New and Investigational Treatment Options for Dermatomycosis in the Era of Antifungal Resistance
Aditya K. Gupta, Amanda Liddy, Tong Wang

TL;DR
This paper reviews new and investigational treatments for fungal skin infections, focusing on novel drugs, repurposed medications, and emerging technologies like nanotechnology.
Contribution
A scoping review of recent (past 10 years) novel antifungal treatments and platforms for dermatomycoses.
Findings
Olorofim and ME1111 are new drug classes targeting intracellular metabolism.
New azole agents like oteseconazole and fosravuconazole offer improved pharmacokinetics and broader antifungal activity.
Nanotechnology and antimicrobial peptides are promising for enhancing antifungal therapy and vaccine development.
Abstract
Superficial mycoses (dermatomycoses) are a growing healthcare concern due to antifungal resistance, particularly among aging and immunocompromised populations. Multiple efforts are underway to develop novel antifungals, including discovering new compounds with known or new mechanisms of action, extending indications or repurposing existing medications, and utilizing vaccination and nanotechnology platforms. Herein, we conducted a scoping review of novel antifungals for the treatment of dermatomycoses. An electronic literature search restricted to the past 10 years was performed in January 2026 using PubMed and Embase (Ovid). Olorofim and ME1111 represent novel drug classes that target intracellular metabolism. New agents belonging to the azole class demonstrate reduced drug–drug interactions (oteseconazole), a broader antifungal spectrum (voriconazole), and reduced pharmacokinetic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
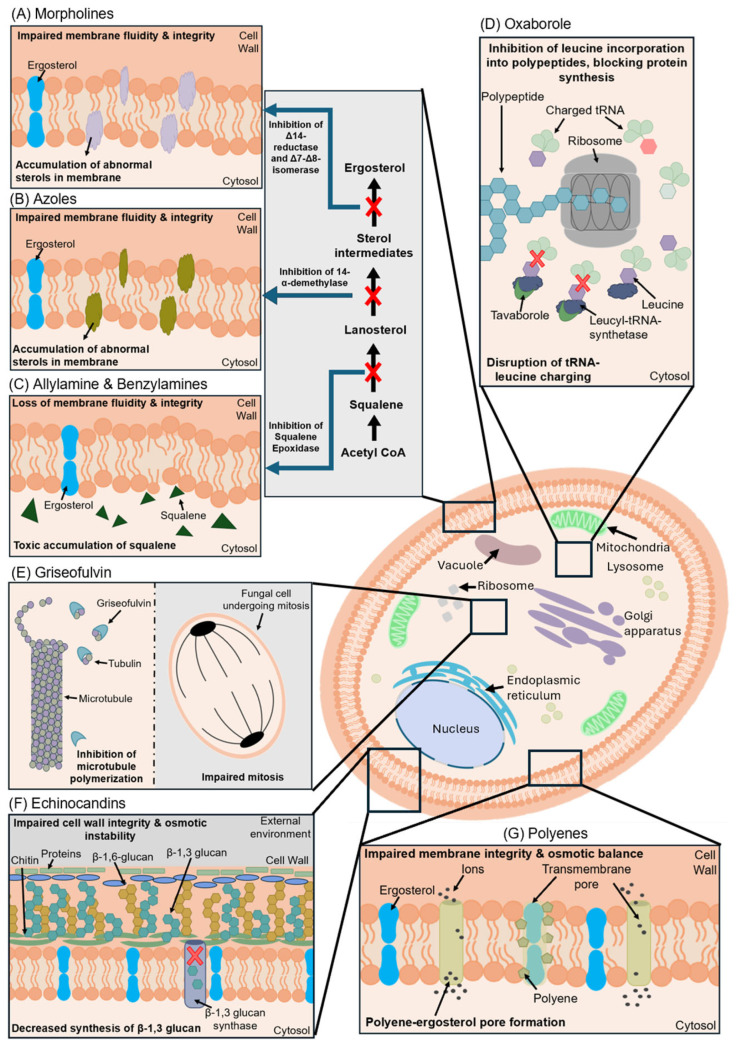 Figure 1
Figure 1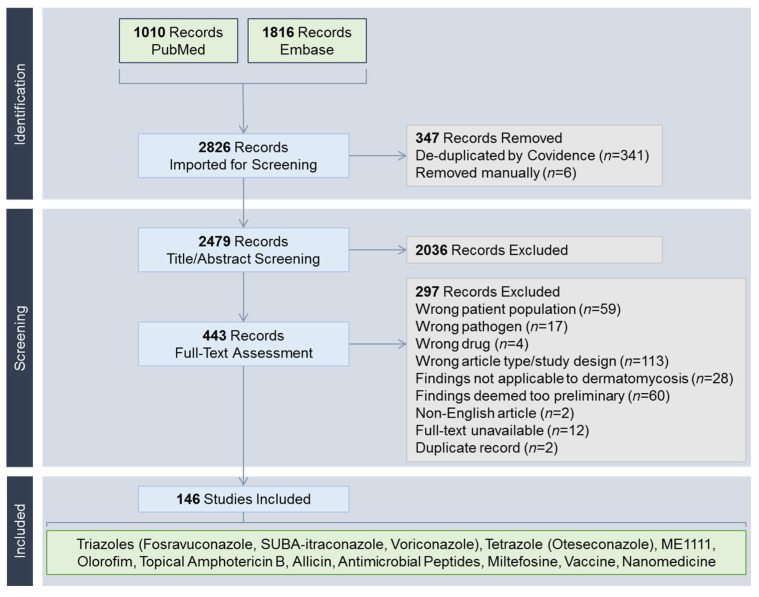 Figure 2
Figure 2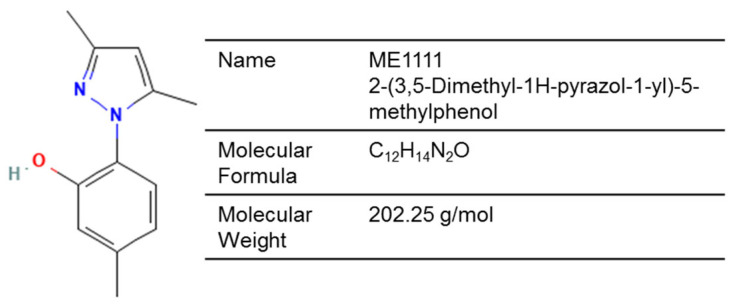 Figure 3
Figure 3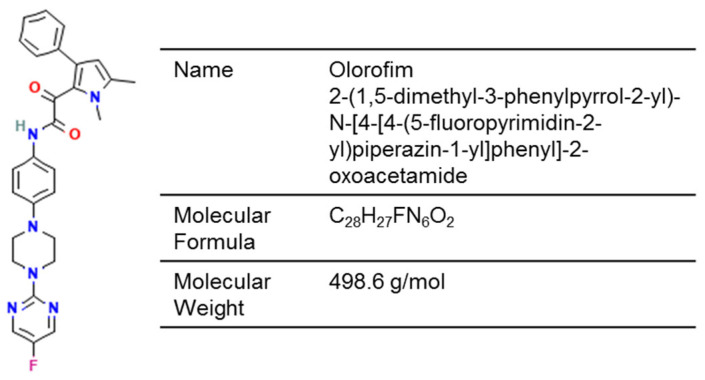 Figure 4
Figure 4 Figure 5
Figure 5 Figure 6
Figure 6 Figure 7
Figure 7 Figure 8
Figure 8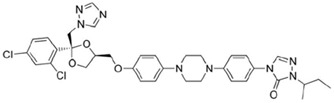 Figure 9
Figure 9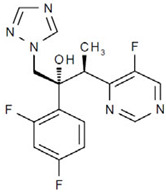 Figure 10
Figure 10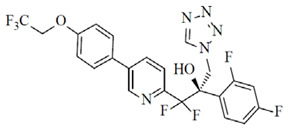 Figure 11
Figure 11| Compound | Target | Clinical Trial a | Phase (Population) | In Vitro Activity b | Topical | Key | ||
|---|---|---|---|---|---|---|---|---|
|
|
|
| ||||||
| Fosravuconazole | ERG11/CYP51 | Watanabe et al. [ | 3 (onychomycosis) | ✓ | ✓ | ✓ | ? | Reduced PK complexity |
| SUBA-ITZ | ERG11/CYP51 | Dhoot et al. [ | 2 (glabrous tinea) | ✓ | ✓ | ✓ | ? | Reduced PK complexity |
| Voriconazole | ERG11/CYP51 | Ali et al. [ | 2 (glabrous tinea) | ✓ | ✓ | ✓ | [ | Broad-spectrum antifungal activity |
| Oteseconazole | ERG11/CYP51 | Elewski et al. [ | 2 (onychomycosis) | ✓ | ? | ✓ | ? | Higher specificity for fungal CYP51 |
| ME1111 | Mitochondria | ? | - | ✓ | ? | ? | [ | Novel drug target |
| Olorofim (Orotomide) | Pyrimidine | ? | - | ✓ | ✓ | No activity | [ | Novel drug target |
| Allicin | Fungal cell and organelle membranes | ? | - | ✓ | ✓ | ✓ | [ | Phytocompound |
| NP213 | Fungal cytoplasmic membrane | Mercer et al. [ | 1 (onychomycosis) | ✓ | ✓ | ✓ | [ | Part of the host innate immunity |
