Kinesiophobia and Psychological Readiness of Return to Sport in High-Performance Judokas After an Injury: A Cross-Sectional Study
Ulises Puchalt-Muñoz, Mireia Yeste-Fabregat, Helio Carratalá-Bellod, Marta Martínez-Soler, Rómulo J. González-García, Juan Vicente-Mampel

TL;DR
This study explores how psychological factors like fear of movement and readiness to return to sport vary among injured high-performance judokas.
Contribution
The study identifies three distinct psychological profiles related to injury recovery and return to sport in judokas.
Findings
Three psychological profiles were identified based on kinesiophobia and self-perceived readiness to return to sport.
One profile showed high kinesiophobia and low readiness, with longer recovery times.
Another profile showed low fear and readiness, with younger athletes and shorter recovery times.
Abstract
Background and Objectives: Judo is an Olympic contact sport with a high risk of injury owing to its physical, technical, and competitive demands. The role of psychological factors in recovery and Return to Sport (RTS), such as kinesiophobia and self-perception, is key in the injury process. These factors influence both the success and timing of return and are affected by variables such as locus of control, previous experience, and contextual factors. This study sought to analyse the relationship between sociodemographic, clinical, sports, and psychological variables with kinesiophobia and self-perception of RTS to identify psychological profiles. Materials and Methods: A cross-sectional observational study was conducted at the Centro de Alto Rendimiento de Judo (CEAR) in Valencia, Spain; involving 51 high-performance judokas (mean age 23.0 ± 3.8 years) competing at national or…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
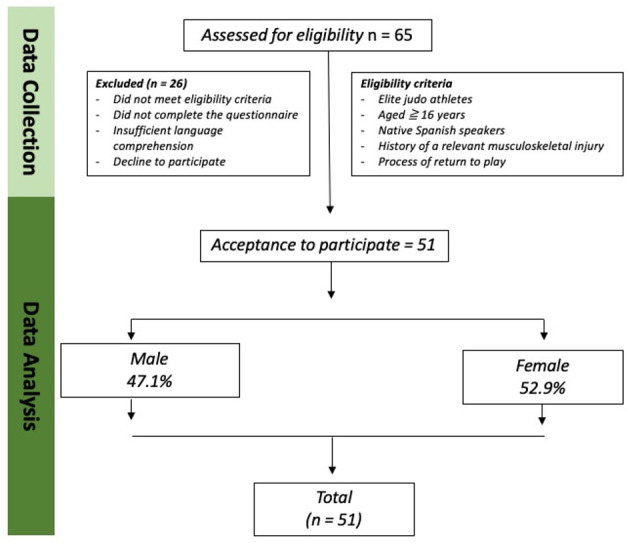 Figure 1
Figure 1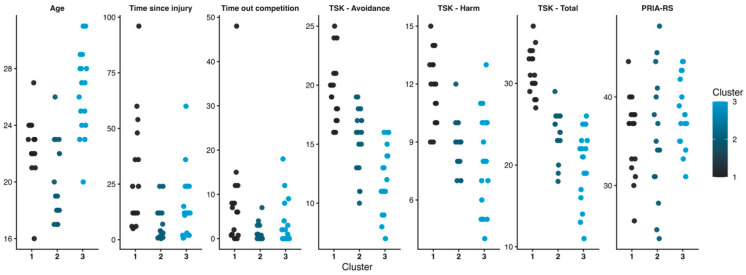 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSport Psychology and Performance · Sports injuries and prevention · Sports Performance and Training
1. Introduction
Judo is an Olympic combat sport combining standing and groundwork techniques, requiring physical capacities such as maximal strength, endurance, power, flexibility, and aerobic and anaerobic conditioning [1,2,3], along with complex technical and tactical skills [4,5]. Its dynamic, high-contact nature leads to a significant injury risk, comparable to or higher than in team sports [6,7], with reported incidence ranging from 11 to 12% in Olympic competitions [8] to 1.18 injuries per athlete per year [9]. Most injuries are mild, though 24.4% require ≥8 treatment days [6], with the knee and shoulder being most affected [8,10]. Heavier female athletes often sustain more severe injuries, while lightweight athletes experience milder injuries, a pattern possibly linked to Rapid Weight Loss (RWL) practices [6], which affect up to 96% of athletes [11] and may cause dehydration, performance decline, and psychological effects such as tension, fatigue, irritability, sleep disturbances, and disordered eating [12]. Early RWL may predispose athletes to chronic stress, emotional dysregulation, and eating disorders [11].
