Scedosporium apiospermum: An Emerging yet Overlooked Fungal Pathogen in Veterinary Medicine—A Case-Based Review
Dubravka Milanov, Suzana Vidaković-Knežević, Vladimir Polaček, Marko Pajić

TL;DR
This paper reviews Scedosporium apiospermum, a fungal pathogen causing infections in animals, emphasizing its underdiagnosis and the need for better detection and treatment.
Contribution
The paper presents a case-based review of S. apiospermum infections in animals, including a first confirmed isolate in the Western Balkans and a tabulated overview of documented cases.
Findings
S. apiospermum is an emerging pathogen causing infections in immunocompromised animals.
Infections are often misdiagnosed as aspergillosis or fusariosis due to morphological similarities.
A confirmed case in a cow with mastitis highlights the need for improved diagnostic approaches.
Abstract
Scedosporium apiospermum is an emerging filamentous fungus of increasing clinical relevance in human and veterinary medicine. Previously regarded as a ubiquitous soil saprophyte, it is now recognized as an opportunistic pathogen causing a wide spectrum of localized and systemic infections, particularly in immunocompromised hosts. Although infections in animals are considered rare, they are likely underdiagnosed or misidentified as aspergillosis or fusariosis due to overlapping clinical features and morphological similarities. The first confirmed animal isolate of S. apiospermum in the Western Balkans, identified in 2024 from the milk of a cow with clinical mastitis, highlights the need for increased awareness and accurate diagnostic approaches for this neglected pathogen in veterinary practice. This review outlines key information on S. apiospermum infections in animals, including…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
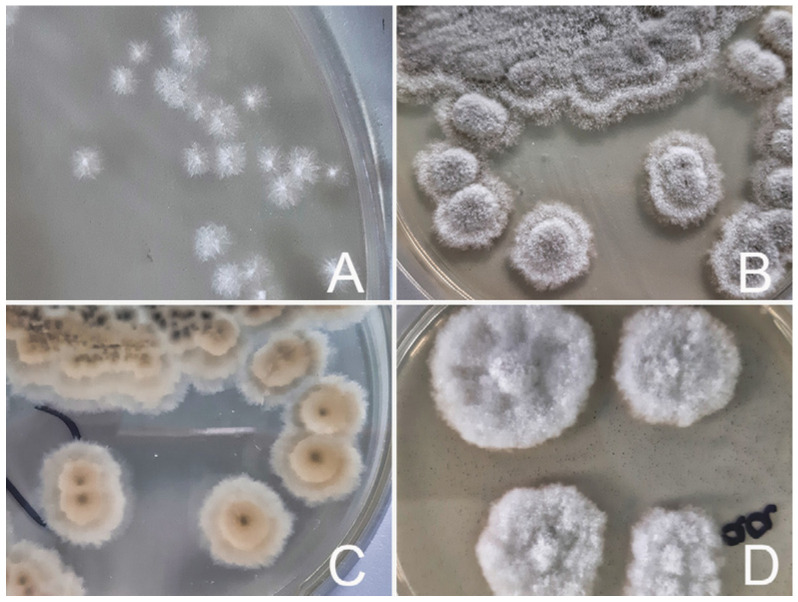 Figure 1
Figure 1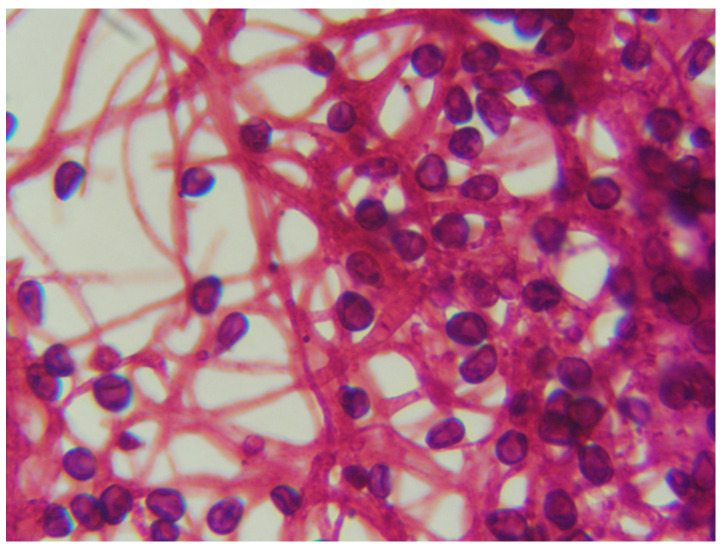 Figure 2
Figure 2| Country | Age, Sex and Breed | Anamnesis, Disease Symptoms, and Clinical Findings | Treatment and Outcome | Causative Agent Identification | Reference |
|---|---|---|---|---|---|
| (a) | |||||
| Dogs | |||||
| Spain | 10-month-old Male | -6-month history of mucopurulent bilateral nasal discharge and some sneezing; unresponsive to antibiotics; | -oral ketoconazole and amoxicillin; | Culture | [ |
| New Zealand | 2-year-old Female | -6-month history of sneezing and mucous discharge from the right nostril; reduced airflow; | -no treatment; | Culture | [ |
| Spain | 2-year old intact Female Labrador retriever | -8-month history of bilateral mucopurulent nasal discharge; | -surgical debridement with topical clotrimazole treatment; | Culture | [ |
| USA | 9-year-old | -3-month history of intermittent, right-sided epistaxis; previously treatment with enrofloxacin, prednisone and amoxicillin/clavulanate. | -debridement, frontal sinus trephination and clotrimazole therapy; | Culture, | [ |
| Italy | 4-year-old Female neutered Bull Terrier | -history of partially hemorrhagic, unilateral, mucopurulent left-sided nasal discharge and reverse sneezing; failure to respond to antibiotic therapy; | -nasal cavities infused with miconazole; | Culture | [ |
| Australia | 8-year-old | -history of violent sneezing and licking at the nasal planum; | -the grass seed was removed; | Culture, | [ |
| UK | 10-year-old | -unilateral nasal discharge; long-term treatment with prednisolone; | -3-month treatment with itraconazole, followed by topical treatment with clotrimazole without surgical debridement; | Culture | [ |
| Cat | |||||
| France | 3-year-old neutered Male Bengal cat | -history of mucopurulent bilateral nasal discharge and chronic sneezing; several courses of antibiotics without any improvement; | -surgical debridement; | Culture | [ |
| Cattle | |||||
| USA | 2-year-old Hereford cow | -chronic upper respiratory dysfunction, increased respiratory noise, and bloody nasal discharge; prior empiric therapy with parenteral oxytetracycline and sodium iodide; | -parenteral antihistamine | Culture | [ |
| Horses | |||||