| Miltefosine | Membrane lipids | ? | - | ✓ | ? | ✓ | [ | Repurposed antileishmanial medication |
| Agent | Approved Indication (Country) | PK/PD | Effects of Food | Drug–Drug |
|---|---|---|---|---|
|
| ||||
| Fosravuconazole [ | Onychomycosis caused by dermatophytes | AUC/MIC | No difference in systemic absorption (AUC0−t) between fed and fasted states | CYP3A substrates |
| SUBA-ITZ † [ | Invasive fungal infections: Blastomycosis (USA); Histoplasmosis (USA, Australia); Aspergillosis (USA, Australia); Candidiasis (Australia) | AUC/MIC | High-fat meal decreases steady-state absorption (Cmax, AUCtau) | CYP3A4 substrates |
| Voriconazole [ | Serious fungal and yeast infections, such as aspergillosis, scedosporiosis, fusariosis, candidemia, and deep tissue or esophageal candidiasis ** | AUC/MIC | High-fat meal reduces absorption (Cmax, AUCΤ) | CYP2C19, CYP2C9, and CYP3A4 inducers or inhibitors |
|
| ||||
| Oteseconazole [ | Recurrent vulvovaginal candidiasis in patients without reproductive potential (USA) | AUC/MIC | High-fat meal increases absorption (Cmax, AUC0–72h) | BCRP substrates |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNail Diseases and Treatments · Dermatology and Skin Diseases · Antifungal resistance and susceptibility
1. Introduction
Dermatomycoses represent an increasing global healthcare burden, due in part to the emergence of antifungal resistance [1,2]. Initially reported as sporadic cases prior to 2015, the issue of terbinafine resistance has since escalated into a public health concern following the outbreak of Trichophyton (T.) indotineae infections, which have demonstrated intercontinental spread [3]. Although typically regarded as mild infections, the epidemiological landscape of dermatomycoses is evolving, as reflected by recent reports of widespread, recalcitrant infections and invasive, systemic infections, particularly among immunocompromised populations [4,5,6]. Moreover, pathogens previously considered uncommon in the Global North may be emerging in new geographical regions, possibly related to climate change [7]. These developments underscore the need to investigate alternative treatment strategies.
A summary of antifungals currently approved by the U.S. Food and Drug Administration (FDA) is shown in Figure 1. The development of novel antifungals is a complex process that includes considerations of the drug target, pharmacodynamics (mode of action), pharmacokinetics including absorption, distribution, metabolism, and elimination, as well as dosage forms, off-target systemic toxicity concerns, and drug–drug interactions. For dermatomycosis, demonstration of in vitro efficacy (minimum inhibitory concentration [MIC]) alone does not accurately reflect clinical utility; rather, distribution, permeation, and retention in the stratum corneum relative to the MIC are also key indicators of efficacy [8,9]. Furthermore, agents with minimal risk of cross-resistance to terbinafine and azoles—such as those belonging to a new chemical class, with a novel target, and/or a new mode of action as per the World Health Organization's innovation criteria—are also relevant given the current global scenario [10].
