Predictability of Severity Scores in Patients over 70 Years Old with COVID-19 Infection: Results from a Single-Center Retrospective Observational Study
Andreea Magdalena Ghibu, Ionela Maniu, Victoria Birlutiu

TL;DR
This study evaluates how well different severity scores predict mortality in elderly patients with COVID-19.
Contribution
It compares the predictive accuracy of five severity scores in patients over 70 years old with SARS-CoV-2 infection.
Findings
PADUA score had the highest predictive accuracy (AUC of 0.914) for mortality in elderly patients with COVID-19.
Tumor pathology, ICU admission, and mechanical ventilation were significant risk factors for increased mortality.
PSI, MuLBSTA, and PADUA scores showed acceptable prediction ability for mortality in this population.
Abstract
Background: The elderly remain a population group at risk of developing severe forms of SARS-CoV-2 infection. Age and the prevalence of comorbidities are important risk factors for mortality related to COVID-19. Severity scores enhance medical practice, proving to be useful tools in predicting mortality. Objectives: The purpose of this study is to assess the predictive accuracy of the CURB-65, Pneumonia Severity Index, MuLBSTA, COVID-GRAM and PADUA scores in patients over 70 years of age diagnosed with SARS-CoV-2 infection. Methods: We performed a retrospective study between June 2023 and December 2024, analyzing demographic data, vaccination status, comorbidities, discharge status, and computed the five scores. Results: A total of 173 patients aged over 70 years old were included in the study. Among them, 56.06% were male with a median age of 79.72 ± 6.55. Many patients had at least…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1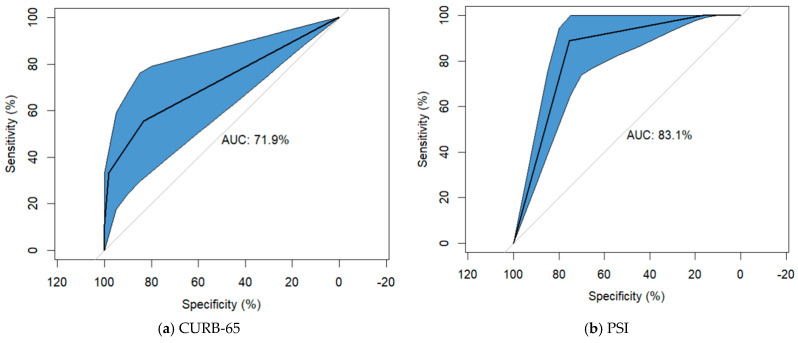 Figure 2
Figure 2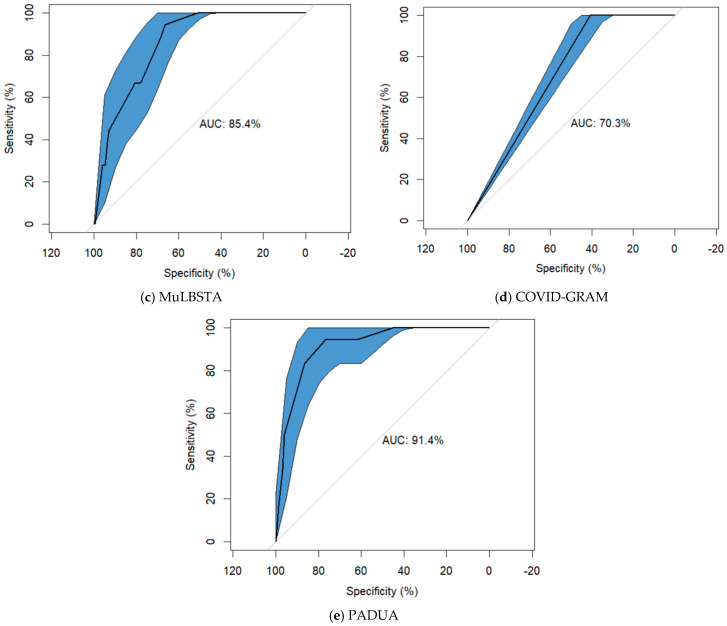 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 Clinical Research Studies · COVID-19 and healthcare impacts · Long-Term Effects of COVID-19
1. Introduction
The first case of SARS-CoV-2 infection in Wuhan, China and the quick spread of this virus led to a pandemic with global implications [1,2]. From that moment until now (1 December 2025), 778,922,858 cases of COVID-19 have been reported, with 7,103,341 deaths according to the World Health Organization, and Europe and the Western Pacific region being most affected [3].
