Attitudes and participation in fall risk management: A tripartite, multicenter cross-sectional study of physicians, nurses, and patients
Qianqian Mou, Min You, Lin Tao, Junying Li, Yan Jiang, Xiaolian Jiang

TL;DR
This study examines how doctors, nurses, and patients approach fall risk management, finding that nurses lead efforts while doctors' involvement is limited and influenced by nurse invitations.
Contribution
The study identifies nurse-initiated collaboration as a key factor in physician participation in fall risk management.
Findings
Physicians and nurses had similar attitudes but physicians participated more in fall risk management.
Physician engagement was influenced by education, gender, and nurse invitations.
Nurses primarily lead fall management, with patient noncompliance and disease complexity as major challenges.
Abstract
This study aims to explore the attitudes and involvement of physicians, nurses and patients in fall risk management, focusing on the factors influencing physicians’ participation. This study utilized a convenience sampling, 4,272 participants (580 physicians, 2,775 nurses, 917 patients) from 19 Chinese provinces were enrolled via Questionnaire Star from 11 April to 31 May, 2024. The survey included general information, tripartite fall management perspectives, and 27-item medical staff/patient questionnaires. Medical staff evaluated fall risk through assessment, prevention, and management; patients reported adherence and staff participation. Physicians and nurses showed comparable attitude scores (55.02 ± 8.124 vs 54.58 ± 9.096, P = 0.227), but physicians had higher participation (51.47 ± 9.703 vs 42.77 ± 12.052, P < 0.001). Key factors influencing physicians’ engagement included…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
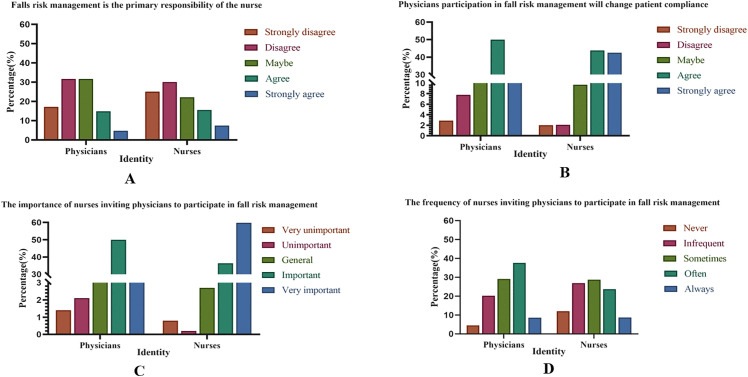 Fig 1
Fig 1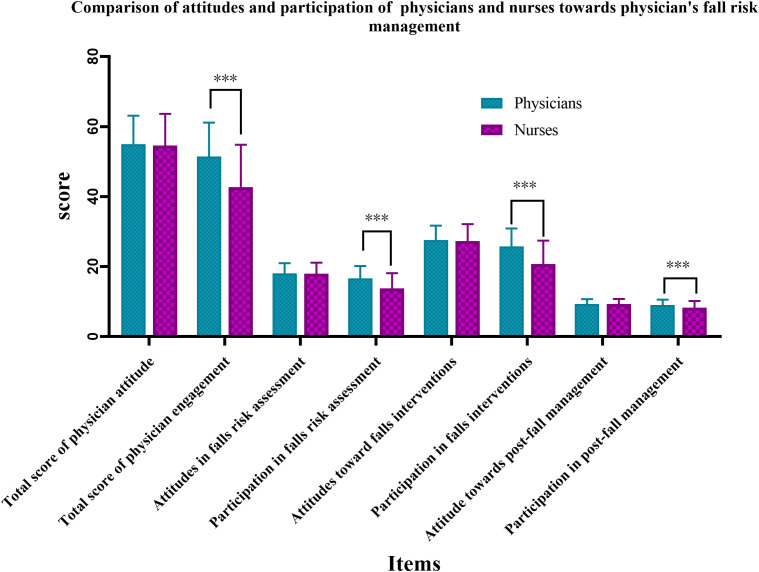 Fig 2
Fig 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBalance, Gait, and Falls Prevention · Frailty in Older Adults · Patient Safety and Medication Errors
1. Introduction
Patient safety is a critical concern in healthcare, with patient falls representing a serious threat to both physical and mental health, as well as quality of life, while imposing a substantial burden on public health systems [1,2]. According to the Global Report on Falls Prevention in Older Adults, falls are the leading cause of pain, disability, functional limitations, and even mortality among older adults [3]. The World Health Organization (WHO) reports that annually, 28% to 35% of individuals aged 65 and older experience at least one fall, with the prevalence increasing to 32% to 42% among those aged 70 and above [4]. Globally, approximately 37.3 million people require medical attention due to fall-related injuries each year, with over 680,000 fatalities, predominantly in low and middle-income countries [5]. In China, the age-standardized incidence rate (ASIR) and age-standardized mortality rate (ASMR) for falls among older adults have been rising, with the ASIR increasing from 1972.47/100,000 in 1990 to 3404.53/100,000 in 2019, reflecting an average annual growth rate of 1.929%. Similarly, the ASMR rose from 20.17/100,000 to 30.67/100,000, with an average annual growth rate of 1.535% [6].