Traditional approaches to developing antifungals can be broadly summarized as novel agents belonging to existing drug classes, agents with novel mechanisms of action, or formulation developments that address safety and/or bioavailability concerns. Off-label extension and drug repurposing are alternative strategies that reduce developmental costs, given that efficacy and safety profiles are already established, particularly for older agents with lapsed patents and without regulatory data protection. Recent technological advances may enable vaccination strategies as more virulence factors are discovered [11]. Nanoparticle systems can be applied either as new antifungal agents or as a topical delivery vehicle [12]. Beyond the scope of this review, non-pharmacological, device-based interventions such as photodynamic therapy theoretically bypass drug-resistance mechanisms and exert fungicidal effects via the localized induction of heat or oxidative stress [13]; furthermore, iontophoresis and ultrasound can enhance drug delivery across the nail plate for the treatment of onychomycosis [14]. In this scoping review, we collated literature from the past decade to provide a snapshot of novel antifungals under development for the treatment of dermatomycosis.
2. Materials and Methods
A scoping review was conducted on 21 January 2026 in accordance with the PRISMA recommendations (Open Science Framework: https://doi.org/10.17605/OSF.IO/JMC42 [accessed on 19 February 2026]) [15]. PubMed and Embase (Ovid) were searched with a restriction to publications from the past 10 years. The search strategy was based on the names or codes of investigational antifungals (from preclinical to clinical stages of development), as well as off-label antifungals not indicated for dermatomycoses, discussed in recently published reviews [16,17,18]. Emerging treatment modalities, including immunotherapies, vaccines, and nanomedicinal products, were also included. These terms were combined with the following keywords (including MeSH and Emtree terms): ‘dermatophytosis’, ‘dermatomycoses’, ‘fungal skin diseases’, ‘tinea’, or ‘ringworm’.
Search results were ported into Covidence (https://www.covidence.org/ [accessed on 21 January 2026]) for de-duplication and screening. The inclusion criteria were original studies of novel antifungals that demonstrated efficacy against dermatomycosis pathogens and/or showed favorable stratum corneum pharmacokinetics. Pharmacovigilance studies and reports on novel formulations relevant to dermatomycosis were also included. Novel agents supported by only in vitro susceptibility testing results were excluded. Non-pharmacological interventions (photodynamic therapy, laser) were also excluded. Fungal nomenclature was standardized according to recommendations by de Hoog et al. [19].
3. Results and Discussion
The search yielded 2826 records (Figure 2). Following full-text review, the following modalities were deemed to have sufficient pre-clinical and/or clinical evidence for discussion: fosravuconazole [20,21,22,23,24,25,26,27,28,29,30,31,32,33,34], super-bioavailable (SUBA) itraconazole [35,36,37,38,39,40,41,42,43,44,45], voriconazole [46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116], oteseconazole [117,118], ME1111 [119,120,121,122,123,124,125,126], olorofim [127,128,129], topical amphotericin B [130,131,132,133,134,135], allicin [136,137,138,139], antimicrobial peptides [140,141], miltefosine [142,143,144,145], vaccines [146], and nanomedicines [147,148,149,150,151,152,153,154,155,156,157,158,159,160,161,162,163,164,165]. A summary of newer antifungal compounds is shown in Table 1. Echinocandins (anidulafungin, caspofungin, micafungin, rezafungin) were not included due to their limited penetration into the stratum corneum relative to plasma concentrations, the necessity for parenteral administration, and the absence of novel formulation developments relevant to dermatomycosis [9].
3.1. Azoles
Azole antifungals exert their fungistatic effect through inhibition of sterol 14-α-demethylase (CYP51), a cytochrome P450 (CYP450) enzyme essential to ergosterol biosynthesis. By antagonizing this enzymatic step, azoles deplete the intracellular pool of ergosterol, thereby reducing the structural integrity and fluidity of the fungal cell membrane. Broadly, the clinical use of azoles faces issues of pharmacokinetic variability that can lead to supra- or subtherapeutic levels, as well as drug–drug interactions due to the off-target inhibition of human CYP450 enzymes, which can cause hepatotoxicity.
Triazoles—characterized by three nitrogen atoms in the azole ring (itraconazole, fluconazole)—represent the mainstay systemic treatment option for dermatomycoses [166]. By contrast, imidazoles—with two nitrogen atoms—generally show a greater risk of systemic toxicity and are therefore largely limited to topical use (e.g., ketoconazole, sertaconazole, fenticonazole, oxiconazole). Compared with triazoles, tetrazoles—with four nitrogen atoms—are designed to further reduce off-target effects on the human CYP51A isoform, thereby improving the safety profile. A summary of newer triazole and tetrazole agents is shown in Table 2.
3.1.1. Fosravuconazole
Fosravuconazole is a triazole and a prodrug of ravuconazole with improved lipophilicity and absorption while exhibiting reduced off-target effects on human CYP3A4 compared with itraconazole. Unlike itraconazole, its total systemic absorption (AUC_0−t_) is not affected by food intake [168]. Following oral administration, fosravuconazole is converted to ravuconazole, which accumulates in nails, reaching a concentration of 120.1 ng/g in the toenails of onychomycosis patients after receiving 100 mg/d for 12 weeks [168]. Beyond its use in onychomycosis, recent research has highlighted its utility in treating glabrous tineas, tinea barbae, tinea capitis, kerion celsi, and resistant cases [23,25,26,29,30,33,34].
In 2018, a fosravuconazole 100 mg capsule was approved for the treatment of onychomycosis in Japan [168]. In a phase 3 trial, 153 patients with moderate-to-severe onychomycosis—positive for T. rubrum or T. mentagrophytes—were randomized to receive either fosravuconazole 100 mg/d or placebo for 12 weeks [20]. At week 48, 59.4% (60/101) of patients receiving fosravuconazole achieved complete cure (clinical resolution with negative KOH microscopy) compared with 5.8% (3/52) in the placebo arm. Common drug-related adverse events were gastrointestinal symptoms [20]. Liver enzyme elevations (ALT, AST, γ-GTP) occurred at a rate of 18.8% (19/101), which resolved after treatment completion [20]. Follow-up studies have reaffirmed its efficacy in treating total dystrophic onychomycosis, as well as in hemodialysis patients, patients nonresponsive to topical antifungals, and infections complicated by dermatophytomas [21,24,27,28].
