family members provided written informed consent for their own participation and for the participation of their children. Additionally, the children provided written assent prior to their inclusion in the study.
2.2. Context
The ProSaúde Kids program, linked to the Pontifical Catholic University of Paraná (PUCPR), was launched in August 2022 to promote healthy habits and improve the quality of life of children aged 3 to 12 years. The program is open to the public and has selection criteria, and in 2024 it had approximately 86 participants. Organized in age-based groups, sessions take place twice a week, combining physical education activities exploring various sports modalities with interventions from other fields—such as psychology and nutrition—scheduled on the same day as the sports classes. The model prioritizes a multidisciplinary and integrated approach focused on child development, promoting holistic care that considers physical, emotional, and social aspects. In addition, the program maintains affordable fees to encourage inclusivity.
2.3. Participants
The study population consisted of 51 children aged 3 to 12 years enrolled in the ProSaúde Kids program in 2023, in Curitiba, Brazil. Eligible participants were children aged 7 to 12 years who were classified as overweight or obese based on BMI-for-age, calculated using WHO AnthroPlus software (version 1.0.4; World Health Organization, Geneva, Switzerland), along with their families. The decision to include only children aged 7 years and older was due to the cognitive and verbal comprehension limitations of younger children (3–6 years), which could compromise their understanding and the validity of interview data.
Children were excluded if they: (i) missed any of the interviews (initial or final); (ii) withdrew from the ProSaúde Kids program before completion; or (iii) presented any neurodivergent condition that impaired comprehension at any stage of the study.
Parents or guardians were automatically included when the child met eligibility criteria and were excluded if they: (i) failed to attend both interviews; (ii) withdrew following their child’s dropout; or (iii) presented cognitive limitations or neurodivergence that impaired participation.
The initial sample included 13 children and their respective parents/guardians (n = 24). After applying exclusion criteria, the final sample comprised 5 children and their families (n = 9). One family (child + guardian) was excluded due to the absence of parents during the interview, and the remaining exclusions were due to early program withdrawal. Among the included children, four were female and one was male. Of the five guardians interviewed, two were fathers and two were mothers. No data on guardian age or socioeconomic status were collected, which limits contextual interpretation of the findings. None of the participants presented neurodivergent conditions that interfered with comprehension.
It is important to note that this study was embedded within the ProSaúde Kids program; therefore, participant recruitment and follow-up depended on children’s continuous enrollment in the program. Consequently, when families withdrew from the program, they were no longer available to continue in the research, directly contributing to the attrition rate and reduced final sample size.
This study did not seek to achieve theoretical saturation. Instead, all eligible children and families available and retained in the ProSaúde Kids program during the data collection period were invited to participate, and the final sample represents the total accessible population within this context. Although no a priori saturation criterion guided sample definition, data analysis indicated recurrence of themes across interviews, supporting analytical coherence within the study’s exploratory scope.
Despite the small sample, this size is consistent with the exploratory and in-depth nature of qualitative research, which prioritizes richness of data over numerical representativeness.
2.4. Research Phases
The planning and delivery of the interactive nutritional workshops, as well as the preparation of educational materials, were entirely carried out by the research team. The researchers also developed qualitative data collection instruments, including the interview guides. This full involvement allowed alignment between the study objectives, methodological strategies, and field implementation, consistent with qualitative research principles that recognize the researcher’s active role in knowledge production.
2.4.1. Phases 1 and 3—Preliminary and Final Semi-Structured Interviews
Two sets of interviews were conducted with the children and their families: one before the nutritional intervention and another after its completion. The initial interview aimed to characterize pre-intervention eating behaviors, family eating routines, and consumption patterns. The final interview, conducted within two weeks after the last workshop, sought to assess participants’ perceptions and learnings from the intervention, exploring possible behavioral and attitudinal changes and how the workshop content had been integrated into daily life. The final interview revisited the same thematic axes as the initial one, adding questions to identify what had or had not been learned throughout the process.
