Smart Drug-Delivery Approaches for Enhanced Management of Comorbid Conditions in Alzheimer’s Disease
Gabriela-Dumitrita Stanciu, Ivona Costachescu, Camelia Dascalu, Bogdan-Ionel Tamba

TL;DR
This paper reviews smart drug-delivery systems for Alzheimer’s disease, focusing on how they can better manage the condition and its comorbidities.
Contribution
The paper highlights recent advances in nanotechnology-based drug delivery systems tailored for Alzheimer’s disease and comorbidities.
Findings
Smart drug-delivery systems can enhance brain targeting and reduce systemic toxicity.
Nanocarriers can modulate amyloid aggregation and neuroinflammation in Alzheimer’s.
Controlled release platforms are critical for translational success and regulatory readiness.
Abstract
Alzheimer’s disease (AD) remains a major unmet medical challenge due to its complex pathology, high interpatient heterogeneity and frequent association with systemic comorbidities. Conventional pharmacotherapy is limited by poor blood–brain barrier permeability, off-target effects and reduced efficacy in polymedicated elderly populations. Smart drug-delivery systems (DDS), particularly nanotechnology-based platforms, have emerged as promising strategies to enhance brain targeting, optimize controlled drug release and mitigate systemic toxicity. This review examines recent advances in intelligent DDS for AD, with a focus on nanocarriers designed to modulate amyloid aggregation, neuroinflammation, oxidative stress and cholinergic dysfunction. Special attention is given to the impact of the most common comorbid conditions on DDS pharmacokinetics, safety and clinical performance.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
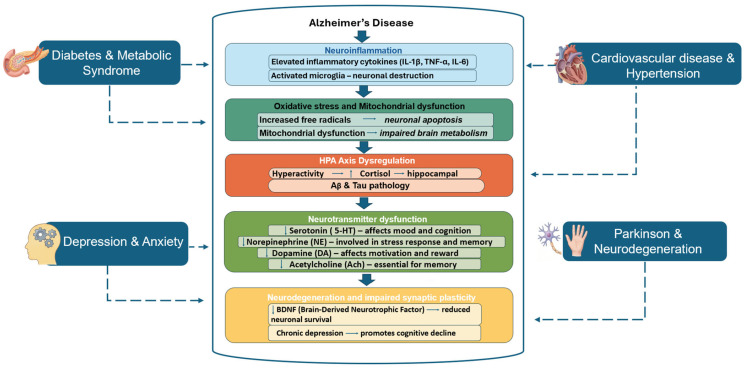 Figure 1
Figure 1- —Smart Growth, Digitalization and Financial Instruments Program (PoCIDIF)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAlzheimer's disease research and treatments · Advanced Drug Delivery Systems · Nanoparticle-Based Drug Delivery
1. Introduction
Alzheimer’s disease (AD) and related dementias represent one of the most pressing global health and socioeconomic challenges of the twenty-first century [1]. According to the World Health Organization, more than 55 million individuals are currently living with dementia worldwide, with prevalence expected to rise to over 152 million by 2050 due to aging populations and increased life expectancy [1,2]. This growing burden is accompanied by substantial direct healthcare costs and indirect societal impacts, including long-term caregiving, loss of productivity and profound effects on families and caregivers [2,3].
AD is clinically defined by progressive cognitive decline, memory impairment and behavioral changes, and neuropathologically characterized by extracellular beta-amyloid (Aβ) plaques, intracellular neurofibrillary tangles composed of hyperphosphorylated tau, synaptic loss, neuroinflammation and widespread neuronal dysfunction [4,5]. These pathological processes are intertwined with disturbances in neuronal communication, oxidative stress, mitochondrial dysfunction, and chronic inflammation, collectively contributing to irreversible neurodegeneration.
In addition to the complex central nervous system (CNS) pathology, AD frequently co-exists with systemic comorbid conditions that not only increase the risk for the development of AD but also modulate its progression and clinical presentation. Epidemiological evidence has consistently demonstrated associations between AD and type 2 diabetes mellitus, cardiovascular disease, depression, metabolic syndrome and chronic inflammatory disorders [6,7,8,9,10,11,12,13]. These comorbidities share overlapping mechanistic pathways, including insulin resistance, dysregulated lipid metabolism, endothelial dysfunction and chronic low-grade inflammation, which can exacerbate neurodegenerative processes and further compromise cognitive function [14,15]. Moreover, the presence of comorbidities complicates therapeutic management by altering drug absorption, distribution, metabolism and elimination, increasing the likelihood of polypharmacy, drug–drug interactions and adverse effects. Consequently, comprehensive therapeutic strategies must consider both central neurodegeneration and peripheral dysfunctions to optimize patient outcomes.
A critical barrier in the pharmacological management of AD is the restricted access of therapeutic agents to the brain imposed by the blood–brain barrier (BBB). The highly selective nature of the BBB limits the passive diffusion of most small molecules and effectively excludes large biologics, including many monoclonal antibodies and nucleic acid-based therapeutics [16]. This physiological protection contributes to the disappointing translational outcomes of many candidate drugs, which demonstrate promising results in preclinical models but fail to achieve sufficient brain concentrations in clinical settings. Conventional delivery strategies also suffer from rapid systemic clearance, off-target effects and suboptimal pharmacokinetic profiles, further limiting therapeutic efficacy [17,18].