In onychomycosis patients with suboptimal response or experienced recurrence, retreatment with fosravuconazole 100 mg/d for 12 weeks was not associated with serious adverse events or new safety signals [31,32]. However, a retrospective analysis of 36 onychomycosis patients identified a risk of renal injury (27.8% [10/36]), defined as either an increase in serum creatinine by ≥0.3 mg/dL or ≥50%, or a decrease in estimated glomerular infiltration rate of ≥50% [22]. The exact cause is unclear; however, being on angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers was identified as a risk factor [22].
3.1.2. Super-Bioavailable (SUBA) Itraconazole
The SUBA technology was developed to incorporate itraconazole into a pH-dependent polymeric matrix, which enhances dissolution and targets drug release in the proximal small intestine. Since its absorption is not dependent on an acidic gastric environment, unlike conventional itraconazole, inter-patient pharmacokinetic variability is also reduced. Compared to conventional itraconazole, SUBA-itraconazole has a relative bioavailability of 173% with 21.3% less interpatient variability [176]. Furthermore, it exhibits higher tissue distribution to the stratum corneum compared to the deeper epidermis or dermis [37]. In the USA, a SUBA-itraconazole 65 mg capsule is approved for the treatment of invasive fungal infections, but it is not recommended for use in dermatomycosis [169]. By contrast, a SUBA-itraconazole 50 mg capsule is approved in Australia for the treatment of superficial and systemic mycoses [167]. In India, SUBA-itraconazole is actively investigated as a treatment for recalcitrant dermatophytosis, and is available as 50 mg, 65 mg, 100 mg, or 130 mg capsules [35,39].
In dermatomycosis patients administered either SUBA-itraconazole 130 mg/d or conventional itraconazole 200 mg/d for 4 weeks, similar serum and sebum concentrations were observed, suggesting bioequivalence [36]. Head-to-head studies confirmed a similar degree of clinical and mycological response in patients who received SUBA-itraconazole 100 mg/d or 130 mg/d compared to conventional itraconazole 200 mg/d, while a less favorable response was observed in patients who received conventional itraconazole 100 mg/d [38,43,45]. A randomized trial compared moderate-to-severe toenail onychomycosis patients receiving either SUBA-itraconazole 100 mg/d or conventional itraconazole 200 mg/d for 12 weeks [167]. At week 24, SUBA-itraconazole was shown to be non-inferior to conventional itraconazole. Another study demonstrated that SUBA-itraconazole 130 mg/d may be superior to SUBA-itraconazole 100 mg/d [40]; however, there are conflicting findings and opinions on the optimal starting dosage due to its non-linear pharmacokinetics [35,39,41]. Overweight or obesity (BMI ≥ 25 kg/m^2^) was not a significant factor in treatment response [42].
None of the identified studies in dermatomycosis patients reported serious adverse events or acute liver injuries. In a case report, an adolescent tinea cruris patient developed a probable case of drug eruption (intertriginous and flexural exanthema) after receiving SUBA-itraconazole 130 mg/d [44]. Regardless of formulation, itraconazole use also carries a risk of cardiac dysfunction due to possible mitochondrial toxicity [169]; in a retrospective case review, patients experiencing cardiac events—including edema, heart failure, and worsening or new hypertension—were mostly older adults (average age: 66 years) with an average serum drug level of 5.2 µg/mL [177]. Similar to conventional itraconazole, therapeutic drug monitoring (TDM) can help tailor dosage to prevent supra- or subtherapeutic levels and reduce systemic toxicity risks. Although SUBA-itraconazole may be taken with or without food [167], its bioavailability is reduced by 26.9% in the fed state compared to the fasted state, which can lead to variable clinical outcomes when food intake is not specified in treatment protocol [176]. The U.S. FDA still recommends that SUBA-itraconazole be taken with food [169].
3.1.3. Voriconazole
Voriconazole is a broad-spectrum triazole agent with significant inter- and intrapatient pharmacokinetic variability (e.g., CYP2C19 polymorphisms, food intake, drug–drug interactions), which can lead to sub- or supratherapeutic drug levels and unpredictable treatment outcomes, warranting TDM and consultation with an infectious disease specialist. In 2002, voriconazole (tablets, oral suspension, intravenous injection) was approved in the USA for the treatment of invasive fungal infections, including those caused by Aspergillus, Fusarium solani, Scedosporium apiospermum, and Candida [170]. Although voriconazole tablets have recently been tried off-label for recalcitrant dermatomycosis, its utility is still debated due to high medication costs, lack of information on skin/nail pharmacokinetics, and safety concerns, including photosensitivity and photocarcinogenesis. To minimize systemic toxicity risks, recent research has developed topical voriconazole formulations with demonstrated permeation across the skin and nails.
Antifungal susceptibility testing has demonstrated broad-spectrum activity against isolates from dermatomycosis patients. For onychomycosis caused by non-dermatophyte molds, voriconazole has demonstrated efficacy against Aspergillus spp. and Fusarium spp. (F. solani species complex, F. fujikuroi species complex, F. oxysporum), including in strains with high terbinafine, griseofulvin, or fluconazole MICs [46,47,55,69]. Candida isolates from onychomycosis patients also exhibited high susceptibility, including C. albicans and non-albicans Candida (C. parapsilosis, C. krusei, C. tropicalis) [64,65,113]. Additionally, voriconazole was effective in vitro against dermatophytes [48,49,50,54,56,57,58,59,60,62,65,73,74,76,80,91,102,115,116], including T. rubrum, the T. mentagrophytes complex, and, importantly, T. indotineae resistant to standard antifungals [51,52,53,61,63,66,67,68]. However, a cautious approach is warranted, given that itraconazole resistance may be emerging in dermatophytes, which can confer cross-resistance to voriconazole [52,70,75,78,86,88,93]. The indiscriminate dual use of azoles in agriculture and medicine has been linked to resistance development in Fusarium [72]. A recent study also reported reduced voriconazole and fluconazole susceptibility in non-albicans Candida causing onychomycosis [71].
