Thyroidectomy-Related Dysphagia: A Systematic Literature Review
Eleni Litsou, Chrissa Sioka, Konstantinos Mpakogiannis, Labrini Magou, Polyxeni Fakitsa, Alexandros Giannakis, Sakkou Sissy Foteini, Fotios Fousekis

TL;DR
This paper reviews how often and how long swallowing problems last after thyroid surgery, finding they are common but usually temporary.
Contribution
A systematic review of thyroidectomy-related dysphagia, analyzing incidence, progression, and associated factors across a large patient cohort.
Findings
Dysphagia incidence peaks in the first 1–2 weeks post-surgery and typically resolves within 2–3 months.
Persistent dysphagia is linked to factors like surgery extent, age, and adjuvant therapies.
Most patients improve, but some experience long-term symptoms affecting quality of life.
Abstract
Background and Objectives: Dysphagia is a frequently reported symptom among patients undergoing thyroidectomy, yet its incidence, underlying mechanisms, and temporal progression remain insufficiently clarified. The aim of the present systematic review was to synthesize the existing literature on the occurrence and evolution of swallowing disorders following thyroidectomy, without restriction regarding the extent of surgery, surgical approach, indication, or concomitant complications. Materials and Methods: A systematic literature review, according to PRISMA guidelines, was conducted in the electronic databases PubMed, MEDLINE, and SciELO, using the terms “dysphagia”, “deglutition disorder”, “swallowing disorder”, “thyroid surgery” and “thyroidectomy” in the appropriate combinations. A narrative synthesis of the results followed. Results: 31 eligible studies encompassing a total of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
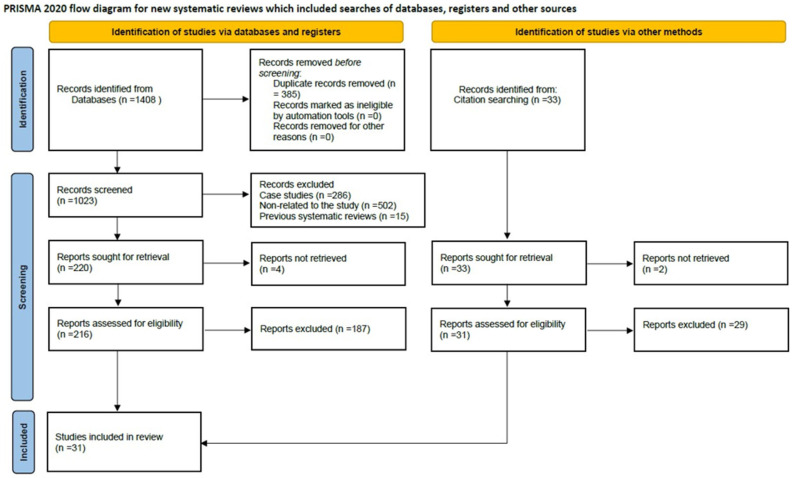 Figure 1
Figure 1| Authors | Year | Country | Study Design | Study Period | Indications | Sample | Preoperative Symptoms/Symptom | Operative Technique/Treatment | Results |
|---|---|---|---|---|---|---|---|---|---|
| Ben Nun et al. [ | 2006 | Israel | R | January 1990– | Retrosternal goiter | 75 | Choking, dyspnea | Cervical TT: 68 (91%). | Symptomatic improvement. |
| Almeida et al. [ | 2009 | Brazil | C-S | 1997–2006 | DTC | 154 | HR-QOL | TT: 100%; ND: | Better scores: Patients |
| Pradeep et al. [ | 2011 | India | R | Not specified | Hashimoto’s thyroiditis | 271 | Tightness in the neck, discomfort in swallowing | Thyroidectomy Group A: | Discomfort in swallowing and tightness in the neck were relieved at 3 months after surgery. |
| Silva et al. [ | 2012 | Brazil | C-S | May 2006– | DTC (46%), | 308 | UADS | Thyroidectomy: 208 OS without IONM, | Positive impact of IONM: decreasing the prevalence and degree of disturbance of long-term UADS after thyroidectomy. |
| Xu et al. [ | 2012 | China | RC | Not | Thyroid | 240 | POST severity | Thyroid Surgery: | Decrease in severity and |
| Gal et al. [ | 2013 | USA | C-S, R | 1992–2008 | Well DTC | 34 | QOL | 11 patients only TT | XRT group reported worse chewing, appetite, swallowing, and pain compared to RAI and TT groups. |
| Ryu et al. [ | 2013 | Republic of Korea | P, RC | Not specified | Elective thyroidectomy | 90 | Incidence and | All patients: | Adjusting the endotracheal cuff pressure during thyroidectomy decreased the incidence and degree of POST. |
