Factors Related to the Etiology of Hallux Abducto Valgus: A Systematic Review
Marta María Moreno-Fresco, Stephen Mizzi, Pedro V. Munuera-Martínez, Priscila Távara-Vidalón

TL;DR
This review explores the causes of hallux abducto valgus, finding that it results from a mix of genetic, biomechanical, and lifestyle factors.
Contribution
The study provides a systematic review of etiological factors for hallux abducto valgus, highlighting a multifactorial model with hereditary and biomechanical components.
Findings
Genetic factors, including collagen-related genes, show strong familial aggregation in HAV development.
Biomechanical factors like first-ray hypermobility and reduced abductor hallucis muscle activity are consistently linked to HAV.
Female sex, older age, and narrow footwear are recurring risk factors for HAV.
Abstract
Background: The origin of hallux abducto valgus (HAV) is considered to be multifactorial; however, evidence regarding the factors involved in its development is scattered and often contradictory. Understanding the factors that contribute to the onset of HAV is crucial for informing both prevention and clinical management strategies. This review aims to explore the etiological factors associated with the development of HAV. Methods: A literature search was conducted in PubMed, Embase, Web of Science and Scopus. The search included observational studies that investigated etiological or risk factors related to the development of HAV. Methodological quality was assessed using the Joanna Briggs Institute (JBI) checklists, and the level of evidence was classified according to the Oxford Centre for Evidence-Based Medicine (OCEBM). Results: A total of 36 observational studies (20…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
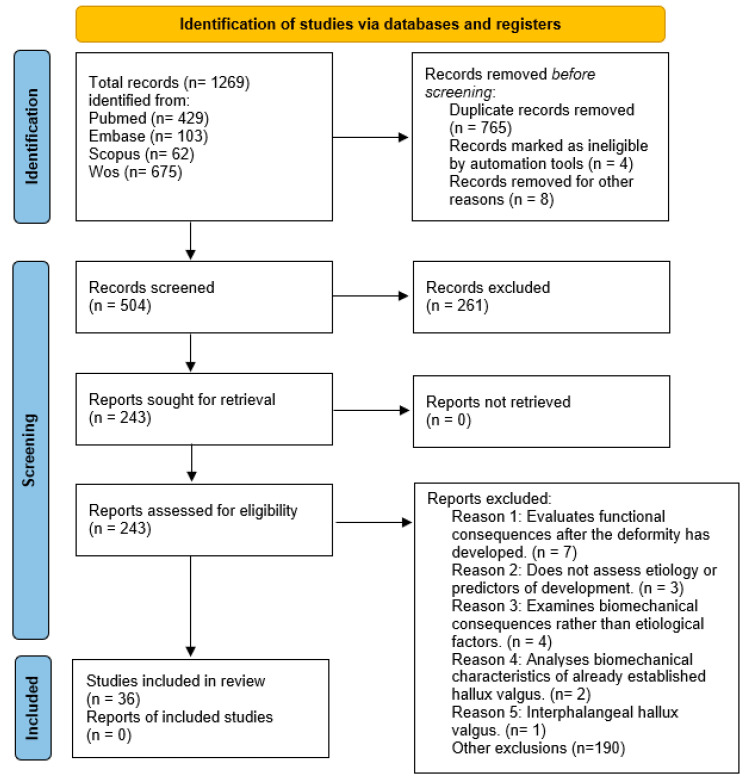 Figure 1
Figure 1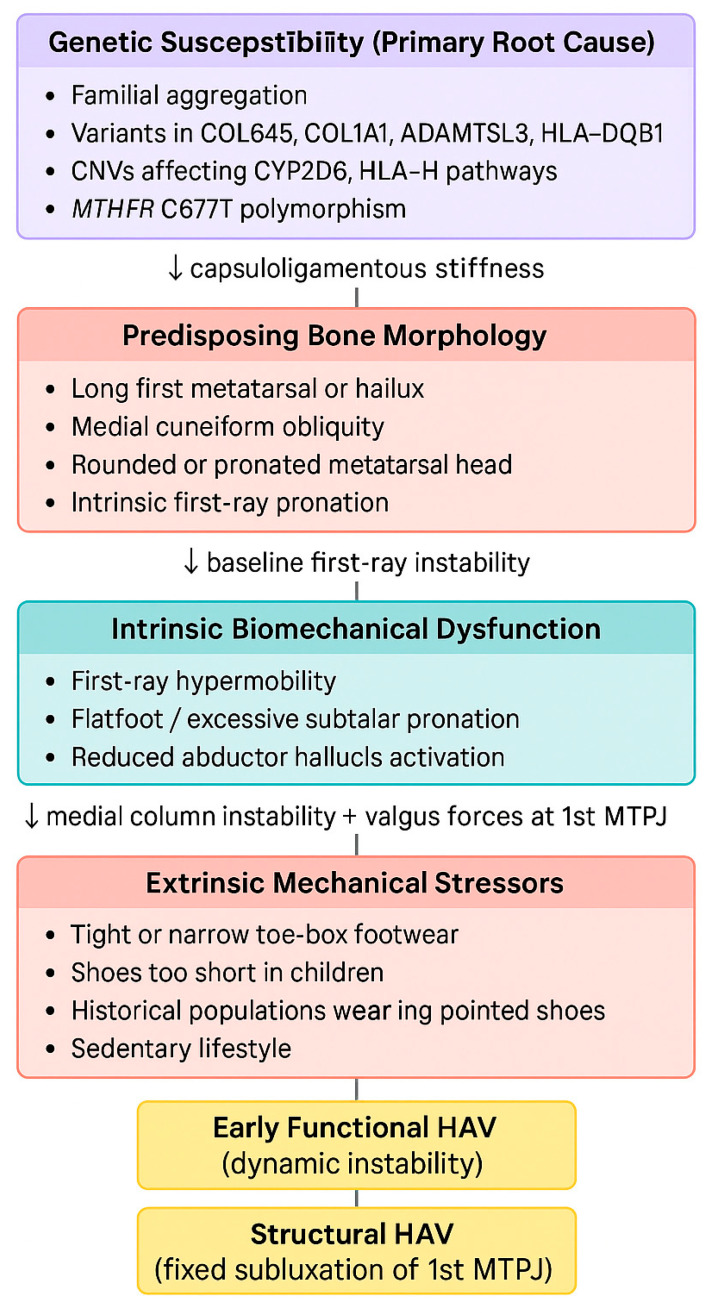 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFoot and Ankle Surgery · Tendon Structure and Treatment · Lower Extremity Biomechanics and Pathologies
1. Introduction
Hallux abducto valgus (HAV) is a foot deformity affecting the first ray, characterized by subluxation of the first metatarsophalangeal joint (1st MTPJ), accompanied by lateral deviation of the hallux and, in severe cases, plantarflexion and eversion of the great toe. The deformity also involves medial deviation of the first metatarsal with dorsiflexion and inversion, often associated with a medial exostosis at the head of the first metatarsal, commonly referred to as a bunion [1,2].