Judo injuries affect not only athletes’ physical well-being but also have a significant psychological and social impact [13,14]. The return-to-sport process involves multiple physical, psychological, and contextual factors, such as competition demands, environmental conditions, or external pressure; making it a difficult and highly relevant decision [15]. Kinesiophobia is a common post-injury response, initially expressed as fear of movement leading to avoidance and, near the RTS phase, as fear of reinjury [16,17]. This fear–avoidance cycle promotes disuse and muscle inhibition, reinforcing the perception of disability and ultimately impairing physical function and self-confidence [18]. Athletes who are not psychologically ready to RTS display stronger fear–avoidance behaviours and adopt protective or hypervigilant attitudes, which can negatively affect performance [19]. In addition, returning before adequate psychological readiness increases fear, anxiety, and performance decline [19], and higher fear–avoidance levels are associated with poorer functional outcomes [20].
Therefore, addressing fear of movement during rehabilitation is essential. Ardern et al. emphasized that factors such as motivation, confidence, and the absence of fear are associated with a faster and more successful return [21]. Moreover, athletes’ self-perceived competence has been shown to directly influence RTS outcomes, as believing in one’s ability to meet performance demands is crucial for a confident and sustainable return to competition [22]. In judo, athletes’ self-perceived readiness plays decisive roles in Return to Sport (RTS) outcomes. For instance, recent research in judo athletes reported that 55.9% returned to sport after injury, whereas 44.1% did not resume sport participation [23]. Judokas who successfully return to training and competition report significantly higher levels of psychological readiness, and self-perceived psychological status has been identified as a significant predictor of RTS, even after accounting for clinical and injury-related factors [23]. Recent evidence highlights the clinical relevance of assessing psychological readiness during the RTS process. A recent systematic review reported that self-reported measures of psychological readiness are associated with return-to-sport outcomes, reinjury risk, and post-return performance and emphasised the value of multidimensional assessments integrating cognitive, emotional, and behavioural components. These findings support the use of comprehensive self-reported instruments to evaluate psychological readiness in injured athletes [24].
Several psychological factors influence kinesiophobia and self-perceived readiness to return to sport (RTS). Locus of control, or the extent to which individuals perceive outcomes as determined by their own actions (internal) versus external factors such as luck, affects recovery: an internal locus promotes self-regulation and responsibility, while an external locus is linked to greater vulnerability [25,26]. Identification with other injured athletes can either support injury prevention or increase fear, avoidance, and negative self-perception [27,28]. Fear of reinjury and kinesiophobia can delay rehabilitation and reduce the likelihood of returning to pre-injury performance, with the intensity of these responses varying according to injury severity and characteristics. Despite growing recognition of the psychological dimension of injury, research on high-performance judo remains limited, with most studies focusing on physical factors. Understanding the relationship between kinesiophobia and psychological readiness may inform more effective and safer rehabilitation strategies. This study aimed to analyse sociodemographic, clinical, and psychological determinants of kinesiophobia and self-perceived readiness in injured competitive judokas, while also reporting injury incidence and characteristics and identifying psychological profiles associated with RTS. We hypothesised that higher kinesiophobia would be associated with longer recovery times and lower perceived readiness in high-performance judokas.
2. Materials and Methods
2.1. Study Design
A cross-sectional, descriptive, quantitative study was conducted to analyse the presence of psychological variables influencing high-performance judokas during the injury process. This study was approved by the Ethics Committee of the Catholic University of Valencia (reference number: UCV/2022-2023/082). All participants voluntarily and anonymously agreed to participate by providing written or electronic informed consent prior to participation, in accordance with the ethical principles of the Declaration of Helsinki [29]. The trial adhered to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines in both its design and the progression of participants [30].