Both interviews followed semi-structured guides developed based on Urie Bronfenbrenner’s Ecological Systems Theory of Human Development [5,6,12], considering its multiple systems. The interviews, lasting approximately 20 min each, included open-ended questions on general information, eating behaviors, and family food-related aspects.
Each interview was conducted using a printed guide and a notebook for audio recording. Before beginning, participants signed the informed consent form authorizing the use of audio and images for research purposes and the child assent form.
Interviews were conducted by a team of researchers who were not involved in the intervention phase and had no prior relationship with the ProSaúde Kids program to reduce bias and enhance neutrality. Two trained female health professionals from the field of dentistry conducted the interviews, ensuring standardized procedures and consistent data collection.
2.4.2. Phase 2—Group Intervention for Children and Families
The intervention consisted of nine interactive nutritional workshops held between July and November 2024, on pre-scheduled days, focusing on health literacy [17] and using participatory methodologies [18,19] with family participation. The sessions took place in classrooms at PUCPR.
Each session was facilitated by three health professionals—two female and one male. They led interactive and educational activities promoting health and improving family eating behavior. Alignment among facilitators was maintained through asynchronous meetings to standardize practices and ensure methodological coherence. Health students from an interprofessional program also participated as observers, assisting with logistics and supporting children during activities.
The workshop themes were selected based on the Brazilian Dietary Guidelines [20] and the complementary literature, particularly those focusing on behavioral nutrition [5,21]. This approach allowed a broader understanding of eating beyond nutritional aspects, incorporating habits, culture, and social context—core principles of the Brazilian Dietary Guidelines [20]. The topics covered were: (1) “What is Healthy Eating”; (2) “Hunger for What?”; (3) “Food Selectivity”; (4) “Time to Go Grocery Shopping”; (5) “Autonomy in Choices”; (6) “Sharing Moments and Meals”; (7) “My Body Image”; (8) “Difficulties in My Child’s Feeding/Eating”; (9) “Applying What I’ve Learned”.
2.5. Data Analysis
Interview data were analyzed using the collective subject discourse (CSD) methodology proposed by Lefèvre and Lefèvre [22], which reconstructs collective thought from individual discourse synthesis. The analytical process followed the methodological stages defined by the authors: reading the transcripts, identifying key expressions, formulating central ideas (CIs), and constructing the final collective discourses (CSDs). For example, individual excerpts expressing children’s involvement in food choices (key expressions) were synthesized into central ideas related to autonomy, which were then integrated into collective subject discourses representing shared meanings across participants.
Interviews were transcribed using TurboScribe^®^ (TurboScribe Inc., San Francisco, CA, USA) and organized in Microsoft^®^ Word 2010 (Microsoft Corp., Redmond, WA, USA). Key expression identification and CI organization were performed using ATLAS.TI^®^ (version 23.4.0; ATLAS.ti Scientific Software Development GmbH, Berlin, Germany). To enhance analytical rigor and trustworthiness, two researchers independently conducted the initial stages of analysis without access to each other’s interpretations. Subsequent joint meetings were held to compare findings, resolve discrepancies through consensus, and refine the central ideas and final CSDs. This process supported reflexivity and consistency in qualitative interpretation. Analytical discussions focused on thematic recurrence, internal consistency, and alignment with the study objectives, rather than on achieving theoretical saturation, given the predefined and context-bound nature of the sample. In this context, formal member checking was not undertaken. Instead, credibility was enhanced through researcher triangulation, including independent analysis, consensus meetings, peer debriefing, and reflexive discussions.
The analytical lens was Bronfenbrenner’s Ecological Systems Theory of Human Development, which posits that sustainable changes in eating and lifestyle behaviors occur through the individual’s continuous interaction with multiple environmental systems [23]. The theory identifies interconnected systems—such as family, school, parents’ work, and the broader sociocultural context—that influence human development [10,23]. The definitions and descriptions of each system proposed by Bronfenbrenner’s theory are presented in Table 1.