| UK | 8-year-old mare | -for two years several episodes of left-sided purulent to mucopurulent nasal discharge; treated with sulphonamides; | -mare was euthanized at the owner’s request. | Culture | [ |
| USA | 18-year-old | -bilateral, mucopurulent nasal discharge; empirical judgment with penicillin G and trimethoprim-sulfamethoxazole; | -topical treatment with miconazole and systemic treatment with sodium iodide and potassium iodide; | Culture | [ |
| (b) | |||||
| Dogs | |||||
| USA | 8-year-old West Highland White Terrier | -bilateral chronic keratoconjunctivitis sicca and corneal ulceration in the right eye; a history of chronic topic ocular therapy with antibiotics and corticosteroids. | -the owner chose to proceed with orbital exenteration due to the uncertain prognosis and the prospect of long-term treatment. | Culture | [ |
| UK | 6-year-old dog Male castrated Norfolk Terrier | -21-day history of an increasingly painful eye; the dog had been on systemic steroids for inflammatory bowel disease for the previous 3 months and 21-day period of antibiotic use; | -keratectomy; | PCR (DNA was extracted from the corneal scrape). | [ |
| Horses | |||||
| USA | Quarter Horse | Keratomycosis. Despite topical treatment with miconazole and natamycin, the cornea developed a stromal abscess. Orbital exenteration was performed after 3 weeks. Full-text not available. | [ | ||
| USA | 11-year-old American Saddlebred gelding | -2 years earlier a painless white corneal opacity in the left eye;1 month previously noted mass involving the left eye and had subsequently increased in size; | -initial: neomycin–bacitracin–polymyxin; | Culture | [ |
| Poultry | |||||
| Australia | 42-day-old birds | -42-day-old birds in a layer pullet flock have ocular abnormalities, unilateral keratoconjunctivitis and apparent exophthalmos; thick, cream apparently fibrinous ocular discharge; | -not treated. | Culture | [ |
| (c) | |||||
| Dogs | |||||
| Australia | 2y | -immune-mediated polyarthritis and immune-mediated hemolytic anemia; immunosuppressant therapy; | -successful treatment with itraconazole, azathioprine and terbinafine. | Culture | [ |
| India | age and sex-not specified | -a history of dogfight, which had caused a bite wound on its right front leg, | -successful oral treatment with itraconazole and voriconazole for 4 weeks and another two months to avoid relapse. | Culture and molecular confirmation by gene sequencing | [ |
| Horse | |||||
| USA | 11-year-old Quarter Horse gelding | -a cutaneous mass adjacent to the medial canthus of the left eye, present for approximately six months; | -successful treatment: curative excision. | Immunofluorescent examination of | [ |
| Country | Age, Sex and Breed | Anamnesis, Disease Symptoms, and Clinical Findings | Treatment and Outcome | Pathological | Causative Agent Identification | Reference |
|---|---|---|---|---|---|---|
| Dogs | ||||||
| USA | 6-year-old spayed Miniature Poodle | -previous rupture of the uterus and ovariohysterectomy with stainless steel sutures, antibiotics treatment; | -surgical excision of the mass; | -acute peritonitis; | Culture | [ |
| USA | 2-year-old | -at six months of age, the dog underwent an ovariohysterectomy, but recovery was complicated by abdominal incision dehiscence and subsequent evisceration; previously antibiotic treatment for six weeks; chronic weight loss, fever, diarrhea, vomiting; | -supportive therapy with intravenous fluids and antibiotic; | -pathological diagnosis: pyogranulomatous peritonitis, hepatitis, pneumonia, vasculitis and thrombosis. | Culture | [ |
| USA | 5-year-old castrated Male German Shepherd | -3-week history of lethargy, intermittent fever; left forelimb lameness; | -the dog was euthanized. | -large cranial mediastinal mass; generalized lymphadenomegaly, | Immunofluorescence | [ |
| USA | 3-year-old Male Siberian Husky | -1 month history of weight loss and signs of depression, fever, vomiting; previous treatment: penicillin and dexamethasone parenterally; | -orchiectomy and ketoconazole; | -purulent peritonitis; | Culture and immunofluorescence (using fluorescein isothiocyanate-conjugated immunoglobulins specific for | [ |
