ALM Resuscitation Without Transfusion Improves Platelet Function and Survival After Liver Injury and Uncontrolled Hemorrhage
Hayley Letson, Geoffrey Dobson

TL;DR
A new treatment using adenosine, lidocaine, and magnesium improves survival and platelet function in rats after severe liver injury and bleeding, without needing blood transfusions.
Contribution
ALM resuscitation without transfusion improves survival and platelet function after non-compressible hemorrhage in a rat model.
Findings
ALM therapy without transfusion achieved 100% survival in rats after liver injury and uncontrolled bleeding.
ALM reduced lung injury, preserved platelet function, and decreased immune and metabolic dysfunction.
Transfusions of FFP or FWB administered 5 hours after injury did not significantly improve survival.
Abstract
Background and Objectives: Traumatic hemorrhage is a leading cause of death. Our aim was to examine the effect of adenosine, lidocaine and magnesium (ALM) resuscitation therapy with and without fresh frozen plasma (FFP) or fresh whole blood (FWB) in a rat model of non-compressible hemorrhage. Materials and Methods: Anesthetized adult male Sprague-Dawley rats (439 ± 46 g) randomly assigned to (1) Shams (surgical trauma and liver isolation only without hemorrhage) (n = 34), (2) Saline controls (n = 34), or (3) ALM therapy (n = 34), underwent liver resection and uncontrolled bleeding. After 5 h 3% NaCl ± ALM bolus and 0.9% NaCl ± ALM drip fluid resuscitation, each group was randomized to receive no transfusion (NT) (n = 10 per treatment group), FFP (n = 12), or FWB (n = 12), and monitored for 72 h. Survival, hemodynamics, lactate, hematology, coagulation, platelet function, and lung…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
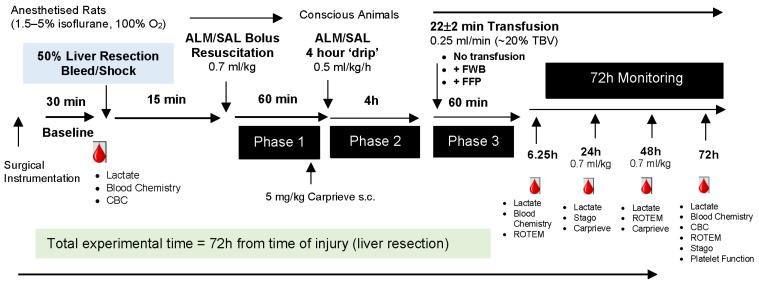 Figure 1
Figure 1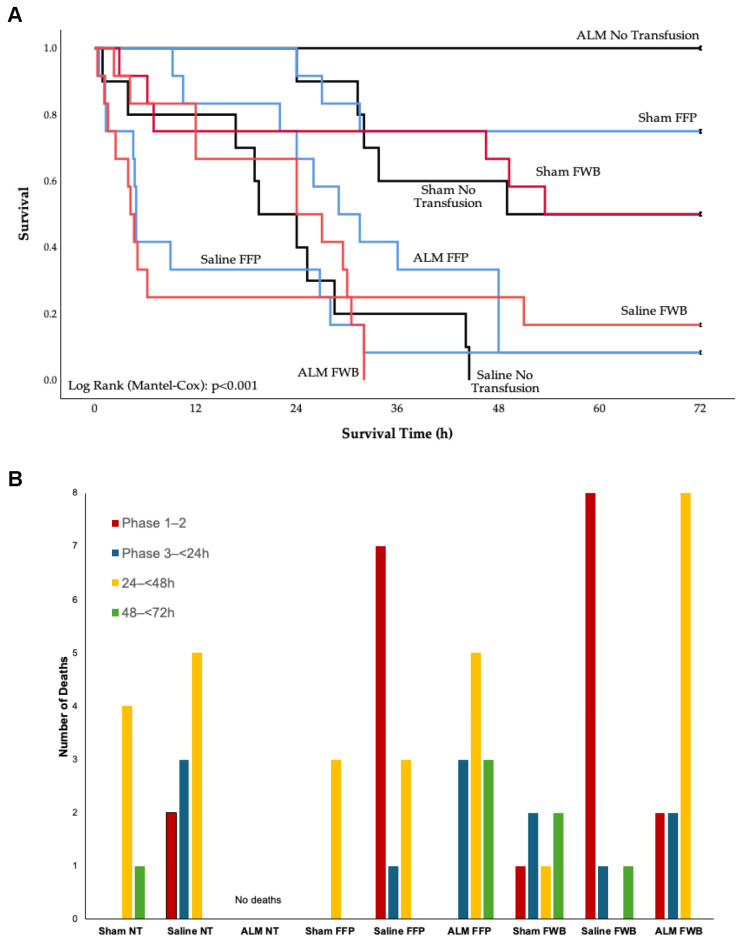 Figure 2
Figure 2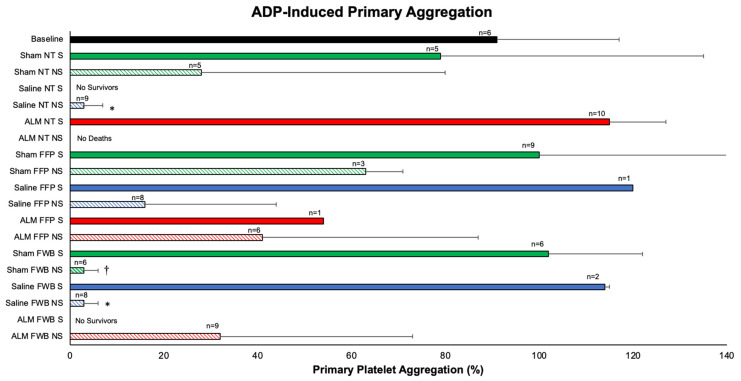 Figure 3
Figure 3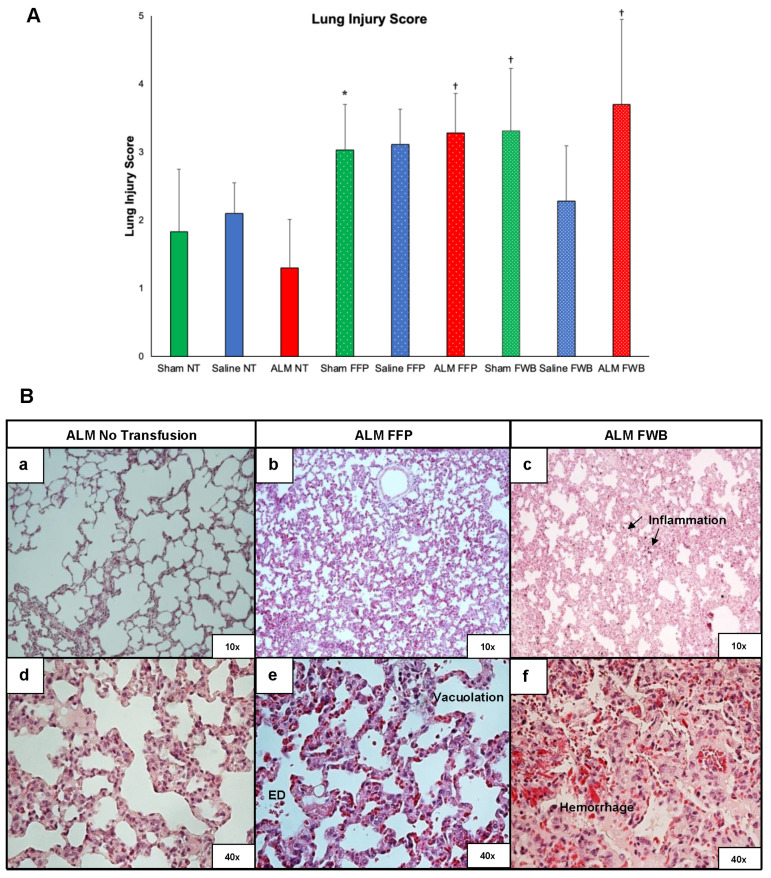 Figure 4
Figure 4- —USSOCOM, USAMRMC proposal SO150053
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTrauma, Hemostasis, Coagulopathy, Resuscitation · Blood transfusion and management · Hemostasis and retained surgical items
1. Introduction