| Alkan et al. [ | 2014 | Turkey | P | Not specified | Benign multinodular goiter | 16 | Pre- and postoperatively: | Primary TT: Group 1: | The use of seprafilm between larynx and strap muscles during TT does not result in any electrophysiological difference regarding swallowing. |
| Del Rio et al. [ | 2015 | Italia | P | Not specified | Benign and malignant of thyroid diseases | 80 | Self-evaluation of dysphagia to liquids and pain | Traditional thyroidectomy using reusable vs. disposable | Dysphagia for liquids on a scale from 0 to 10: Group A: |
| Chun et al. [ | 2015 | Republic of Korea | P, RC, | July 2013–February 2014 | Elective thyroid lobectomy of unspecified etiology | 64 | MDADI, LPS | General anesthesia provided with an LMA or ETI. | The use of LMA in general anesthesia for thyroid surgery has advantages over the ETI in relieving the laryngopharyngeal symptoms, and in decreasing patients’ subjective and objective voice symptoms, reducing the duration of symptoms. |
| Kim, D. Y. [ | 2015 | Republic of Korea | RC, | Not specified | Papillary thyroid carcinoma | 39 | Swallowing Impairment Index | Conventional, open TT: | ADM-assisted implants improve post-thyroidectomy scarring and swallowing impairments without prolonging operative |
| Exarchos et al. [ | 2016 | Greece | R | September 2012– | Not specified | 118 | SIS-6, | TT: | 48 h after TT: significantly lower SIS-6 in patients who received perioperative dexamethasone. |
| Wang et al. [ | 2016 | China | R | December 2012– | Substernal goiter | 27 | Not specified | 15 patients with laparoscopic thyroidectomy via areola approach; 12 patients with open thyroidectomy via low-neck collar cervical approach. | Laparoscopic thyroidectomy for the treatment of substernal goiter via the areola approach is feasible. |
| Sorensen [ | 2018 | Denmark | P, C-C, RC | November 2014– | Benign nodular goiter | 33 | Goiter symptom scale of ThyPRO, questionnaire HREM | TT, | Swallowing symptoms often worsened immediately after surgery but typically showed significant improvement compared to baseline by the 6-month mark. |
| Koo et al. [ | 2019 | Republic of Korea | P, RC | June 2016–November 2017 | Intraparenchymal thyroid cancer with a | 104 | Incidence and severity of hoarseness, | SERT: | No differences in the incidence of dysphagia hoarseness, or cough |
| Goswami et al. [ | 2019 | USA | R, C | Not specified | Thyroid Cancer Survivors | 1743 | HRQOL score, online survey regarding clinical history, PROMIS 29 | Surgery and RAI ablation. | High incidence of complications related to surgery and RAI ablation. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid and Parathyroid Surgery · Dysphagia Assessment and Management · Esophageal and GI Pathology
1. Introduction to the Systematic Review
Thyroidectomy is currently a very common surgical procedure and, more specifically, the most frequently performed procedure involving the endocrine glands. Swallowing disorders are now a recognized complication of this particular surgery, reported both after intraoperative nerve injury and after uncomplicated operations. However, it is worth noting that symptoms suggestive of dysphagia have also been reported after other surgeries, a fact that tends to dissociate thyroidectomy from being the sole operation potentially causing the onset of such symptoms. Furthermore, since in quite a few cases the patients-reported symptoms are not confirmed by objective examinations, several authors refer to these cases as “post-thyroidectomy syndrome.”