Falls not only inflict physical and psychological harm on patients but also contribute to extended hospital stays and potential medical disputes [7,8]. The financial burden of treating fall-related injuries escalates with aging populations and rising medical expenses [9]. In 2015, the medical expenses associated with falls among older adults amounted to approximately 6,669 per hospitalization in Australia [2]. In China, the cost per fall injury ranged from 3,812/ person [10]. In response, the WHO has issued guidelines emphasizing the need for healthcare organizations to implement patient safety management systems to prevent adverse events such as falls. The Joint Commission International (JCI) includes fall incidence as a criterion for accreditation [11]. Moreover, China has incorporated fall prevention into its patient safety objectives, as outlined in the “Healthy China 2030” Plan, highlighting the importance of fall prevention interventions for the elderly as a key component of health promotion [12]. The increasing demand for high-quality healthcare services has underscored the importance of fall risk management as a crucial aspect of quality improvement and patient safety in healthcare organizations.
Despite efforts to enhance fall risk management, progress has been hindered by medical staff’ insufficient knowledge, beliefs, and behaviors [13], as well as poor patient compliance [14,15]. As evidenced by nurse-led fall prevention protocols, the primary responsibility for managing fall risk typically lies with nursing staff, with physicians providing input primarily in complex cases [16–18]. This lack of collaboration, coupled with infrequent invitations from nurses for physicians to participate, has resulted in underutilization of physicians’ roles. A study published in The Lancet [19]demonstrated that fall risk management involving physicians, nurses, and patients reduced fall incidence and injury rates compared to conventional management, with fall rates of 7.80/1,000 in the experimental group versus 13.78/1,000 in the control group, and injury rates of 2.63/1,000 versus 4.75/1,000, respectively. A hospital in China implemented a “nurse-led, multi-departmental collaboration model” to prevent falls, resulting in a decrease in fall incidence from 0.07/1,000 to 0.04/1,000 and a reduction in injury rates from 11.54% to 5.0% within one year [20]. These findings highlight the critical role of both medical staff and patient self-management in fall prevention, emphasizing the need to enhance medical staff’ participation and improve patient adherence.
The collaborative role of medical staff and patients in managing fall risk has garnered increasing attention. However, most existing studies focus on either medical staff or patients, with limited systematic analysis of their interactions. This study aims to fill this gap by using a questionnaire survey to explore the attitudes, behaviors, and influencing factors of medical staff and patients in fall risk management. The goal is to provide a scientific basis for developing more personalized, targeted, and effective fall risk management strategies.
2. Methods
2.1. Design and study population
This study employed a multicenter cross-sectional survey, selecting physicians, nurses, and patients from several provinces across the China using convenience sampling from April 11 2024 to May 31 2024. While this non‑probability method may limit the generalizability of the results, it was chosen for two primary reasons. First, the study is exploratory, aiming to preliminarily assess attitudes and behaviors toward fall risk management among physicians, nurses, and patients. Second, randomized probability sampling was not feasible within the clinical workflow and time constraints of the project. To enhance internal validity, strict inclusion and exclusion criteria were applied to ensure data quality and comparability within the sample.