The prevalence of HAV increases with age, affecting approximately 23% of adults between 18 and 65 years and 36% of individuals over 65 years [3]. Recent epidemiological studies continue to confirm its high global prevalence, estimated at approximately 19% in the general population, with higher rates observed among women and older individuals [4]. Significant sex-related differences have also been reported, with women being 2.3 times more likely to develop HAV than men, with prevalence rates of 30% and 13%, respectively [3]. Despite its high prevalence, the exact etiology of HAV remains unclear. It is widely recognized as a multifactorial condition influenced by both intrinsic and extrinsic factors that contribute to the development and progression of the deformity [1,5].
HAV can lead to functional impairments, biomechanical alterations, and substantial pain, negatively impacting patients’ quality of life. Over the years, numerous studies have attempted to identify the factors that predispose individuals to develop HAV. Biomechanical, genetic and environmental factors have been proposed as potential contributors [6,7,8,9,10,11,12,13,14]; however, the findings have often been contradictory and sometimes inconsistent. Given the wide range of factors potentially involved in the etiology of HAV and the lack of consensus in the literature, determining which mechanisms play a key role in its development remains challenging.
A clearer understanding of the factors that contribute to the onset of HAV is essential to optimize therapeutic strategies, improve risk identification, and facilitate early intervention. In this context, the present systematic review aims to synthesize the available evidence on the etiological factors associated with HAV, thereby providing an updated scientific foundation that may serve as a reference for both clinical research and professional practice. Recent studies continue to support the multifactorial nature of HAV, highlighting the interaction between genetic, morphological, biomechanical, and environmental factors [11,12,14]. Therefore, the primary objective of this systematic review is to examine the etiological factors related to the development of HAV.
2. Materials and Methods
2.1. Protocol and Registration
This review was conducted in accordance with the PRISMA 2020 (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. The protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO; registration number: CRD420251004614) and can be accessed at the following link: https://www.crd.york.ac.uk/PROSPERO/myprospero (accessed on 7 March 2025).
2.2. Research Question
The research question guiding this review was as follows: in individuals of any age and sex, which etiological factors are associated with the development of HAV?