After serial dosing in a guinea pig model, voriconazole was detected in skin biopsies at concentrations nearly twice as high as in blood, while skin microdialysates exhibited lower concentrations than in blood [178]. Clinically, oral voriconazole has been tried successfully in recalcitrant glabrous tinea and onychomycosis, albeit with significant variations in dosage and duration, as well as unclear safety concerns such as abnormal vision and liver enzyme elevations requiring regular monitoring. In a randomized study, recalcitrant tinea corporis/faciei patients received a loading dose of voriconazole 800 mg on day 1, followed by 400 mg/d for a total of 6 weeks [79]. Compared with patients who received itraconazole 200 mg/d for 6 weeks, the voriconazole group achieved significantly higher mycological (negative culture and KOH microscopy; 86.7% [26/30] vs. 56.7% [17/30]) and complete cure rates (clinical resolution with mycological cure; 83.3% [25/30] vs. 53.3% [16/30]) by month 6, with abnormal vision occurring in 6.7% (2/30) of patients and without laboratory abnormalities [79]. A similar study of 40 patients reported clinical resolution after administering the same regimen for a shorter duration of 2 weeks [82]. In the absence of a loading dose, 200 mg twice daily and 200 mg/d were also tried successfully when administered for 2 weeks or more [81,83,85,93]. For onychomycosis patients, 200 mg twice daily for 3 months was tried for fingernails [77], and 200 mg twice daily on day 1 followed by 200 mg/d for 3–4 months was given to treat toenails [87]. Voriconazole was generally reported as well-tolerated with self-limiting adverse events; however, a large study of 227 tinea corporis/cruris patients receiving 200 mg twice daily for 2 weeks reported a 4.9% frequency of developing jaundice [99], reinforcing the issue of pharmacokinetic variabilities and the need for TDM to tailor dosage.
Safety Considerations and Novel Topical Formulations
TDM is strongly recommended for voriconazole due to its complex, non-linear pharmacokinetics [170]. Following oral administration, the maximum plasma concentration (C_max_) is reached after 1–2 h, with 96% bioavailability and extensive tissue distribution [170]. It is metabolized by CYP450 enzymes, particularly by CYP2C19, with voriconazole-N-oxide being the main metabolite that does not show significant antifungal activity [170]. Due to saturation of its metabolism, the rate of systemic exposure increases disproportionately with dose [170]. Furthermore, a significant portion of the population is poor metabolizers—15–20% in Asians, 3–5% in Caucasians and Blacks—attributed to CYP2C19 genetic polymorphisms [170]. The absorption of voriconazole is further complicated by food intake, and it is recommended to fast for at least one hour before and one to two hours after administration [170]. For treating invasive fungal infections, a serum concentration of ≥1.0 µg/mL is correlated with efficacy, while a supratherapeutic concentration of >4.0 µg/mL is correlated with hepatotoxicity [89,92].
In view of systemic toxicity concerns, topical voriconazole formulations offer a promising alternative. Due to its poor water solubility, the addition of penetration enhancers or a hydrophilic vehicle has been investigated [101]. Given the lipophilic nature of the stratum corneum, voriconazole loaded in a lipid matrix has been demonstrated to penetrate the stratum corneum down to the deep dermis [100]. A hydrogel formulation containing menthol (a lipophilic enhancer) has been shown to improve both the solubility and skin permeability of voriconazole, with in vitro efficacy against fluconazole-resistant Candida albicans [103]. A voriconazole 1% cream was also tried successfully in a terbinafine-resistant T. indotineae patient with an intracutaneous drug concentration of 0.5 µg/mL [114].
To maximize drug-tissue contact and improve drug-release kinetics, nanoparticle-based delivery systems have been explored for topical voriconazole administration. This includes chitosan-based nanoparticles [105], ethosomes [106,107], hyalurosomes [108], invasosomes [109], and transethosomes [110]. A liposomal formulation has demonstrated in vitro efficacy against T. rubrum, with skin permeation and follicular retention [111]. For nail delivery, the addition of thioglycolic acid—a reducing agent targeting the disulfide bonds in hard keratins—into a lipid-based formulation (nanomicelles) significantly increased drug retention by softening and hydrating the nail plate and disrupting the lipid barrier [112].
Photosensitivity reactions are another safety concern for voriconazole, with an almost 50-fold higher odds compared to other medications according to the U.S. FDA Adverse Events Reporting System [90]. Through its chromosomal localization that disrupts the initiation of DNA nucleotide excision repair, prolonged voriconazole use is linked to benign and malignant skin neoplasms, including nevi, actinic keratosis, and squamous cell carcinoma (SCC) [94]. The risk of SCC is further increased in rapid CYP2C19 metabolizers; this is postulated to result from the photoreaction of voriconazole-N-oxide that induces oxidative DNA damage [95]. The risk quantification remains unclear for the treatment of dermatomycosis, as voriconazole-related SCC cases generally occur in immunocompromised populations following prolonged treatment [96,97,98]. Consequently, patients receiving voriconazole should be advised to minimize direct sunlight exposure and use photoprotection [170].
3.1.4. Oteseconazole
Oteseconazole (VT-1161) is a tetrazole agent that demonstrated greater target specificity for fungal CYP51. Both itraconazole and oteseconazole showed similar binding affinities for CYP51 from T. rubrum—preventing the demethylation of eburicol—compared with fluconazole and ketoconazole [117]. Similar findings were shown with Candida albicans CYP51 [179]. Furthermore, oteseconazole showed no evidence of binding to the heme iron of human CYP51, in contrast to clotrimazole, fluconazole, itraconazole and voriconazole [179].
In the USA, oteseconazole was approved in 2022 for the treatment of recurrent vulvovaginal candidiasis (RVVC) in patients without reproductive potential [174]. Across three phase 3 trials, RVVC patients receiving oteseconazole—either alone or sequentially with fluconazole—were significantly less likely to experience acute episodes than those receiving placebo [174]. In a phase 2 trial evaluating oteseconazole for the treatment of distal lateral subungual onychomycosis [118], a total of 259 patients were randomized to receive a 2-week induction dose of either 300 mg/d or 600 mg/d, followed by a weekly maintenance dose of either 300 mg or 600 mg, respectively, for 10 or 22 weeks. Compared to the placebo arm, patients receiving oteseconazole achieved significantly higher complete cure rates (clinical resolution with a negative KOH microscopy and culture; 40.7–45.3%) at week 60 [118]. Treatment-related adverse events were primarily gastrointestinal symptoms, with no abnormalities in liver function parameters or QT intervals [118].
