C-Reactive Protein in Saliva as a Non-Invasive Marker of Metabolic Syndrome: A Systematic Review and Meta-Analysis
Mohammad Khalfan, Yash Brahmbhatt, Sarah Pagni, Ripple Garg, Ahmad A. Alkandari, Abrar Alkhesaili, Nouf Alsheredah, Nawal AlDhafeeri, Hawra Baroon, Woroud Al-Sulimmani, Shaikha Almatrouk, Fahad Alali, Hend Alqaderi

TL;DR
This study reviews evidence that salivary C-reactive protein levels may be a non-invasive indicator of metabolic syndrome, though more consistent research is needed.
Contribution
The paper provides a systematic review and meta-analysis on salivary CRP as a potential non-invasive marker for metabolic syndrome.
Findings
Salivary CRP levels were higher in individuals with metabolic syndrome compared to controls.
There was substantial heterogeneity across studies, likely due to differences in population and methodology.
No publication bias was detected in the included studies.
Abstract
Metabolic syndrome (MetS) is a cluster of conditions that rely on low-grade systemic inflammation and increase the risk of cardiovascular disease, type 2 diabetes, and stroke. C-reactive protein (CRP) has attracted growing interest in saliva as a non-invasive alternative to serum CRP testing, though existing evidence remains inconsistent. This systematic review and meta-analysis evaluated the association between salivary CRP levels and MetS and examined the consistency of findings across populations and methodological approaches. PubMed, the Cochrane Library, and Web of Science were searched up to December 2024 following PRISMA 2020 guidelines. Nineteen studies involving 3265 participants with and without MetS were included. Random-effects meta-analysis demonstrated higher salivary CRP levels in individuals with MetS compared with controls (SMD = 1.02; 95% CI −0.23 to 1.81), with…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