| France | 6-year-old Female German Shepherd Dog | -progressive rear limb paresis/paralysis; | -enrofloxacin and intravenous corticosteroid; | -chronic, severe, pyogranulomatous fungal T13-L1 vertebral osteomyelitis and discospondylitis. | PCR and sequencing on formalin-fixed, paraffin- embedded | [ |
| Germany | 4-year-old mixed-breed | -chronic gastrointestinal signs (vomiting, lethargy anorexia); polydipsia; previously: antibiotic therapy; | -surgical resection (hepatic lobectomy and enterectomy of parts of the descending duodenum); | NA | DNA sequencing | [ |
| Italy | 10-month-old Female | -weakness, lethargy, lateral decubitus, miosis and muscular rigidity; | -supportive therapy with intravenous fluids and amoxicillin-clavulanic acid; | -Severe multifocal fungal pyogranulomas in kidney, mesentery, lymph nodes, and mammary gland. | Culture | [ |
| USA | 10-year-old intact Male | -prior history of septic peritonitis caused by gastrointestinal perforation related to the use of nonsteroidal anti-inflammatory drugs, as well as a right femoral head and neck ostectomy; | -itraconazole: 5 mg/kg for 6 months; | NA | Culture, | [ |
| USA | 5-year-old, spayed Female, Basset Hound | -hematuria, stranguria, and urinary incontinence over a period of 4 months; | -surgical excision of the mass; | NA | Culture and | [ |
| Japan | 6-year-old castrated Male Golden Retriever | -history of gastrointestinal anastomosis under laparotomy 2 years earlier; | -surgical removal of the masses; | NA | Culture and | [ |
| USA | 2-year-old intact Female mixed-breed dog | -a chronic history of nonspecific gastrointestinal signs: vomiting, hyporexia and progressive weight loss; -unsuccessfully managed with famotidine; | -due to the extensive nature of the lesions and the poor prognosis associated with intra-abdominal fungal infection, the owner elected euthanasia. | -the peritoneum was diffusely thickened, exhibiting dark-red discoloration and extensive fibrous adhesions involving the liver, pancreas, intestines, stomach, and mesentery. | Culture and | [ |
| Cattle | ||||||
| India | 45 days old dead calf | NA | NA | -severe pneumonic granulomatous lesions containing septate, pleomorphic hyphae were observed in the central caseated core, which had a bright eosinophilic periphery surrounded by polymorphonuclear cells and macrophages, followed by a zone of epithelioid cells mixed with lymphocytes. | Culture | [ |
- —Ministry of Science, Technological Development and Innovation of the Republic of Serbia, Belgrade, Serbia
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMilk Quality and Mastitis in Dairy Cows · Antifungal resistance and susceptibility · Nail Diseases and Treatments
1. Introduction
1.1. The Genus Scedosporium: Taxonomy and History
Filamentous fungi of the genus Scedosporium belong to the family Microascaceae, order Microascales, and phylum Ascomycota [1,2]. The genus currently comprises ten species: S. aurantiacum, S. cereisporum, S. desertorum, S. dehoogii and S. minutisporum, in addition to the S. apiospermum species complex, which includes S. angustum, S. apiospermum, S. boydii, S. ellipsoideum, and S. fusoideum [2,3,4]. Species are distinguished phylogenetically by comparing the sequences of a fragment of the β-tubulin gene (TUB2) [3]. S. apiospermum, S. boydii and S. aurantiacum are considered the most clinically relevant species, causing infections in both humans and animals [1,2].
The earliest documented infection caused by fungi of the Pseudallescheria/Scedosporium complex dates back to 1889, when Pseudallescheria boydii was identified as the etiological agent of human otitis [5,6]. The generic name of the genus was proposed in 1911 by Saccardo, who described an isolate obtained from a patient with mycetoma in Italy and named it Monosporium apiospermum. The isolate developed only the asexual state and was classified as a deuteromycete. In the same year, Saccardo proposed the generic name Scedosporium, which was later validated in 1919 by Castellani and Chalmers, who established the combination Scedosporium apiospermum [3,7,8]. However, the term was not widely adopted at that time.