Traumatic hemorrhagic shock is a leading cause of potentially preventable mortality, particularly in far-forward battlefield environments and prehospital civilian environments [1,2,3]. Volume resuscitation at the point-of-injury is essential to raise mean arterial pressure (MAP) and ensure adequate oxygen delivery to tissues [4]. Fresh whole blood (FWB) was the primary resuscitation fluid during World Wars I and II and the Korean War until the Vietnam War, with a wider adoption of crystalloids and colloids [5]. However, the use of high fluid volumes became associated with hemodynamic compromise, trauma-induced coagulopathy, acidosis and “shock lung” [6,7]. In recent years, crystalloids have mostly been replaced with component therapy (1:1:1 plasma:platelets:red blood cells) [4,5,8]. Two randomized clinical trials have also shown a survival benefit with fresh frozen plasma (FFP), although its use remains controversial [9,10]. In addition, there are logistical problems using FFP far-forward because it requires special handling, storage and preparative requirements compared to whole blood, which can be obtained from ‘buddy’ donors in the field [6,11]. Fresh whole blood has other physiological advantages, and two retrospective trials have shown a potential survival benefit of FWB or equivalence to component therapy in severe combat casualties [12,13]. Despite this, use of prehospital transfusion remains rare and widespread adoption faces ongoing challenges, particularly in rural and remote areas, which are disadvantaged by limited resources and availability of medical support [14,15].
We have been developing a small-volume adenosine, lidocaine and magnesium (ALM) fluid therapy for point-of-injury and prolonged field care after hemorrhagic shock [16,17]. ALM bolus and drip resuscitation therapy led to 3-day survival in the rat model of non-compressible hemorrhage, compared to 22 h for Saline controls [18]. The ALM survival phenotype was associated with improved cardiac function, correction of coagulopathy, platelet preservation, reduced inflammation, and upregulation of the master genes of metabolism and mitochondrial function (Ampk, Sirt-1, Pgc1a, Mtco3, and Tfam) in central tissues [18,19,20,21]. The aim of the present study was to examine the effect of FFP or FWB transfusion in addition to ALM therapy in the rat model of laparotomy, liver resection and non-compressible hemorrhage.