Population (P): Individuals of any age and sex diagnosed with HAV.Exposure (E): Etiological factors.Outcome (O): Development of HAV.Study design: Observational studies, including cross-sectional, case–control, and cohort studies (both retrospective and prospective).
2.3. Search Strategy
The search strategy was conducted in the following databases, PubMed (MEDLINE), Embase, Scopus, and Web of Science, from their inception to the most recent update (12 October 2025). The search strategy used in all databases is presented in Table 1. No restrictions were applied regarding language or publication date. The screening process was performed in three stages by two independent reviewers (MMF and PTV), and disagreements were resolved through consensus or consultation with a third reviewer (PMM): (1) removal of duplicates; (2) title and abstract screening using predefined eligibility criteria; (3) full-text assessment of potentially relevant studies to determine final inclusion.
2.4. Selection Criteria
The inclusion criteria were as follows: (1) studies involving individuals diagnosed with HAV; (2) articles reporting data on the onset, prevalence or predisposing factors of HAV; (3) studies examining risk factors associated with the development of HAV (biomechanical, genetic, footwear-related or physical activity factors); (4) observational study designs (cohort, case–control and cross-sectional studies). The exclusion criteria were: (1) studies that included other forefoot deformities different from HAV; (2) studies focused exclusively on surgical, orthotic or rehabilitative treatment, unless they provided relevant information regarding etiology or predisposing factors; (3) clinical trials, narrative reviews, letters to the editor, editorials, government reports, clinical guidelines, conference proceedings, conference abstracts, consensus statements or documents lacking methodological description; (4) studies with empirical data that were incomplete or insufficient for the analysis of etiological factors.
2.5. Methodological Quality Assessment and Risk of Bias
Methodological quality and risk of bias were assessed using the JBI critical appraisal checklists, adapted to each study design and following the guidelines of the JBI Manual for Evidence Synthesis [15]. The following tools were applied: the JBI Checklist for Analytical Cross-Sectional Studies for cross-sectional designs and the JBI Critical Appraisal Checklist for Case–Control Studies for case–control designs [16]. Although some of the included studies employed descriptive cross-sectional designs, they were evaluated using the analytical cross-sectional checklist, as the JBI Manual does not provide a specific tool for descriptive studies within reviews addressing etiology and risk. This decision was made to ensure methodological consistency and facilitate comparability across scores. Items related to confounder control or statistical analysis were considered not applicable for purely descriptive studies.
Each item was scored as 1 (yes), 0.5 (unclear), or 0 (no). Total scores, quality levels (low, moderate or high), and the percentage (%) of bias were calculated (Table 2 and Table 3). Studies were classified as having low risk of bias (≥75% of total points), moderate risk (50–74%) or high risk (<50%). This approach allows simultaneous assessment of methodological rigor and key sources of bias, including sample representativeness, validity of exposure and outcome measurements, identification of confounding factors, and adequacy of statistical analysis.
The level of evidence for each study was determined according to the OCEBM, 2011 classification, which categorizes research designs into five levels (1–5) based on their ability to establish causal relationships in etiology and risk research [50].
Two reviewers independently performed the quality assessment in duplicate, resolving discrepancies through consensus or consultation with a third reviewer.
3. Results
3.1. Study Selection
The initial search identified a total of 1269 articles. After applying the predefined inclusion and exclusion criteria and evaluating the study data, 36 studies were finally selected for analysis (Figure 1).
3.2. Study Characteristics
The characteristics of the included studies are presented in Table 4. A total of 20 cross-sectional studies [12,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,51] and 16 case–control studies [9,14,36,37,38,39,40,41,42,43,44,45,46,47,48,49] were included. The overall sample comprised 14,500 participants, of whom 9085 (62.7%) were women and 5415 (37.3%) were men. The mean age of the total population was 47.3 ± 15.2 years, ranging from pediatric to older adult populations. Most studies reported a predominance of female participants [12,14,20,21,23,24,30,38,39,43,44,46,51]. Four studies were conducted exclusively in women [20,31,41,42], while one study involved only young male participants [37]. The studies were grouped thematically and are discussed in the following sub-sections based on key contributing factors associated with the development of HAV.
3.2.1. Genetic Factors and Family History
Nine studies examined the genetic contribution and the presence of family history in the development of HAV [14,23,31,34,35,41,46,49,51]. Two of these employed observational family-based cross-sectional designs [23,34], whereas seven used case–control designs involving genetic or clinical assessment [14,31,35,41,46,49,51].