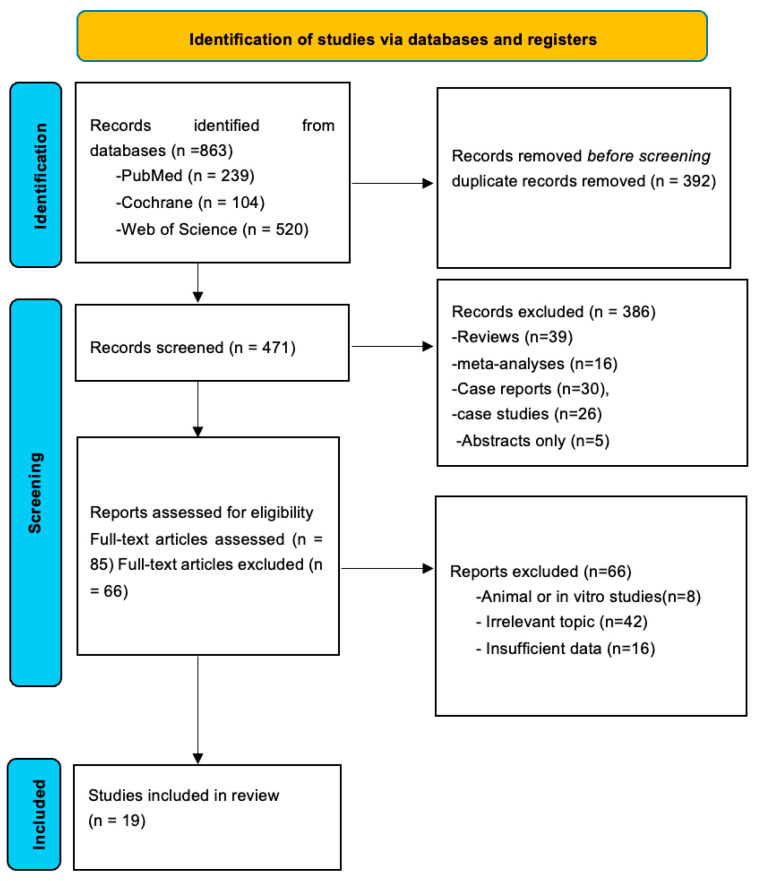 Figure 1
Figure 1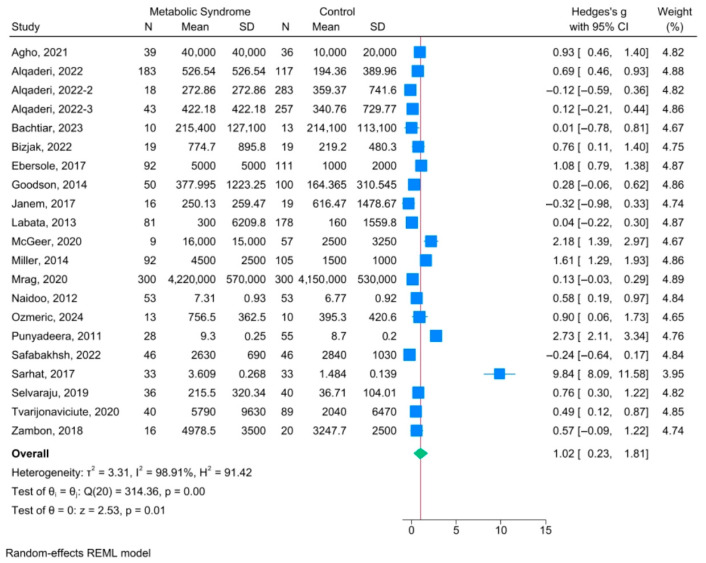 Figure 2
Figure 2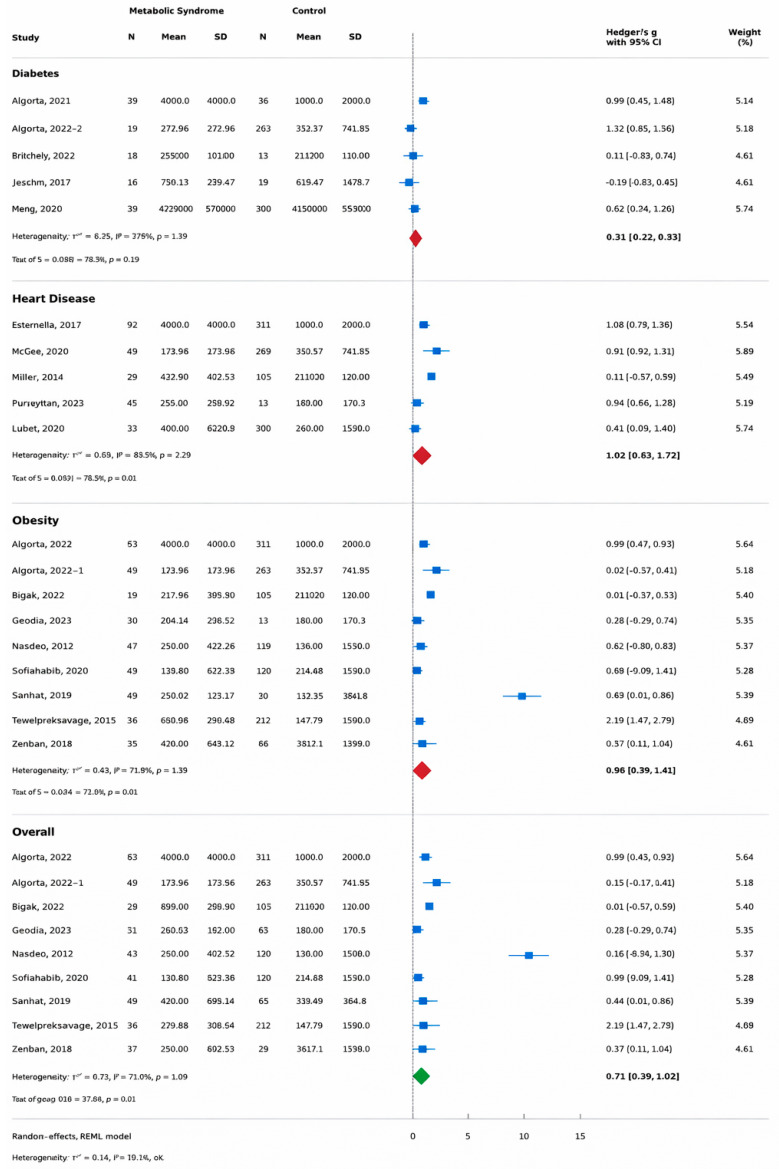 Figure 3
Figure 3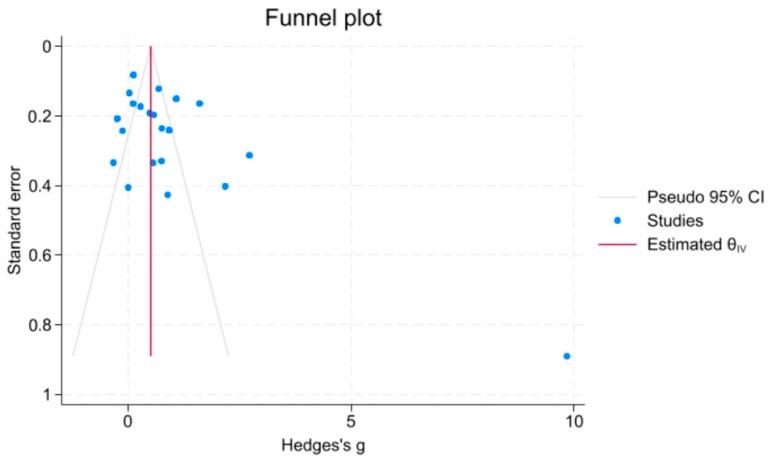 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSalivary Gland Disorders and Functions · Oral microbiology and periodontitis research · Stress Responses and Cortisol
1. Introduction
Metabolic syndrome (MetS) has emerged as a significant global health challenge, characterized by a constellation of interconnected metabolic abnormalities, including central obesity, elevated blood pressure, dyslipidemia, insulin resistance, and impaired glucose regulation [1]. Together, these risk factors significantly elevate the likelihood of developing type 2 diabetes (T2D) and cardiovascular diseases (CVDs), the two leading causes of global morbidity and mortality [2]. Alarmingly, current estimates suggest that nearly one-quarter of the world’s adult population is affected by MetS, with prevalence continuing to rise in parallel with the global obesity epidemic and sedentary lifestyles [3,4].
Although MetS is not classified as a disease in itself, it functions as a potent indicator of underlying pathophysiological dysregulation [5]. The clustering of its components reflects a shared basis in chronic low-grade systemic inflammation and insulin resistance [6]. One of the challenges with MetS is its insidious progression [7]. Often asymptomatic in its early stages [2], it may go undetected until serious complications such as myocardial infarction [8], stroke [9], or T2D manifest [10]. This silent nature underscores the need for early identification and proactive management of individuals at risk [11].