2. Materials and Methods
2.1. Animals and Ethics
This study was approved by James Cook University Animal Ethics Committee (A2296) and US Army Animal Care and Use Review Office (ACURO: SO150053) and complies with the Australian Code for the Care and Use of Animals for Scientific Purposes (8th Edition, 2013) and National Institutes of Health Guide for Care and Use of Laboratory Animals (8th Edition, 2011). The study is reported in accordance with the Animal Research: Reporting In Vivo Experiments (ARRIVE) guidelines [22] (Supplementary Material S1). Conventional adult male Sprague-Dawley rats (n = 102; 439 ± 46 g) sourced from the non-specific pathogen-free James Cook University breeding colony, were housed in individually ventilated Tecniplast cages in a 14–10 h dark–light cycle with free access to environmental enrichment, food and water ad libitum. Animals were randomly assigned using a random number generator (GraphPad Prism 8; GraphPad Software L.L.C, San Diego, CA, USA) to (1) Sham No Transfusion (NT) (n = 10), (2) Saline NT (n = 10), (3) ALM NT (n = 10), (4) Sham FFP (n = 12), (5) Saline FFP (n = 12), (6) ALM FFP (n = 12), (7) Sham FWB (n = 12), (8) Saline FWB (n = 12), or (9) ALM FWB (n = 12). Animals were anesthetized with isoflurane 1.5–5% in 100% oxygen during surgical instrumentation, laparotomy, liver resection, and throughout Phase 1 bolus resuscitation. Carprieve^®^ (Norbrook Laboratories; Newry, Northern Ireland) (carprofen 5 mg/kg s.c.) was administered prior to recovery from anesthesia for postoperative analgesia and again at 24 h and 48 h (Figure 1).
2.2. Surgical Protocol
Anesthetized animals had sterile chronic catheters (Access Technologies, Skokie, IL, USA) implanted in the left femoral artery and vein for blood pressure monitoring (BridgeAMP coupled to Powerlab; ADInstruments, Bella Vista, Australia), blood sampling, and fluid/drug infusions respectively. Lead II electrocardiogram was subcutaneously implanted for heart rate monitoring (BioAMP/Powerlab). Animals had a 30 min baseline stabilization period after surgical instrumentation, with the exclusion of any animal that exhibited complex ventricular arrhythmias or a sustained fall in MAP < 80 mmHg (Figure 1).
2.3. Liver Injury and Uncontrolled Bleeding
Animals had a 3 cm transverse laparotomy, and 50% of the left lateral and medial liver lobes were resected with sharp dissection and allowed to bleed freely into the peritoneal cavity, as in previous studies [19,20]. This model of liver resection-induced non-compressible hemorrhage has been validated [23], and is more clinically relevant than other pressure- or volume-controlled hemorrhage models [24,25]. As the largest solid abdominal organ, the liver is susceptible to both blunt and penetrating injury, and subsequent non-compressible hemorrhagic shock [26,27]. Consistency of liver injury was ensured by comparing the weight of resected liver with total body weight (Saline NT: 0.52 ± 0.04%, ALM NT: 0.54 ± 0.05%, Saline FFP: 0.53 ± 0.04%, ALM FFP: 0.57 ± 0.06%, Saline FWB: 0.54 ± 0.07%, ALM FWB: 0.58 ± 0.05%; p = 0.117). Sham animals underwent surgical instrumentation, laparotomy and liver isolation, without resection and bleeding, to determine surgical trauma-induced responses in the absence of traumatic hemorrhagic shock.
2.4. Resuscitation and Transfusion
Fifteen minutes after liver injury, animals received a 0.7 mL/kg intravenous (IV) bolus of 3% NaCl (Saline and Sham) or 3% NaCl ALM (ALM; 1 mM adenosine, 3 mM lidocaine, 2.5 mM MgSO_4_; Sigma-Aldrich. Castle Hill, Australia [19]) via the femoral vein catheter (Figure 1). Animals were recovered from anesthesia after 60 min Phase 1 bolus resuscitation and received a 4 h infusion of 0.5 mL/kg/h 0.9% NaCl (Saline and Sham) or 0.9% NaCl ALM (ALM; 0.25 mg/kg/h adenosine, 0.5 mg/kg/h lidocaine, 0.25 mg/kg/h MgSO_4_ [19]) (Figure 1). After Phase 2 drip resuscitation was complete, animals received NT, FFP or FWB according to group allocation for Phase 3 transfusion. The timing of resuscitation and transfusion was chosen to reflect prehospital times for trauma patients in regional, rural and remote Australia, which are significantly prolonged (4–9 h) [28,29] compared to those in the United States [14,30] and Europe [31], which average 50–60 min. Northern Australia currently has very limited capability for prehospital transfusion due to availability and logistic challenges, with transfusion commencing on hospital admission, often hours after injury. FFP and FWB, equivalent to 20% total blood volume calculated from [(0.06 × weight) + 0.77] [32], warmed to 37 °C, were transfused at 0.25 mL/min through a Hemo-Nate Syringe Filter (Sound Veterinary Equipment; Rowville, Australia). Mean transfusion time was 21.7 ± 2.2 min. Animals were monitored for 72 h post-injury with administration of 0.7 mL/kg IV bolus of 0.9% NaCl (Saline and Sham) or 0.9% NaCl ALM (ALM; 1 mM adenosine, 3 mM lidocaine, 2.5 mM MgSO_4_) at 24 h and 48 h (Figure 1).