The study by Hardy and Clapham [49] was the first to document family history as part of the clinical evaluation, reporting a high proportion of relatives with HAV among affected individuals, although no genetic analyses were performed. This early clinical observation was later confirmed by more systematic investigations. Piqué-Vidal et al. [34] and Zhou et al. [23] assessed familial aggregation of HAV; the former used structured questionnaires with clinical and radiographic confirmation, while the latter applied whole-exome sequencing to identify copy number variations (CNVs). Both studies reported a high prevalence of HAV in first-degree relatives, with Zhou et al. [23] identifying structural genetic alterations specific to affected individuals.
Three studies [31,46,51] recorded family history through standardized clinical interviews, confirming a higher frequency of familial involvement among participants with HAV. In Nery et al. [46], this association was more pronounced in men with greater clinical severity, whereas Okuda et al. [31] found a significant association with affected mothers and/or grandmothers in young women.
Tao et al. [41] investigated genetic susceptibility by genotyping polymorphisms of the vitamin D receptor gene (VDR), identifying a higher prevalence of the TaqI-C and BsmI-A alleles in the HAV group. In the study by Jia et al. [14], whole-exome sequencing was used to detect genetic variants associated with HAV. The authors analyzed more than 18,000 genes and identified pathogenic mutations in COL6A5, COL1A1, HLA-DQB1 and ADAMTSL3. More recently, Kuo et al. [35] conducted a targeted genetic analysis using PCR, demonstrating that the TT genotype of the MTHFR C677T polymorphism is significantly associated with an increased risk of developing HAV, whereas A1298C showed no association.
Two studies [46,51] performed sex-stratified analyses to explore sex-related differences in familial aggregation, and one study focused on a juvenile population, allowing for the examination of hereditary influence at early developmental stages [31].
3.2.2. First-Ray Bone Morphology and Multiplanar Deformity
Nine studies examined the bone morphology of the first ray and the multiplanar component of HAV using imaging techniques in adult populations [24,27,38,39,42,43,47,48,49].
Of these, seven were case–control studies [38,39,42,43,47,48,49] primarily assessing morphometric parameters through weightbearing radiographs [43,47,48,49] or computed tomography (CT/WBCT) [38,39,42]. The variables analyzed included the intermetatarsal angle (IMA), relative first metatarsal length, geometric asymmetry of the proximal phalanx (medial–lateral diameter difference), as well as frontal-plane rotation of the first ray and the hallux. All studies reported significant between-group differences, with higher angular deviation, increased osseous pronation, or greater structural asymmetry in individuals with HAV.
Two studies employed a cross-sectional design [24,27]. Bu et al. [24] analyzed the morphology of the medial cuneiform using digital radiography and identified angular variations in the Metatarsocuneiform Angle (MCA), Metatarsus Adductus Angle (MAA), and Proximal Metatarsal Articular Angle (PMAA) associated with HAV. Manceron et al. [27] used dynamic ultrasound to quantify the multiplanar mobility of the first ray and the first tarsometatarsal joint (1st TMTJ) exclusively in HAV feet, observing greater displacement in cases with more advanced deformity.
3.2.3. Intrinsic Biomechanical Factors
Eight studies examined intrinsic biomechanical factors associated with the development of HAV, grouped into first-ray hypermobility, flatfoot/pronation, and intrinsic foot muscle function [9,17,18,27,37,40,42,51]. Four of these were case–control studies [9,37,40,42], three were analytical cross-sectional studies [17,18,51], and one was a descriptive cross-sectional study [27].
With regard to first-ray hypermobility, two studies evaluated its multiplanar motion [27,42]. Kimura et al. [42] compared individuals with HAV and controls using WBCT, identifying significantly greater first-ray mobility in dorsiflexion, inversion and adduction in the HAV group. Conversely, Manceron et al. [27] analyzed only HAV-affected feet using dynamic ultrasound, observing increased motion at the 1st TMTJ in cases presenting with more advanced deformities.
Four studies investigated parameters related to rearfoot alignment and arch structure [17,18,37,51]. Atbaşı et al. [37] analyzed weightbearing radiographs in young adult males and observed a reduced calcaneal pitch and increased lateral talocalcaneal angle in the HAV group. Choi et al. [18] employed an artificial intelligence-based classification system to assess flatfoot severity using radiographs and found a significant association between flatfoot and increased HAV severity. Nguyen et al. [51], in an older general population, used MatScan baropodometry and reported that flatfoot was associated with a higher likelihood of HAV in men, although this association was not observed in women.
Two studies investigated the activity of the abductor hallucis (AbdH) muscle using surface electromyography [9,40]. Arinci Incel et al. [9] observed significantly lower AbdH activity in individuals with HAV during voluntary hallux abduction tasks. Similarly, Mortka et al. [40] reported reduced motor unit action potential amplitude in the HAV group, although this reduction did not correlate with radiographic severity.