2.2. Participants and Settings
The study included 51 high-performance judokas from the Centro de Alto Rendimiento de Judo (CEAR) of Valencia, Spain, all of whom had participated in national or/and international competitions. Recruitment and data collection took place on-site at the CEAR facilities in April 2025. All participants were informed of the data collection procedures. This research was conducted within the framework of a project led and supervised by the UCV. The inclusion criteria were as follows: (i) active male and female high-performance judokas (≥16 years old); (ii) Spanish-speaking athletes; (iii) having suffered a relevant musculoskeletal injury during judo practice; (iv) currently out of competition or in the process of returning to training or competition (RTS); and (v) voluntary acceptance of informed consent. The exclusion criteria were as follows: (i) incomplete questionnaires; (ii) chronic sequelae that had previously prevented the athlete from continuing professional sports practice; (iii) current pain intensity ≥ 4 on the Visual Analogue Scale (VAS); and (iv) time since injury <2 weeks at the time of assessment.
2.3. Sample Size
The sample size was considered appropriate for a cross-sectional descriptive and analytical study in sports psychology and injury perception, given the exploratory nature of the research and limited accessibility of elite athletic populations. Comparable sample sizes have been reported in previous cross-sectional studies, including those by Borsati et al., who examined exercise perception in samples of approximately 50 participants, and Khalil et al., who identified robust clinical and demographic associations in a cohort of 30 participants who underwent meniscal procedures [31,32]. Participants were recruited through a non-probabilistic convenience sampling strategy, commonly used in high-performance athletes due to their limited accessibility. The sample consisted exclusively of national and international-level competitors, enhancing the specificity and contextual relevance of the findings. No a priori sample size calculation was performed due to the exploratory nature of the study and the limited accessibility of elite athletic populations.
2.4. Measurement Variable
Data were collected at a single time point without follow-up or therapeutic intervention. Participants completed an online self-administered questionnaire under supervision to ensure consistency and high data quality. The questionnaire included sociodemographic and clinical–sport variables and incorporated two validated instruments to assess psychological variables.
2.4.1. Sociodemographic and Clinical-Sport Variables
Sex and age were sociodemographic variables. The clinical and sports variables included competitive weight category, according to the International Judo Federation (IJF), injury type (ligament, muscle, fracture, contusion, or dislocation), injury location (by anatomical region), time since injury onset (in months), and time out of competition (in months).
2.4.2. Tampa Scale for Kinesiophobia: 11 Items Version (TSK-11)
Fear of movement was assessed using the TSK self-administered questionnaire. The instrument consists of 11 items, each rated on a 4-point Likert scale ranging from “strongly disagree” to “strongly agree” The total score is interpreted as a continuous index, with higher values indicating a greater degree of kinesiophobia. Although the TSK-11 is commonly interpreted using a total score, factorial analyses of the Spanish version have identified a stable two-factor structure comprising Activity Avoidance (AA) and Harm (H). The Spanish version, validated for the Spanish-speaking population in 2011, demonstrated adequate psychometric properties in patients with both acute and chronic pain, confirming a stable two-factor structure and showing good internal consistency (Cronbach’s α = 0.79 for the total score; α = 0.79 for AA; α = 0.70 for H), as well as evidence of convergent validity through significant associations with pain-related psychological variables and predictive validity over time [33]. The TSK-11 has proven to be a widely used tool across multiple populations, and its short version reduces respondent burden without compromising measurement quality, making it particularly suitable for athletic populations owing to its reliability and accessibility [34,35].
2.4.3. Psychological Readiness of Injured Athlete to Return to Sport Questionnaire (PRIA-RS)
Self-perceived psychological readiness for RTS was assessed using PRIA-RS in its original Spanish version. The instrument consists of 10 items rated on a 5-point Likert scale (total score 10–50), with higher values indicating greater readiness. Scores ≥ 40 reflect adequate readiness, 35–39 suggest the need for further assessment, and <35 indicate inadequate readiness. This questionnaire was developed and validated in Spanish using the Delphi method, with high content validity (Aiken’s V > 0.90) [36]. Additionally, the questionnaire has been translated and culturally adapted into other languages, including English, Greek, and Turkish, further supporting its international applicability [37,38,39].
It was inspired by recognised scales such as the TSK, Anterior Cruciate Ligament–Return to Sport after Injury (ACL-RSI) and Injury-Psychological Readiness to Return to Sport (I-PRRS), addressing key components including coping, confidence, emotional state, external pressure, and perceived security [36]. Its psychometric performance has also been confirmed in later analyses of injured athletes [40].