2.5. Preparation of FFP and FWB
FFP and FWB were prepared from donor syngeneic female Sprague-Dawley rats, matched according to breeding pair. Fresh shed citrated blood (FWB) collected from anesthetized donors was incubated at 37 °C with gentle rolling to maintain homogeneity until transfusion. For fresh frozen plasma (FFP), blood was left to sit at room temperature for 30 min, then passed through a neonatal leukocyte reduction filter (Nanodyne Filter 0.2 μm; Pall Corporation, Dandenong South, Australia) and centrifuged at 4000× g for 15 min [33]. Plasma was separated from red cells and stored at −80 °C until use.
2.6. Blood Sampling, Moribund Score and Mortality
Animals were continuously monitored for the first 6 h after liver injury and reconnected for hemodynamic monitoring every 12 h until 72 h. Blood was sampled at baseline (post-surgical instrumentation), end Phase 3 transfusion (6.25 h post-injury), and at 24 h, 48 h and 72 h for lactate, blood chemistry, complete blood count, and coagulation and platelet function assessments (Figure 1). Mortality was defined as MAP < 25 mmHg for 5 min. Animals were assessed twice daily using the humane endpoints of Morton [34], Toth [35], and Nemzek and colleagues [36]. Weight loss, behavior/alertness, mobility, appearance/coat condition, wound healing, breathing/respiration, food/water intake and feces were scored 0–3. Any animal scoring ≥10, or 3 in any category, was categorized as being in a moribund state preceding imminent death and was euthanized. Surviving animals were sacrificed at the end of the 72 h experimental period. At the time of sacrifice, animals were re-anesthetized with isoflurane for blood sampling from the femoral artery catheter, followed by euthanasia with 100 mg/kg IV pentobarbitone sodium (Lethabarb^®^; Virbac Australia; Milperra, Australia).
2.7. Blood Chemistry, Hematology, Coagulation and Platelet Function
Blood chemistry and lactate were measured using a Radiometer ABL800 analyzer (Radiometer Pacific; Mount Waverley, Australia), and VetScan HM5 (Zoetis Diagnostics; Rhodes, Australia) was used for complete blood counts, as in previous studies [18,20].
Prothrombin time (PT, s), activated partial thromboplastin time (aPTT, s), fibrinogen (g/dL), tissue activatable fibrinolysis inhibitor (TAFI, %), Protein C (%), and antiplasmin (%) were measured in citrated plasma on the STA Compact (Diagnostica Stago; Doncaster, Australia).
Rotational thromboelastometry (ROTEM^®^; Tem International, Munich, Germany) was conducted according to the manufacturer’s instructions and previous studies [20,37]. Whole blood collected in 3.2% sodium citrate tubes was warmed to 37 °C. Three assays were performed: EXTEM (extrinsically activated test using tissue factor), INTEM (intrinsically activated test using ellagic acid), and FIBTEM (fibrin-based EXTEM-activated test with 50 μg/mL cytochalasin D, to inhibit platelet contribution to clot formation).
Platelet function was assessed in platelet-rich plasma (PRP) using the PAP-8e Platelet Aggregation Profiler (BioData Corporation; Horsham, PA, USA) and agonists ADP (200 μM) and Collagen (equine tendon, 100 μg/mL) from Helena Laboratories (Mount Waverley, Australia). PRP was prepared using a standardized technique of double centrifugation [38].
2.8. Lung Histopathology
Sections of lung collected at the time of sacrifice were fixed in 10% neutral buffered formalin, processed, and paraffin-embedded. Six 4 μm paraffin-embedded sections were cut from each block, spaced at 100 μm intervals and spanning the entire tissue sample. Alternate sections (2nd, 4th and 6th sections) were stained with hematoxylin and eosin (H&E). Stained sections were visualized with light microscopy (Nikon Eclipse i50; Nikon, Tokyo, Japan) and digitized (Nikon NIS-Elements Basic Research Software) for semi-quantitative assessment of pathological changes. Lungs were examined for vacuolation, alveolar infiltration, inflammation, hemorrhage/congestion, and epithelial degeneration. Sections were scored from 0 to 4 (none-severe, >80% tissue affected) for each parameter by two blinded investigators (total possible score = 20).
2.9. Statistical Analysis
A priori power analysis was conducted using the G-power^3^ program (Heinrich Heine University Düsseldorf; Düsseldorf, Germany) to determine the minimum sample size to minimize Type 1 errors (outcome measure = MAP 6.25 h post-injury [19]; effect size = 1.33; α err prob = 0.05; Power (1-β error prob) = 0.8; calculated sample size n = 10). SPSS Statistical Package 25 was used for all statistical analyses (IBM, Sydney, Australia). Survival was assessed using the Kaplan–Meier method with a log-rank test for comparison between groups. Data normality was assessed graphically and with the Shapiro–Wilk test. Data are expressed as mean ± standard deviation (SD). Normally distributed data were analyzed using one-way analysis of variance (ANOVA). Longitudinal data were assessed with General Linear Model Repeated Measures ANOVA. Within-group differences were assessed using a paired-samples t-test. Non-parametric data were analyzed using a Kruskal–Wallis test followed by Dunn’s test. Point-biserial correlations were conducted to determine the relationship between continuous variables and mortality. Statistical significance was defined as p < 0.05.