3.2.4. Anthropometric and Demographic Factors
Six studies evaluated the influence of anthropometric and demographic characteristics on the development of HAV [12,20,21,30,46,51]. Five of these were analytical cross-sectional studies [12,20,21,30,51], and one employed a case–control design [46].
Three studies [21,30,51] included sex- and age-stratified analyses. Nguyen et al. [51] reported a higher prevalence of HAV in women than in men and found sex-specific associations when analyzing BMI and flatfoot. Nishimura et al. [30] also identified a higher frequency of HAV in older women, with a mean age of 75.5 ± 6.4 years. Nakao et al. [21], using multivariable analysis with feature selection (SVM-RFE), identified age, female sex and body weight as key variables distinguishing participants with HAV from those without.
Two studies analyzed foot morphological variables and their association with HAV [12,20]. Martín-Casado et al. [12] assessed foot length and width, heel width and arch height using a 3D scanner, reporting that greater foot length and wider heel width were associated with HAV. Liu et al. [20] examined adolescent athletes and found higher prevalence and severity in females, as well as an increased risk associated with greater weekly training load.
Finally, in the study by Nery et al. [46], which included adult participants of both sexes, a more deviated first ray and greater HAV severity were more frequent in men, despite the overall lower prevalence in this group.
3.2.5. Lower-Limb Alignment and Biomechanics
Two analytical cross-sectional studies evaluated the influence of lower-limb characteristics on the development of HAV [36,45]. In the study by O’Reilly et al. [36], ankle dorsiflexion and gastrocnemius contracture were measured using the Silfverskiöld test, revealing reduced dorsiflexion and a higher prevalence of gastrocnemius tightness in individuals with HAV compared with controls. Steinberg et al. [45] assessed proximal alignment using goniometric measurements (Q-angle, tibiofemoral angle, rearfoot angle) and recorded generalized hypermobility through the Beighton Score, a validated nine-item scale used to quantify joint laxity. They found significantly higher values among participants with HAV. Both studies demonstrated proximal biomechanical differences between individuals with and without HAV.
3.2.6. Extrinsic, Metabolic and Lifestyle Factors
Six analytical cross-sectional studies evaluated the relationship between footwear characteristics and hallux valgus angles across different developmental stages [25,26,28,29,32,44].
In pediatric populations, Klein et al. [32] used 3D scanning combined with a device specifically designed to measure internal shoe length, reporting higher hallux valgus angle (HVA) values in children whose footwear provided insufficient toe allowance. González-Elena et al. [28] combined direct anthropometric foot and shoe measurements with weightbearing podoscopy, identifying significant correlations between reduced shoe allowance and higher HVA within age- and sex-specific subgroups. Puszczalowska-Lizis et al. [29] used podoscopy and digital measurements of shoe “functional excess,” finding significantly greater HVA values in children wearing shoes that were too short. Similarly, Kinz et al. [26] digitally evaluated internal shoe length and HVA and observed a high prevalence of short footwear and higher HVA values in such cases, while habitual barefoot walking was associated with smaller angles.
In an adult population, Menz et al. [44] used a validated retrospective questionnaire featuring line drawings of forefoot shapes. Their findings indicated a significantly higher likelihood of HAV among participants who had worn narrow toe boxes during their 20s and 30s. Additionally, Dittmar et al. [25], through physical anthropology of skeletal remains, found a greater prevalence of HAV during historical periods associated with tight, pointed footwear compared to barefoot populations.
Finally, Liu et al. [19] investigated the relationship between sedentary behavior and HAV risk using a genetics-based statistical approach known as Mendelian Randomization, drawing data from large European population cohorts. Sedentary behavior was quantified using leisure screen time. The authors found that higher screen time was significantly associated with an increased risk of developing HAV.
3.3. Risk of Bias in the Included Studies
The methodological quality of the 36 included studies was generally adequate. According to the scores obtained using the JBI tools, 31 studies (87.1%) demonstrated a low risk of bias, whereas five studies (12.9%) showed a moderate risk, and none were classified as having a high risk of bias.
By study design, cross-sectional studies showed a predominantly low risk of bias (17/18; 94.4%), with only one study rated as moderate. In contrast, case–control studies presented 10 out of 13 (76.9%) with low risk and three out of 13 (23.1%) with moderate risk.
The items with the highest risk of bias were related to the lack of control for confounding factors, insufficient reporting on the reliability and validity of measurements, and the use of non-probabilistic sampling methods. In contrast, the best-performing items were the clarity of inclusion criteria, the adequate measurement of exposures and outcomes, and the use of appropriate statistical analyses in most analytical studies. The detailed scoring for each study is presented in Table 2.