3.2. ME1111
ME1111 is being investigated as a topical onychomycosis treatment due to its favorable nail pharmacokinetics and antifungal effects—via inhibition of succinate dehydrogenase (complex II)—that disrupt mitochondrial function (Figure 3) [119,121]. Its 10% solution has shown improved permeation of full-thickness human nails ex vivo when compared with ciclopirox 8% or amorolfine 5% [120]. After repeated once-daily applications for 14 days, significant distribution was detected in the ventral nail plate and the subungual space of human toenails and fingernails [122,123]. Distribution to the stratum corneum was also demonstrated in a guinea pig model [126].
Antifungal susceptibility testing has demonstrated its in vitro efficacy against T. rubrum, T. mentagrophytes complex, T. tonsurans, and Epidermophyton floccosum [120,124]. In a guinea pig model infected with the T. mentagrophytes complex, ME1111 10% applied once daily for 7 days induced significant clinical and mycological response compared with placebo [125], and exhibited a dose-dependent relationship [126].
3.3. Olorofim (F901318)
Olorofim is an investigational orotomide compound with activity against a specific spectrum of molds and dimorphic fungi, but not yeasts and Mucorales (Figure 4) [175]. It disrupts pyrimidine biosynthesis by inhibiting fungal dihydroorotate dehydrogenase (DHODH), leading to downstream fungicidal effects including inhibition of germination and hyphal growth, cell wall disruption, and cell cycle arrest.
Initially developed as a treatment for azole-resistant Aspergillus fumigatus [180], olorofim may also bind to dermatophyte DHODH due to overlap in the conserved amino acid residues required for binding [127]. In a guinea pig model, olorofim was effective in treating dermatophytosis caused by Nannizia gypsea [127]. Olorofim also demonstrated favorable in vitro efficacy against Trichophyton spp. and Microsporum canis, including strains exhibiting terbinafine and itraconazole resistance, as well as T. indotineae [128,129].
In the treatment of invasive fungal infections, the antifungal activity of olorofim is time-dependent, as reflected by its C_min_/MIC [175]. Olorofim may cause drug–drug interactions due to its metabolic pathway involving multiple CYP450 enzymes and its inhibition of CYP3A4 [175]. In a phase 1 trial of eight healthy volunteers, olorofim tablets (360 mg/d for 10 days) did not lead to serious adverse events and the average plasma trough level was 1–2 µg/mL, albeit with liver enzyme elevation (ALT) occurring in one patient [181].
3.4. Topical Amphotericin B
Polyenes, such as amphotericin B, exhibit a broad spectrum of fungicidal activity by binding to ergosterol, which forms transmembrane pores and leads to the leakage of intracellular contents. However, the clinical use of amphotericin B is significantly limited by systemic toxicity, particularly nephrotoxicity. Although lipid-based formulations have improved its safety profile, issues related to stability, bioavailability, and the need for parenteral administration—as well as limited tissue distribution in the skin—restricts their use in dermatomycosis patients [9].
Topical delivery strategies offer a promising alternative; however, their development is complicated by the compound’s high molecular weight, which impedes its penetration across the skin barrier. A deformable liposomal amphotericin B formulation was developed, incorporating an edge activator to increase membrane elasticity, allowing the liposomes to pass through smaller pores [130]. Using human skin explants, this formulation exhibited permeation across the stratum corneum and into the deeper epidermis [130]. Nano-scaled lipid carriers for amphotericin B have also demonstrated in vitro efficacy against Trichophyton spp., including T. indotineae [131,132]. To further facilitate skin permeation, a dissolvable microneedle patch was developed, allowing permeation across both the epidermal and dermal layers [135].
For treating onychomycosis, Souza et al. incorporated amphotericin B into a commercial nail lacquer, demonstrating enhanced nail permeation compared to a control solution (amphotericin B in dimethyl sulfoxide), as well as in vitro efficacy against Candida spp. (albicans and non-albicans) [133]. In a pilot study, 15 onychomycosis patients were treated with a topical nanoliposomal amphotericin B 0.4% gel, applied twice daily for 12 weeks for fingernails or 36 weeks for toenails [134]. At week 36, 73.3% (11/15) of patients achieved complete cure (clinical resolution with negative KOH microscopy and culture), with application-site adverse events including transient nail discoloration occurring in all treated patients and onycholysis occurring in one patient [134].
3.5. Other Investigational Agents
3.5.1. Allicin
Allicin is a sulfur-based phytocompound derived from garlic that has demonstrated fungistatic effects in vitro against dermatophytes and Candida, including disruption of germination and hyphal growth in Trichophyton spp., as well as protective effects on keratinocytes (Figure 5) [182]. In Candida guilliermondii and Rhodotorula mucilaginosa isolates from an onychomycosis patient, allicin penetrated cell and organelle membranes, resulting in cytoplasmic disruption and nuclear destruction [138]. Additionally, in keratinocytes challenged by reactive oxygen species (ROS), allicin demonstrated a protective effect against apoptosis and attenuated the pro-inflammatory response [137].
In Microsporum canis isolates from tinea capitis patients, allicin exhibited synergistic interactions with terbinafine and itraconazole [136]. A new formulation delivering allicin in a nanoparticle carrier mixed with hydrogels has been described, which may improve skin permeability and release kinetics for topical applications [139].
3.5.2. Antimicrobial Peptides
Keratinocytes secrete antimicrobial peptides as part of the inmate immune response against dermatophytes [183]. Based on antimicrobial peptides found in onychomycosis patients, NP213 was developed for topical application, demonstrating effective nail permeation due to its cationic property and resistance to proteases, as well as in vitro fungicidal activity against T. rubrum through disrupting the cytoplasmic membrane (Figure 6) [141]. In a phase 2a trial, topical NP213 was administered once daily in 47 onychomycosis patients for 4 weeks [140]. Based on the per-protocol population, patients receiving NP213 achieved a significantly higher mycological cure rate (culture-negative) of 56.5% (13/23) by month 12 compared to no cured cases with the placebo.
3.5.3. Miltefosine
Miltefosine, an alkyl phospholipid compound originally developed as a cancer treatment, was repurposed for the treatment of leishmaniasis in 2014 (Figure 7) [184]. Its proposed mechanisms of action include interactions with membrane lipids, ROS generation via the inhibition of cytochrome c oxidase, and induction of apoptosis [184]. Miltefosine has also demonstrated therapeutic potential against infections caused by Fusarium, Candida, and dermatophytes [185,186,187]. However, its oral administration is complicated by gastrointestinal side effects.