3. Results
The central ideas (CIs) identified in the initial and final stages addressing the same topics were placed side by side in comparative tables to facilitate comparison of perceptions and reported behaviors across study stages. Table 2 presents the discourses of parents/guardians and children related to the microsystem, while Table 3 presents the collective subject discourses related to the mesosystem, focusing on interactions between family, school, and health professionals before and after the intervention.
At the microsystem level, caregivers and children described changes in family routines after the intervention. Children reported greater involvement in food-related decisions, particularly during grocery shopping. Increased openness to trying new foods, such as fruits and vegetables, was also described, and workshop content was shared with other family members.
Participants reported a gradual reorganization of meals, including perceived reductions in the consumption of ultra-processed foods and greater attention to dietary balance and satiety. Although not all changes were fully consolidated, families described progress in awareness and daily practices related to eating habits.
Although the nutritional intervention did not take place directly within the school environment, the mesosystem (particularly at the interface between school and family) remained relevant to children’s eating habits. The school maintained a structured eating routine, with fixed schedules and predefined menus, serving as the setting for many main meals, such as lunch and snacks. However, limitations imposed by this environment, such as the inability to change the school menu, remained unchanged in the post-intervention period. Despite this, changes were reported in the content of snacks brought from home, which were described as healthier, alongside greater family involvement in food-related practices.
Furthermore, the interaction among different environments—especially between school, caregivers, and other health professionals—continued to be described as influencing children’s eating behavior. Additionally, even without a formal school-based intervention, existing initiatives such as cooking classes and nutrition education activities were remembered positively by some families, serving as stimuli for children’s food autonomy. These school experiences, when combined with family involvement, were associated with children’s interest in healthier foods and cooking. Thus, even though the school’s structure itself was not altered by the intervention, its connection with the family context remained present in participants’ narratives about eating practices.
After the intervention, children and their families began to share the knowledge acquired about healthy eating with other family members and in external settings. Children reported teaching grandparents and peers about healthy eating habits, while parents mentioned applying the guidance they received within their social and professional circles.
Table 4 presents the collective subject discourses related to the exosystem, focusing on indirect influences on children’s eating behavior, such as media exposure and family work routines, before and after the intervention.
Before the intervention, participants reported frequent exposure to food-related content disseminated through media, especially the internet and television. Despite this exposure to recipes and dietary tips, participants described limited changes in the eating habits of children and their families. Information was described as being consumed without clear criteria for accuracy or practical application. After the intervention, participants reported changes in how media content was interpreted—particularly among children, who described questioning the reliability of information and expressing a more critical view.
Prior to the intervention, caregivers described demanding routines and work schedules as barriers to adopting healthier eating habits. Meal preparation was often reported as compromised, with frequent consumption of ready-made or ultra-processed foods chosen for convenience. After the intervention, although time constraints and routine challenges persisted, participants reported greater organization of family meals, including more structured planning and greater attention to food choices. Even though structural barriers remained, changes in daily meal organization and planning were described.
Table 5 presents the collective subject discourses related to the macrosystem, addressing broader sociocultural values, beliefs, and norms associated with food, body image, and childhood obesity before and after the intervention.
The results derived from the analyzed statements describe changes in children’s perceptions of food and body image after the educational intervention. Prior to the intervention, participants described concerns related to controlling children’s weight, often in the context of aesthetic standards and fears of obesity, alongside restriction of foods perceived as “fattening.” Food was also described as being used as an expression of affection or as a reward, with occasional allowances for less healthy foods in specific situations. In addition, children expressed dissatisfaction with certain body characteristics, which participants associated with external comments and beauty standards.
After the intervention, children described greater acceptance of body diversity and expressed more positive perceptions of their own bodies. Parents and caregivers reported reflecting on their feeding practices, seeking to balance the provision of healthy foods with moments of enjoyment—particularly on weekends—although some association between food and reward was still reported.