In this context, smart drug-delivery systems have emerged as a transformative approach in neurotherapeutics. These engineered platforms, often based on nanoscale materials such as polymeric nanoparticles, lipid-based carriers, gold nanoparticles, dendrimers, and superparamagnetic iron oxide nanoparticles, are designed to enhance BBB penetration, improve drug stability, prolong systemic circulation and enable controlled or stimuli-responsive release of therapeutic agents [18,19]. Through surface functionalization with targeting ligands, receptor-mediated transport mechanisms can be exploited to facilitate selective accumulation in the CNS, while stimuli-responsive elements allow drug release to be modulated according to local pathological cues, such as pH gradients, oxidative stress or enzymatic activity [19,20].
Importantly, these systems offer opportunities to tackle the therapeutic challenges imposed by AD comorbidities. By enabling the co-delivery of multiple agents, smart nanocarriers can simultaneously address central neurodegeneration and peripheral pathologies. For example, multifunctional platforms can encapsulate neuroprotective drugs alongside antidiabetic, antihypertensive, antidepressant, or anti-inflammatory agents, providing an integrated therapeutic approach that may improve clinical outcomes while reducing systemic toxicity [20]. “Self-regulated” delivery mechanisms, capable of adjusting drug release kinetics or dosing in response to patient-specific factors such as glucose levels, further exemplify the potential for personalized intervention strategies. Despite encouraging preclinical evidence, the translation of these smart delivery systems from bench to bedside remains challenging. Critical issues include large-scale manufacturing, long-term safety, immunogenicity, regulatory approval and cost-effectiveness. Nonetheless, continued innovation in material science, stimuli-responsive designs, and integration with artificial intelligence and precision medicine holds promise for next-generation therapeutic modalities that simultaneously target central and peripheral aspects of Alzheimer’s disease.
While previous studies have focused primarily on individual nanocarrier platforms or their ability to deliver anti-Alzheimer agents, this narrative review offers a novel perspective by integrating the challenges posed by systemic comorbidities with the design and application of multifunctional smart delivery systems. It highlights co-delivery strategies, self-regulated mechanisms, and emerging AI-assisted and personalized approaches as a comprehensive framework for next-generation interventions.
2. Major Comorbid Conditions Associated with Alzheimer’s Disease
Alzheimer’s disease develops in the context of aging-related systemic vulnerability and is frequently accompanied by multiple chronic disorders that shape disease susceptibility, clinical heterogeneity and rates of progression [3]. Accumulating evidence indicates that metabolic, vascular, psychiatric, inflammatory and neurodegenerative comorbidities interact with hallmark AD pathology through overlapping biological pathways that become increasingly dysregulated with age [6,7,8,9,10,11,12,13]. Figure 1 schematically summarizes these interactions, emphasizing convergent mechanisms that link peripheral organ dysfunction to central nervous system neurodegeneration.
2.1. Metabolic Dysregulation: Type 2 Diabetes Mellitus and Metabolic Syndrome
Type 2 diabetes mellitus (T2DM) and metabolic syndrome are highly prevalent in aging populations and represent significant risk factors for cognitive decline and dementia, including AD. Multiple epidemiological studies indicate that individuals with T2DM have an elevated risk of developing AD compared with non-diabetic peers, with pooled analyses reporting hazard ratios ranging from approximately 1.5 to 3.0 [21,22].
The proposed mechanistic links between T2DM and AD are thought to begin with neuronal insulin resistance and impaired cerebral glucose metabolism [23]. Insulin plays a crucial role in brain function by modulating synaptic plasticity and supporting neurotrophic signaling. Deficits in insulin signaling have been detected in post-mortem AD brains and are associated with reduced activation of downstream pathways such as PI3K/Akt, which normally inhibit amyloidogenic processes and tau hyperphosphorylation [24].
Preclinical models reinforce this connection: rodents with diet-induced obesity or genetic models of diabetes exhibit exacerbated Aβ deposition, increased tau phosphorylation, compromised hippocampal neurogenesis, impaired long-term potentiation, deficits in learning and memory, and reduced functional performance, which may be interpreted as treatment failure or decreased therapeutic efficacy in these contexts. These observations support the concept that metabolic dysregulation can accelerate core neurodegenerative processes that characterize AD [25,26]. Beyond intrinsic pathology, diabetes and sustained hyperglycemia induce structural and functional alterations in the BBB that have direct implications for drug delivery and pharmacokinetics. Chronic high glucose levels promote oxidative stress, inflammation and upregulation of the glycation end products and receptor for AGEs (AGE–RAGE) axis, which disrupt tight junction integrity and increase BBB permeability, altering the transport of endogenous substrates (e.g., glucose, insulin) and xenobiotics across the cerebral endothelium [27,28]. These changes can result in regional BBB dysfunction, including tight junction disruption and dysregulated expression of key transporters such as P-glycoprotein, low-density lipoprotein receptor-related protein 1 (LRP1) and insulin transporters—all of which shape how drugs and pathological peptides traverse the BBB [29,30].