The nomenclature and taxonomy of the genus Scedosporium have long been a source of confusion and have undergone multiple revisions throughout the twentieth century. Historically, Scedosporium apiospermum (formerly Monosporium apiospermum) and Pseudallescheria boydii (previously Allescheria boydii and Petriellidium boydii) were regarded as two morphological forms of a single fungal species, representing the asexual (anamorphic) and sexual (teleomorphic) states, respectively [7]. Subsequent phylogenetic analyses using multilocus sequencing revealed clear genetic distinctions, confirming that S. apiospermum and P. boydii are, in fact, distinct species [2,4]. For practical purposes, however, these fungi are often referred to collectively as the “Scedosporium/Pseudallescheria Complex Fungi” (SPCF), a group comprising six pathogenic species: S. boydii, P. angusta, S. minutispora, S. dehoogii, S. aurantiacum, and S. apiospermum [9]. The term “species complex” may refer to a formally recognized taxonomic grouping below the genus level, some closely related strains with uncertain taxonomic status, or distinct species that cannot be precisely identified due to practical limitations [10].
1.2. Distribution in the Environment
S. apiospermum is a saprophytic fungus commonly found in soil worldwide, particularly in temperate climates and less frequently in tropical regions [1,5,11]. It has successfully adapted to environments characterized by low oxygen levels and high osmotic pressure. Consequently, they are more frequently isolated from urban and industrial environments such as sewers, polluted waters, sediments, agricultural soils, poultry and cattle manure, hydrocarbon-contaminated soils, gardens, urban parks, playgrounds, hospital areas, and farmlands [1,6,8,12]. None of the Scedosporium species were isolated from soil samples collected in natural environments such as woods, wetlands, and sludge in Austria and the Netherlands, but S. apiospermum was the most abundant species in areas characterized by intense human activity [12]. Similarly, S. apiospermum was the predominant species detected in soil and water samples obtained from public parks in Thailand [6]. It was also found in soils collected from urban gardens and industrial parks across different regions of Mexico [13], further underscoring its strong ecological association with anthropogenically influenced habitats. A total of 155 soil samples were obtained from diverse ecological settings throughout Lebanon, encompassing both urbanized and undisturbed environments. Of these, 25.16% were culture-positive for Scedosporium spp. [14]. S. apiospermum represented the dominant taxon, accounting for 80.56% of isolates. Scedosporium spp. were predominantly isolated from pigsties, refugee camps, and various urban or semi-urban settings, including recreational spaces, port facilities, and cultivated plant beds. Moderate detection rates were observed in industrial areas, agricultural fields, and waste disposal facilities. Conversely, markedly reduced isolation rates were noted in natural and domestic environments, such as parks, woods, residential areas, gardens, gas stations, and roadways. Notably, no isolates were obtained from the Palm Islands Nature Reserve or coastal shorelines. Soil pH analysis revealed that culture-positive samples ranged from 6.2 to 7.87 (mean = 6.98), whereas the culture-negative samples from Palm Islands and shoreline sites exhibited alkaline values exceeding 8.19 [14]. Collectively, these findings indicate that anthropogenic activity substantially influences the environmental distribution and abundance of Scedosporium spp. The absence of the fungus in undisturbed coastal and island habitats further supports the hypothesis that Scedosporium may serve as a potential bioindicator of human impact on soil ecosystems [14]. The increasing rate of environmental detection of S. apiospermum raises concern that infections could become more frequent in domestic animals and poultry, as they have in humans.
1.3. Scedosporium apiospermum as a Causative Agent of Animal Diseases
Most knowledge about Scedosporium infections comes from human cases; whereas, this review focuses only on infections observed in animals, with the aim of highlighting the diagnostic and therapeutic challenges encountered in this field. In veterinary medicine, infections caused by S. apiospermum are reported less frequently than in humans; however, their true prevalence is likely underestimated [15,16]. This apparent discrepancy may reflect diagnostic challenges rather than a genuinely lower incidence. Many cases may remain undiagnosed or misdiagnosed—most commonly as aspergillosis due to similar clinical manifestations, similar radiological findings, and comparable histopathological features—or scedosporiosis may not be suspected, partly due to limited awareness of these infections among veterinary practitioners [15,16,17,18].
Infections caused by S. apiospermum are generally classified into three main clinical syndromes: (A) localized disease following traumatic inoculation, (B) asymptomatic or symptomatic colonization of body cavities, and (C) systemic invasive disease, particularly in immunocompromised hosts [5]. Owing to historical changes in nomenclature and evolving taxonomic understanding, infections caused by this species have been reported in the literature under a variety of names, including allescheriasis, graphiosis, monosporiosis, petriellidiosis, pseudallescherioma, pseudallescheriasis, pseudoallescheriosis, or scedosporiosis [5,7]. This terminological variability has, in some instances, complicated retrospective data interpretation and epidemiological comparisons across studies.
Mycetoma represents one of the classical and most recognizable clinical manifestations of S. apiospermum infection [5]. Most reports of mycetoma in domestic animals-particularly dogs, cats, and horses-originate from North America, the southern United States, South Africa, the United Kingdom, and Australia [19]. These chronic, progressively destructive infections are caused by a variety of opportunistic microorganisms–including filamentous fungi (eumycetoma) and bacteria (actinomycetoma), which exhibit similar clinical features [19]. Clinically, mycetoma is characterized by tumefaction of affected tissues, formation of draining sinus tracts, and extrusion of grains composed of compacted microorganisms embedded within host inflammatory cells [20].