2.5. Statistical Analysis
Categorical variables were expressed as frequencies and percentages, while continuous variables with a normal distribution were summarized using means, standard deviations (SD), interquartile ranges, and 95% confidence intervals (CIs). Normality of continuous variables was assessed using the Shapiro–Wilk test and visual inspection of Q–Q plots. Relationships between study variables were examined using inferential and correlation analyses. Specifically, independent-sample Student’s t-tests were used to analyse differences by sex, and one-way ANOVA tests were performed to examine differences according to injury type, injury location, and weight category. To assess the relationship between TSK-11 scores and PRIA-RS categories, a one-way ANOVA was conducted to compare kinesiophobia across readiness groups defined by the questionnaire. Effect sizes were calculated to quantify the magnitude of group differences, using Cohen’s d for t-tests and eta squared (η^2^) for ANOVA, together with their corresponding 95% confidence intervals. The effect size (ES) was estimated by calculating Cohen’s d coefficient. ES was classified as trivial (<0.20), small (0.20–0.49), moderate (0.50–0.79), or large (>0.80). Pearson’s correlation coefficients were calculated to explore associations between continuous variables, including age, time since injury onset, time out of competition, and psychological scores (TSK-11 and self-perceived readiness for return to sport). Additionally, a K-means cluster analysis was conducted to identify psychological and clinical profiles based on standardized quantitative variables, including age, time since injury onset, time out of competition, and psychological scores from both questionnaires. Solutions ranging from two to seven clusters were compared using the Silhouette Index, and the configuration with the highest internal cohesion and clinical interpretability was selected. Statistical significance was set at p < 0.05. All analyses were performed using JAMOVI software (version 2.6.26.0.) [41].
3. Results
3.1. Sample Characteristics
Figure 1 provides comprehensive details regarding the recruitment and progression of participants. All 51 participants completed the questionnaire, resulting in no missing data.
The study sample comprised Spanish-speaking judokas competing at national or international levels, all aged over 16 years, including 27 women (52.9%) and 24 men (47.1%), with a mean age of 23.04 ± 3.79 years. Table 1 presents a summary of the descriptive sociodemographic and clinical-sport characteristics of the sample. This summary includes participants age, sex, weight category, injury location and type, time since injury onset and time out of competition.
3.2. Psychological Variables
Descriptive statistics and sex comparison of psychological variables are presented in Table 2. The assumption of homogeneity of variances was met in all analyses, as confirmed by Levene’s test (p > 0.05). No statistically significant differences were observed between sexes for any psychological variable (p > 0.05).
3.3. Inferential Analysis
Prior to group comparisons by weight category, the <100 kg and >100 kg male categories were merged to ensure adequate sample sizes, as statistical analyses cannot be performed on categories containing only one participant. Subsequently, a series of one-way ANOVA tests was conducted to examine differences in psychological scores according to weight category (for both sexes), injury location, injury type, and psychological readiness categories defined by the PRIA-RS. The assumption of homogeneity of variances was met in all analyses, as confirmed by Levene’s test (p > 0.05). No statistically significant differences were observed across groups (p > 0.05). ANOVA comparisons are summarized in Table 3.
Pearson correlation analyses were performed to explore linear associations between age, time since injury onset, time out of competition, and psychological variables. No significant associations were identified (p > 0.05), except for strong positive correlations between the TSK-11 subscales and the total TSK-11 score, confirming the internal consistency of the scale. A positive association was observed between time since injury and time out of competition, showing trend toward statistical significance (r = 0.27, p = 0.055). No other significant associations were detected between TSK-11 scores and PRIA-RS scores. The correlation matrix is presented in Table 4.
3.4. Cluster Analysis
Although the four-cluster solution yielded a higher Silhouette Index (SI = 0.529), it resulted in a single-case cluster and was therefore not retained. Instead, the three-cluster solution was selected as it provided the best balance between internal cohesion and clinical interpretability (SI = 0.471). The three clusters comprised 16, 17, and 18 participants, respectively, and revealed distinct psychological and clinical profiles. Cluster 1 was characterized by elevated levels of kinesiophobia across both TSK-11 subscales, a longer duration since injury onset, extended absence from competition, and slightly below-average self-perceived readiness to RTS scores on the PRIA-RS. Cluster 2 exhibited intermediate kinesiophobia, the lowest PRIA-RS scores, younger age, and shorter durations since injury and competition absence. Cluster 3 demonstrated the lowest kinesiophobia levels, the highest PRIA-RS scores, older age, and near-average values for injury duration and time away from competition. The distribution of participants across clusters is illustrated in Figure 2, while standardized cluster centroids (z-scores) are presented in Table 5.