These pathophysiological alterations have been linked clinically and experimentally to altered drug transport dynamics. Certain antidiabetic agents such as glucagon-like peptide 1 (GLP-1) receptor agonists, sodium-glucose cotransporter 2 inhibitors (SGLT-2) and thiazolidinediones are associated with a reduced risk of dementia in individuals with T2DM [31,32]. In addition, specific antidiabetic drugs may exert neuroprotective effects beyond glucose lowering. For example, GLP-1 receptor agonists enhance insulin signaling in the brain, reduce Aβ deposition and improve synaptic plasticity in preclinical models [33]; SGLT-2 inhibitors may mitigate cerebrovascular dysfunction through improved endothelial function and reduced oxidative stress; and thiazolidinediones activate PPARγ pathways, reducing neuroinflammation and promoting neuronal survival [6,34]. Despite these promising observational findings, results from interventional trials remain mixed. Differences in patient populations, trial duration, cognitive endpoints and drug regimens likely contribute to the variability. Further well-designed, long-term randomized trials are needed to clarify whether these agents can meaningfully prevent or slow cognitive decline in T2DM.
Dyslipidemia and central adiposity, hallmark features of metabolic syndrome, further exacerbate endothelial dysfunction and microvascular injury, leading to widespread compromise of BBB integrity. The resulting BBB disruption impairs cerebral perfusion and reduces the clearance of neurotoxic proteins, including amyloid-β and hyperphosphorylated tau, which accumulate in AD. Mechanistically, dyslipidemia contributes to oxidative stress and inflammation within the cerebrovascular endothelium, while central adiposity promotes chronic low-grade systemic inflammation through the secretion of adipokines and pro-inflammatory cytokines such as tumor necrosis factor alpha (TNF-α) and interleukin-6 (IL-6) [35]. Together, these processes impair cerebrovascular reactivity, disrupt nutrient and oxygen delivery to neurons and facilitate the infiltration of peripheral immune cells into the CNS. Preclinical models have demonstrated that diet-induced obesity or hyperlipidemia leads to exacerbated Aβ deposition, tau pathology and cognitive deficits, providing a mechanistic link between metabolic imbalances and neurodegeneration. Clinically, patients with metabolic syndrome show reduced cerebral perfusion and microvascular rarefaction, correlating with cognitive decline and increased risk of AD [36]. In such patients, systemic metabolic alterations can modify both the pharmacokinetics and CNS availability of neurotherapeutics, leading to either toxicity or suboptimal efficacy. Consideration of metabolic status is therefore critical when evaluating therapeutic outcomes in AD.
2.2. Cardiovascular Disease
Cardiovascular disease (CVD) remains a leading cause of morbidity and mortality in aging populations worldwide, and growing evidence implicates atherosclerosis, the central pathogenic substrate of CVD, in the development of late-life cognitive impairment and Alzheimer’s disease [37]. Population-based cohort studies have demonstrated that elevated blood pressure during midlife confers a substantially increased risk of dementia decades later, while cumulative exposure to vascular risk factors across the lifespan correlates with accelerated cortical thinning, hippocampal atrophy and white-matter disruption on neuroimaging. These associations persist even after adjustment for traditional demographic and lifestyle variables, underscore the direct contribution of vascular pathology to neurodegenerative vulnerability [38,39].
At the level of cerebral hemodynamics, vascular aging is accompanied by progressive arterial stiffening, reduced bioavailability of endothelial nitric oxide and impaired neurovascular coupling. Hypertension and atherosclerosis amplify these alterations, compromising autoregulatory capacity and leading to sustained reductions in regional cerebral blood flow [40]. Chronic hypoperfusion preferentially affects watershed territories and metabolically active regions such as the hippocampus and posterior cingulate cortex, where it induces energetic stress, synaptic failure and increased susceptibility to amyloidogenic processing of amyloid precursor protein. In parallel, diminished perivascular drainage and transporter-mediated efflux across the BBB impair Aβ clearance, fostering parenchymal accumulation [41].
Structural and functional disruption of the BBB represents a further link connecting systemic vascular disease to AD pathology. Experimental and human neuropathological studies reveal loss of endothelial tight junction integrity, pericyte degeneration and basement membrane thickening in hypertensive states, changes that have been associated with microglial activation and perivascular inflammation. Such barrier dysfunction facilitates the entry of circulating cytokines, fibrinogen and immune cells into the brain parenchyma, amplifying local inflammatory signaling and oxidative injury to neurons and glia [40,42]. Importantly, these vascular and BBB alterations may also influence the delivery, CNS penetration and pharmacokinetics of neurotherapeutic agents. Impaired transporter activity, disrupted endothelial function and altered cerebral perfusion can reduce drug availability, modify local concentrations, and potentially diminish efficacy or increase toxicity [37,38,39,40,41,42].