Table 6 presents the collective subject discourses related to the chronosystem, addressing changes and transitions in eating behavior over time and across different life stages before and after the intervention.
The collective discourses constructed from the chronosystem describe changes in eating practices over time. Prior to the intervention, participants reported a history of changes associated with life events, such as the birth of siblings or dieting phases among family members. Many parents mentioned that as their children grew older, adherence to healthy eating habits was described as declining, with frequent replacement of main meals by snacks or ready-made foods.
After the intervention, participants described greater awareness of how life stages influence eating habits, alongside reports of attempts to maintain a more balanced diet despite individual preferences within the family. The transition to adolescence was described as a challenge due to the pursuit of food autonomy, and participants reported reflections on the importance of healthy food choices and acceptance of bodily changes over time.
4. Discussion
Given the growing challenge that childhood overweight and obesity represent, understanding how nutritional interventions can promote changes in children’s eating behavior, especially when involving the family nucleus, becomes essential [24]. Within this context, the present exploratory study sought to examine how children and their families perceived changes associated with participation in a family-centered nutritional intervention. The study offers a contextual and descriptive perspective on eating practices and the environmental and relational factors that influence them. Through participants’ narratives, it was possible to observe perceived changes in eating behaviors and parental engagement in family routines. The following sections discuss the main findings, their implications for child health promotion, and potential directions for improving future educational strategies.
Regarding the family environment, perceived shifts in behaviors were described within the microsystem, as proposed by Bronfenbrenner’s ecological theory [10], including the reproduction of practices learned at home and greater parental awareness of their role in shaping children’s diets. The scientific literature supports the importance of the family as the central nucleus for the formation and dissemination of eating habits. Studies indicate that family members are the primary behavioral models for children and exert a strong influence on dietary habits from early childhood [25]. Moreover, healthy family practices can generate a multiplier effect, benefiting not only children but also the surrounding community [26]. In this sense, the findings align with the existing literature and point to the potential relevance of strategies that go beyond a child-centered focus, involve the family, and promote collaborative action among different professionals [13,27].
It was also observed that busy routines, long working hours, and multiple responsibilities make it difficult for parents to organize meals and offer healthier foods, often leading to quick and less nutritious choices. Eating behavior is influenced by various environmental factors, including family, socioeconomic, and cultural conditions, with the family being one of the main determinants in establishing healthy eating habits [27]. The literature reinforces that interventions involving families are more effective in promoting sustainable changes in children’s eating behavior, as they operate within the environments where these choices are constructed and reproduced [13,26,27].
Within the mesosystem, families reported perceived changes in school snacks, which became healthier, indicating possible greater family participation and responsibility in food-related decisions. Evidence shows that the school setting, including educational activities on healthy eating, can positively influence children’s nutritional status, provided that these initiatives are well implemented [28]. The inclusion of cooking workshops in schools—mentioned by participants—has been recognized as a low-cost, easy-to-implement, and highly applicable educational strategy in school contexts [29,30]. Moreover, such activities can be integrated into multiple curricular subjects, promoting learning in an engaging and practical way [29]. These effects add to positive parental practices, such as involving children in meal preparation and providing healthy options, which have a direct impact on their eating habits [12,13]. The present findings do not demonstrate such effects but suggest how families interpreted and integrated school-related food practices.
However, in Brazil, the presence of school canteens offering ultra-processed foods and the influence of food marketing around schools can undermine these efforts, highlighting the need for stronger regulation of the school food environment [31]. Although some legal initiatives exist, such as state and municipal regulations restricting the sale of ultra-processed foods in schools, e.g., Paraná State Law No. 14.855/2005 [32], in practice, these measures are often insufficient. Schools may comply with current regulations, but surrounding snack bars and candy stands still offer easy access to unhealthy products, since the legislation does not apply to them [33,34]. This gap compromises the progress achieved within schools and demonstrates the need for broader public policies that also encompass the school surroundings as part of children’s food environments.