3. Results
3.1. Survival
Survival in Sham, Saline and ALM NT groups was 50%, 0% and 100%. Saline NT had significantly reduced mean survival time (23 h) compared to Sham (53 h) and ALM (72 h) (p < 0.05) (Table 1, Figure 2). FFP increased Sham survival to 75%, with no change after FWB (50%). FFP and FWB increased overall survival in Saline controls from 0% to 8% and 17%, respectively, but did not increase survival time (16 h and 19 h). In contrast to 100% survival to 72 h in the ALM NT group, ALM FFP and ALM FWB had significantly reduced survival (8%, 34 h and 0%, 22 h, respectively) (p < 0.05) (Table 1, Figure 2).
3.2. Hemodynamics
Liver resection and uncontrolled bleeding led to a marked ~50% fall in MAP (p < 0.05 vs. Sham groups), which recovered at 15 min Phase 1 with a 0.7 mL/kg bolus of 3% NaCl or 3% NaCl ALM (Supplementary Figure S1A). There were no significant differences in heart rate (HR) between groups during Phases 1–3, or in survivors and non-survivors during the 72 h monitoring period (Supplementary Figure S1B). MAP and HR increased after Phase 1 when animals were recovered from anesthesia, and there was a trend towards higher HR at 36 h and 60 h (evening measurements) compared to 48 h and 72 h (Supplementary Figure S1A,B).
3.3. Blood Lactate and Chemistry
Saline NT and FFP animals, and all FWB animals that died early (Phase 1–2), were profoundly acidotic with blood pH ranging from 6.7 to 7.14, and high lactates (7–20 mM) (Table 2). In contrast to other groups that became moribund from Phase 3 to 24 h, which had significantly increased lactates and reduced pH, ALM FWB non-survivors during the same period had no change in blood pH (7.44) or lactate (1.65 mM). After 24 h, pH returned to 7.3–7.6 in non-survivors (except Sham FFP), but lactates remained elevated. In addition to prolonged acidemia, Sham FFP survivors had increased lactate at 72 h compared to all other groups (3.76 vs. <1.8 mM) (Table 2).
Survivors also had blood K^+^ levels comparable to baseline (~4.5 mM), whereas K^+^ increased up to 14.25 mM in moribund animals (Supplementary Table S1). Blood Na^+^ and Cl^−^ increased in earlier moribund groups (Phase 1–2), and after transfusion (Phase 3) in Sham and Saline FFP and FWB groups, but not ALM FFP and FWB. ALM FFP and FWB animals that died after 24 h also maintained normal base excess and bicarbonate, compared to other moribund groups, which showed marked falls (Supplementary Table S1).
3.4. Red Cell and Platelet Profile
Survivors at 72 h had significant 30–37% decreases in red blood cell (RBC) numbers and hematocrit (Hct), and 29–39% falls in hemoglobin (Hb) (Table 3). Non-survivors had similar percentage falls of up to 30% in RBC, Hb and Hct, except for ALM FWB, which only dropped 5–10%. At 72 h, platelet numbers in Sham NT, FFP and FWB survivors fell by 53%, 36% and 53% from baseline, respectively (Table 3). There was a significant negative correlation between platelet count from Phase 1 to 24 h and survival time (rpb = −0.451; p = 0.010). Sham and Saline animals that became moribund after 24 h had 54–95% and 80–94% falls in platelet numbers, respectively. Total platelets fell in ALM FFP and ALM FWB non-survivors at 24–48 h by 16% and 35% respectively, whereas platelet count in ALM NT survivors was only 7% lower than baseline (Table 3).
3.5. White Blood Cell (WBC) Profile
Total white cell count at 72 h in ALM NT group with 100% survival was comparable to baseline (10.68 × 10^9^/L vs. 12.19 × 10^9^/L), compared to a 25% decrease in WBCs in Sham NT survivors (Table 4). Transfusion of FWB in Shams led to a more profound leukopenia at 72 h (48% fall), whereas FFP preserved WBC in Shams (11% increase vs. baseline at 72 h). White cells fell significantly in all FFP and FWB moribund groups between 24 and 72 h (<2.85 × 10^9^/L), indicating immunosuppression; however, in contrast to the Saline NT group, which showed an exponential early decrease in WBC, FFP or FWB appeared to defend against these large falls in the first 48 h (Table 4).
Similar to WBC, Sham survivors also had 33–67% falls in lymphocytes, and 38–45% falls in monocytes, with the exception of Sham FFP animals, where circulating monocytes increased 1.35-fold at 72 h (Table 4). In the Saline and ALM groups, lymphocytes fell significantly in both survivors and non-survivors. Monocytes also decreased in Saline and ALM moribund groups (Table 4). Neutrophils increased 1.3 to 2.2-fold from baseline to 72 h in all survivors; however, there was no evidence of neutrophilia in moribund groups after 24 h. The neutrophil/lymphocyte ratio was increased in both survivors and moribund groups, including 4- to 16-fold increases in Sham survivors, 3.4- to 6-fold and 4- to 20-fold in Saline survivors and non-survivors, and 5.2-fold and 2.9- to 5.4-fold in ALM survivors and non-survivors, with no differences between NT, FFP, and FWB (Table 4). The monocyte/neutrophil ratio at 72 h fell 48–70% in Shams, and 80–86% in Saline FFP and FWB, compared to only 25% in ALM NT with 100% survival.