Inclusion criteria for physicians and nurses included: (1) engagement in clinical work, including those in hospital management positions who also participate in frontline clinical work, (2) possession of a doctor’s qualification certificate or a doctor’s assistant qualification for physicians, and a nurse’s qualification for nurses. Exclusion criteria included those not currently in practice, such as individuals on long-term leave or retired. Inclusion criteria for patients were: (1) age ≥ 18 years, (2) possessed normal communication and literacy abilities, could fill in questionnaires, (3) gave informed consent for voluntary participation in the study. Exclusion criteria for patients included those with critical or deteriorating conditions.
2.2. Sample
The target sample size was determined in accordance with established best practices to ensure the robustness of the psychometric analysis [21]. A larger sample reduces measurement error, yields more stable factor loadings, and enhances the reproducibility and generalizability of the results. For scale development of this kind, a widely cited heuristic recommends including 5–10 respondents per questionnaire item [22]. Accordingly, the sample size for this study was calculated using the standard formula for survey research: , where ‘n’ represents the number of items [23]. Each version of the questionnaire (for physicians, nurses, and patients) contained 27 items. To account for potential invalid responses, the calculated sample was increased by 20% using the adjustment formula: . Based on this calculation, the theoretical sample size range for each group was 169–338 participants. To further ensure the stability and reliability of the findings, we deliberately recruited a sample size exceeding the upper bound of this range for each group.
2.3. Data collection
The research team collaborated with administrative offices at participating hospitals. Before distributing the questionnaires, the research team obtained approval from hospital presidents or nursing directors. Following this, department heads or head nurses were responsible for disseminating the questionnaires within their respective WeChat (version8.0.59, https://weixin.qq.com/) groups. Upon accessing the link, participants encountered an introductory page detailing the study purpose, confidentiality protocols, and electronic consent requirements. Only individuals confirming informed consent were directed to the main questionnaire. The distribution and collection of the questionnaires were managed by the Questionnaire Star (https://www.wjx.cn/), which ensured that each IP address could submit only one response. This measure was implemented to maintain data quality and prevent duplicate entries.
2.4. Measurements
The research team developed a questionnaire using a literature review and expert consultation method. This included socio-demographic questionnaire and the “questionnaire on attitude and participation in falls risk management from the perspective of physicians, nurses, and patients”. For physicians and nurses, the socio-demographic section collected data on gender, age, marriage, degree of education, hospital level, department of work, years of work experience, professional title, and administrative position. For patients, it was collected socio-demographic such as gender, age, marriage, degree of education, hospital level, department of medicine, occupational status, ways of living and medical payment.
2.5. Instrument reliability and validity
Initially, relevant literature was reviewed from both domestic and international databases to construct an initial pool of entries, guided by fall risk management guidelines and expert consensus. The questionnaires for physicians, nurses, and patients each consist of 27 items, comprising both a socio-demographic questionnaire and a fall risk management questionnaire. Subsequently, 11 experts from tertiary hospitals, with an average age of 44.82 ± 6.306 years (range: 35–58) and an average of 20.64 ± 7.827 years of work experience (range: 9–38), participated in two rounds of correspondence. The general characteristics of these experts are detailed in Table 1. Based on their feedback, entries with an importance rating of ≤3 points and a coefficient of variation >0.25 were removed, and necessary modifications and refinements were made. The authority coefficients Ca, Cs and Cr of the questionnaire were all 0.964, and the coefficients of variation for each entry were ≤0.25, indicating high authority and reliability. The Cronbach’s alpha coefficients for the physician, nurse, and patient dimensions were 0.976, 0.954, and 0.960, respectively, demonstrating good reliability and validity of the questionnaire.
Table 1: Demographic characteristics of the experts (n = 11).
2.6. Contents of the questionnaire
The questionnaire was designed to gather comprehensive information from physicians, nurses, and patients regarding fall risk management. The self-assessment component for physicians focused on three primary dimensions: fall risk assessment, fall prevention intervention, and post-fall management. Similarly, the nurse assessment dimension mirrored the structure of the physician section. This section comprised 12 items, each rated on a 5-point Likert scale. Ranging from “I do not agree completely” to “I agree completely”, importance was rated from “very unimportant” to “very important” and implementation from “never” to “always” with scores ranging from 1 to 5 points. The total possible score ranged from 12 to 60 (see Table 2), with higher scores indicating greater participation.