Another finding from the collective subject discourses (CSDs) concerns the influence of media on children’s eating habits. Media content—such as advertisements and online videos—can shape food preferences, often promoting the consumption of ultra-processed and low-nutrient foods [35]. Our findings portray that media, particularly television and the internet, are frequent sources of information for both children and parents. Similarly, regarding media influence, children described a more critical understanding of food-related content after the intervention. These perceptions suggest increased awareness, reinforcing the potential value of incorporating media literacy into nutrition education strategies, as supported by previous studies [36].
Issues related to body image and emotional eating also emerged from the families’ narratives. The findings suggest that the intervention encouraged children to reflect more critically on their body image, showing signs of greater awareness and less influence from external beauty standards. This highlights the positive potential of integrated, developmentally sensitive approaches. Consistent with our findings, studies indicate that interventions addressing body image and eating behaviors can effectively promote healthy habits and build positive self-esteem among children and adolescents [25]. Similarly, educational actions that encourage critical thinking about media-driven beauty standards can reduce social comparison and body dissatisfaction, promoting greater autonomy and healthier eating behaviors [37].
The discourses also reflect how the time and significant life events affect the formation of children’s eating habits. Transitions such as the birth of siblings, changes in routine, or entry into adolescence were linked to altered eating behaviors, often associated with episodes of anxiety and emotional eating—an association well documented in the literature [38]. A systematic review and meta-analysis found that psychological stress in children and adolescents is associated with more unhealthy dietary patterns, including higher consumption of fatty and sugary foods and lower intake of fruits and vegetables [39]. Another meta-analysis identified a significant association between depressive symptoms and disordered eating behaviors in youth, showing that depression is positively related to emotional eating, suggesting that depressive symptoms may lead to harmful eating patterns triggered by negative emotions [40]. These findings emphasize the importance of interventions addressing not only nutritional aspects but also the emotional and psychosocial factors that influence eating behavior. Family-based strategies that promote emotional regulation may be more effective in fostering healthy eating habits and preventing long-term disordered eating patterns.
Some limitations must be acknowledged in this article. As a short-term study, it was not possible to evaluate whether the reported changes were maintained over time. The analysis also relied on self-reported data, which may be subject to bias, particularly social desirability bias [41], where participants may have sought to please researchers by giving more positive responses about the program. Although this tendency was mitigated through the use of external interviewers who were not involved in the intervention, it cannot be completely ruled out. In addition, the absence of objective nutritional indicators and the lack of socioeconomic characterization of participating families restrict the scope of interpretation and limit a more contextualized understanding of the findings.
The small sample size also limits the transferability of the findings, as results may not fully represent the diversity of experiences among children with overweight and obesity. This limitation is partly related to the context in which the study was conducted, as the research was embedded within an ongoing health promotion program. Participation in the study depended on children’s continued enrollment in the ProSaúde Kids program; therefore, withdrawal from the program necessarily resulted in discontinuation from the research, contributing to the high attrition rate and reduced final sample size. In addition, limited engagement from some children during interviews represented another challenge, as responses were occasionally brief or underdeveloped, possibly due to shyness, comprehension difficulties, or discomfort with the interview setting. This limitation may have affected the depth and diversity of children’s perspectives captured in the data.
Taken together, these limitations indicate that the findings should be interpreted as context-specific and exploratory rather than generalizable. Therefore, future interventions should employ mixed-method designs with more robust quantitative and qualitative components and include medium- and long-term follow-up strategies. Longitudinal studies, for instance, could assess the maintenance of acquired habits and provide insight into the long-term effects of educational interventions. Moreover, incorporating systematic evaluation mechanisms for the school food environment and the role of media in shaping eating behavior could broaden the scope and impact of such programs.