4. Discussion
The primary objective of this systematic review was to examine the etiological factors associated with the development of HAV. The findings are associated with the current understanding of HAV as a complex and multifactorial deformity influenced by the interaction of several intrinsic and extrinsic factors. To our knowledge, this work represents the first systematic review to comprehensively synthesize evidence across all these domains, integrating genetic, morphological, biomechanical, anthropometric, and extrinsic factors within a single etiological framework. This integrative perspective provides a clinically oriented synthesis of the etiological factors involved in HAV and may support more individualized preventive and therapeutic strategies.
4.1. Genetic Factors and Family History
The results suggest that genetic inheritance may represent one of the principal etiological factors associated with HAV. Classic studies by Hardy and Clapham [49] and Piqué-Vidal et al. [34] already demonstrated strong familial aggregation, with a prevalence of up to 90% in first-degree relatives. Subsequent research [31,46,51] corroborated this association, showing that a positive family history significantly increases the likelihood of developing HAV.
Recent molecular evidence expands this knowledge. Jia et al. [14], through whole-exome sequencing, identified variants in genes related to collagen synthesis and the extracellular matrix (COL6A5, COL1A1), immune modulation (HLA-DQB1) and connective tissue organization (ADAMTSL3), suggesting a genetic susceptibility that affects the capsuloligamentous stability of the first ray. These findings indicate that HAV may be understood, at least in part, as a disorder linked to connective tissue integrity and extracellular matrix signaling pathways, rather than solely as an acquired forefoot deformity.
Tao et al. [41] reported higher frequencies of the TaqI-C and BsmI-A alleles of the VDR in individuals with HAV, reinforcing the hypothesis of a multifactorial genetic susceptibility modulated by hormonal and metabolic factors. This line of evidence was further expanded by Zhou et al. [23], who identified CNVs in genes related to the cytochrome P450 pathway (CYP2D6, CYP2D7) as well as in immunoregulatory genes (HLA-H, HCG4B), suggesting that HAV may have an immunometabolic basis affecting cartilage homeostasis and local inflammatory responses.
The most recent study, conducted by Kuo et al. [35], provides additional evidence by identifying that individuals carrying the TT genotype of the MTHFR C677T polymorphism have a significantly increased risk of developing HAV. This finding suggests a potential link between folate metabolism, DNA methylation and individual susceptibility to the deformity, introducing a biologically plausible pathway that aligns with the previously described genetic complexity.
Consistent with the clinical observations by Nery et al. [46] and Okuda et al. [31], these genetic alterations appear to manifest differently between men and women and may exert their influence from early ages. Overall, the current genetic evidence supports the view that HAV has a complex hereditary basis, with contributions from both connective tissue structure and immunometabolic mechanisms.
4.2. Bone Morphology and the Multiplanar Component
The literature consistently describes HAV as a multiplanar deformity of the first ray. Imaging studies consistently indicate that structural and rotational changes in the first ray are associated with HAV [24,27,38,39,42,43,48].
Cruz et al. [38], using WBCT, quantified an average first-ray pronation of 15.3° in the HAV group versus 3.4° in controls, and observed significant medial rotation of the hallux, confirming the three-dimensional nature of the deformity. Kimura et al. [42] reported a similar pattern, additionally describing dorsal and medial translation of the first metatarsal. Bu et al. [24] highlighted the involvement of the medial cuneiform, identifying angular variations (MCA, PMAA, MAA) that predispose to medial displacement of the first metatarsal.
Similarly, Mancuso et al. [48] and Munuera et al. [47] provided evidence regarding the role of longitudinal bone morphology, showing that individuals with HAV present a longer first metatarsal than controls. Mancuso et al. [48] further reported that this increased length is often accompanied by a more rounded metatarsal head. Later, Munuera et al. [47] confirmed that, in early stages, individuals with HAV also exhibit a longer hallux. These features, identifiable in the early stages of the deformity, may constitute key predisposing traits that precede the multiplanar deviation of the first ray, reinforcing the notion that certain anatomical configurations may predispose to the deformity independently of functional biomechanical mechanisms.
Manceron et al. [27], through dynamic ultrasound, observed greater multiplanar displacement of the 1st TMTJ in more severe cases, supporting the view that first-ray instability is not only structural but also functional.
Collectively, these findings suggest that the bone morphology of the first metatarsal and medial cuneiform may serve as a primary anatomical predisposition for the development of HAV, with secondary biomechanical factors influencing the severity and progression of the deformity.
4.3. Intrinsic Biomechanical Factors
Intrinsic biomechanical alterations appear to play a relevant role in the development and progression of HAV, particularly those affecting first-ray stability, foot pronation, and intrinsic muscle function.