A growing body of evidence indicates that elevated circulating inflammatory mediators contribute to endothelial dysfunction and accelerate the development of MetS and its individual components [6,11]. Several inflammatory biomarkers have been implicated in this inflammatory process, including interleukin (IL)-6, IL-8, IL-10, leptin, insulin, vascular endothelial growth factor (VEGF), monocyte chemoattractant protein-1 (MCP-1), and C-reactive protein (CRP) [6,12,13,14]. Among the wide range of candidate salivary biomarkers, CRP is one of the most clinically relevant inflammatory markers associated with a wide range of inflammatory conditions, specifically metabolic conditions [15,16]. Serum CRP reflects hepatic acute-phase responses to cytokines such as interleukin-6 (IL-6) [15,17]. The onset and severity of MetS are frequently linked to elevated CRP [18,19], indicating its value in risk stratification and monitoring disease progression [20,21,22,23]. Importantly, CRP is also detectable in saliva [24,25,26,27,28,29]. Its presence in the oral cavity is thought to arise from passive diffusion and ultrafiltration from the bloodstream, as well as transudation through gingival crevicular fluid [25,26,28]. These mechanisms are accentuated during systemic inflammation [26]. Because salivary CRP largely reflects serum CRP, salivary concentrations have been shown to correlate with systemic levels [25,26,27,30,31,32,33,34], supporting the premise that saliva may serve as a practical, non-invasive medium for assessing the inflammatory burden characteristic of MetS.
Despite its clinical utility, measuring CRP in serum presents practical limitations, particularly in large-scale screening contexts or among populations where venipuncture is not feasible [17,24]. Blood collection is invasive, potentially distressing, and may require trained personnel, sterile equipment, and controlled conditions [17]—all of which are barriers in low-resource settings or when high-frequency monitoring is necessary. This has led to growing interest in saliva as a diagnostic fluid [28,29,30,31,32]. Saliva offers a convenient, non-invasive, and cost-effective alternative to blood, with the additional advantage of easy and repeated sampling [27,28,29,30,31,32,33]. The use of saliva for diagnostic purposes is expanding across several domains, including infectious diseases, hormonal disorders, and cardiovascular risk assessment [29,30,31,32,33,34]. Importantly, emerging evidence suggests that salivary CRP levels strongly correlate with serum CRP concentrations [25,26,27,35], indicating that salivary CRP may reflect systemic inflammatory status and thus hold potential as a detecting biomarker for MetS.
Despite the growing number of studies investigating salivary CRP, the literature remains fragmented and inconclusive [35,36,37,38]. Variability in population characteristics, saliva collection protocols, CRP assay methods, and diagnostic criteria has contributed to inconsistent findings. Although some studies have found strong associations between salivary CRP and cardiometabolic risk phenotypes [39,40,41], the consistency of salivary CRP in detecting early metabolic dysfunction compared to its serum counterpart remains inconsistent [42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59]. Given this gap in knowledge, there is a compelling need to systematically evaluate the existing evidence. A comprehensive review of the current research is necessary to determine whether salivary CRP can be considered a reliable, non-invasive alternative to serum-based CRP testing in identifying individuals at risk for MetS.
Therefore, this systematic review and meta-analysis represents the first quantitative synthesis to assess the association between salivary CRP levels and metabolic syndrome-related cardiometabolic phenotypes. By pooling data across diverse populations and study designs, this study aims to (i) estimate the magnitude of difference in salivary CRP between individuals with and without metabolic dysfunction, and (ii) explore sources of heterogeneity related to assay methodology and diagnostic definitions. Clarifying this evidence base may inform future screening strategies and support the development of accessible, saliva-based approaches for metabolic risk assessment, particularly in community and resource-limited settings.
2. Materials and Methods
2.1. Search Strategy
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines [60]. A structured literature search was performed in three electronic databases, PubMed, Cochrane Library, and Web of Science, covering all records from inception to December 2024. A PRISMA flowchart of the selection process is shown in Figure 1. Supplementary Materials include the complete search strategy and a list of the (n = 66) excluded reports.
The PECO (Population, Exposure, Control, Outcome) framework guided study selection. The target population included individuals of all age groups, genders and geographic locations who have metabolic syndrome (MetS). Accepted diagnostic criteria for MetS included NCEP ATP III, IDF, or WHO guidelines [5,39], as shown in Table 1. The exposure of interest was salivary C-reactive protein (CRP) levels. The control group consisted of individuals without MetS or any of its individual components (central obesity, dysglycemia, hypertension, T2D or dyslipidemia). The outcome of interest was one or more MetS risk factors including central obesity (waist circumference, BMI), hypertension, dyslipidemia (high LDL or low HDL) and CVD.
Search terms included combinations of “saliva,” “salivary,” “C-reactive protein,” “CRP,” and metabolic-syndrome–related terms such as “metabolic syndrome,” “MetS,” “insulin resistance,” “cardiometabolic risk,” “Obesity” “dyslipidemia,” “hyperglycemia,” and “hypertension.” Terms relating only to single metabolic abnormalities (e.g., “obesity,” “type 2 diabetes”) were not used as standalone identifiers for MetS. These terms were used with combinations of “OR” and “And”. No language restrictions were applied. After duplicate removal, two reviewers independently screened titles and abstracts before conducting full-text assessment (Figure 1).
2.2. Eligibility Criteria
Inclusion and Exclusion Criteria
Studies were included if they met the following criteria:
- Original, peer-reviewed human research.
- Quantitative measurement of salivary C-reactive protein (CRP).
- Participants diagnosed with metabolic syndrome (MetS) according to established criteria (NCEP ATP III, IDF, or WHO) or with cardiometabolic conditions related to MetS, including obesity or overweight states, hyperglycemia or type 2 diabetes, hypertension, or cardiovascular risk phenotypes.
- Inclusion of a comparator group consisting of individuals without MetS or any of its individual components.