The mycelial biomass of Scedosporium spp. exhibits structural characteristics resembling a biofilm-like organization, consisting of dense aggregates of hyphae embedded within an extracellular polymeric matrix that enhances structural stability and persistence within host tissues [7,21]. Over time, lesions may extend into deeper tissues, potentially resulting in vascular invasion and subsequent hematogenous or lymphatic dissemination [7,18,20]. Scedosporium spp. secrete bioactive molecules that facilitate tissue colonization, nutrient acquisition, survival within host tissues, and evasion of both cellular and humoral immune responses, thereby promoting chronicity and persistence of infection. A recent proteomic analysis identified more than 120 secreted proteins in S. apiospermum, highlighting the complexity of its pathogenic mechanisms [21]. The incubation period for mycetoma is variable, generally ranging from several weeks to several years [22]. Importantly, no zoonotic transmission of Scedosporium spp. has been documented to date [23].
The majority of reported infections in animals involve the nasal cavity and eyes. A significant number of cases of visceral (endogenous) mycetomas and disseminated infections have also been documented. Reports of localized S. apiospermum infections in animals for which full case details were available are summarized in chronological order in Table 1 (nasal cavity, ocular, and cutaneous infections). Visceral eumycotic mycetomas and severe, often fatal disseminated infections are summarized in Table 2.
As clinical manifestations and pathological changes vary considerably depending on the site of infection, detailed case-specific information is provided in Table 1 and Table 2, with all data extracted directly from the original case reports to ensure accurate summarization and minimize the risk of misinterpretation. In the presented cases, P. boydii and S. apiospermum are considered two morphological forms of the same fungus.
2. Overall Observations
2.1. Routes of Infection and Predisposing Factors
Respiratory infections caused by S. apiospermum are typically acquired via the aerogenic route, with exposure to high environmental spore concentrations representing the primary predisposing factor [26]. Ocular infection most commonly results from trauma, as disruption of the corneal epithelium allows direct inoculation of fungal organisms into the cornea, often through contaminated plant material. Previous treatment of corneal ulceration, especially long-term antibiotics and corticosteroid therapy, is a significant predisposing factor [20,34]. Topical application of antibiotics can alter the normal ocular flora and may increase nutrient availability for opportunistic pathogens. Aminoglycosides (including gentamicin) are toxic to the epithelial cells, making the cornea more susceptible to fungal infection. Corticosteroids promote fungal proliferation by facilitating the transition from a saprophytic to a pathogenic state, while simultaneously reducing tissue resistance and impairing host immune responses [33]. In the studies involving fungal inoculation of the rabbit corneas, absence of corticosteroid treatment resulted in a strong cellular inflammatory reaction and fungal elements remained as spores. In contrast, when corticosteroids were administered subconjunctivally or topically to the eye, the cellular inflammatory reaction was much less intense, while fungal spores developed into hyphae, and infection became more widespread [33].
Visceral and systemic infections caused by S. apiospermum are often associated with previous penetrating trauma or surgical procedures. Most reported cases of eumycotic mycetoma in the abdominal cavity of dogs strongly suggest that the surgical site frequently serves as the route of infection [39,40,52]. Although no history of abdominal trauma was reported in this particular case, it was speculated that the fungus most likely disseminated into the abdominal cavity along with intestinal contents during surgery or the postoperative healing process [45]. In another case, detailed pathological findings indicated that fungus-infected plant material embedded in the duodenal wall was the probable source of infection [42]. In a case of Scedosporium infection of the urinary tract in a dog, a history of multiple traumatic injuries over several years was documented [22].
In some rare cases, the exact portal of entry for S. apiospermum remains unknown. Such instances include intra-abdominal infection [17], disseminated infection [18], osteomyelitis and discospondylitis [43], and ureteral and bladder granulomas [44], all of which have been reported in dogs. In a canine case of disseminated intra-abdominal infection [46], no evidence of prior abdominal surgery or traumatic injury was found; however, it was strongly suspected that penetrating trauma through the abdominal wall was the most likely route of infection. Similarly, it has been speculated that the dog may have contracted S. apiospermum through a skin abrasion [18].
Disseminated infections are typically associated with conditions that impair immune function, most notably chronic diseases and immunosuppressive therapy. In most cases presented in Table 2, anamnesis indicated that animals had received repeated and/or prolonged empirical antibiotic treatment and symptomatic corticosteroid therapy following the initial veterinary examination. Both of these mechanisms may contribute to disease progression, consistent with patterns observed in other fungal infections. In rare cases of severe systemic infection, no obvious predisposing factors were identified. Such cases have been specifically attributed to infection with a particularly virulent strain of P. boydii [41], whereas another report has suggested that S. apiospermum may act as a primary pathogen in young and apparently healthy dogs [18].
It has been reported that systemic infections caused by Scedosporium species have been documented in several specific countries, but not in Nigeria or elsewhere on the African continent [11]. It was proposed that the virulence of these strains may vary across geographical regions and that the observed clinical variations could also be influenced by other factors, such as genetic differences in host susceptibility among populations from different regions. To investigate this hypothesis, the virulence of three groups of isolates originating from different geographical areas was examined using an experimental mouse infection model. Their findings revealed that the Spanish control strain exhibited greater virulence than any of the S. apiospermum strains isolated from Nigeria. Moreover, no significant differences in virulence were observed between clinical and non-clinical isolates, indicating that any strain, regardless of its source, has the potential to cause severe infections in individuals with underlying risk factors.