Despite these limitations, the results of this exploratory study suggest the relevance of educational spaces that integrate family and community, highlighting the potential role of the family environment in building healthy habits. By encouraging reflection and mindful eating practices, the intervention appeared to offer opportunities to promote positive changes in children’s eating behavior and their relationship with body image. Furthermore, the use of participatory methodologies can be seen as a valuable approach to promote active listening and the involvement of children and families in the educational process, which can increase engagement, autonomy, and the meaning of the proposed changes. In this sense, the study points to the potential value of strategies that encourage family participation and shared responsibility in food-related decisions, as well as the relevance of integrated actions between health, education, and other sectors that shape children’s social environments. Overall, the contribution of this study is primarily contextual and descriptive, offering exploratory insights that may inform future research and practice, without implying causal effects or generalizability.
5. Conclusions
Our findings suggest that this exploratory intervention was associated with perceived changes in the eating behavior of children and their families, including increased reflection on food choices and everyday practices. Children reported greater critical awareness of body image and food-related media content, indicating possible reductions in the influence of external stereotypes and media standards, and suggesting that the educational experience may have extended beyond nutritional aspects alone.
While these findings should be interpreted in light of the study’s qualitative design, small sample size, and reliance on self-reported data, the results point to the potential relevance of strategies that acknowledge the complexity of social and cultural contexts involved in shaping eating habits. In this sense, the study contributes exploratory insights that may inform the development of family-centered and context-sensitive approaches to health promotion in childhood, without implying generalizable or causal effects.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Departamento de Atenção Básica, Ministério da Saúde Protocolos do Sistema de Vigilância Alimentar e Nutricional (SISVAN): Relatórios de Consumo Alimentar Departamento de Atenção Básica, Ministério da Saúde Brasília, Brazil 2022 Available online: https://sisaps.saude.gov.br/sisvan/(accessed on 19 February 2026)
- 2De Carvalho M.H.C. I Diretriz Brasileira de Diagnóstico e Tratamento Da Síndrome Metabólica Arq. Bras. Cardiol.20058432810.1590/S 0066-782X 200500070000116095065 · doi ↗ · pubmed ↗
- 3Associação Brasileira Para o Estudo da Obesidade e da Síndrome Metabólica (ABESO) Diretrizes Brasileiras de Obesidade 4th ed.ABESOSão Paulo, Brazil 2016 Available online: https://abeso.org.br/wp-content/uploads/2019/12/Diretrizes-Download-Diretrizes-Brasileiras-de-Obesidade-2016.pdf(accessed on 19 February 2026)
- 4Lobstein T. Leach R.J. Powis J. Brinsden H. Gray M. World Obesity Atlas 2023 World Obesity Federation London, UK 2023 Available online: https://www.worldobesity.org/resources/resource-library/world-obesity-atlas-2023(accessed on 19 February 2026)
- 5Alvarenga M. Figueiredo M. Timerman F. Antonaccio C. Nutrição Comportamental 2nd ed.Manole São Paulo, Brazil 2019
- 6Flynn M.A.T. Mc Neil D.A. Maloff B. Mutasingwa D. Wu M. Ford C. Tough S.C. Reducing Obesity and Related Chronic Disease Risk in Children and Youth: A Synthesis of Evidence with “best Practice” Recommendations Obes. Rev.2006776610.1111/j.1467-789X.2006.00242.x 16371076 · doi ↗ · pubmed ↗
- 7Rivera J.Á. De Cossío T.G. Pedraza L.S. Aburto T.C. Sánchez T.G. Martorell R. Childhood and Adolescent Overweight and Obesity in Latin America: A Systematic Review Lancet Diabetes Endocrinol.2014232133210.1016/S 2213-8587(13)70173-624703050 · doi ↗ · pubmed ↗
- 8Birch L.L. Ventura A.K. Preventing Childhood Obesity: What Works?Int. J. Obes.200933 S 74S 8110.1038/ijo.2009.2219363514 · doi ↗ · pubmed ↗