- Sufficient data available to extract or calculate mean and variance for salivary CRP.
Exclusion criteria were:
- Non-human, in vitro, or ex vivo studies.
- No quantitative salivary CRP measurement.
- No appropriate comparison group.
- Studies not related to metabolic dysfunction such as inflammation from infection, autoimmune disease, or oral pathology.
- Publication types such as reviews, systematic reviews, meta-analyses, case reports, case series, conference abstracts, editorials, and commentaries.
- Duplicate publications or overlapping datasets (the most complete dataset was retained).
When data were missing or unclear, study authors were contacted. Two of the three contacted authors provided the required information; one study was excluded due to non-response.
2.3. Data Extraction and Quality Assessment
Study quality was assessed using the Newcastle–Ottawa Scale (NOS) for observational studies [40]. NOS assesses the quality of non-randomized studies across three domains: selection of study groups, comparability of groups, and ascertainment of the outcome, using a star-grading system, with a maximum of nine stars indicating the highest quality [40,41,42]. Studies scoring 1–3 were classified as low quality, 4–6 as moderate, and 7–9 as high quality [42]. Discrepancies in extracted data and quality assessment were resolved through consensus.
2.4. Handling of Mixed Populations
Several studies enrolled heterogeneous populations varying by age, metabolic status, periodontal condition, or disease severity. Where studies reported disaggregated salivary CRP values by relevant subgroups (e.g., MetS vs. controls, obese vs. normal weight, diabetic vs. non-diabetic), subgroup-specific data were extracted for analysis. This approach was applied to studies stratifying by metabolic syndrome components such as obesity [43,44,45,49,50,51,52,53,54,55,58,59,60], T2D [43,46,48,52,54,55], CVD [44,47,56,57,58], or hypertension [60].
When studies involved mixed cardiometabolic populations but only reported combined CRP values [43,44,45,49,50,51,52,53,54,55], the aggregated data were included with this limitation documented. For longitudinal studies with repeated measures [43,47,48,55,57,59,61], the time point most relevant to cardiometabolic assessment was selected.
When studies reported both aggregated cardiometabolic group data and stratified subgroup data, an extraction hierarchy was applied. Subgroup-specific data were preferentially extracted whenever available (e.g., obese vs. non-obese, T2D vs. controls, CVD vs. controls), as these provide greater phenotypic specificity and reduce clinical heterogeneity. Aggregated values were only used when subgroup-level data were not reported or could not be derived from the published results.
For studies reporting multiple metabolic phenotypes within the same cohort, each phenotype was entered separately into the corresponding subgroup meta-analysis, while a single representative comparison was used for the overall pooled analysis to avoid double-counting of participants.
Where participants had concurrent inflammatory conditions such as periodontitis [56,57,58], we prioritized the extraction of metabolically relevant groups and noted periodontal inflammation as a potential confounder in the quality assessment. The substantial heterogeneity observed in the pooled analysis (I^2^ = 98.91%) reflects, in part, the population diversity across studies (Figure 1).
2.5. Saliva Collection and CRP Assay Methods
The main methods of saliva collection included unstimulated whole saliva [43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,59,61] and saliva obtained under standardized conditions (fasting state, morning collection) [43,45,46,49,50,53,54,55,58], with most studies processing samples through centrifugation before storage at −20 °C or −80 °C.
2.6. Statistical Analysis
All meta-analyses were conducted using a random-effects model due to expected clinical and methodological heterogeneity across studies. Standardized mean differences (SMDs) were computed to account for varying measurement scales. Where CRP levels were reported as medians with interquartile ranges, mean and standard deviation values were estimated using validated statistical conversions.
Between-study heterogeneity was assessed using Cochran’s Q test, the I^2^ statistic (interpreted as low, moderate, and high at approximately 25%, 50%, and 75%, respectively), and Tau^2^ to estimate between-study variance. Statistical significance was defined as p < 0.05. Publication bias was evaluated via funnel plot asymmetry and tested with Egger’s and Begg’s tests.
2.7. Subgroup Analysis
Pre-specified subgroup analyses were conducted to explore potential sources of heterogeneity and to examine whether salivary CRP levels differed according to specific metabolic phenotypes and assay methodology. As none of the included studies assessed metabolic syndrome as a unified clinical entity using standardized composite definitions, subgroup analyses were performed based on individual metabolic components, including obesity, T2D, and CVD. However, meta-analysis for the hypertension subgroup was not feasible because only a single study investigated hypertension as an outcome [60].
Additional subgroup analyses were conducted for studies reporting multiple metabolic or inflammatory subgroups (obesity, T2D, heart disease and hypertension); subgroup-specific effect estimates were extracted where available; otherwise, aggregated data were used.
Heterogeneity within each subgroup was quantified using the I^2^ statistic, and differences in pooled effect estimates across subgroups were examined descriptively to assess whether clinical phenotype or assay methodology contributed to variability in effect size.
2.8. Sensitivity Analysis
A leave-one-out sensitivity analysis was conducted to evaluate the robustness of the overall pooled estimate and to identify the influence of individual studies on the summary effect size and heterogeneity. In this analysis, each study was systematically removed from the meta-analysis one at a time, and the pooled standardized mean difference (SMD), 95% confidence interval (CI), and I^2^ statistic were recalculated for the remaining studies. This procedure allowed for the assessment of whether the overall conclusion was disproportionately driven by any single study. The stability of the pooled estimate was determined by observing the range of SMDs and the consistency of the direction and statistical significance of the effect after each exclusion.