3.6. Coagulation
PT remained relatively constant except for the early FWB deaths (Phase 1–24 h), where it increased 3- to 8-fold (Table 5). In contrast, aPTT in all NT groups increased up to 2.6-fold, and similar prolongation was found after FFP and FWB transfusion, indicating hypocoagulopathy, which was not corrected until 72 h. These results were very similar to the small changes in EXTEM clot time (CT) and increases in INTEM CT in non-survivors (Table 5 and Table 6). In contrast to the correction of aPTT in survivors, the INTEM ROTEM equivalent showed increases at 72 h, indicating persistent hypocoagulopathy. However, maximum clot firmness (MCF) and maximum lysis (ML) indicated that the clots were stable with little hyperfibrinolysis (Table 6). Sham NT had a 3.5-times prolongation of INTEM CT, which was reduced by ~50% after FFP (1.24-times) or FWB (1.6-times).
Fibrinogen fell significantly by ~70% in early deaths to 24 h, but increased 2.5 times in 72 h survivors (p < 0.05 vs. baseline), which was consistent with FIBTEM results (Table 5 and Table 6). The increase occurred in the first 24 h and appears to remain high for 3 days. Similar to fibrinogen, TAFI levels increased up to 2-fold in survivors at 72 h (Table 5). In early moribund groups (Phase 1–24 h), no change in TAFI occurred with the exception of ALM FWB, which fell by 50% (p < 0.05 vs. ALM NT and FFP). In contrast, TAFI increased by 1.3 to 1.5-fold in Sham FWB and Saline FWB over the same period (p < 0.05 vs. ALM FWB), and almost doubled in ALM NT group to 112% at 24 h and 119% at 72 h. Protein C in early moribund groups (Phase 1–24 h) for Saline NT and ALM FWB underwent no change, whereas Saline FWB and all FFP groups increased 3- to 6-fold to 48 h (Table 5). Transfusion of FWB significantly reduced Protein C levels at 24–72 h with falls of 57%, 67% and 87% in Sham FWB, Saline FWB, and ALM FWB, respectively. Early deaths (Phase 1–24 h) were associated with reduced antiplasmin, except ALM FWB, which was comparable to baseline. Antiplasmin fell by 35% in the Sham NT group and did not recover, but increased by 15% and 37% in Sham FFP at 24 h and 72 h, respectively (Table 5). Antiplasmin also increased 1.5 to 1.8-fold in ALM NT and Sham FWB survivors.
3.7. Platelet Function
ADP-induced primary platelet aggregation (ADP PA), defined as the extent of aggregation during the first minute, for Sham NT survivors was 13% lower than baseline (79 vs. 91%), whereas Sham NT non-survivors fell by 69% (Figure 3). Platelet aggregation was restored in Sham FFP and FWB survivors (1.1-times baseline), but fell by 31% and 93% in Sham FFP and FWB non-survivors, respectively. Similarly, the addition of FFP or FWB in Saline survivors restored platelet aggregation to ~1.3-times baseline, compared to falls of 83–93% in non-survivors (p < 0.05 vs. ALM NT). ALM NT aggregation was 1.27 × baseline, and all survived, whereas aggregation in ALM FFP and FWB non-survivors were 45% and 35% of baseline (Figure 3). ADP PA was very strongly correlated with survival (rpb = 0.857; p < 0.0001) and strongly correlated with survival time (rpb = 0.766; p < 0.0001). Collagen-induced platelet aggregation showed similar findings, including strong positive associations with survival (rpb = 0.667; p < 0.0001) and survival time (rpb = 0.627; p < 0.0001).
3.8. Lung Pathology
Total lung injury scores were significantly higher in Sham FWB, Saline FFP, ALM FFP, and ALM FWB compared to all NT groups (Figure 4A). Lung injury score showed a weak significant correlation with mortality (rpb = 0.296; p < 0.012), while hemorrhage/congestion score was moderately associated with death (rpb = 0.330; p < 0.005). ALM FFP had significantly increased hemorrhage and inflammation compared to ALM NT, and all ALM FWB animals showed mild-to-moderate hemorrhage and epithelial degeneration (p < 0.05 vs. ALM NT) (Figure 4B). ALM FWB animals had a distinct gross pathophysiological profile of lung congestion, edema, and excess pericardial fluid. No such lesions or congestion were found in the ALM NT group.
4. Discussion
Uncontrolled hemorrhage remains a leading cause of potentially survivable death in prehospital civilian and military environments [1,2,3]. We have previously shown that small-volume ALM therapy can resuscitate, correct trauma-induced coagulopathy, and provide multiple organ protection, in both small and large animal models of traumatic hemorrhage [17,18,19,20,21,39]. We report in the rat model of laparotomy, liver resection and uncontrolled hemorrhage, that transfusion of 20% total blood volume of FFP or FWB 5 h after resuscitation with ALM therapy reduced 72 h survival. In contrast, ALM without transfusion led to 100% survival. Mortality appeared to be related to transfusion-related acute lung injury (TRALI), reduced platelet function, metabolic and immune dysfunction, and hypocoagulopathy. We also found that surgical and abdominal trauma from laparotomy and liver isolation was a major contributor to poor outcomes because Shams (no hemorrhage) had similar profiles. Higher systemic fibrinogen levels in survivors and non-survivors appeared to be due to activation of the innate immune response induced by surgical trauma. These results are discussed next.