The symptoms associated with dysphagia after thyroidectomy, as well as their severity, vary considerably from patient to patient. They may include pain or discomfort when swallowing, a choking sensation, a feeling of a foreign body, the sensation of a “lump” in the throat, coughing, and others. Explaining the causes of these symptoms is not always possible, even after a series of examinations to investigate dysphagia.
Finally, dysphagia often appears preoperatively in patients with thyroid diseases and constitutes one of the possible indications for surgery in these cases. The scientific surgical community’s interest in the subject lies in the fact that such symptoms seem to negatively affect patients’ quality of life, even when the procedure is not performed in the context of malignancy. The impact of dysphagia on both daily life and the broader social life of patients is the reason they often seek medical assistance.
In addition to patient-reported symptoms, several studies have attempted to objectively assess swallowing function following thyroidectomy using instrumental methods, including videofluoroscopic swallowing studies, fiberoptic endoscopic evaluation of swallowing, high-resolution esophageal manometry, electromyography, and ultrasound-based kinematic analysis. These objective approaches have provided insight into postoperative alterations in laryngeal elevation, hyoid bone displacement, pharyngoesophageal segment pressure, and esophageal motility, particularly during the early postoperative period. However, the use of such tools remains inconsistent across studies, and objective findings do not always correlate with subjective symptom severity [1,2,3,4,5,6].
2. Materials and Methods
2.1. Search Strategy
The present systematic literature review on the occurrence of swallowing disorders in thyroidectomy, following the recently revised PRISMA guidelines for systematic reviews (File S1), was conducted in the electronic databases PubMed, MEDLINE, and SciELO, using the combination of keywords: [“dysphagia” OR “swallowing disorder” OR “deglutition disorder”] AND [“thyroidectomy” OR “thyroid surgery”]. These terms were chosen as umbrella terms, which consequently facilitated the inclusion of the broadest possible spectrum of relevant published studies. Duplicates were removed from the preliminary compilation of studies. Subsequently, the remaining articles were reviewed twice. Firstly, two independent reviewers (E.L. and M.K.) screened titles, abstracts, and full texts according to the eligibility criteria. The final evaluation of the process was confirmed by a third independent investigator (F.F.). Discrepancies were resolved by consensus and inter-rater agreement. The search was performed between August and September 2025.
2.2. Inclusion and Exclusion Criteria
The criteria by which the articles retrieved from the search were deemed eligible for inclusion in the study were as follows:
- ✓Research focusing on thyroidectomy performed on human subjects.
- ✓Swallowing disorder had to be reported at least at one time point after thyroidectomy and expressed as an absolute number of patients.
- ✓Both studies employing patient-reported assessments of dysphagia and those utilizing objective diagnostic methods for swallowing disorders were incorporated.
- ✓According to the definition of dysphagia in the literature, based on the symptoms through which it manifests, the present review also included studies that did not explicitly use the terms “dysphagia” or “swallowing disorder,” but described symptoms such as the sensation of a “lump,” a foreign body, or any other related discomfort.
- ✓Both prospective and retrospective studies, randomized or non-randomized, were included, regardless of the number of patients enrolled, whether the condition was benign or malignant, the extent of surgery (total thyroidectomy or lobectomy), the surgical technique (open, robotic, or endoscopic procedures), or the language of the text.
Conversely, from the outset, the following were excluded:
- ❖Articles that were previous reviews, case reports, animal studies, or those that could not be retrieved in full.
- ❖Studies that used questionnaire-based rating scales but did not report the absolute number of patients presenting the disorder, as their results were not comparable with those of other studies.
- ❖Articles that did not provide information on this specific postoperative disorder.
- ❖Studies involving patients with comorbidities capable of explaining the symptoms independently of thyroid disease (e.g., gastroesophageal reflux, neurological disorders).