3. Results
3.1. Study Selection and Characteristics
A total of 863 records were identified through database searching. Following the removal of 392 duplicates, 471 records underwent title and abstract screening. At this stage, review articles (n = 39), meta-analyses (n = 16), case reports (n = 30), case series (n = 26), and abstracts without available full texts (n = 5) were excluded. Eighty-five studies were subsequently assessed for full-text eligibility. Of these, 66 records were excluded after full-text review due to irrelevance to the research question (n = 42), insufficient data (n = 16), or animal and in vitro study design (n = 8). Ultimately, 19 studies met the inclusion criteria and were included in the quantitative synthesis, comprising a total of 3265 participants (Figure 1) [33,43,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61].
The included studies represented diverse populations across five continents and 15 countries. Studies were conducted in Asia [43,49], Africa [44,45,48], Middle East [49,55], Europe [47,52,54,59,60], and North America [53,57]. Study populations included children and adolescents [43,45,49,50,53,54], adults [33,46,47,48,51,55,56,57,58,61], pregnant women [55], and elderly individuals [59]. Sample sizes ranged from 23 participants [57,61] to 600 participants [48], with several large cohorts derived from school-based screening programs [43,45,49,50,53,54]. Most studies em-ployed cross-sectional designs [45,46,47,50,53,54,58,59], with the remainder using case–control [33,51,52,56,57] or cohort designs [43,48,49,55,61] (Table 2).
The included studies examined individual cardiometabolic phenotypes related to metabolic syndrome, including obesity [43,44,45,49,50,51,52,53,54,55], T2D [43,46,48,53,61], CVD [33,47,58,59], hypertension [57], or combinations of these conditions (Table 2).
Salivary CRP concentrations were quantified using validated immunoassay techniques, predominantly high-sensitivity enzyme-linked immunosorbent assays (ELISA) [43,44,45,46,47,49,53,55,57,58,59] and multiplex bead-based platforms [33,50,52,54,61]. Methodological quality assessed using the Newcastle–Ottawa Scale ranged from moderate to high (scores 4–9), indicating a generally acceptable methodology across included studies [40,41,42] (Table 2).
3.2. Overall Meta-Analysis of Salivary CRP
Nineteen studies involving 3265 participants (1399 individuals with metabolic conditions and 1857 healthy controls) compared salivary CRP concentrations between groups [33,43,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61] (Table 3).
Absolute salivary CRP concentrations demonstrated substantial variability across studies, ranging from 9.3 pg/mL to >420,000 pg/mL in metabolic disease groups and from 7.3 pg/mL to 415,000 pg/mL in control groups, representing a >40,000-fold difference [43,44,45,49,50,51,52,53,54,55,58,59,61]. The observed heterogeneity (I^2^ = 98.91%; p < 0.001) likely reflects differences in CRP assay methodologies, reporting units, saliva collection protocols, and the metabolic phenotypes represented across study populations. Random-effects meta-analysis demonstrated statistically significant higher salivary CRP levels in individuals with any component of metabolic syndrome compared with healthy controls (standardized mean difference [SMD] = 1.02; 95% confidence interval [CI]: 0.23–1.81; p = 0.01) (Figure 2).
Most studies reported positive associations between metabolic conditions and elevated salivary CRP. Several studies demonstrated large effect sizes, including McGeer et al. [59] (g = 2.18), Punyadeera et al. [58] (g = 2.73), and Miller et al. [56] (g = 1.61). In contrast, a minority of studies reported non-significant or negative associations, including Janem et al. [43], Alqaderi et al. [49], and Safabakhsh et al. [51]. Sarhat et al. [44] was identified as a prominent outlier, reporting an exceptionally large effect size (g = 9.84), contributing substantially to overall heterogeneity.
3.3. Subgroup Analysis: Obesity
Ten studies comprising 1293 participants (526 overweight or obese individuals and 693 controls) evaluated salivary CRP concentrations in relation to obesity status (Figure 3) [43,44,45,49,50,51,52,53,54,55]. The pooled random-effects meta-analysis demonstrated significantly higher salivary CRP levels in individuals with obesity compared with normal-weight controls (g = 0.90; 95% CI: 0.39–1.41; z = 3.46; p < 0.001).
Between-study heterogeneity was substantial (τ^2^ = 0.59; I^2^ = 93.27%), indicating considerable variability across studies in the magnitude of the effect.
While nine of the eleven studies reported positive associations between obesity and salivary CRP, only one study found a negative association [43]. Zambon et al. [55], which examined salivary CRP in pregnancies complicated by obesity and gestational diabetes, was included in the obesity subgroup analysis accordingly.
3.4. Subgroup Analysis: Cardiovascular Disease
Five studies involving 808 participants (371 individuals with CVD and 437 controls) assessed salivary CRP concentrations in relation to cardiovascular disease status [33,47,58,59] (Figure 3). The pooled random-effects analysis demonstrated significantly higher salivary CRP levels in individuals with cardiovascular disease (g = 1.02; 95% CI: 0.31–1.72; z = 2.81; p = 0.005). Heterogeneity within this subgroup was substantial (τ^2^ = 0.60; I^2^ = 94.68%), indicating marked between-study variability.
3.5. Subgroup Analysis: Type 2 Diabetes
Five studies comprising 1034 participants compared salivary CRP concentrations between individuals with T2D (n = 383) and healthy controls (n = 651) [43,46,48,53,61] (Figure 3). The pooled random-effects analysis did not demonstrate a statistically significant difference in salivary CRP levels between groups (g = 0.16; 95% CI: −0.22 to 0.53; z = 0.82; p = 0.41). Moderate heterogeneity was observed within this subgroup (τ^2^ = 0.12; I^2^ = 70.50%), suggesting more consistency across studies compared with the obesity and cardiovascular disease subgroups.