4.1. Sham Mortality Was Due to the Trauma of Surgery, Not Hemorrhage
An unexpected result was that 50% of Sham animals that did not receive a transfusion died, which was slightly improved after FFP infusion (75% survival), but not with FWB. Shams underwent anesthesia, surgical catheterization involving groin and neck cut-downs, a 3 cm open laparotomy, and liver isolation, but no resection. Our data emphasize the importance of including Shams to accurately interpret the physiological responses to resuscitation therapies in animal models. Unfortunately, many preclinical studies investigating blood product transfusion efficacy either do not include Shams or they are not present for the entire experiment [40,41,42], which may lead to contradictory results in the literature.
4.2. ALM Therapy Led to 100% Survival Without Blood Products
The other unexpected finding of our study was that transfusion of FFP or FWB 5 h after ALM resuscitation resulted in higher mortality than ALM alone, which led to 100% survival after 3 days. Possible reasons include the timing of transfusion, currently unknown contraindications, as well as the effect of these blood products on lung pathology and immune function, and are discussed below. Similarly, FFP or FWB failed to improve survival in Saline controls, although the sample sizes were smaller due to high early mortality prior to the transfusion phase. The limited resuscitative and hemostatic capacity of saline alone is supported by previous studies [37,43,44].
4.3. FWB and FFP Led to Poor Outcomes in All Groups
Mortality in FFP and FWB groups appeared to be associated with TRALI, which was not apparent in groups without transfusion. In addition, lung hemorrhage was not present in the Sham group that did not receive blood products, confirming that this effect was directly related to transfusion. Mortality in ALM animals receiving FWB or FFP was accompanied by pulmonary congestion and hemorrhage, edema, inflammation, and epithelial degeneration, which may be associated with varying degrees of early or delayed TRALI. The pathophysiology of TRALI is believed to arise from a breach of endothelial, interstitial, and epithelial barriers driven by inflammation and exacerbated by fluid therapies, leading to extravasation of proteinaceous fluid into the airspace [45], and similar to the pathology we observed. Our findings are consistent with studies reporting TRALI and acute respiratory distress syndrome (ARDS) following both FFP and FWB administration after hemorrhagic trauma [40,46].
4.4. Mortality, Platelet Exhaustion and Coagulopathy
In addition to transfusion, another important factor associated with mortality was a dramatic loss of ADP- and collagen-induced platelet aggregation. Our findings of a significant strong correlation between both ADP- and collagen-induced primary platelet aggregation are consistent with clinical studies reporting reduced platelet function in trauma patients, which was associated with increased mortality (up to 10-fold) [47,48]. An “exhausted platelet syndrome” begins with an initial hyperactivation of platelets from the widespread release of ADP from injured endothelial cells, which subsequently become unresponsive via mechanisms not well understood [49]. Loss of platelet aggregation may also be exacerbated by reduced platelet numbers. Since Sham NT non-survivors had 69% and 93% falls in platelet aggregation and count, respectively, we conclude that reduced platelet function was most likely due to surgical trauma [50], not the use of blood products or hemorrhage. This illustrates the complexity of our polytrauma model, on one hand, and yet its ability to tease apart the different mechanisms contributing to death after hemorrhagic shock, on the other.
Platelet exhaustion was also associated with hypocoagulopathy in all groups, as indicated by a prolonged aPTT and prolonged INTEM clot times, with some failing to form a clot. The use of FFP or FWB partially corrected hypocoagulopathy, with reduced INTEM clot times and improved INTEM and FIBTEM clot firmness. Stronger clots after administration of blood products are often supported by higher circulating fibrinogen levels, which is consistent with significantly higher FIBTEM MCF. However, increased fibrinogen normally favors platelet aggregation by binding to platelet GPIIb/IIIa receptors [51], yet this was not the case in our moribund animals with or without blood products. How do we explain this paradox? One possibility is that the 2- to 2.8-fold increase in systemic fibrinogen, irrespective of treatment, was part of the positive acute-phase response to inflammation, trauma, and/or tissue damage, separate from its effect in combining with platelets and forming strong clots [52]. Once present in blood, fibrinogen and other acute-phase proteins, such as C-reactive protein, C3 complement and alpha-globulin glycoprotein, can in turn modulate the inflammatory response via the recruitment of immune cells and cytokine production [52]. This may also be related to the leukopenia and lymphopenia we found over the 72 h experimental period, and may contribute to a trauma-induced immunosuppression. Thus, we conclude that viscoelastic INTEM and FIBTEM parameters in vitro do not necessarily imply that increased clot firmness is occurring in vivo, given impaired platelet aggregation, reduced platelet count, and 50% falls in platelet/fibrinogen ratios that are incompatible with the formation of viable clots. This linkage between acute-phase response to trauma, inflammation and coagulopathy is an area that requires further study.
4.5. Survivors Preserved Platelet Aggregation and Reduced Coagulopathy and Immune Activation
In contrast to non-survivors, platelet aggregation in survivors was maintained close to baseline, regardless of the use of blood products. Maintenance of platelet aggregation in survivors occurred despite ~50% falls in platelet numbers in most groups. Preserved platelet function was also associated with reduced coagulopathy among the survivors, including normal PT, aPTT, EXTEM and FIBTEM clot times, as well as a recovery of INTEM CT towards baseline. This is consistent with what is now known about the significant contribution platelet dysfunction makes to early trauma-induced coagulopathy (TIC) and the potential limitation of FFP alone [10].