Clinico-pathological investigations in aging cohorts consistently indicate that cerebrovascular lesions rarely occur in isolation from classical AD pathology. Lacunar infarcts, cerebral microbleeds, white-matter hyperintensities and arteriolosclerosis frequently coexist with amyloid plaques and neurofibrillary tangles, producing a mixed vascular–Alzheimer’s disease phenotype that dominates in advanced age [43]. This combined pathology is associated with more precipitous cognitive decline, earlier functional dependency and greater neuropsychiatric burden than either disease process alone, highlighting the synergistic rather than additive nature of vascular and neurodegenerative abnormalities [44].
Insights from preclinical models further substantiate these clinical observations. Rodents subjected to chronic hypertension or experimental hypoperfusion develop endothelial dysfunction, breakdown of BBB integrity and exaggerated neuroinflammatory responses. When superimposed on transgenic AD backgrounds, these vascular perturbations accelerate Aβ deposition, intensify tau phosphorylation, and exacerbate synaptic loss and memory impairment [45,46]. Conversely, interventions that improve cerebrovascular function including antihypertensive treatment, restoration of endothelial signaling or enhancement of cerebral perfusion attenuate neuropathological burden and partially rescue cognitive deficits, supporting a causal role for vascular dysfunction in AD pathogenesis [45,46,47].
2.3. Psychiatric Comorbidities: Depression and Anxiety in Late Life
Depression and anxiety are among the most common neuropsychiatric comorbidities in Alzheimer’s disease, with prevalence estimates reaching 50% for depressive symptoms and 30% for anxiety in affected cohorts [48,49,50]. Epidemiological studies indicate that late-life anxiety and depression may precede the clinical onset of AD and act as prodromal markers or modifiers of disease progression. A 10-year longitudinal community study reported that clinically significant anxiety at baseline was associated with a nearly threefold increased risk of developing AD, even after adjusting for depression and other confounders [51]. Case–control data from the HUNT study found that depression significantly increased AD risk (OR ~4.39), whereas anxiety showed variable associations depending on dementia subtype [52]. In contrast, the Rotterdam study observed no significant link between anxiety symptoms and dementia risk, highlighting heterogeneity across populations [53]. Cohort data further indicate that individuals with AD have a substantially higher subsequent risk of developing major depression compared with age-matched controls [54].
Preclinical models provide mechanistic support for these clinical observations. APP/PSEN1 transgenic mice display anxiety-like and depression-like behaviors preceding amyloid plaque deposition, mirroring human prodromal features [55]. Similarly, in 3 × Tg-AD mice, pharmacological inhibition of phosphodiesterase-4 (PDE4) with rolipram reduced both neurodegenerative pathology and affective symptoms, implicating neuroinflammation, Aβ accumulation and tau phosphorylation in contributing to the comorbidity of AD and mood dysregulation [56].
Mechanistically, chronic activation of the hypothalamic–pituitary–adrenal (HPA) axis and prolonged glucocorticoid exposure are implicated in both mood dysregulation and AD progression, promoting hippocampal neuronal vulnerability, impairing neurogenesis and enhancing amyloidogenic processing of APP [57]. Elevated systemic inflammatory signaling, evidenced by increased circulating cytokines in depressed patients and stressed animal models, further primes central microglia toward a pro-inflammatory phenotype, exacerbating Aβ and tau pathology [57,58,59]. These mechanistic insights are consistent with findings in APP/PSEN1 and 3 × Tg-AD mice, where HPA axis dysregulation and neuroinflammation accelerate cognitive decline and neuropathological progression [55,56]. These alterations can compromise BBB integrity, modulate drug transporter activity and affect pharmacokinetics, reducing the penetration and efficacy of CNS-targeted therapies. Dysregulated neurochemical signaling associated with affective disorders may further alter receptor responsiveness and pharmacodynamic outcomes [57,58,59].
Together, clinical and preclinical evidence supports a bidirectional and mechanistically convergent relationship between depression/anxiety and AD. Early identification and management of affective symptoms may improve quality of life and modulate neuropathological progression, highlighting the importance of integrated therapeutic strategies for aging populations.
2.4. Parkinsonism and Mixed Neurodegenerative Syndromes
Parkinsonian features and mixed neurodegenerative syndromes frequently co-occur with Alzheimer’s disease, contributing to clinical heterogeneity and accelerating cognitive, motor and functional decline. Epidemiological studies indicate that a substantial subset of AD patients present parkinsonian signs, including bradykinesia, rigidity and tremor, often preceding or developing alongside cognitive deficits [60,61]. These motor features are associated with more rapid cognitive deterioration, earlier gait instability, increased neuropsychiatric symptoms and higher rates of falls compared with AD patients without Parkinsonism [62].
Biomarker studies demonstrate that misfolded α-synuclein in cerebrospinal fluid (CSF) often co-exists with phosphorylated tau and elevated Aβ levels, correlating with emergent cognitive deficits in at-risk older adults and suggesting the presence of mixed pathology even in prodromal stages of AD [62,63]. Post-mortem neuropathological analyses reveal overlapping distributions of Aβ, tau and α-synuclein in AD, dementia with Lewy bodies (DLB), and mixed AD/DLB cases, confirming that protein co-pathologies are prevalent in aging brains and contribute to clinical heterogeneity [63,64,65]. Longitudinal imaging studies indicate that Lewy body co-pathology exacerbates regional hypometabolism, synaptic dysfunction and neurodegeneration, accelerating cognitive decline compared with pure AD [66,67].