Table 2: The description of the questionnaire’s content and scoring.
For patients, it primarily assessed patients’ evaluations of physicians’ and nurses’ participation in fall risk management and their own adherence. This section included 8 items, with scores ranging from 8 to 40 (see Table 2), where higher scores indicated better evaluation and adherence.
The final number of items for the socio-demographic questionnaire combined with the fall risk management questionnaire in each version of the questionnaire (physician, nurse, patient) after the two rounds of expert review, confirming it remained at 27.
2.7. Ethical and research approvals
The clinical trial and biomedical ethics committee of West China Hospital of Sichuan University approved the study (No. 2024 [656]). All procedures strictly adhered to the Declaration of Helsinki and relevant regulatory guidelines. Electronic informed consent was obtained from all participating physicians, nurses, and patients following comprehensive explanation of study protocols. Their personal information was strictly protected.
2.8. Statistical analysis
Data were meticulously entered into Excel by two specialists from the research team, and statistical analyses were conducted using IBM SPSS software (version 26.0, https://www.ibm.com/). The analysis included:(1) Statistical description, where measurement data were expressed as M ± SD and count data as frequency and composition ratio (%). (2) Wilcoxon rank-sum test to compare self-assessed participation by physicians and nurse-assessed participation; paired t-test to evaluate differences in patient assessments of physicians and nurses. (3) Difference-Analysis, employing t-test or ANOVA to compare sample means between groups. (4) Multi-factorial analysis, variables demonstrating statistically significant results in the univariate analysis were subjected to collinearity diagnosis, and those with a variance inflation factor (VIF) <5 were subsequently included in the multivariate analysis. Using linear regression to explore differences in participation of physicians based on varying characteristics. considering a statistical significance level of P < 0.05.
3. Results
3.1. Description of the participants
The study encompassed participants from 19 provinces and cities in China. As a result, 4,272questionnaires were finally analyzed, including 580 from physicians, 2,775 from nurses, and 917 from patients. A description of the participants’ demographic and developmental characteristics is presented in Table 3.
Table 3: Demographic and developmental characteristics of the participants.
The majority of the medical staff respondents were female (3355, 89.57%). A comparable proportion of physicians (48.4%) and nurses (45.5%) were categorized as young and middle-aged. The majority of both groups were married-76.9% physicians and 71.5% nurses. In terms of education, 53.1% of physicians held a master’s degree or higher, while 77.1% of nurses had undergraduate degrees. The majority of the staff were employed in tertiary hospitals (94.0% physicians vs. 93.2% nurses respectively). A significant portion of physicians (29.5%) and nurses (26.5%) were specifically working in oncology wards. The most common range of work experience for both physicians and nurses were 11–20 years (27.6% vs 36.6%). Over a half of nurses (n = 1485, 53.5%) were junior level, while among physicians, 38.6% (n = 224) were at the middle level. A similar percentage of physicians and nurses were work position (63.3% resident physician vs 64.2 charge nurse). In both professional groups, the majority of staff did not hold any administrative positions.
In our patient cohort, represented age group was individuals over 60 (n = 385, 39.0%). The majority of these patients were married. In terms of education, 30.9% had completed only junior high school. An overwhelming 86.8% were treated in tertiary hospitals, with a notable concentration in oncology wards. Over half (n = 489, 53.5%) were unemployed. Nearly half, at 47.7%, lived with their spouse. The majority of patients relied on employee insurance to cover their medical costs. A significant proportion, 56.5% indicated they would follow their physicians’ advice.
Fig 1 revealed that nearly half of the physicians (44.8%) and nurses (55.0%) disagreed with the notion that fall risk management is primarily a nurse’s responsibility. A significant majority of physicians (63.8%) and nurses (86.3%) held a positive view that physician involvement enhances patient compliance in fall risk management. Furthermore, 80.0% of physicians and 96.2% of nurses considered it crucial for nurses to invite physicians to participate in managing patient fall risks. However, it was noteworthy that 53.8% of physicians and 67.6% of nurses reported that nurses seldom actively invite physicians to engage in fall risk management.