A nanoparticle-based formulation (miltefosine niosomal gel 1%)—with improved stability and drug-release kinetics—was developed and tested in a guinea pig model of T. indotineae infection [142]. Compared to untreated animals or those treated with the vehicle or oral terbinafine, miltefosine niosome gel 1% led to improved clinical and mycological responses, corroborated by histopathologic examination [142]. Other similar formulations under development include a dissolvable microneedle patch for intradermal administration of niosomes, as well as topical transfersome and lipid-based preparations [143,144,145].
3.6. Vaccines
Although fungal antigens have been discovered, development of antifungal vaccines faces challenges related to cost-effectiveness and uncertain protection in immunocompromised populations in whom invasive infections are more frequent [11]. For dermatophytes, the existence of natural immunity is supported by in vitro evidence of CD4^+^ and CD8^+^ T-cell proliferation and cytotoxic activity in patients recently recovered from acute dermatophytosis, which clinically manifests as a delayed-type hypersensitivity reaction [188]. Similarly, dermatophyte reinfection in animals has been associated with faster disease clearance and infiltration of peripheral blood mononuclear cells [189].
Given the increasing global prevalence of dermatomycosis—estimated to have affected 1.7 billion individuals in 2021—vaccine development for the general population could represent a cost-effective strategy [1]. Furthermore, therapeutic vaccines may help curb the spread of antifungal-resistant species, such as T. indotineae [4], by augmenting the host immune response to aid antifungal treatments. Using live and inactivated vaccines prepared from crude extracts of T. mentagrophytes, T. verrucosum, and Microsporum canis, Abo-Elyazeed et al. demonstrated a protective response in a guinea pig model, evidenced by the induction of dermatophyte-specific IgG and delayed-type skin hypersensitivity reactions [146]. Further isolation of protein fractions containing exo-keratinases confirmed their antigenic role in eliciting immune responses in vaccinated animals [146].
Subtilisin 6, also known as Tri r 2, is a serine protease expressed by Trichophyton spp. during in vivo infection and has been shown to elicit a protective T-cell response, as evidenced by delayed-type hypersensitivity reactions [190,191,192]. Notably, an immunodominant epitope was identified that induced lymphoproliferation and interferon-gamma (IFN-γ) secretion from peripheral blood mononuclear cells in healthy individuals, suggesting its potential as a vaccine target [193]. Further genomic investigations may help in developing a polyvalent vaccine that broadly targets the subtilisin family of endopeptidases [194].
3.7. Nanomedicines
In dermatomycosis, the site of infection—stratum corneum—presents a challenge for both drug penetration and retention. While topical antifungals are commonly used, their utilities may vary when applied on densely packed, hard keratins like nails or hyperkeratotic skin, and they are generally used in patients without extensive skin involvement. In contrast, oral antifungals like terbinafine and itraconazole distribute through the sebum and are retained in the skin by adhering to keratins, while fluconazole penetrates the stratum corneum via diffusion from the capillaries [8]. However, oral antifungals carry systemic toxicity risks and drug–drug interactions. Nanotechnology—involving the manipulation of particles ranging from 1 to 100 nm in size—is an active area of research that can be applied either directly, as new antifungals (e.g., metal nanoparticles), or in the formulation of traditional antifungals to improve their pharmacokinetics (e.g., liposomes) [12].
Metal nanoparticles have been investigated for their direct fungicidal mechanisms, potentially through the induction of oxidative stress. This strategy shows promise in bypassing common antifungal resistance mechanisms, such as alterations in ergosterol biosynthesis enzymes (e.g., squalene epoxidase mutations and terbinafine resistance); however, it remains uncertain whether they can be effective as monotherapies. Against T. rubrum, topically applied nanoparticles that release nitric oxide have demonstrated efficacy in a mouse model as well as in vitro synergistic interactions with efinaconazole [152,160]. Application of silver and zinc oxide nanoparticles has been shown to inhibit the in vitro growth of the T. mentagrophytes complex and T. verrucosum, likely by reducing keratinase activity, preventing ergosterol synthesis, and disrupting the integrity of the mycelial network [159]. For cutaneous candidiasis, a gold nanoparticle solution demonstrated a similar degree of clinical efficacy in infected mice compared with topical nystatin [165].
For glabrous tineas, nanoparticle systems for antifungals currently indicated for oral or intravenous routes of administration with safety concerns—such as voriconazole (see Section Safety Considerations and Novel Topical Formulations) and amphotericin B (see Section 3.4)—are being actively investigated. Furthermore, in a mouse model, a ketoconazole-based nanoparticle system was developed for intradermal administration [150], as the oral formulation has been restricted or discontinued due to idiosyncratic hepatotoxicity. Compared to the topical ketoconazole 2% cream, this formulation showed increased dermal drug retention without significant inflammatory infiltrations [150]. Similar efforts have been reported in developing ketoconazole in nanoparticle gel formulations, terbinafine and itraconazole in lipid nanoparticles, and itraconazole nanocrystals in a dissolvable microneedle patch [153,154,155,156,157].
For onychomycosis, nanoparticle systems for ciclopirox, efinaconazole, ketoconazole, and griseofulvin have demonstrated enhanced nail permeation and ex vivo efficacy against nails infected with T. rubrum, the T. mentagrophytes complex, and/or Candida albicans [147,148,151,162]. Lipid nanoparticles, chitosan nanoparticles, and hydrogel embedded with polymeric nanospheres have been designed to incorporate terbinafine [158,163,164]. In a randomized, double-blind trial, 20 onychomycosis patients applied terbinafine-loaded lipid nanoparticle 1% gel twice daily for 2 months [161]. Compared to patients who received the standard terbinafine 1% cream or vehicle, a significant increase in clinical improvement was observed, albeit without differences in mycological response, possibly due to terbinafine-resistant strains [161].
Interestingly, nanoparticles may also be applied as a disinfectant against dermatophytes. In an effort to prevent infection recurrence or relapse, sock pieces coated with a zinc oxide nanoparticle 2% solution were incubated with dermatophyte isolates from tinea pedis patients [149]. A reduced number of viable isolates was observed compared to the control without co-incubation of sock pieces [149].