Preclinical studies provide mechanistic insight into these associations. Transgenic mouse models co-expressing Aβ, tau and α-synuclein recapitulate key features of the human mixed phenotype, including cognitive and motor deficits, synaptic loss, oxidative stress, and enhanced microglial and astrocyte activation [68,69]. These pathological processes may alter transporter activity and receptor responsiveness, potentially reducing the efficacy of CNS-targeted therapies. Pharmacological interventions targeting α-synuclein aggregation, neuroinflammation or mitochondrial dysfunction partially restore cognitive and motor outcomes, demonstrating the translational relevance of these models for testing multi-target therapies [70,71,72].
Together, these findings indicate that Parkinsonism and mixed neurodegenerative syndromes act as accelerators of AD-related neurodegeneration. Recognition of co-pathology is critical for diagnostic accuracy, prognosis and personalized therapeutic strategies, emphasizing the importance of integrated approaches targeting protein aggregation, neuroinflammation and synaptic resilience [62,63,64,65,71,72]. Translationally, preclinical models incorporating both AD and Parkinsonian pathology provide a platform for the development of multi-target therapeutics and biomarker validation, reducing reliance on multiple disease-specific models while supporting ethical and efficient preclinical research.
2.5. Chronic Systemic Inflammation and Immune Aging
Chronic systemic inflammation and age-related immune dysregulation (immunosenescence) are increasingly recognized as central contributors to Alzheimer’s disease pathogenesis. Epidemiological studies indicate that elevated peripheral inflammatory markers, including IL-1β, TNF-α, IL-6 and C-reactive protein, predict both incident AD and faster cognitive decline in older adults [73,74]. Longitudinal cohort analyses show that individuals with persistently high systemic inflammation exhibit accelerated hippocampal atrophy, reduced cortical thickness and increased amyloid deposition, supporting a mechanistic link between peripheral immune activation and central neurodegeneration [75,76].
Biomarker studies demonstrate that age-associated immune dysfunction promotes a pro-inflammatory milieu, characterized by dysregulated T cell populations, impaired regulatory networks and chronic low-grade cytokine elevation. This systemic inflammation is mirrored in the central nervous system by microglial priming and astrocytic activation, which exacerbate Aβ accumulation, tau phosphorylation and synaptic dysfunction [77,78]. Chronic cytokine elevation can downregulate hepatic and extrahepatic cytochrome P450 enzymes and drug transporters, altering drug metabolism, clearance and bioavailability. In parallel, inflammation-induced changes in BBB integrity and transporter function can reduce CNS penetration of pharmacological agents, thereby modifying drug efficacy and pharmacodynamic response [79]. Preclinical studies further support a causal role for immune aging in AD. In mouse models, chronic peripheral inflammation accelerates amyloid and tau pathology, induces microglial activation and impairs synaptic plasticity [73,74,80,81]. Conversely, interventions that reduce systemic inflammation, such as anti-cytokine therapies or senolytic agents—ameliorate cognitive deficits and reduce neurodegenerative markers, highlighting translational potential [82,83]. Age-related dysfunction in innate and adaptive immunity also synergizes with other comorbidities, including metabolic syndrome, cardiovascular disease, and neurodegenerative pathologies, amplifying neurodegeneration via convergent inflammatory pathways [35,36,47,54,74].
3. Smart Drug-Delivery Systems: Nanotechnology-Based Delivery Approaches
The therapeutic management of Alzheimer’s disease and its prevalent comorbidities remains highly challenging, largely due to limited BBB permeability, rapid systemic clearance, off-target toxicity and subtherapeutic drug concentrations at pathological sites. Smart nanotechnology-based drug delivery systems have emerged as versatile tools capable of enhancing brain targeting, improving pharmacokinetics and enabling temporally and spatially controlled interventions [84]. Such platforms are particularly well-suited to the complex and convergent pathophysiology of AD, which encompasses Aβ and tau aggregation, synaptic dysfunction, neuroinflammation, oxidative stress and mitochondrial impairment. By facilitating precise delivery of small molecules, biologics or nucleic acid therapeutics, nanocarriers can simultaneously modulate multiple pathological pathways, potentially mitigating both core AD pathology and associated comorbid processes such as metabolic dysregulation, vascular dysfunction and mood disorders [85,86].
Preclinical evidence consistently demonstrates that liposomes, polymeric nanoparticles, solid lipid nanoparticles and exosome-like carriers improve central nervous system bioavailability, attenuate neurodegenerative cascades and enhance functional outcomes in AD models [87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127]. Early translational approaches, including intranasal formulations for nose-to-brain delivery and pharmacokinetic optimization studies provide encouraging evidence for clinical applicability and safety profiling. Representative preclinical examples are summarized in Table 1, illustrating the potential of nanotechnology-based systems to address the multifactorial challenges of AD therapy.