4. Discussion
The overall sample homogeneity, particularly regarding sex and age, provided a balanced context for comparison. Knee and shoulder injuries were the most prevalent, in line with previous epidemiological data [8], although the predominance of ligamentous and muscular injuries differs from reports describing higher rates of sprains, fractures, and dislocations [10]. No significant differences were found in psychological variables according to sex, weight category, injury characteristics, or self-perceived readiness to RTS groups, nor were relevant correlations observed with age or injury-related timelines, except for strong associations within the TSK-11. Injury timelines showed the expected wide variability, consistent with the inclusion of athletes with diverse injury types and severities. However, cluster analysis revealed three psychological profiles, indicating that person-centred approaches capture meaningful psychological variability not detected by traditional group-based analyses. These findings align with previous cluster-based studies in sports psychology that identified psychological profiles in athletes using self-reported constructs and considering differences in age and competitive experience [42,43].
The absence of sex and weight categories differences contrasts with studies reporting greater psychological vulnerability among female athletes, strongly linked to the widespread use of RWL practices, often poorly controlled and accompanied by negative emotional profiles [11,44]. Female judokas appear particularly vulnerable, showing greater emotional distress and body image dissatisfaction, as well as a high risk of developing eating disorders, with Rouveix et al. reporting that 91.7% were at significant risk [45]. Similarly, heavier weight categories, where RWL practices are generally less frequent, were expected to show more favourable psychological profiles; however, no differences emerged despite the documented negative effects of RWL [12]. Injuries within interdependent training environments may also disrupt team dynamics, decrease motivation, and foster an external locus of control [19].
Among contextual factors, competitive pressure, rapid decision-making under stress, sustained focus amid changing and aggressive stimuli, and the individual nature of performance outcomes intensify psychological demands [45,46]. The lack of significant differences in the present study may reflect the influence of unmeasured psychological factors that modulate individual emotional responses to injury. Previous studies have shown that coping styles mediate the relationship between resilience and perceived stress, modulating athletes’ emotional responses to injury, while both trait and state anxiety are associated with perceived stress, with this relationship moderated by cognitive reappraisal strategies [47,48]. Moreover, an internal locus of control and higher openness to experience personality trait have been associated with faster recovery and greater readiness to RTS [49]. These psychological responses may also be influenced by individual biological variability, potentially contributing to heterogeneous post-injury adaptation [46]. Overall, these factors may be key to athletes’ psychological adaptation after injuries.
Neither clinical nor sport-related variables showed significant correlations, which may reflect sample-specific factors (case selection, injury severity, timing of assessment) or differences in diagnostic or reporting criteria. Specifically, the lack of associations with injury-related timelines differs from previous evidence, which has suggested that positive psychological readiness facilitates RTS [21]. Instead, factors such as rehabilitation support, injury severity, and individual coping processes, particularly acceptance of the recovery process and lower catastrophizing, may exert a stronger influence on psychological adjustment and readiness to return [50]. The main psychological outcomes reflected an intermediate profile, with a mean TSK-11 score below the scale midpoint, indicating mild fear of movement without clinically relevant kinesiophobia. This pattern suggests a cautious but functional response and aligns with the findings in both combat and non-contact sports [51,52], with similar scores across athletic samples. Similarly, PRIA-RS scores indicated an intermediate self-perceived readiness to RTS, with only 19% of athletes showing adequate predisposition to return, while approximately 80% presented some degree of psychological vulnerability, highlighting the relevance of self-perception in the return-to-sport process. No association between TSK-11 and PRIA-RS further implies that kinesiophobia does not necessarily entail low confidence in RTS.