Physicians’ and nurses’ attitudes towards fall risk management.
3.2. Comparison of attitudes and participation of medical staff
Physicians’ self-assessed scores for fall risk management attitude and participation were 55.02 ± 8.124 and 51.47 ± 9.703, respectively. In contrast, nurses assessed physicians’ fall risk management attitude and participation with scores of 54.58 ± 9.096 and 42.77 ± 12.052, respectively. Upon further examination (Fig 2), the t-test for physicians’ attitude scores yielded a P-value >0.05, we performed a post*-hoc power analysis based on the two-sample mean difference test was conducted given the current sample size. The resulting power was 0.21. This suggests that the lack of significant inter-*group differences may be attributed to insufficient sample size. Future studies should consider expanding the sample size for further investigation. However, a statistically significant difference was observed in the scores related to the implementation of fall risk management (P < 0.001), indicating potential deficiencies in physicians’ execution of these practices in clinical work.
Comparison of attitudes and participation of medical staff ‘self-evaluation & other evaluation’ towards doctor’s fall risk management.
3.3. Influence factors of physicians’ participation in fall risk management
The linear regression analysis results, as presented in Table 4, indicated several key factors influencing physicians’ participation in fall risk management. Notably, degree of education, gender, the perceived importance of nurses inviting physicians, and the frequency of invitations emerged as significant determinants. Specifically, a higher literacy level among physicians was associated with lower participation in fall risk management. In contrast, female physicians demonstrated higher participation rates compared to their male counterparts. Furthermore, the perceived importance of nurses’ invitations significantly correlated with increased physicians participation. Additionally, a higher frequency of invitations from nurses was linked to greater physicians involvement in fall risk management.
Table 4: Multiple linear regression analysis of general information on physicians’ participation in fall risk management.
3.4. Patients’ perception of medical staffs’ participating in fall risk management
The results of this study showed that the patient-rated physician fall risk management participation score averaged 26.21 ± 7.842, while the adherence score was 8.04 ± 2.076. In comparison, the patient-rated nurse fall risk management participation score was 23.84 ± 6.025, with an adherence score was 8.35 ± 1.856. Comparative analyses revealed statistically significant differences between the scores for physician and nurse participation in fall risk management, as well as in patient adherence scores. These results are detailed in Table 5.
Table 5: Differential analysis of patients’ perception of physicians’ & nurses’ participating in fall risk management.
3.5. Major difficult factors of fall risk management
This study’s systematic analysis reveals differing perspectives on the challenges of implementing fall risk management. Physicians and nurses identified the primary obstacles as patient’s disease, insufficient patient attention, and low patient compliance. Conversely, patients attributed the difficulties mainly to their self-illness, Insufficient knowledge for falls, and environmental condition limitations. For further details, referred to Table 6.
Table 6: Ranking of factors that make it difficult to implement fall risk management in medical staff and patients.
4. Discussion
This study was a multi-center, large-sample survey design, which encompassed various regions and levels of medical institutions in China. This approach enhanced the representativeness and generalizability of the findings, providing a comprehensive reflection of the attitudes and behaviors of medical staff and patients in fall risk management. Furthermore, the study’s design considered the interactions between medical staff and patients, offering a holistic perspective for constructing an improved patient fall risk management system.
This survey revealed that while physicians, nurses, and patients all recognize the importance of fall risk management, actual participation in implementing these measures is suboptimal. Among the 2,775 nurses surveyed, the expected participation of physicians, based on the typical nurse-to-doctor ratio in China, should have been at least 925. However, only 580 physicians actively participated, indicating low motivation among physicians, similar to findings from a study of 60 hospitals in the United States [24]. Another study found that although participants acknowledged the importance of fall prevention, but 90% of them were willing to spend less than five minutes on it [25]. This may be due to some physicians perceiving fall risk management as primarily a nursing responsibility [3], and believing their involvement has minimal impact on patient adherence [26]. Patients, despite expressing willingness to cooperate, often fail to comply with fall prevention measures due to inadequate risk perception and attention. Active patient involvement in fall management is key to reducing fall rates in hospitals and increasing awareness of fall prevention. This success is tied to better self-awareness among patients, specialized care from medical staff, and broad interventions like improved environments, all of which are vital for effective fall prevention in healthcare.