Prevalent comorbidities in Alzheimer’s disease critically influence both the pathophysiology and the delivery of therapeutics across the blood–brain barrier. These conditions can impair BBB integrity, exacerbate oxidative stress and alter systemic pharmacokinetics, necessitating design considerations for nanocarrier systems. For instance, neuroinflammation-driven BBB disruption and increased reactive oxygen species highlight the need for multi-mechanistic nanoparticles with anti-inflammatory and antioxidant properties [96,113,120,122,128]. In patients with metabolic comorbidities (e.g., diabetes or hyperlipidemia), biomimetic coatings such as HDL-mimetic, RBC-coated or platelet–CCR2 membrane systems can enhance brain delivery while minimizing off-target effects [95,115,116,117,129,130]. Similarly, vascular comorbidities that reduce perfusion or exacerbate amyloid deposition support the application of nanocarriers exploiting receptor-mediated BBB transport (e.g., B6-SA-SeNPs, sialic acid-modified systems) [120,122,124]. Overall, these considerations demonstrate that smart nanocarrier design must integrate disease- and comorbidity-specific pathophysiological features to optimize targeting efficiency and therapeutic outcomes
4. Clinical Translation and Regulatory Challenges
Despite extensive preclinical promise of smart drug-delivery systems (DDS) in overcoming the blood–brain barrier and improving therapeutic outcomes in animal models, no nanoparticle-based therapeutics for Alzheimer’s disease have yet reached advanced clinical trials or regulatory approval. Translation remains limited due to insufficient brain targeting in humans, potential safety and toxicity concerns, complex pharmacokinetics and clearance, and difficulties in scalable manufacturing under Good Manufacturing Practices (GMP) [131,132,133,134,135]. In AD, these challenges are amplified by patient heterogeneity, widespread polypharmacy and disease-associated alterations in BBB permeability [131,136,137,138]. Consequently, biomarker-driven patient stratification and adaptive clinical trial designs are increasingly required to ensure meaningful therapeutic evaluation [137,138,139,140,141]. Bridging this translational gap will require: (i) comprehensive toxicological and pharmacokinetic characterization of nanocarrier physicochemical properties, (ii) robust Quality by Design (QbD)-based scale-up to ensure batch-to-batch consistency, (iii) early engagement with regulatory agencies to establish GMP-compliant manufacturing criteria, and (iv) ethical frameworks that balance technological innovation with patient protection [131,142,143].
The safety profile of smart DDS is of particular importance in AD due to the chronic nature of the disease and the vulnerability of elderly patients with multiple comorbidities. Nanocarriers engineered to cross the altered BBB characterized by increased permeability resulting from amyloid-induced endothelial damage may accumulate in cerebral and peripheral tissues, especially in patients with cardiovascular comorbidities, potentially leading to unintended toxicity [143,144]. Polymeric nanoparticles may persist within the brain, inducing oxidative stress or impairing neuronal function due to incomplete clearance via BBB efflux transporters, the reticuloendothelial system or AD-associated dysfunction of the glymphatic–lymphatic pathways, which exacerbates waste accumulation in aging brains, particularly in individuals with renal insufficiency [131,137,138]. Surface-modified nanocarriers, such as PEGylated liposomes, may also elicit immune responses, including complement activation or cytokine release, potentially aggravating AD-related neuroinflammation and tau pathology [137,145,146]. Importantly, chronic toxicity associated with repeated administration remains insufficiently explored, with limited long-term data on genotoxicity or organ damage, especially in patients with impaired renal function, where reduced clearance may prolong DDS exposure [131,147]. These risks are further compounded by polypharmacy; in polymedicated individuals, drug–drug interactions may compromise safety, as nanocarrier-encapsulated cholinesterase inhibitors can alter the metabolism of concomitant antihypertensive agents, particularly in patients with hepatic insufficiency affecting DDS metabolism [128,134]. Collectively, these gaps highlight the need for chronic toxicity studies in animal models that recapitulate AD with relevant comorbidities, incorporating biomarkers of neurotoxicity and systemic burden. In parallel, post-marketing pharmacovigilance remains essential to capture real-world safety outcomes, including rare hypersensitivity reactions or cumulative toxicity [139].
Scaling smart DDS from laboratory synthesis to industrial production presents significant technological challenges that directly impact clinical translation for AD therapies. Regulatory agencies, including the Food and Drug Administration (FDA), provide specific guidance for liposomal and nanoparticle formulations, covering physicochemical characterization, preclinical safety, pharmacokinetics, biodistribution, and GMP-compliant manufacturing [132,133]. Manufacturing inconsistencies, such as variations in particle size (<100 nm), surface characteristics or drug-loading efficiency, can compromise BBB penetration, release kinetics, and pharmacokinetic predictability, thereby reducing therapeutic efficacy in patients where precise dosing is critical to counteract neuroinflammation and impaired lymphatic clearance [132,134,135]. Formulation stability represents an additional challenge, as nanocarriers may aggregate or degrade during storage, adversely affecting shelf life and therapeutic integrity. This issue is particularly problematic for long-term treatment regimens in patients with renal or hepatic dysfunction, which further influences DDS clearance and metabolism [131,134,135]. Batch-to-batch variability complicates regulatory compliance and quality assurance, underscoring the importance of early process standardization using QbD principles and rigorous preclinical biodistribution and clearance studies, alongside adaptive biomarker-driven clinical monitoring [131,133,142]. Advanced quality control strategies, including in-process monitoring via Process Analytical Technology (PAT), are increasingly recognized as essential to ensure consistent nanomedicine quality [135]. Addressing these manufacturing challenges is critical for the development of scalable, cost-effective DDS aligned with the clinical demands of AD management in comorbid populations [134].