Cluster analysis offers a more nuanced characterisation of psychological profiles beyond group-based comparisons. The youngest athletes (Cluster 2) exhibited low kinesiophobia but reduced confidence in returning to sport, suggesting limited psychological maturity and less consolidated self-regulatory resources, likely influenced by fewer prior injury experiences. In contrast, older athletes (Cluster 3) showed low fear of movement alongside high self-perceived readiness, consistent with more effective emotional regulation and adaptive strategies, potentially associated with age-related maturity in sports and certainly shaped by previous recovery experiences. Finally, Cluster 1 presented high kinesiophobia, prolonged recovery times, and low self-perceived readiness to RTS. This profile may reflect the maladaptive fear–avoidance pattern described in the previous literature, where avoidance strategies progressively consolidate and may contribute to longer injury timelines. Specifically, this model proposes that when pain or injury-related sensations are interpreted as threatening, athletes may develop fear of movement, leading to protective avoidance behaviours. Furthermore, according to Pavlov’s and Skinner’s conditioning models, movements associated with pain can trigger an automatic fear response, which explains how avoiding painful movements temporarily reduces anxiety, reinforcing the fear–avoidance pattern and potentially delaying functional recovery and RTS, as avoidance behaviours become maladaptive strategies over time [53,54]. Moreover, the combination of elevated fear and reduced self-perceived readiness observed in this cluster may reflect greater psychological vulnerability during the recovery process [18]. Personality traits such as neuroticism or perfectionism may favour avoidant coping, while active coping and cognitive restructuring support better adaptation [55]. Finally, some authors have suggested that genetic differences may modulate psychological traits relevant to injury recovery [46].
4.1. Limitations
This study has several limitations that should be considered when interpreting the results. First, the psychological variables assessed captured only a part of the multidimensional return-to-sport process. The lack of detailed injury-related information, added to the absence of relevant contextual and RWL variables, may have constrained the analysis, as well as the absence of information about previous injuries and prior sports experience, as predicted by the literature [8]. Furthermore, the uneven distribution of some variables limited the representativeness, as not all injury types, locations, or weight categories were equally represented. In this context, the uneven distribution of some variables limited representativeness, and the weight category could not be included in the cluster analysis due to its nominal nature and low representation at certain levels. The cross-sectional design and reliance on self-reported questionnaires introduce potential sources of bias. Selection bias may be present due to voluntary participation, possibly favouring athletes with greater awareness of their rehabilitation process. Information bias and social desirability bias cannot be excluded, particularly in psychological variables, despite assurances of anonymity and supervised data collection. Moreover, as only Spanish-speaking athletes were included to ensure instrument validity, the generalisability of the findings to other linguistic and cultural contexts may be limited.
4.2. Future Research
Future research should incorporate more psychological constructs such as coping strategies, anxiety, locus of control, personality traits, injury acceptance, and catastrophizing, along with completed injury assessments and considering athletes’ previous injury and athletic maturity. Additionally, contextual factors including training environment, the influence of rapid weight loss practices, and social support should be considered or assessed. Longitudinal studies are needed to better understand how psychological readiness changes throughout the injury and recovery process and to assess the effects of multidisciplinary rehabilitation approaches. Finally, future research may benefit from adopting enactive perspectives of injury recovery, acknowledging that psychological responses are shaped through ongoing interactions between the athlete and their environment, including rehabilitation contexts, social dynamics, and sport-specific demands [56].
4.3. Practical Applications
The findings of this study may have several practical implications for clinicians, physiotherapists, sport psychologists, and coaches involved in the rehabilitation and return-to-sport (RTS) process of high-performance judokas.
First, the identification of different psychological profiles suggests that injured athletes should not necessarily be managed through a single standardized rehabilitation approach. Incorporating brief psychological screening tools such as the Tampa Scale for Kinesiophobia (TSK-11) and the Psychological Readiness of Injured Athlete to Return to Sport (PRIA-RS) questionnaire into routine assessments may help professionals identify athletes who could benefit from additional psychological support during rehabilitation. Early recognition of fear of movement or reduced psychological readiness may allow clinicians to adapt rehabilitation strategies more individually.
Second, athletes presenting with higher levels of kinesiophobia and longer recovery periods may particularly benefit from integrating psychological strategies into the rehabilitation process. Approaches such as progressive exposure to sport-specific movements, reassurance and education about the injury and recovery process, as well as gradual return-to-training protocols, may help reduce fear–avoidance behaviours and increase confidence in movement.
Third, the profile observed in younger athletes—characterized by relatively low kinesiophobia but lower perceived readiness to return to sport—suggests the possible influence of psychological maturity and previous injury experience in the recovery process. In this context, intervention strategies including educational guidance, confidence-building strategies, and structured decision-making during the RTS phase may help improve athletes’ perceived competence and readiness to resume sport participation. In addition, the literature on mental preparation in combat sports highlights the role of psychological skills training aimed at enhancing athletes’ confidence, stress regulation, anxiety management, and attentional control. Techniques such as visualization, inner speech regulation, mindfulness-based strategies, and relaxation training have been proposed as useful tools to support athletes’ mental preparation in demanding sport situations [57].