We found that higher literacy levels among physicians correlate with lower engagement in fall risk management. This might result from insufficient targeted education and training [27]. As well as imbalanced work pressure and time allocation [28,29]. Despite physicians were well-educated, they may lack systematic training in fall risk management during their education and clinical practice. The demands of complex disease diagnosis, clinical teaching, and research further pressure physicians to prioritize more urgent tasks, relegating fall management. Additionally, female physicians were found to be more engaged than their male counterparts, possibly due to personality traits and empathy. Female physicians often exhibit greater empathy [30]and sensitivity to risk [31], enabling them to better understand patient conditions and identify potential fall risks, leading to more active participation in fall risk management.
Importantly, the frequency and perceived importance of nurses’ invitations to physicians significantly correlated with physicians’ participation. Nurses’ invitations enhance physicians’ sense of responsibility in patient safety, increasing their awareness and attention to fall risk management. Consequently, frequent invitations help establish a continuous habit of participation. Thus, encouraging nurses to invite physicians more frequently and advocating for physicians’ active participation are crucial for enhancing the effectiveness of fall risk management.
The study found that patients rated physicians’ participation in fall risk management higher than nurses’. This may stem from patients’ traditional cognitive biases, focusing more on disease treatment and overlooking risk prevention. Physicians are traditionally associated with diagnosis and treatment, while nurses are linked to risk prevention, leading to misconceptions about their roles. Interestingly, patients tend to adhere more to nurses due to the emphasis on fall prevention as a quality care indicator [32]. This focus prompts nurses to implement effective measures to reduce falls and injuries, whereas physicians may pay less attention to specific nursing operations related to fall prevention.
Medical staff and patients often have differing perceptions regarding the challenges of fall risk management. From the perspective of medical staff, three primary factors contribute to the difficulty in managing fall risks: insufficient patient attention, patient’s disease, and low patient compliance. Insufficient patient attention is a significant concern, as many patients fail to recognize the seriousness and potential harm of falls. This lack of awareness leads to a disregard for the advice and preventive measures recommended by medical staff, thereby increasing the risk of falls [33,34]. Additionally, patient disease factors play a crucial role. Certain medical conditions, such as neurological disorders, can impair physical functions, leading to balance disorders [35]and muscle weakness [36]. These conditions complicate the task of accurately predicting and preventing falls, as medical staff must consider the diverse characteristics and effects of various diseases. Moreover, low patient compliance further exacerbates the issue [37]. Despite medical staff dedicating substantial time and effort to developing detailed fall prevention plans and explaining their importance, some patients’ noncompliance hinders the effective implementation of these measures, significantly reducing management effectiveness.
Conversely, patients identify their self-illness, environmental condition limitations, and inadequate knowledge base as the primary challenges in managing fall risks. The presence of diseases such as cardiovascular [38]and skeletal muscle disorders [39]not only restricts mobility but also affects balance and cognitive functions, thereby increasing fall likelihood. Environmental conditions also pose significant challenges [40,41]Factors such as slippery floors, inadequate lighting, and inappropriate furniture layouts can trigger falls, and the inability to promptly modify these conditions to meet individual needs complicates fall risk management. Furthermore, patients often face a lack of knowledge regarding fall prevention [42]. This knowledge gap prevents them from accurately assessing their physical condition and mobility, understanding safe activities, and taking necessary precautions, thereby increasing fall risk and leaving them feeling overwhelmed by fall prevention efforts.
5. Limitations
The study had several limitations. First, the use of convenience sampling may restrict the generalizability of the findings, and the cross-sectional design precludes any analysis of temporal changes in attitudes or behaviors. Future research could employ probability sampling and longitudinal designs to enhance representativeness and trace developmental trajectories. Second, the reliance on self-reported quantitative data introduces potential discrepancies between stated attitudes and actual behaviors, and may not fully capture nuanced subjective experiences. Integrating qualitative methods in future studies could help explore underlying influencing factors in greater depth. Third, social desirability bias may have inclined participants to provide responses perceived as socially acceptable, rather than reflecting their true perspectives. Finally, the study’s focus was limited to in-hospital settings, leaving fall risk management in post-discharge contexts unexamined. Subsequent research should broaden its scope and increase the sample size to include transitional and community-based care.