Mrag et al. [48], which contributed the largest sample size within this subgroup, reported no statistically significant difference in salivary CRP levels between individuals with T2D and controls. Similarly, Janem et al. [43] reported no significant difference in salivary CRP between obese individuals with T2D and control participants.
3.6. Sensitivity Analysis
A series of sensitivity analyses were conducted to evaluate the robustness of the pooled effect estimate and explore potential sources of heterogeneity.
In the leave-one-out analysis, the pooled standardized mean difference (SMD) ranged from 0.52 (95% CI: 0.28 to 0.76; excluding Sarhat 2017 [44]) to 0.77 (95% CI: 0.45 to 1.08; excluding Selvaraju 2019 [50]). In all iterations, the direction of effect remained positive and statistically significant (p < 0.001), indicating that no single study reversed the overall association (Table 4).
Given the presence of studies reporting extreme salivary CRP concentrations, additional sensitivity analyses were performed. Exclusion of the most extreme statistical outlier (Sarhat 2017 [44]; Hedges’ g = 9.84) reduced the pooled SMD to 0.52 (95% CI: 0.28 to 0.76), with heterogeneity decreasing from I^2^ = 92.3% to I^2^ = 87.4%. When all four studies reporting extreme absolute CRP values (Sarhat 2017 [44], Mrag 2020 [48], Bachtiar 2023 [61], and Agho 2021 [46]) were excluded, the pooled SMD was 0.55 (95% CI: 0.28 to 0.83) with I^2^ = 87.3% (Table 5). In both scenarios, the association remained positive and statistically significant, although attenuated in magnitude.
To assess whether studies involving periodontal disease influenced the pooled estimate, a sensitivity analysis excluding Ebersole 2017 [56], Ozmeric 2024 [57], and Punyadeera 2011 [58] was conducted. The resulting pooled SMD was 0.71 (95% CI: 0.37 to 1.05) with I^2^ = 93.0%, which was comparable to the primary analysis (Table 4), suggesting that inclusion of periodontal cohorts did not substantially alter the overall findings.
To further contextualize heterogeneity, 95% prediction intervals were calculated. The overall prediction interval ranged from −0.71 to 2.14, indicating that although the average pooled effect was positive, the true effect in a future study could plausibly range from a small negative to a large positive value. Subgroup prediction intervals were similarly wide: Diabetes (−1.10 to 1.41), Heart Disease (−1.70 to 3.73), and Obesity (−0.97 to 2.77) (Table 6).
Exploratory meta-regression analyses were undertaken to investigate potential contributors to heterogeneity. Total sample size was not a statistically significant predictor of effect size (coefficient = −0.0017, p = 0.118). When cardiometabolic condition type was included as a categorical covariate, borderline differences were observed between Heart Disease and Diabetes (p = 0.054) and between Obesity and Diabetes (p = 0.077), suggesting that the underlying disease phenotype may partially account for between-study variability (Table 7).
3.7. Publication Bias
Visual inspection of the funnel plot suggested some asymmetry, with clustering of smaller studies and the presence of an extreme outlier (Figure 4). However, formal statistical testing did not indicate significant publication bias (Egger’s regression test: p = 0.421; Begg’s rank correlation test: p = 0.553). Given the small number of included studies (n = 19) and the presence of substantial heterogeneity, the power of these tests is limited, and publication bias cannot be completely excluded.
4. Discussion
This systematic review and meta-analysis demonstrate that salivary C-reactive protein (CRP) levels are elevated across a range of metabolic disorders, including obesity, type 2 diabetes mellitus (T2D), hypertension, and cardiovascular disease (CVD), compared with healthy controls. The overall pooled effect size indicated a notable increase in salivary CRP among individuals with metabolic dysfunction, although this finding was accompanied by high between-study heterogeneity (I^2^ = 98.91%). Subgroup analyses demonstrated phenotype-specific differences in the association between salivary CRP and metabolic disorders. Significant pooled elevations in salivary CRP were observed for both obesity and cardiovascular disease, whereas no statistically significant association was identified for T2D. Despite these significant findings, heterogeneity remained substantial within the obesity and CVD subgroups, indicating wide variability in effect size magnitude across studies [33,43,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61]. In contrast, the T2D subgroup exhibited comparatively lower heterogeneity, suggesting greater consistency but a weaker overall association, which is consistent with recent reviews of salivary biomarkers [61,62,63].
This variability likely reflects differences in salivary CRP measurement methodologies, reporting units, and saliva collection protocols, with absolute concentrations of >40,000-fold difference between the MetS groups versus control groups [33,43,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61].
The observed elevation of salivary CRP across cardiometabolic conditions aligns with current understanding of MetS as a chronic low-grade inflammatory state [6,7,12]. Inflammatory pathways involving cytokines such as IL-6, tumor necrosis factor-α, and monocyte chemoattractant protein-1 drive hepatic CRP synthesis and contribute to endothelial dysfunction, insulin resistance, and atherosclerosis [12,13,14,18,19]. CRP is therefore not merely a passive biomarker but a downstream integrator of inflammatory activity central to metabolic dysregulation [15,16]. The detection of this inflammatory signal in saliva supports previous evidence demonstrating moderate-to-strong correlations between salivary and serum CRP concentrations across diverse clinical contexts [25,26,27,35,58].