First-ray hypermobility was identified as a key element [27,42]. Kimura et al. [42] reported significantly greater dorsal and medial displacement of the first metatarsal in individuals with HAV, while Manceron et al. [27] confirmed through dynamic ultrasound that mobility of the 1st TMTJ progressively increased with greater deformity severity. Chen et al. [17] further validated this functional impairment using dynamic biomechanical assessment and baropodometry, demonstrating a redistribution of plantar load toward the first metatarsal head and an increase in medial pressure mechanisms that perpetuate the progressive displacement of the hallux and the first ray.
Regarding rearfoot alignment and arch structure, Atbaşı et al. [37] found reduced calcaneal pitch and increased lateral talocalcaneal angle values in young men with HAV, indicative of flatfoot. Choi et al. [18] used artificial intelligence algorithms applied to radiographs to quantify flatfoot severity, identifying a significant association with the presence of HAV. In older adults, Nguyen et al. [51] demonstrated that flatfoot was associated with a higher likelihood of HAV in men but not in women, suggesting sex-specific biomechanical patterns.
Additionally, electromyographic studies by Arinci Incel et al. [9] and Mortka et al. [40] revealed significantly reduced activity of the abductor hallucis muscle, an important stabilizer of the medial column reinforcing the role of intrinsic musculature in the progression of the deformity.
Together, these findings support the notion that HAV is associated with medial instability, excessive pronatory loading and neuromuscular deficits, which contribute to the progressive displacement of the hallux and the first ray.
4.4. Anthropometric and Demographic Factors
Female sex and older age are the primary demographic factors associated with HAV [21,22,30,51]. Jung et al. [22] found that being female, over the age of 50, and having a low medial longitudinal arch significantly increase the likelihood of developing HAV, highlighting the interplay between hormonal, structural, and mechanical influences.
Liu et al. [20] examined adolescent athletes and found a higher prevalence and severity of HAV in females, as well as a positive relationship between weekly training load and the deformity. This suggests that repetitive stress on a vulnerable forefoot may precipitate HAV at an early age.
From an anthropometric perspective, Martín-Casado et al. [12] identified associations between greater foot length, wider heel width, and reduced arch height with the presence of HAV. Additionally, Munuera et al. [47] reported that individuals with early-stage HAV exhibited a proportionally longer first metatarsal and hallux, suggesting that particular longitudinal forefoot configurations may form part of a presuppositional anthropometric profile.
Collectively, these findings suggest an influence of morphological phenotype and load distribution patterns on susceptibility to HAV.
4.5. Lower-Limb Alignment and Biomechanics
The influence of lower-limb alignment and global postural patterns also appear to contribute significantly to the onset and progression of HAV. The limitations in ankle dorsiflexion and gastrocnemius tightness described by O’Reilly et al. [36] may promote a distal compensatory pattern characterized by increased subtalar pronation and higher medial loading during stance phase conditions that may amplify the deviating forces acting on the first ray.
Similarly, the proximal alignment alterations and generalized hypermobility observed by Steinberg et al. [45], including an increased Q-angle and greater ligamentous laxity, may compromise the stability of the tarsometatarsal complex, facilitating progressive medial deviation of the first metatarsal.
These findings indicate that specific patterns of proximal alignment and mobility may act as biomechanical modulators that favor or accelerate the manifestation of HAV in predisposed individuals.
4.6. Extrinsic, Metabolic, and Lifestyle Factors
The use of narrow or ill-fitting footwear remains one of the most frequently cited extrinsic factors associated with HAV, particularly during childhood and early adulthood. In children, Klein et al. [32], Puszczalowska-Lizis et al. [29], González-Elena et al. [28] (2021), and Kinz et al. [26] demonstrated a significant correlation between wearing small or narrow shoes and higher HVA values, suggesting that forefoot compression during growth influences hallux alignment.
In adults, Menz et al. [44] found that wearing narrow toe-box footwear between the ages of 20 and 39 doubled the risk of developing HAV (OR = 2.7; 95% CI: 1.46–5.00). From a historical perspective, Dittmar et al. [25] demonstrated through osteological analyses that the prevalence of HAV was higher in populations that wore tight or pointed footwear compared with those that went barefoot.
Collectively, these findings support the notion that footwear acts as a modulating factor capable of precipitating or exacerbating an underlying anatomical predisposition rather than serving as a primary cause of HAV.
More recently, Liu et al. [19] established a causal relationship between sedentary behavior and HAV development, partially mediated by low serum calcium levels. This suggests that reduced physical activity and metabolic imbalances may affect muscle function and bone integrity, indirectly contributing to the onset or progression of HAV. Furthermore, the authors propose that lifestyle modifications and the optimization of mineral metabolism should be considered in future preventive and rehabilitative strategies.