Finally, the results reinforce the importance of adopting a multidisciplinary approach in the rehabilitation of high-performance judokas. Combining physical rehabilitation with psychological monitoring may support more informed return-to-sport decisions, potentially contributing to safer reintegration into training and competition while reducing the risk of reinjury and supporting long-term performance.
From a practical perspective, the psychological profiles identified through cluster analysis may help clinicians adapt rehabilitation strategies according to the athletes’ psychological characteristics. Athletes belonging to the cluster with higher kinesiophobia and longer recovery periods may require specific interventions aimed at reducing fear of movement, such as gradual exposure to sport-specific tasks and reassurance during rehabilitation. In contrast, younger athletes with lower levels of kinesiophobia but reduced perceived readiness to return to sport may benefit from strategies focused on improving confidence, providing education about the recovery process, and offering structured guidance during the return-to-sport phase. Considering these psychological profiles during rehabilitation may help physiotherapists better individualize treatment and support safer return-to-sport decisions.
5. Conclusions
This study provides an overview of musculoskeletal injuries and psychological responses in high-performance judokas. No significant associations were found between sociodemographic or clinical-sport variables and psychological responses. Overall, athletes presented non-disabling levels of kinesiophobia but reduced self-perceived readiness to return to sport (RTS), with a high proportion reporting low readiness. Cluster analysis identified three distinct psychological profiles differing in age, recovery time, kinesiophobia, and self-perceived readiness to RTS. These findings highlight the importance of considering psychological factors during rehabilitation and return-to-sport decision-making in high-level judokas and support the need for further research examining how experience and injury-related factors influence recovery and RTS outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chaabene H. Negra Y. Bouguezzi R. Mkaouer B. Franchini E. Julio U. Hachana Y. Physical and Physiological Attributes of Wrestlers: An Update J. Strength. Cond. Res.2017311411144210.1519/JSC.000000000000173828030533 · doi ↗ · pubmed ↗
- 2Karatrantou K. Katsoula C. Tsiakaras N. Ioakimidis P. Gerodimos V. Strength Training Induces Greater Increase in Handgrip Strength than Wrestling Training per Se Int. J. Sports Med.20204153353810.1055/a-1128-716632215897 · doi ↗ · pubmed ↗
- 3Torres-Luque G. Hernández-García R. Escobar-Molina R. Garatachea N. Nikolaidis P.T. Physical and Physiological Characteristics of Judo Athletes: An Update Sports 201642010.3390/sports 401002029910268 PMC 5968945 · doi ↗ · pubmed ↗
- 4Branco B.H.M. Massuça L.M. Andreato L.V. Marinho B.F. Miarka B. Monteiro L. Franchini E. Association between the Rating Perceived Exertion, Heart Rate and Blood Lactate in Successive Judo Fights (Randori)Asian J. Sports Med.2013412513010.5812/asjsm.3449423802054 PMC 3690732 · doi ↗ · pubmed ↗
- 5Franchini E. Del Vecchio F.B. Matsushigue K.A. Artioli G.G. Physiological Profiles of Elite Judo Athletes Sports Med.20114114716610.2165/11538580-000000000-0000021244106 · doi ↗ · pubmed ↗
- 6Kim K.-S. Park K.J. Lee J. Kang B.Y. Injuries in National Olympic Level Judo Athletes: An Epidemiological Study Br. J. Sports Med.2015491144115010.1136/bjsports-2014-09436526216871 · doi ↗ · pubmed ↗
- 7Kujala U.M. Taimela S. Antti-Poika I. Orava S. Tuominen R. Myllynen P. Acute Injuries in Soccer, Ice Hockey, Volleyball, Basketball, Judo, and Karate: Analysis of National Registry Data BMJ 19953111465146810.1136/bmj.311.7018.14658520333 PMC 2543722 · doi ↗ · pubmed ↗
- 8Pocecco E. Ruedl G. Stankovic N. Sterkowicz S. Del Vecchio F.B. Gutiérrez-García C. Rousseau R. Wolf M. Kopp M. Miarka B. Injuries in Judo: A Systematic Literature Review Including Suggestions for Prevention Br. J. Sports Med.2013471139114310.1136/bjsports-2013-09288624255909 · doi ↗ · pubmed ↗