Outcome assessment included both subjective patient-reported measures and objective instrumental evaluations of swallowing function. Subjective assessment was performed using validated or author-modified questionnaires, such as the Swallowing Impairment Score (SIS), SWAL-QOL, ThyPRO, and visual analog scales. Objective assessment methods, when available, included videofluoroscopic swallowing studies, fiberoptic endoscopic evaluation of swallowing, ultrasound evaluation of hyoid and laryngeal movement, electromyography, and high-resolution esophageal manometry. Due to methodological heterogeneity, objective data were narratively synthesized rather than quantitatively pooled [1,2,3,4,5,6].
2.3. Risk of Bias Assessment (ROBINS-I)
Risk of bias in non-randomized studies was assessed using the ROBINS-I tool (Table 1), while randomized controlled trials (RCTs) were evaluated using principles aligned with the Cochrane RoB 2 tool. Overall, studies showed a moderate to serious risk of bias, primarily due to confounding and outcome measurement.
Important confounders—such as preoperative swallowing status, extent of surgery, nerve monitoring, anesthesia-related factors, and adjuvant therapies—were inconsistently measured or adjusted for, limiting causal inference. Selection bias was common because of single-center designs, unclear recruitment, and lack of appropriate control groups.
Outcomes were mainly assessed using subjective, often non-validated patient-reported questionnaires, with limited use of objective measures, resulting in a high risk of detection bias. Blinding was rarely reported. Several longitudinal studies inadequately addressed missing data and loss to follow-up, increasing attrition bias. Selective reporting was suspected when absolute dysphagia rates or complete time-point data were not provided.
RCTs generally had lower risk of bias but were limited by small sample sizes, short follow-up, and incomplete blinding. Overall, these methodological limitations reduce confidence in estimates of post-thyroidectomy dysphagia and highlight the need for standardized outcomes and better-controlled prospective studies.
3. Results
3.1. Search Results
The initial search identified 1408 articles from the PubMed, MEDLINE, and SciELO databases. The removal of duplicate publications (n = 385) followed by those deemed irrelevant to the research content based on their title and abstract (n = 502), case reports (n = 286), and pre-existing reviews (n = 15) first excluded 1188 articles. Of the remaining articles (n = 220), four reports could not be retrieved. Thus, 216 reports were assessed for eligibility. After reading them, 187 articles were excluded as they did not meet the criteria of the present study. Only 29 studies were found to meet the inclusion criteria. Two more were retrieved after thorough scanning of the references of the above. Eventually, 31 studies were included in the systematic review. Search and screening results are shown in the PRISMA flowchart (Figure 1).
From the articles ultimately included, data were extracted regarding the type of study conducted and its time frame, demographic data of the study populations, and preoperative and postoperative data related to the occurrence of dysphagia. A comparison of these data then followed. Of these, 64.5% (n = 20) were prospective in design, 12.9% were retrospective (n = 4), while only 9.7% (n = 3) were randomized controlled trials. In 12.9% (n = 4), the methodology for symptom assessment or data collection was either insufficiently described or entirely unclear. An overview of the basic characteristics of each study is presented in Table 2.
3.2. Study Population and Design Characteristics
A total of 64,123 patients were included.The mean patient age was approximately 45 years, with one notable outlier affecting distribution.There was a predominance of female patients, consistent with thyroid disease epidemiology.There was wide variation in sample sizes (ranging from small case series to large multicenter studies).Studies showed broad geographic representation (USA, Brazil, Italy, China, and others).
3.3. Preoperative Dysphagia: Prevalence and Characteristics
Reported incidence varies widely (3.3–77.8%), reflecting substantial heterogeneity.Variability is largely attributable to non-standardized assessment methods (questionnaires, interviews).Symptoms are often intermittent, mild, and not always functionally limiting.Many patients report multiple swallowing-related complaints.Dysphagia is a significant factor influencing the decision for surgery, despite inconsistent severity.Only 11 of 31 studies reported preoperative dysphagia data, indicating probable under-recognition.