The robustness of the pooled estimate was systematically evaluated through multiple sensitivity analyses. The leave-one-out analysis demonstrated that no single study was solely responsible for the observed association, with pooled SMDs ranging from 0.52 to 0.77 across all iterations. Notably, the exclusion of Sarhat et al. (2017) [44], which reported an exceptionally large effect size (Hedges’ g = 9.84), produced the greatest attenuation of the pooled estimate (from 0.71 to 0.52), although the association remained statistically significant. Similarly, excluding all four studies reporting extreme CRP concentrations did not eliminate the positive association (SMD = 0.55, 95% CI: 0.28 to 0.83), further supporting the consistency of the finding.
Subgroup analysis by metabolic phenotype provided partial insight into sources of heterogeneity, though with important limitations. T2D demonstrated the lowest heterogeneity among subgroups, suggesting that salivary CRP elevation may be more consistent in established hyperglycemic states, possibly reflecting more uniform inflammatory mechanisms associated with chronic glucose dysregulation [43,46,48,53,61] or more standardized diagnostic criteria for diabetes compared to other metabolic conditions [52,63]. In contrast, obesity and CVD exhibited substantial heterogeneity, which may reflect differences in adiposity distribution (visceral vs. subcutaneous), metabolic health status [43,44,45,49,50,51,52,53,54,55,58,59,60], disease severity, and the presence of comorbidities such as CVD across study populations [33,47,58,59]. However, the lack of statistically significant associations between salivary CRP and specific metabolic phenotypes in subgroup analyses, combined with persistent high heterogeneity even within disease categories, indicates that phenotype-specific stratification alone cannot fully explain the observed variability. This reinforces the likelihood that methodological inconsistencies in saliva collection, assay techniques, and inadequate control for confounders such as periodontal disease contribute significantly to effect size dispersion across the evidence base and limit our ability to draw condition-specific conclusions about salivary CRP as a biomarker.
The sensitivity analysis excluding studies with a known periodontal disease [56,57,58] component yielded results comparable to the primary analysis (SMD = 0.71, 95% CI: 0.37 to 1.05), indicating that oral inflammatory cohorts did not disproportionately drive the pooled effect. Nevertheless, residual confounding by periodontal status remains plausible, as most included studies did not comprehensively assess or adjust for oral health conditions.
The 95% prediction interval for the overall effect (−0.71 to 2.14) warrants cautious interpretation. Although the confidence interval indicates a statistically significant average association, the prediction interval crossing zero suggests that the true effect in a future study could plausibly be null. This finding is consistent with the substantial between-study heterogeneity and underscores that salivary CRP elevation may not be uniformly observed across all populations or clinical contexts.
Exploratory meta-regression analyses did not identify total sample size as a significant contributor to heterogeneity. Condition type demonstrated borderline associations, with heart disease and obesity tending toward larger effect sizes compared with diabetes. However, given the limited number of studies within subgroups and the exploratory nature of these analyses, these findings should be interpreted cautiously.
Several methodological and clinical factors likely contributed to this heterogeneity. Methodological variability was substantial, including differences in saliva collection protocols (stimulated versus unstimulated, fasting versus non-fasting), sample processing and storage conditions, and CRP assay platforms. Although both ELISA-based and multiplex bead-based assays demonstrated significant elevations in salivary CRP, heterogeneity remained high within each subgroup, suggesting that analytical variability alone does not fully explain the observed dispersion of effect sizes [43,44,46,47,48,51,55,58,59,60]. Differences in assay sensitivity, calibration ranges, and reporting units further complicate cross-study comparisons [24,25,26,27,28,29].
Clinical heterogeneity was also substantial. The included studies encompassed pediatric, adult, pregnant, and elderly populations, with wide variation in sex distribution, ethnicity, and comorbidity profiles [33,43,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61]. The overall pooled analysis was therefore conceptualized to examine whether salivary CRP reflects a shared inflammatory signal across cardiometabolic disorders that comprise the MetS spectrum, rather than to represent a diagnosis-specific meta-analysis of formally defined MetS. Obesity, T2D, hypertension, and cardiovascular disease are linked through chronic low-grade systemic inflammation, insulin resistance, endothelial dysfunction, and cytokine-mediated hepatic CRP synthesis. CRP thus functions as an integrative downstream biomarker of cardiometabolic inflammatory burden rather than a disease-specific marker.
Importantly, none of the included studies applied a formal, unified diagnostic definition of metabolic syndrome based on established criteria such as NCEP ATP III, IDF, or WHO [5,11,21]. Instead, most investigations examined individual cardiometabolic components, including obesity, T2D, or cardiovascular disease. As MetS is defined by the co-occurrence of multiple metabolic abnormalities—typically central obesity, dyslipidemia, hypertension, and impaired glucose regulation—the absence of standardized diagnostic criteria indicates that pooled estimates reflect inflammatory burden across heterogeneous metabolic phenotypes rather than metabolic syndrome as a discrete clinical entity. Consequently, the specificity of inferences regarding salivary CRP as a biomarker for metabolic syndrome per se is limited [11,13]. The overall pooled estimate should therefore be interpreted as reflecting inflammatory burden across cardiometabolic disorders rather than as a proxy for formally diagnosed metabolic syndrome.
A further critical limitation is inadequate control for confounding factors, particularly oral inflammatory conditions. Periodontal disease is a well-established source of elevated salivary CRP through local immune activation and gingival crevicular fluid transudation, independent of systemic inflammation [37,58]. Given the strong bidirectional relationship between periodontal disease and metabolic disorders such as obesity and diabetes, elevated salivary CRP observed in metabolic populations may partly reflect undiagnosed or unadjusted oral inflammation rather than systemic metabolic dysfunction [12,37,56,57,58]. Most included studies did not perform comprehensive periodontal assessments or adjust for oral health status, representing a plausible alternative explanation for both elevated CRP levels and inter-study heterogeneity.