2.2. Diagnosis
Etiological diagnosis of scedosporiosis depends largely on the clinical manifestation of disease and typically requires a combination of clinical evaluation, hematological and biochemical analyses, imaging procedures (radiography, ultrasonography, computed tomography), biopsy, and histopathological examination. These comprehensive diagnostic approaches impose a considerable financial burden on animal owners and are usually not performed in food-producing animals due to economic constraints.
The clinical and histopathological features of scedosporiosis (as summarized in Table 1 and Table 2) closely resemble those observed in infections caused by other hyaline hyphomycetes. Histopathological examination remains a valuable tool for the diagnosis of fungal infections and for distinguishing them from non-infectious inflammatory or neoplastic diseases [29,44]. However, in tissue sections, the hyphae of S. apiospermum exhibit morphological features that closely resemble those of Aspergillus and Fusarium species, making differentiation based on histopathology alone unreliable [9,18,20].
Nevertheless, certain histopathological features have been described that may assist in differentiating Scedosporium from Aspergillus species. Aspergillus typically exhibits regular, dichotomous branching, whereas Scedosporium tends to display more irregular branching patterns and can also form terminal or intercalary chlamydospores, which may be mistaken for yeast cells [7]. The observation of oval conidia in biopsy specimens can support a presumptive identification of Scedosporium [16]. However, definitive species-level identification typically requires molecular diagnostic methods. In some early reports, the etiological diagnosis was confirmed using immunohistochemistry with fluorescein isothiocyanate (FITC)-conjugated immunoglobulins specific for P. boydii [38,41].
2.3. Microbiological Diagnosis
Fungal culture is widely regarded as the gold standard for the diagnosis of Scedosporium infections [16]. In the cases summarized in Table 1 and Table 2, S. apiospermum was isolated from affected tissues or biopsy specimens, abdominal fluid collected during surgical removal of mycetoma masses, as well as from nasal and corneal ulcer swabs. However, isolation of S. apiospermum from corneal swabs was unsuccessful in some reported cases. In such instances, PCR analysis of DNA extracted from corneal scrapings was more sensitive than culture for diagnosing ophthalmic mycoses [34].
Isolation of S. apiospermum does not require specialized media or particular cultivation conditions. The fungus grows on standard mycological media such as Sabouraud dextrose and potato dextrose agar, and it can also grow on routine bacteriological media, blood and chocolate agar. The optimal growth temperature ranges from 25 °C to 35 °C, consistent with that of most pathogenic fungi. Some strains are capable of growth at elevated temperatures of 42 °C [7], and even 45 °C [8]. In addition, S. apiospermum has demonstrated the ability to grow under anaerobic conditions [7,8,53,54].
Colonies grow rapidly and are typically woolly to cottony in texture, initially white, and becoming olive green to dark gray with maturation. On the reverse side of culture plates, colonies develop a dark gray or grayish-brown pigmentation in the center after 5–7 days, coinciding with the conidia (asexually produced spores) formation [7,18,20,54]. In documented cases, growth of S.apiospermum on blood and chocolate agar incubated at 37 °C was observed within 24 h [40] and in another report after 4 days [39]. On Sabouraud dextrose agar incubated between 25 °C and 37 °C, growth was noted after 24 h [22], 72 h [16,18] or 4 days [46]. On potato dextrose agar incubated at 35 °C, growth was noted after 24 h [45].
Under aerobic conditions, S. apiospermum spores become visible after approximately 15 days of incubation, whereas no spore formation is observed under anaerobic conditions, even after 30 days of incubation [53]. Figure 1 illustrates the macroscopic colony morphology of an S. apiospermum animal isolate.
Mycological culture combined with microscopic examination enables reliable differentiation of Scedosporium species from Aspergillus, Fusarium, and other morphologically similar fungi [9,20,25,32]. Under light microscopy, isolates typically exhibit hyaline, non-pigmented, septate hyphae with terminal conidiophores bearing single-celled, ovoid to elongate conidia [16,25]. No evidence of sexual reproduction–specifically the formation of cleistothecia–was observed even after prolonged incubation of up to 11 days, which is consistent with previous reports indicating that clinical isolates rarely develop teleomorphic structures in culture [20]. Figure 2 illustrates the microscopic morphology of an S. apiospermum animal isolate.
Based on both macroscopic and microscopic characteristics, accurate species-level identification of Scedosporium cannot be reliably achieved. Species-level identification is not routinely available in most veterinary diagnostic laboratories; therefore, submission of isolates to specialized reference centers with expertise in medical mycology is recommended [9,17,23,46].
For the identification of clinically important fungal species, many laboratories employ matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS) [2,55]. Commercial MALDI-TOF MS systems, such as the MALDI Biotyper (Bruker Daltonics, Germany), Andromas (Andromas SAS, France), and Axima SARAMIS (Shimadzu/AnagnosTec, Germany), are generally inadequate for reliably identifying Scedosporium or Lomentospora species if used with standard reference databases alone. Accurate species-level identification often requires supplementation with in-house spectral libraries [2]. In our case, the Bruker MALDI Biotyper (Bruker Daltonics GmbH, Bremen, Germany) (Identification Method: MALDI Biotyper MSP Identification Standard Method 1.1; Applied MSP Library: Filamentous Fungi) identified the isolate only to the genus level (score 2.03) [54]. Subsequent whole-genome sequencing on this isolate confirmed species-level identification as S. apiospermum [56].