3.4. Factors Associated with Preoperative Dysphagia
3.4.1. Laryngeal Function
Dysphagia was observed in patients both with and without laryngeal mobility abnormalities.This suggests mechanisms beyond structural or neurological impairment.
3.4.2. Sex-Related Anatomical Differences
Men demonstrate greater laryngeal range of motion on ultrasound.There were differences attributed to anatomical variation in thyroid cartilage angle (≈90° in men vs. ≈120° in women).Clinical relevance remains uncertain.
3.4.3. Thyroid Size and Goiter Extension
There was no consistent association between thyroid gland size and dysphagia.Substernal goiters did not show higher dysphagia rates compared with overall averages.
3.5. Surgical Approaches and Indications
The majority of studies focused on conventional open thyroidectomy.Smaller numbers examined endoscopic, robotic, MIVAT, or combined techniques.Studies included total, subtotal thyroidectomy and lobectomy for both benign and malignant disease.Postoperative dysphagia incidence was not consistently stratified by surgical type or indication.
3.6. Postoperative Dysphagia: Temporal Pattern
Symptoms typically increase early postoperatively.They peak within the first postoperative week.Symptoms remain elevated during the first month, with gradual improvement after 2 weeks.Return to preoperative levels occurs by approximately 3 months.Limited long-term data are available; isolated late symptom increases lack baseline comparison.
3.7. Outcome Measurement Tools
Structured questionnaires were frequently used.The Swallowing Impairment Score (SIS) was the most commonly applied tool.Objective assessments were inconsistently employed.
3.8. Role of Surgical Complications
3.8.1. Uncomplicated Thyroidectomy
Dysphagia was commonly reported despite intact recurrent laryngeal nerves.This indicates that dysphagia can occur independently of overt nerve injury.
3.8.2. Possibly Complicated Thyroidectomy
Includes transient nerve paresis or unspecified nerve status.Higher dysphagia incidence was observed at one month postoperatively.Early postoperative dysphagia was more frequent in uncomplicated cases.
3.9. Comparative Findings and Limitations
Conflicting results were reported regarding the impact of nerve injury and surgical technique.Small number of comparative studies limits interpretability.Evidence was insufficient to draw definitive conclusions regarding causation or prevention.
4. Discussion
This systematic review evaluated the occurrence, progression, and determinants of swallowing disorders following thyroidectomy. Unlike prior reviews, this analysis encompassed all types of thyroid surgery—total or partial, open, endoscopic, robotic, or minimally invasive—regardless of the underlying diagnosis or concomitant complications, allowing a comprehensive assessment of postoperative dysphagia across diverse clinical settings.
Patients most commonly report dysphagia as a sensation of a “lump” or foreign body, difficulty clearing the larynx, throat dryness, or pain during swallowing [1,31]. Interestingly, subjective complaints often exceed the frequency of objectively detectable abnormalities, suggesting a multifactorial etiology that includes mechanical trauma, postoperative pain, tissue adhesions, psychosomatic factors, or neural injury, particularly to the recurrent or superior laryngeal nerves [13,19,20].
Across the literature, dysphagia generally peaks during the first one to two postoperative weeks and progressively declines to preoperative levels by 2–3 months, with further improvement by 4–6 months [1,2,10,11,13,19,20,27]. Objective assessments using the Swallowing Impairment Score (SIS) or videofluoroscopy confirm early postoperative impairment in laryngeal motility and hyoid excursion, with gradual recovery over the first three months [1,4,6,19,20,22]. Notably, patients with preoperative laryngeal mobility impairment may experience more severe and prolonged symptoms [1,19]. Although most patients recover, some reports describe persistent dysphagia extending into the long-term postoperative period, even years after surgery [9,13,16]. Conversely, patients presenting with preoperative dysphagia often benefit from thyroidectomy, particularly in cases of substernal goiters [3,10,11,12,15,33,34].