Clinical trial design for smart DDS in AD must rigorously account for patient heterogeneity, disease stage and comorbidities to achieve translational success [137,145]. AD progression is highly variable and influenced by genetic factors, such as APOE genotype, as well as common comorbid conditions (e.g., diabetes and hypertension) that can alter DDS pharmacokinetics via changes in renal clearance or hepatic metabolism [137,145]. The high prevalence of polypharmacy in elderly AD patients further increases the risk of drug–drug interactions, necessitating systematic evaluation of DDS compatibility with concomitant medications [137].
Biomarker-driven patient stratification using amyloid positron emission tomography (PET), cerebrospinal fluid tau measurements or emerging blood-based biomarkers enables targeted enrollment of early-stage patients, who are most likely to benefit from disease-modifying DDS interventions in the context of chronic neuroinflammation [142,145]. Primary endpoints should integrate validated cognitive scales (e.g., ADAS-Cog), functional outcome measures and comorbidity-specific metrics, such as cardiovascular events, with extended follow-up to distinguish sustained clinical benefit from isolated biomarker changes [145]. Unlike conventional pharmacological trials, DDS studies require adaptive designs that allow real-time monitoring of brain penetration and release kinetics through imaging or pharmacodynamic biomarkers, as well as strategies to mitigate attrition associated with cognitive decline [137,139]. Long-term efficacy assessment in comorbid cohorts remains challenging due to confounding factors, emphasizing the need for phase-specific approaches—prioritizing safety and dose optimization in Phase I/II and adequately powered efficacy assessments in later-stage trials [137,145]. Integration of real-world evidence following regulatory approval may further refine stratification strategies and ensure that DDS address the heterogeneous phenotypes encountered in clinical practice [137,145].
The successful clinical translation of DDS for AD ultimately depends on robust ethical and regulatory frameworks that promote innovation while safeguarding vulnerable patients [132,133,142]. Given the frequent impairment of decision-making capacity in AD, informed consent procedures must incorporate legally authorized representatives while preserving patients’ residual autonomy [142]. Long-term safety uncertainties necessitate transparent risk communication and continuous post-marketing surveillance, particularly in elderly individuals with renal or hepatic insufficiency [133,135,142].
Equitable access represents an additional challenge, as the high development and manufacturing costs associated with advanced DDS may limit availability in underserved regions, potentially exacerbating healthcare disparities [133,142]. Regulatory agencies such as the FDA and the European Medicines Agency (EMA) provide guidance for nanomedicines based on case-by-case evaluations of safety and efficacy; however, divergent regulatory requirements exemplified by EMA reflection papers on liposomal formulations versus FDA nanomaterial guidance continue to impede global harmonization and delay widespread clinical adoption [132,133,135]. Furthermore, AD-specific physiological barriers, including BBB dysfunction and compromised glymphatic clearance, must be explicitly addressed within regulatory assessments [137,138]. Ultimately, integrating technological innovation with ethically grounded, patient-centered regulatory strategies and continuous ethical oversight will be essential to ensure that the anticipated benefits of smart DDS outweigh their inherent risks, particularly in comorbid AD populations [133,137,142].
5. Future Perspectives
Future advances in Alzheimer’s disease therapy will increasingly depend on the development of smart drug-delivery systems that move beyond disease-centric paradigms toward patient-centered and translationally viable solutions. The marked heterogeneity of AD, compounded by prevalent comorbidities necessitates delivery platforms capable of adapting drug release profiles to individual pathophysiological conditions [6,7,8,9,10,11,12,13]. In this context, versatile controlled release systems that allow modular adjustment of dose, release kinetics and targeting properties represent a critical step toward precision medicine in neurodegenerative disorders.
A key direction for the future is the design of intelligent DDS that respond dynamically to the pathological microenvironment of the AD brain. Stimuli-responsive nanocarriers that sense changes in pH, oxidative stress, enzymatic activity or blood–brain barrier integrity have the potential to enhance therapeutic efficacy while minimizing systemic exposure and cumulative toxicity [15,59,62]. Such adaptive systems are particularly relevant in AD, where BBB permeability and clearance mechanisms evolve throughout disease progression and are further altered by aging and comorbid conditions.
The translation of nanoparticle-based DDS from preclinical models to humans remains challenging. In this context, artificial intelligence provides a complementary dimension by enabling the analysis and interpretation of complex datasets, including neuroimaging, proteomics and longitudinal patient monitoring [148]. Machine learning models have proven useful for identifying early disease signatures, stratifying patients into molecular subtypes, and supporting personalized therapeutic strategies. Concurrently, AI-driven materials informatics can accelerate the optimization of nanoparticle formulations, predict BBB permeability and facilitate adaptive DDS that adjust in real time based on biomarker feedback [149,150].