Genetic variations may produce a more unstable articular architecture or an altered inflammatory response; on this substrate, excessive pronation, hypermobility, and restrictive footwear act as mechanical triggers. This model explains the gradual progression of HAV from functional instability to structural deformity consistent with the theory of progressive medial instability described by Coughlin et al. [33] and Okuda et al. [31].
A conceptual model of this etiologic pathway is presented in Figure 2.
From a clinical perspective, understanding the multifactorial etiological model of HAV may support a more precise and personalized therapeutic approach. The identification of risk profiles based on the interaction between genetic predisposition, bone morphology, biomechanical patterns, and extrinsic factors opens the door to early preventive strategies and to treatment selection directed at the predominant mechanisms in each patient. This integrative perspective may contribute to a more individualized form of medicine, aimed not only at correcting the deformity, but also at modifying the factors that condition its onset and progression.
4.7. Limitations
This review presents several limitations that must be considered when interpreting the findings. Although most studies demonstrated a low risk of bias according to the JBI tool, the overall evidence is constrained by methodological heterogeneity, the predominantly cross-sectional design of many studies, and the limited inclusion of confounding variables. Most included studies were cross-sectional or case–control, which allow the identification of associations but do not establish causality or determine the temporal sequence between exposure and HAV onset. The lack of longitudinal or cohort studies therefore represents the main limitation of this review. Additionally, some studies used small samples or highly specific populations, which may restrict the generalizability of the findings.
In addition, although most studies showed a low risk of bias according to the JBI assessment, the overall level of evidence remains limited due to the predominance of observational designs. Consequently, the current evidence does not allow for the establishment of strong clinical recommendations or the development of robust clinical guidelines, highlighting the need for well-designed longitudinal and prospective studies.
5. Conclusions
HAV is a multifactorial deformity associated with the interaction between genetic susceptibility, predisposing bony morphology, biomechanical dysfunction, and environmental factors. Current evidence supports a dynamic and three-dimensional etiological model in which intrinsic factors determine structural vulnerability, while extrinsic factors act as triggers. Understanding this interaction is essential for developing individualized preventive and therapeutic strategies focused on functional correction and early detection in predisposed individuals. This integrative etiological framework provides a conceptual basis for future longitudinal research and improved patient-specific risk assessment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Munuera-Martínez P.V. El Primer Radio: Biomecánica y Ortopodología 2nd ed.Exa Editores SL Santander, Spain 2012978-84-616-0833-1
- 2Giannestras N.J. Hallux Valgus y Hallux Rigidus Trastornos del Pie Salvat Editores SA Barcelona, Spain 1979
- 3Nix S. Smith M. Vicenzino B. Prevalence of Hallux Valgus in the General Population: A Systematic Review and Meta-Analysis J. Foot Ankle Res.201032110.1186/1757-1146-3-2120868524 PMC 2955707 · doi ↗ · pubmed ↗
- 4Cai Y. Song Y. He M. He W. Zhong X. Wen H. Wei Q. Global Prevalence and Incidence of Hallux Valgus: A Systematic Review and Meta-Analysis J. Foot Ankle Res.2023166310.1186/s 13047-023-00661-937726760 PMC 10510234 · doi ↗ · pubmed ↗
- 5Glasoe W.M. Nuckley D.J. Ludewig P.M. Hallux Valgus and the First Metatarsal Arch Segment: A Theoretical Biomechanical Perspective Phys. Ther.20109011012010.2522/ptj.2008029819926679 · doi ↗ · pubmed ↗
- 6Wong D.W.-C. Wang Y. Chen T.L.-W. Yan F. Peng Y. Tan Q. Ni M. Leung A.K.-L. Zhang M. Finite Element Analysis of Generalized Ligament Laxity on the Deterioration of Hallux Valgus Deformity (Bunion)Front. Bioeng. Biotechnol.2020857119210.3389/fbioe.2020.57119233015022 PMC 7505935 · doi ↗ · pubmed ↗
- 7Uchiyama E. Kitaoka H. Luo Z. Grande J. Kura H. An K. Pathomechanics of Hallux Valgus: Biomechanical and Immunohistochemical Study Foot Ankle Int.20052673273810.1177/10711007050260091116174504 · doi ↗ · pubmed ↗
- 8Castanov V. Vienneau M. Arakawa T. Hassan S. Agur A. Tyczynski D. Three-Dimensional Architecture of the Great Toe Muscles: Functional Implications in Hallux Valgus Anatomy 202014778510.2399/ana.20.779018 · doi ↗