Age and sex have been explored as potential risk factors. Older age may correlate with worse early postoperative symptoms in some studies [19,30], but the evidence is inconsistent [4]. Female sex and lower psychological well-being have been associated with increased subjective complaints preoperatively [29], highlighting the interplay of psychosocial factors in symptom perception.
Objective assessment of swallowing function after thyroidectomy has demonstrated measurable, predominantly transient impairments in laryngeal elevation, hyoid excursion, and pharyngoesophageal segment dynamics. Studies employing videofluoroscopy and kinematic analysis have confirmed early postoperative pharyngeal phase abnormalities with gradual recovery within the first three postoperative months. High-resolution esophageal manometry has shown postoperative alterations in upper esophageal sphincter pressure and esophageal motility, particularly in patients with large goiters, with significant improvement over time. Ultrasound-based studies have further identified reduced hyoid bone displacement during swallowing in the early postoperative period. Importantly, objective findings do not consistently parallel patient-reported symptom severity, underscoring the multifactorial and partially subjective nature of post-thyroidectomy dysphagia [1,3,4,5,6].
The extent of surgery, particularly total thyroidectomy, and procedures involving central or lateral lymph node dissection is consistently associated with higher rates of postoperative dysphagia [16,26,28,29]. The comparison between total thyroidectomy and lobectomy yields mixed results; some studies show higher symptom scores with total thyroidectomy in the first three months postoperatively, reflecting transient laryngeal mobility impairment [5,28]. Minimally invasive and robotic techniques offer potential advantages in reducing tissue trauma, adhesions, and scarring, potentially mitigating dysphagia [8,14,18]. However, studies comparing open, endoscopic, and robotic thyroidectomy demonstrate heterogeneous outcomes, likely due to differences in access routes, trocar positioning, and surgeon experience [17,21,23,24,25,32,35]. Current evidence does not definitively confirm superiority of minimally invasive techniques in improving swallowing function, emphasizing the need for large-scale, controlled trials. Technical modifications, including the subfascial versus subplatysmal approach, selective ligation of superior thyroid vessels, and the use of anti-adhesion materials, may influence postoperative outcomes, though the evidence remains limited [19,36,37,38]. Intraoperative nerve monitoring reduces the incidence of postoperative swallowing complaints [16]. From an anesthesiological perspective, strategies that minimize airway trauma—such as using smaller endotracheal tubes, flexible laryngeal masks, intraoperative cuff pressure monitoring, or intravenous lidocaine—have been shown to reduce early postoperative dysphagia [39,40,41,42]. Similarly, perioperative administration of corticosteroids may further mitigate symptoms [43]. Studies related to modifications in treatment practice, perioperative strategies or technical equipment of thyroidectomy in order to reduce postoperative dysphagia are presented in Table 3.
Radioactive iodine and external beam radiotherapy, while essential in oncologic management, may exacerbate postoperative dysphagia [44,45]. These findings underscore the importance of balancing therapeutic efficacy with functional outcomes when planning adjuvant treatment.
Dysphagia has a substantial negative effect on health-related quality of life, influencing both physical and psychological domains [3,46,47]. Even when symptoms are mild or transient, they may reduce patient satisfaction and motivation for surgery, highlighting the need for comprehensive preoperative counseling and long-term monitoring.
Overall, postoperative swallowing dysfunction after thyroidectomy is multifactorial, influenced by patient characteristics, surgical extent, technique, perioperative management, and adjuvant therapies. Recognition of the temporal pattern of recovery, coupled with individualized surgical planning, technical modifications, and perioperative interventions, can help mitigate symptoms and improve patient-centered outcomes. Future research should prioritize standardized definitions and objective assessment tools, and directly compare surgical approaches in high-quality, multicenter studies.
5. Conclusions
Post-thyroidectomy dysphagia represents a clinically significant complication with important implications for patient care and surgical planning. Its multifactorial nature underscores the need for individualized perioperative strategies, including careful patient counseling, optimized surgical technique, meticulous perioperative management, and consideration of adjuvant therapies. Emerging minimally invasive and robotic approaches may offer functional and esthetic benefits, but current evidence does not conclusively demonstrate superiority in reducing swallowing dysfunction. Objective and subjective assessments of swallowing, alongside long-term follow-up, are critical for identifying at-risk patients and guiding interventions. By highlighting the clinical relevance of dysphagia and its determinants, this review provides a foundation for future research aimed at optimizing surgical outcomes, minimizing functional morbidity, and improving quality of life for patients undergoing thyroidectomy.