6. Implications for practice
In this study, we present an interesting point, to enhance fall risk management, it is crucial to increase nurses’ awareness of the need to involve physicians, encourage nurses to invite physicians more frequently, and motivate physicians to participate actively. These measures are gaining popularity as effective strategies for improving management efficiency.
7. Conclusion
This study revealed that physicians, nurses, and patients generally possess a high level of cognitive awareness regarding fall risk management. This shared understanding underscores the collective recognition of the importance of patient safety and establishes a solid foundation for developing an effective fall risk management system. However, a notable discrepancy exists between this high level of cognition and actual participation, particularly among physicians. This gap might be attributed to factors such as physicians’ busy schedules and insufficient knowledge, as well as patients’ limited cognitive abilities and weak self-management skills. To address this issue, medical institutions should develop a comprehensive and systematic fall risk management system. This system should include measures to enhance communication and collaboration between physicians and patients, optimize healthcare resource allocation, and improve professional training programs. Additionally, medical staff should consider patients’ individual differences and provide comprehensive support and guidance to help them overcome self-management barriers, ultimately minimizing fall occurrences and ensuring patient safety and health.
Supporting information
S1 FigDescription of fall risk management by physicians and nurses.(TIF)
S2 FigComparison of attitudes and participation of physicians and nurses.(TIF)
S1 FileData on patients.(XLSX)
S2 FileData on physicians and nurses.(XLSX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lee D-CA, Day L, Hill K, Clemson L, Mc Dermott F, Haines TP. What factors influence older adults to discuss falls with their health-care providers?. Health Expect. 2015;18(5):1593–609. doi: 10.1111/hex.12149 26039594 PMC 5060806 · doi ↗ · pubmed ↗
- 2Ghosh M, O’Connell B, Afrifa-Yamoah E, Kitchen S, Coventry L. A retrospective cohort study of factors associated with severity of falls in hospital patients. Sci Rep. 2022;12(1):12266. doi: 10.1038/s 41598-022-16403-z 35851400 PMC 9293967 · doi ↗ · pubmed ↗
- 3Su Q, Song M, Mao Y, Ku H, Gao Y, Pi H. An analysis of the associated factors for falls, recurrent falls, and fall-related injuries among the older adults in senior Chinese apartments: A cross-sectional study. Geriatr Nurs. 2023;52:127–32. doi: 10.1016/j.gerinurse.2023.05.016 37290218 · doi ↗ · pubmed ↗
- 4Moreland B, Kakara R, Henry A. Trends in nonfatal falls and fall-related injuries among adults aged ≥65 years - United States, 2012-2018. MMWR Morb Mortal Wkly Rep. 2020;69(27):875–81. doi: 10.15585/mmwr.mm 6927 a 5 32644982 PMC 7732363 · doi ↗ · pubmed ↗
- 5Salari N, Darvishi N, Ahmadipanah M, Shohaimi S, Mohammadi M. Global prevalence of falls in the older adults: A comprehensive systematic review and meta-analysis. J Orthop Surg Res. 2022;17(1):334. doi: 10.1186/s 13018-022-03222-1 35765037 PMC 9238111 · doi ↗ · pubmed ↗
- 6Wang YLL. Trends and age-period-cohort model analysis of incidence and mortality of falls among elderly in China from 1990 to 2019. Chin J Evid-Based Med. 2024;24(07):783–91.
- 7Takase M, Kisanuki N, Nakayoshi Y, Uemura C, Sato Y, Yamamoto M. Exploring nurses’ clinical judgment concerning the relative importance of fall risk factors: A mixed method approach using the Q Methodology. Int J Nurs Stud. 2024;153:104720. doi: 10.1016/j.ijnurstu.2024.104720 38408403 · doi ↗ · pubmed ↗
- 8Guirguis-Blake JM, Perdue LA, Coppola EL, Bean SI. Interventions to prevent falls in older adults: Updated evidence report and systematic review for the US preventive services task force. JAMA. 2024;332(1):58–69. doi: 10.1001/jama.2024.4166 38833257 · doi ↗ · pubmed ↗