Key to ALM therapy survival, in addition to preservation of platelet function, was attenuation of immune activation, reduced blood lactate and normal acid-base status. Immune dysfunction and hyperinflammation after traumatic injury and hemorrhage are important contributors to secondary injury progression, including immunosuppression, infection and development of multiple organ dysfunction, including lung injury [53]. Trauma-induced immune dysfunction and inflammation may, in turn, be exacerbated by blood product administration, an effect known as transfusion-associated immunomodulation (TRIM) [54]. It is possible in this study that delayed administration of FFP or FWB after successful resuscitation, correction of TIC and stabilization with ALM therapy led to a “second-hit” injury.
4.6. Clinical Significance and Limitations
While administration of fresh whole blood in humans appears to offer clinical advantages over balanced component therapy (red blood cells, plasma, and platelets) [55], the quality of the data is poor, and more high-quality studies are required [3,56]. In our rat model, transfusion with FWB or FFP 5 h after fluid resuscitation surprisingly led to poor outcomes, which may be a reflection of the severity of our model and timing of transfusion, with multiple clinical studies demonstrating benefit with earlier transfusion [57,58,59]. Our preclinical model combining uncontrolled hemorrhage with a laparotomy and liver manipulation had a high mortality and high individual variability, which limited time-matched comparisons of all endpoints. Despite this, the model may have military significance in Role 2 facilities where casualties with suspected abdominal hemorrhage requiring an emergent laparotomy have high mortality rates [60]. Our data showing that ALM therapy alone was effective against non-compressible hemorrhage and major surgical trauma with 100% survival is directly relevant to battlefield medicine and forward surgical facilities when blood products may be in short supply. In addition to the model’s severity, another limitation of our study was that the individual effects of FFP or FWB alone were not tested in our model. Finally, in order to comply with ethical restrictions and the 3Rs of preclinical studies, only male rats were evaluated, with female rats used exclusively as donors for blood products. Despite no current evidence in rats, clinical studies have shown that sex-mismatched transfusion is associated with increased mortality [61]. Further studies are required to determine any sex-specific differences, particularly relating to sex hormones and transfusion-induced immunoinflammatory responses.
5. Conclusions
In the rat model of laparotomy, liver resection, and hemorrhage, Sham groups had 25–50% mortality, indicating that the trauma of surgery was a significant contributor to poor outcomes. ALM resuscitation therapy without blood products led to 100% survival, and was associated with improved hemostasis, platelet aggregation and metabolic and immune function. Our study showed that ALM protection was lost with administration of FFP or FWB, which led to reduced survival, and was related to acute lung injury, platelet exhaustion, hypocoagulopathy, and transfusion-associated immunomodulation. Further studies are required to evaluate the underlying mechanisms and to assess the clinical significance of our findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Eastridge B.J. Mabry R.L. Seguin P. Cantrell J. Tops T. Uribe P. Mallett O. Zubko T. Oetjen-Gerdes L. Rasmussen T.E. Death on the battlefield (2001–2011): Implications for the future of combat casualty care J. Trauma. Acute Care Surg.201273 S 431S 43710.1097/TA.0b 013e 3182755 dcc 23192066 · doi ↗ · pubmed ↗
- 2Spinella P.C. Cap A.P. Prehospital hemostatic resuscitation to achieve zero preventable deaths after traumatic injury Curr. Opin. Hematol.20172452953510.1097/MOH.000000000000038628832355 · doi ↗ · pubmed ↗
- 3Brunskill S.J. Disegna A. Wong H. Fabes J. Desborough M.J.R. Dorée C. Davenport R. Curry N. Stanworth S.J. Blood transfusion strategies for major bleeding in trauma Cochrane Database Syst. Rev.20254 CD 01263510.1002/14651858.CD 012635.pub 240271704 PMC 12019925 · doi ↗ · pubmed ↗
- 4Anand T. Shin H. Ratnasekera A. Tran M.L. Huckeby R. Butts L. Stejskal I. Magnotti L.J. Joseph B. Rethinking balanced resuscitation in trauma J. Clin. Med.202514211110.3390/jcm 1406211140142918 PMC 11943041 · doi ↗ · pubmed ↗
- 5Bloch E.M. Jacobs J.W. Sachais B.S. Ziman A. Cushing M. Cap A.P. Gurney J.M. Beckett A. Yazer M.H. Spinella P.C. Revisiting whole blood transfusion for the massively bleeding patient: The origins of resistance to change Transfusion 2025 Online Ahead of Print 10.1111/trf.70002 PMC 1269664041235916 · doi ↗ · pubmed ↗
- 6Cap A.P. Pidcoke H.F. De Pasquale M. Rappold J.F. Glassberg E. Eliassen H.S. Bjerkvig C.K. Fosse T.K. Kane S. Thompson P. Blood far forward: Time to get moving!J. Trauma. Acute Care Surg.201578 S 2S 610.1097/TA.000000000000062626002259 · doi ↗ · pubmed ↗
- 7Dobson G.P. Morris J.L. Davenport L.M. Letson H.L. Traumatic-induced coagulopathy as a systems failure: A new window into hemostasis Sem. Thromb. Hemost.20204619921410.1055/s-0039-170101832069514 · doi ↗ · pubmed ↗
- 8Holcomb J.B. Tilley B.C. Baraniuk S. Fox E.E. Wade C.E. Podbielski J.M. del Junco D.J. Brasel K.J. Bulger E.M. Callcut R.A. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma JAMA 201531347148210.1001/jama.2015.1225647203 PMC 4374744 · doi ↗ · pubmed ↗