Difficulties and Limitations
This systematic review was limited by gaps and inconsistencies in the existing literature. Many studies lacked detailed preoperative data, making it difficult to determine whether postoperative changes reflect true improvement or decline. Short follow-up periods and reliance on heterogeneous or author-modified rating scales further restricted assessment of long-term outcomes and comparability across studies. Overall, the absence of standardized evaluation protocols for swallowing function before and after thyroidectomy limits the reliability of pooled findings and underscores the need for uniform assessment methods in future research. According to the ROBINS-I assessment, the overall certainty of evidence was limited by a moderate to serious risk of bias, particularly due to confounding and non-standardized outcome measurement.
Furthermore, although several studies incorporated objective instrumental assessments, their limited number, heterogeneous methodologies, and inconsistent timing of evaluation precluded meaningful quantitative synthesis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Arakawa-Sugueno L. Ferraz A.R. Morandi J. Capobianco D.M. Cernea C.R. Sampaio M.A. Kulcsar M.A.V. Simões C.A. Brandão L.G. Videoendoscopic Evaluation of Swallowing After Thyroidectomy: 7 and 60 Days Dysphagia 20153049650510.1007/s 00455-015-9628-z 26087901 · doi ↗ · pubmed ↗
- 2Lombardi C.P. D’Alatri L. Marchese M.R. Maccora D. Monaco M.L. De Crea C. Raffaelli M. Prospective electromyographic evaluation of functional post thyroidectomy voice and swallowing symptoms World J. Surg.2012361354136010.1007/s 00268-012-1481-822382763 · doi ↗ · pubmed ↗
- 3Sorensen J.R. The impact of surgery on quality of life, esophageal motility, and tracheal anatomy and airflow in patients with benign nodular goiter Dan. Med. J.201865 B 547229619937 · pubmed ↗
- 4Costa B.O.I.d. Rodrigues D.d.S.B. Magalhães D.D.D.d. Santos A.S. Santos R.V. Azevedo E.H.M. Almeida A.A. Pernambuco L. Quantitative Ultrasound Assessment of Hyoid Bone Displacement During Swallowing Following Thyroidectomy Dysphagia 20213665966910.1007/s 00455-020-10180-532889628 · doi ↗ · pubmed ↗
- 5Cho J.-G. Byeon H.K. Oh K.H. Baek S.-K. Kwon S.-Y. Jung K.-Y. Woo J.-S. Objective Assessment of Postoperative Swallowing Difficulty Through Ultrasound in Patients Undergoing Thyroidectomy Dysphagia 20203525326010.1007/s 00455-019-10020-131127378 · doi ↗ · pubmed ↗
- 6Im I. Jun J.-P. Crary M.A. Carnaby G.D. Hong K.H. Longitudinal Kinematic Evaluation of Pharyngeal Swallowing Impairment in Thyroidectomy Patients Dysphagia 20193416116910.1007/s 00455-018-9949-930298382 · doi ↗ · pubmed ↗
- 7Page M.J. Mc Kenzie J.E. Bossuyt P.M. Boutron I. Hoffmann T.C. Mulrow C.D. Shamseer L. Tetzlaff J.M. Akl E.A. Brennan S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews BMJ 2021372 n 7110.1136/bmj.n 7133782057 PMC 8005924 · doi ↗ · pubmed ↗
- 8Ikeda Y. Takami H. Sasaki Y. Takayama J. Niimi M. Kan S. Comparative study of thyroidectomies. Endoscopic surgery versus conventional open surgery Surg. Endosc.2002161741174510.1007/s 00464-002-8830-x 12140635 · doi ↗ · pubmed ↗