Additional confounders, including smoking, age, sex, medication use, acute infections, and socioeconomic factors, were inconsistently reported and rarely adjusted for across studies [17,63]. These variables are known to influence systemic inflammatory markers and may have contributed to variability in salivary CRP concentrations. The lack of standardized confounder adjustment further limits causal interpretation and underscores the need for more rigorous study designs.
The distinction between analytical validity and clinical utility is particularly important when interpreting these findings. Analytical validity refers to the ability to reliably and accurately measure CRP in saliva, which is supported by multiple studies demonstrating correlations between salivary and serum CRP concentrations [25,26,27,35,54]. In contrast, clinical utility requires evidence that salivary CRP improves disease detection, risk stratification, or patient outcomes beyond existing clinical tools. Although our meta-analysis confirms that salivary CRP is elevated in metabolic conditions, the substantial overlap in salivary CRP values between cases and controls and the absence of standardized thresholds preclude its use as a standalone diagnostic or screening tool at present [30,36].
No included studies evaluated the prognostic value of salivary CRP for incident metabolic syndrome, cardiovascular events, or diabetes progression, nor did they assess whether salivary CRP-guided interventions improve clinical outcomes [8,9,11]. Without prospective validation and clearly defined clinical action thresholds, salivary CRP remains a promising research biomarker rather than a clinically actionable test. This distinction is critical to avoid premature translation into practice without sufficient evidence.
Our findings are broadly consistent with recent narrative and systematic reviews on salivary biomarkers, which have highlighted the potential of salivary CRP while emphasizing the need for methodological standardization and cautious interpretation [35,37,63]. However, this meta-analysis extends previous work by providing the first quantitative synthesis of salivary CRP across metabolic disease phenotypes and by explicitly characterizing the magnitude and sources of heterogeneity that limit clinical application. By demonstrating that heterogeneity is intrinsic to the current evidence base, rather than a minor methodological inconvenience, this study reframes heterogeneity as a central finding that must be addressed before clinical implementation can be considered.
Several priorities for future research emerge from this analysis. First, studies should explicitly recruit participants meeting standardized diagnostic criteria for metabolic syndrome, as defined by international consensus guidelines, to allow condition-specific evaluation of salivary CRP [5,39]. Second, harmonization of saliva collection protocols and CRP assay methodologies is essential, including standardized timing, fasting status, storage conditions, assay sensitivity, and reporting units [24,25,26,27,28,29]. Third, rigorous control for confounding factors, particularly periodontal disease, should be incorporated through comprehensive oral examinations or validated inflammatory markers [37,60]. Finally, prospective longitudinal studies are needed to establish temporal relationships, define clinically meaningful thresholds, and determine whether salivary CRP predicts disease onset or progression or responds to therapeutic interventions such as weight loss, glycemic control, or anti-inflammatory treatments [6,7,18,19].
5. Conclusions
In conclusion, this meta-analysis provides exploratory evidence that salivary CRP tends to be elevated across a range of metabolic disorders, suggesting a possible association with systemic inflammatory burden related to metabolic dysfunction. The findings highlight the promise of salivary CRP as an accessible, non-invasive candidate biomarker that warrants further investigation. However, the between-study heterogeneity and variability in study design and measurement methods emphasize the need to standardize salivary CRP assessment. The inclusion of studies examining related but distinct metabolic conditions limits the specificity of inferences regarding MetS itself. Future high-quality studies employing harmonized definitions of metabolic syndrome, standardized salivary CRP assays, and prospective designs are required to clarify consistency, establish clinically meaningful thresholds, evaluate predictive performance, and determine whether salivary CRP has a role in metabolic risk stratification and early prevention strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Samson S.L. Garber A.J. Metabolic syndrome Endocrinol. Metab. Clin.20144312310.1016/j.ecl.2013.09.00924582089 · doi ↗ · pubmed ↗
- 2Huang P. A comprehensive definition for metabolic syndrome Dis. Model. Mech.2009223123710.1242/dmm.00118019407331 PMC 2675814 · doi ↗ · pubmed ↗
- 3Saklayen M.G. The Global Epidemic of the Metabolic Syndrome Curr. Hypertens. Rep.2018201210.1007/s 11906-018-0812-z 29480368 PMC 5866840 · doi ↗ · pubmed ↗
- 4Pigeot I. Ahrens W. Epidemiology of metabolic syndrome Pflügers Archiv.202547766968010.1007/s 00424-024-03051-739862247 PMC 12003477 · doi ↗ · pubmed ↗
- 5Alberti K.G.M. Zimmet P. Shaw J. The metabolic syndrome—A new worldwide definition Lancet 20053661059106210.1016/S 0140-6736(05)67402-816182882 · doi ↗ · pubmed ↗
- 6Hotamisligil G.S. Inflammation and metabolic disorders Nature 200644486086710.1038/nature 0548517167474 · doi ↗ · pubmed ↗
- 7Grundy S.M. Metabolic syndrome pandemic Arterioscler. Thromb. Vasc. Biol.20082862963610.1161/ATVBAHA.107.15109218174459 · doi ↗ · pubmed ↗
- 8Wilson P.W. D’Agostino R.B. Parise H. Sullivan L. Meigs J.B. Metabolic syndrome as a precursor of cardiovascular disease and type 2 diabetes mellitus Circulation 20051123066307210.1161/CIRCULATIONAHA.105.53952816275870 · doi ↗ · pubmed ↗