Integrating AI with predictive pharmacokinetic–pharmacodynamic models enhances the rational design of DDS. Physiologically based pharmacokinetic models combined with AI frameworks allow researchers to simulate nanoparticle transport, brain accumulation and systemic clearance, incorporating patient-specific factors such as genetic background, comorbidities and disease stage [151]. This approach supports individualized dosing and treatment planning while minimizing unnecessary preclinical experiments. The concept of digital twins further enables the iterative refinement of DDS in silico, providing a platform for testing therapeutic strategies under simulated patient-specific conditions [152,153,154].
Equally important is the consideration of scalable and reproducible manufacturing strategies. Many nanotechnology-based DDS fail to progress clinically due to challenges in ensuring batch-to-batch consistency, long-term stability, and regulatory compliance [17,152]. Future platforms should be developed alongside QbD frameworks and real-time process monitoring tools, such as Process Analytical Technology, to maintain robust control over critical material and process attributes. Advanced manufacturing approaches, including microfluidics and additive manufacturing techniques, provide opportunities to produce reliable, clinically relevant formulations [155,156].
Principles derived from versatile controlled release platforms originally developed for advanced topical formulations can be adapted to central nervous system and intranasal delivery strategies. Modular architectures, predictable release kinetics and standardized characterization pipelines enable cross-application of these platforms, facilitating rapid adaptation to diverse therapeutic routes while maintaining consistent performance and safety profiles [157]. This translational flexibility is particularly valuable in neurodegenerative diseases, where alternative routes may help overcome the restrictive properties of the BBB.
Future progress in smart DDS for AD will require early and sustained engagement with regulatory and ethical frameworks. Systems should be designed with regulatory readiness in mind, supported by comprehensive characterization, predictive toxicology and transparent risk–benefit assessment. The growing role of AI in DDS design introduces additional considerations, including data standardization, algorithm transparency and oversight requirements, highlighting the importance of harmonized guidelines to balance innovation with patient safety [158].
By combining AI-assisted design, mechanistic modeling, predictive pharmacokinetics, and scalable manufacturing, versatile controlled-release platforms provide a pathway toward safe, adaptable and clinically translatable therapies for Alzheimer’s disease. Integrating nanotechnology, computational modeling and precision medicine holds the potential to deliver personalized interventions that address the complex, heterogeneous nature of this disorder.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clare L. Jeon Y.H. World Alzheimer Report 2025: Reimagining Life with Dementia—The Power of Rehabilitation Alzheimer’s Disease International London, UK 20251144
- 2Alzheimer’s Disease International World Alzheimer Report 2024: Global Changes in Attitudes to Dementia Alzheimer’s Disease International London, UK 20241176
- 3Twiss E. Mc Pherson C. Weaver D.F. Global diseases deserve global solutions: Alzheimer’s disease Neurol. Int.2025179210.3390/neurolint 1706009240559330 PMC 12196516 · doi ↗ · pubmed ↗
- 4Tahami Monfared A.A. Tafazzoli A. Ye W. Chavan A. Zhang Q. Long-term health outcomes of lecanemab in patients with early Alzheimer’s disease using simulation modeling Neurol. Ther.20221186388010.1007/s 40120-022-00350-y 35469060 PMC 9095799 · doi ↗ · pubmed ↗
- 5Dominguez-Gortaire J. Ruiz A. Porto-Pazos A.B. Rodriguez-Yanez S. Cedron F. Alzheimer’s Disease: Exploring Pathophysiological Hypotheses and the Role of Machine Learning in Drug Discovery Int. J. Mol. Sci.202526100410.3390/ijms 2603100439940772 PMC 11816687 · doi ↗ · pubmed ↗
- 6Stanciu G.D. Ababei D.C. Solcan C. Bild V. Ciobica A. Beschea Chiriac S.-I. Ciobanu L.M. Tamba B.-I. Preclinical studies of canagliflozin, a sodium-glucose co-transporter 2 inhibitor, and donepezil combined therapy in Alzheimer’s disease Pharmaceuticals 202316162010.3390/ph 1611162038004485 PMC 10674192 · doi ↗ · pubmed ↗
- 7Kciuk M. Kruczkowska W. Gałęziewska J. Wanke K. Kałuzińska-KołatŻ. Aleksandrowicz M. Kontek R. Alzheimer’s disease as type 3 diabetes: Understanding the link and implications Int. J. Mol. Sci.2024251195510.3390/ijms 25221195539596023 PMC 11593477 · doi ↗ · pubmed ↗
- 8Tini G. Scagliola R. Monacelli F. La Malfa G. Porto I. Brunelli C. Rosa G.M. Alzheimer’s disease and cardiovascular disease: A particular association Cardiol. Res. Pract.20202020261797010.1155/2020/261797032454996 PMC 7222603 · doi ↗ · pubmed ↗