With growing interest in this field, the toxicity profile of nanomedicinal products remains to be fully examined. In addition to possible hypersensitivity reactions, metal nanoparticles can induce oxidative cellular damage associated with neurotoxicity and nephrotoxicity [195,196]. Accidental exposure to aerosolized nanoparticles—such as through inhalation or dermal absorption (skin and eyes)—may be associated with chronic toxicity [197]. Further mechanistic and clinical evaluations are warranted.
4. Conclusions
Our review of the current literature shows multiple novel avenues for developing dermatomycosis treatments, which can be categorized as (a) agents with innovative modes of action targeting intracellular metabolism (olorofim, ME1111) or inducing oxidative stress ([topical] nanoparticles); (b) a tetrazole agent with reduced drug–drug interactions (oteseconazole); (c) new and off-label extensions of triazole agents with reduced pharmacokinetic complexities (fosravuconazole, SUBA-itraconazole) or a broader antifungal spectrum (voriconazole); (d) a repurposed antileishmanial drug (miltefosine); (e) an antimicrobial peptide derived from the natural host immune response (NP213); (f) a biologically active phytocompound (allicin); (g) a vaccination strategy targeting dermatophyte virulence factors (keratinases); and (h) topical formulation developments—some incorporating nanotechnology—that potentially enable the safer use of antifungals while increasing bioavailability (amphotericin B, ketoconazole, voriconazole).
A universal challenge in developing traditional antifungal compounds is the risk of toxicity due to similarities in the cellular and biochemical features of humans and fungi. To this end, novel agents targeting virulence factors (e.g., subtilisins), therapeutic vaccines, or other immunotherapies (e.g., IFN-γ) show promise. For treating resistant strains, agents that block resistance mechanisms—such as efflux pump inhibitors or heat shock protein 90 inhibitors—represent a novel adjuvant treatment strategy not covered in the present review [198,199]. In contrast to the antifungal development pipeline for invasive fungal infections, topical agents have a unique role in the treatment of dermatomycoses as they may enhance bioavailability while posing a lower risk of systemic toxicity and drug–drug interactions, warranting further research into nanoparticle systems.
Although the worldwide emergence of antifungal resistance calls for the expansion of our therapeutic arsenal, identifying microbiological resistance in dermatophytes is complicated due to the lack of clinical breakpoints, which hinders the evaluation of cross-resistance risks for novel antifungals. Recent epidemiological cut-off values proposed for the standard broth microdilution method, using protocols by the Clinical & Laboratory Standards Institute and the European Committee on Antimicrobial Susceptibility Testing, can help in the preclinical evaluation of drug candidates [52,200]. When novel agents enter clinical testing, variations in trial design—such as endpoint definitions (e.g., mycological cure determined by direct microscopic examination and/or culture) and follow-up intervals—can limit comparability between studies. The former reflects ongoing limitations in fungal testing capacity across healthcare settings, including, but not limited to, resource-constrained settings. Technological advances such as real-time PCR, which do not rely on obtaining a culture, may improve the efficiency of patient selection and outcome evaluation. Overall, more work is needed to establish a clear regulatory pathway as more novel antifungals enter the developmental pipeline. This review is also limited by potential publication bias, as trial results may remain unpublished and drug candidates may be terminated without notice. Greater transparency and collaboration should be encouraged to allow more drug candidates to enter the clinical development pipeline.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Li D. Fan S. Zhao H. Song J. Guo L. Li W. Xu X. Li Q. Worldwide Trends and Future Projections of Fungal Skin Disease Burden: A Comprehensive Analysis from the Global Burden of Diseases Study 2021 Front. Public Health 202513158022110.3389/fpubh.2025.158022140535451 PMC 12174046 · doi ↗ · pubmed ↗
- 2Lockhart S.R. Chowdhary A. Gold J.A.W. The Rapid Emergence of Antifungal-Resistant Human-Pathogenic Fungi Nat. Rev. Microbiol.20232181883210.1038/s 41579-023-00960-937648790 PMC 10859884 · doi ↗ · pubmed ↗
- 3Rhodes J. Hui S.T. Dellière S. Summerbell R.C. Scott J.A. Kaur A. Barton R.C. Leitao R. Hemmings S. Goiriz R. Emerging Terbinafine-Resistant Trichophyton indotineae between 2018 and 2023: A Multinational Genomic Epidemiology Study Lancet Microbe 2026710127310.1016/j.lanmic.2025.10127341581521 · doi ↗ · pubmed ↗
- 4Khurana A. Sharath S. Sardana K. Chowdhary A. Clinico-Mycological and Therapeutic Updates on Cutaneous Dermatophytic Infections in the Era of Trichophyton indotineae J. Am. Acad. Dermatol.20249131532310.1016/j.jaad.2024.03.02438574764 · doi ↗ · pubmed ↗
- 5Galili E. Barzilai A. Lev A. Amit S. Barel O. Lubitz I. Gazit Z. Lyakhovitsky A. Somech R. Shemer A. Genetic, Immunological and Clinical Assessment of Isolated Chronic Recalcitrant Dermatophytosis: A Prospective Study Br. J. Dermatol.202519397898610.1093/bjd/ljaf 26940663635 · doi ↗ · pubmed ↗
- 6Gupta A.K. Wang T. Susmita Saunte D.M.L. Hay R. Piguet V. Deep and Disseminated Dermatophytosis in Immunocompromised Populations—A Systematic Review J. Eur. Acad. Dermatol. Venereol.2025 In press 10.1111/jdv.7011541104791 · doi ↗ · pubmed ↗
- 7Gupta A.K. Thornbush M. Wang T. Climate Change, Natural Disasters, and Cutaneous Fungal Infections Int. J. Dermatol.2025641349135510.1111/ijd.1790840506838 PMC 12256753 · doi ↗ · pubmed ↗
- 8Sardana K. Arora P. Mahajan K. Intracutaneous Pharmacokinetics of Oral Antifungals and Their Relevance in Recalcitrant Cutaneous Dermatophytosis: Time to Revisit Basics Indian J. Dermatol. Venereol. Leprol.20178373073210.4103/ijdvl.ijdvl_1012_1628936991 · doi ↗ · pubmed ↗