PCR-based methods and nucleotide sequencing remain the current gold standard for species-level identification of Scedosporium [16,18,37,44]. For example, internal transcribed spacer (ITS) region sequencing and beta-tubulin gene analysis were employed to accurately identify the causative agent of disseminated pseudallescheriosis in a German Shepherd as P. boydii, which was distinct from another isolate identified as S. apiospermum [57]. These molecular approaches provide definitive species-level identification, which is particularly valuable when conventional culture and MALDI-TOF methods are inconclusive.
Owing to these technical limitations, most laboratories typically report isolates only as members of the Scedosporium/Pseudallescheria complex (SPCF) without specifying species. This generalization persists despite well-documented differences in pathogenicity, antifungal susceptibility, and genetic profiles among species within the complex [9].
2.4. Antifungal Susceptibility Testing
Scedosporium spp. exhibit intrinsic resistance to many antifungal agents, although susceptibility may vary significantly among strains [8,37,55]. This intrinsic and often unpredictable resistance profile represents a major determinant of therapeutic decision-making in both human and veterinary medicine. Determination of antifungal susceptibility is therefore a crucial step for therapy selection and improving clinical outcomes; however, most veterinary laboratories do not routinely perform such testing, primarily due to limited technical capacity and the absence of standardized protocols in many settings. Consequently, isolates are often sent to specialized or national reference mycology laboratories for further characterization and susceptibility testing [9,22,44,45].
In the cases summarized in Table 3, antifungal susceptibility testing was performed on only 13 S. apiospermum isolates: 11 from dogs, one from a cat [29], and one from a horse [32]. Clinical MIC breakpoints for Scedosporium spp. have not been formally established by EUCAST or CLSI [37]. Susceptibility classifications (susceptible or resistant) reflect the original authors’ interpretation. The limited number of tested isolates highlights a substantial gap in the available data regarding antifungal susceptibility patterns in veterinary cases. The results indicate that the isolates were largely resistant to amphotericin B and fluconazole, and showed susceptibility to ketoconazole and voriconazole. It has been reported that all Scedosporium species are resistant to amphotericin B, flucytosine, fluconazole, and itraconazole [2]. However, other studies have demonstrated in vitro activity of itraconazole [17,22,25,29] and fluconazole [26] against clinical S. apiospermum isolates from animals, suggesting that susceptibility is strain-dependent and emphasizing the importance of isolate-specific testing.
Voriconazole is strongly recommended as first-line treatment for Scedosporium infections in human medicine [58] and is also recommended in veterinary cases in which antifungal susceptibility testing has not been performed [34,37]. However, in vitro susceptibility results do not necessarily predict in vivo therapeutic success, and the clinical relevance of susceptibility testing remains limited [15]. In fungal infections, particularly those caused by Scedosporium, treatment failure may result not only from antifungal resistance but also from factors related to the structural and biological characteristics of the infection. These include the formation of dense granulomatous lesions surrounded by a dense, fibrotic, and sometimes calcified capsule, which can significantly impair drug penetration and reduce drug efficacy [31,45]. Recent evidence indicates that biomass formed during Scedosporium infections consists of dense hyphal networks embedded in an extracellular polymeric matrix characteristic of biofilms. Biofilm-forming Scedosporium and Lomentospora species exhibit a 2- to 1024-fold increase in resistance to azoles (e.g., voriconazole), echinocandins (e.g., caspofungin), and polyenes (e.g., amphotericin B) compared with their planktonic (free-living) counterparts [21].
Antifungal susceptibility testing of 15 S. apiospermum strains isolated from landfill-derived samples showed increased activity of azoles and amphotericin B under anaerobic conditions, as reflected by substantially lower minimum inhibitory concentration (MIC) values compared with those obtained under aerobic conditions [53]. These findings highlight the need to revise clinical breakpoints for antifungal agents, including the potential for dose reduction during prolonged treatment of infections occurring in hypoxic or anoxic tissue. The study further indicates that the facultative anaerobic capacity of S. apiospermum may contribute to its pathogenic potential by enhancing environmental persistence and facilitating cyclical transmission between hosts via environmental reservoirs such as landfills. Notably, this investigation represents the first report of differential antifungal susceptibility of pathogenic fungi under varying oxygen tensions. Furthermore, the findings indicate that antifungal resistance in S. apiospermum is not solely an intrinsic characteristic but may also be modulated by environmental factors such as oxygen availability. This underscores the need for a more nuanced understanding of antifungal susceptibility testing and supports further research aimed at optimizing therapeutic protocols and clinical breakpoints for antifungal agents in order to enhance the treatment of invasive fungal infections, particularly those developing in hypoxic tissue environments [53].
2.5. Therapy
No standardized treatment protocol has been established for S. apiospermum infections in either human or veterinary medicine [26,29]. Consequently, therapeutic decisions are based on infection site, disease severity, host immune status, and antifungal susceptibility patterns. Localized infection can often be managed successfully through complete surgical excision or debridement, combined with topical and/or systemic antifungal therapy. Early surgical intervention is considered crucial to prevent progression to more aggressive or disseminated disease [26].
Complete surgical removal of lesions in endogenous infections, such as visceral eumycetomas, is often challenging [18,43]. Sustained remission has been documented in a limited number of canine cases treated with surgery and long-term systemic antifungal therapy, including pyogranulomatous cystitis and focal peritonitis [22], urinary bladder granulomas [44], advanced intra-abdominal infection [17], and disseminated abdominal granulomas [45]. Antifungal therapy may last for several months to years [22], reflecting the chronic nature of the infection and the relative resistance of the organism to multiple antifungal agents. Long-term treatment and repeated follow-up examinations are expensive. The daily cost of voriconazole therapy has been estimated at approximately €70, rendering prolonged treatment financially impractical [17]. Disseminated infections generally carry a poor prognosis and are often fatal. In advanced cases, some owners ultimately elect euthanasia due to the unfavorable clinical outlook and the substantial financial strain associated with prolonged treatment attempts [31,41,43,46].
3. Conclusions
In veterinary medicine, S. apiospermum remains an often underrecognized etiological agent of both localized and systemic infections. These infections exhibit numerous clinical and morphological similarities to other fungal granulomatous diseases, such as aspergillosis and fusariosis, which complicates accurate diagnosis.
In the confirmed cases presented in this review, anamnesis clearly shows that affected animals were initially treated empirically with antibiotics and corticosteroids by veterinarians. While such empirical treatment—particularly with antibiotics—is a concerning practice in the context of the growing global crisis of antimicrobial resistance, it also potentially contributes to the progression of infections caused by S. apiospermum.
Laboratory isolation of the pathogen is not technically demanding and allows for reliable differentiation of Scedosporium spp. from other fungal species. However, species-level identification and antifungal susceptibility testing typically require collaboration with external laboratories specialized in mycology.
Given the increasing levels of environmental pollution, a rise in the incidence of S. apiospermum infections is expected. Consequently, there is a pressing need to increase awareness of scedosporiosis and its potential implications among veterinarians and veterinary institutions, including diagnostic laboratories, clinical settings, and field practices. Furthermore, integrating knowledge of such infections into veterinary education programs is essential to strengthening future diagnostic and therapeutic capabilities.
While recent studies emphasize molecular and genomic aspects of S. apiospermum, this review highlights its clinical relevance in animals, offering practical guidance for veterinarians and identifying gaps for future research.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bouchara J.-P. Papon N. Scedosporium apiospermum Trends Microbiol.2019271045104610.1016/j.tim.2019.07.00331378439 · doi ↗ · pubmed ↗
- 2Chen S.C. Halliday C.L. Hoenigl M. Cornely O.A. Meyer W. Scedosporium and Lomentospora infections: Contemporary microbiological tools for the diagnosis of invasive disease J. Fungi 202172310.3390/jof 701002333406673 PMC 7823285 · doi ↗ · pubmed ↗
- 3Abrantes R.A. Refojo N. Hevia A.I. Fernández J. Isla G. Córdoba S. Dávalos M.F. Lubovich S. Maldonado I. Davel G.O. Scedosporium spp. from clinical setting in Argentina, with the proposal of the new pathogenic species Scedosporium americanum J. Fungi 2021716010.3390/jof 703016033668188 PMC 7995985 · doi ↗ · pubmed ↗
- 4Bronnimann D. Garcia-Hermoso D. Dromer F. Lanternier F. French Mycoses Study Group Scedosporiosis/lomentosporiosis observational study (SOS): Clinical significance of Scedosporium species identification Med. Mycol.20215948649710.1093/mmy/myaa 08633037432 · doi ↗ · pubmed ↗
- 5Guarro J. Kantarcioglu A.S. HorréR. Rodriguez-Tudela J.L. Cuenca Estrella M. Berenguer J. de Hoog G.S. Scedosporium apiospermum: Changing clinical spectrum of a therapy-refractory opportunist Med. Mycol.20064429532710.1080/1369378060075250716772225 · doi ↗ · pubmed ↗
- 6Luplertlop N. Pseudallescheria/Scedosporium complex species: From saprobic to pathogenic fungus J. Mycol. Med.20182824925610.1016/j.mycmed.2018.02.01529567285 · doi ↗ · pubmed ↗
- 7Cortez K.J. Roilides E. Quiroz-Telles F. Meletiadis J. Antachopoulos C. Knudsen T. Buchanan W. Milanovich J. Sutton D.A. Fothergill A. Infections caused by Scedosporium spp Clin. Microbiol. Rev.20082115719710.1128/CMR.00039-0718202441 PMC 2223844 · doi ↗ · pubmed ↗
- 8Luna-Rodríguez C.E. Treviño-Rangel R.J. Montoya A.M. Becerril-García M.A. Andrade A. González G.M. Scedosporium spp.: Chronicle of an emerging pathogen Med. Univ.20192141310.24875/RMU.18000032 · doi ↗