In Europe, most cases of infection reported in 2025 were recorded in Greece, Poland, and the Czech Republic. In Romania, 2200 cases were diagnosed and 20 deaths were recorded (eighth and fourth place in Europe, respectively). Most infections were reported in older people over 65, predominantly male, with or without comorbidities [3]. The continued spread of the virus and the emergence of new strains, correlating with older age, comorbidities, immunization status and the clinical status of patients on admission, highlights the necessity of using predictability scores in clinical practice [4,5]. Currently, no score has been developed for elderly patients, who remain at risk of developing severe forms of the disease and, consequently, a higher risk of mortality. Identifying a score or key parameters as predictors of mortality in this age group would significantly improve management and also provide an important base for managing future pandemics [6].
The literature identifies several scores used in the prognosis of this infection, whose accuracy has been proven or not over time. The CURB-65 score, created to assess the need for hospitalization in patients with pneumonia, is a tool often used in COVID-19 infection, including five easily assessed parameters (Appendix A Table A1) [7]. The Pneumonia Severity Index is a complex severity score that combines anamnestic elements with clinical and biological parameters, classifying patients into five risk groups (Appendix A Table A2) [8]. MuLBSTA is also an easy-to-use score that evaluates six parameters to predict the 90-day mortality of patients with COVID-19 (Appendix A Table A1) [9]. Moreover, the COVID-GRAM score stratifies patients with COVID-19 infection into three risk groups, evaluating, in addition to the above-mentioned parameters, the presence of lung damage, having been created for viral pneumonia (Appendix A Table A2) [10]. Considering the procoagulant status of the SARS-CoV-2 infection, the PADUA score evaluates 11 parameters, including age over 70 years, with a score above four pointing to being associated with an increased risk of embolism (Appendix A Table A1) [11].
These scores are useful tools for clinicians to quantify mortality in patients with this type of infection in a high-risk age group. The elderly are more susceptible to severe forms of the disease, as they often have several comorbidities and a higher risk of death from infection. The purpose of this study is to assess the performance of these scores to predict mortality in patients over 70 years old with SARS-CoV-2 infection hospitalized in our department.
2. Materials and Methods
2.1. Study Design
We conducted a retrospective, observational study in a single center among patients diagnosed with SARS-CoV-2 infection between 1 June 2023 and 31 December 2024, admitted to the Infectious Diseases Clinic of Academic Emergency Hospital Sibiu. This study was conducted in accordance with the Declaration of Helsinki and with the approval of the Ethics Committee of the “Lucian Blaga” University of Sibiu No. 4/25.07.2022, No. 26/16.06.2025 and Academic Emergency Hospital Sibiu No. 32143/22.12.2021.
2.2. Participants
A sample of 173 patients diagnosed with SARS-CoV-2 infection by an antigen test or RT-PCR was included in the current study, representing patients over 70 years of age (Figure 1). Patients under the age of 70, patients diagnosed with SARS-CoV-2 infection in other hospital wards but not transferred to the Infectious Diseases Department, and patients with incomplete/unavailable laboratory parameters, medical history or clinical data were excluded.
2.3. Data Sources
After the completion of the selection process, data were manually extracted from patient records. We took into consideration data related to symptoms, vital signs and level of consciousness evaluated in ED and recorded in patient documentation. Scores were calculated using parameters available at baseline.
Demographic data were analyzed, including place of origin, age, gender, vaccination status (including dose number), length of hospitalization, admission to the Intensive Care Unit, ventilation modes and status at discharge. Imagistically, patients were evaluated by chest X-ray and computed tomography, establishing the pulmonary involvement. The imaging data obtained during the patients’ initial assessment in the emergency department was taken into account, given that the majority of our hospitalized patients had initially passed through this department.
Comorbidities were classified into cardiovascular diseases (including hypertension, ischemic heart disease, and cardiac arrhythmias), nutritional status (based on the body mass index), metabolic disorders (e.g., type 1 and 2 diabetes mellitus), neurological disorders (e.g., sequelae of stroke, Parkinson’s disease, epilepsy), tumor pathology (e.g., colon, rectal, lung, renal neoplasm, hepatocellular carcinoma), endocrine (e.g., hypothyroidism, hyperthyroidism, autoimmune disorder), digestive (e.g., ulcer, gastritis, inflammatory bowel disease), urological, and psychiatric disorders (e.g., depression, psychosis, schizophrenia). All this information and patient history was taken from anamnesis which was performed at the admission in our department.
Furthermore, the following severity scores were calculated: CURB-65, MuLBSTA, Pneumonia Severity Index, COVID-GRAM, PADUA (Appendix A). All these data were input into a Microsoft Office Excel dataset. The primary outcome was to evaluate the accuracy of these scores regarding in-hospital mortality.
2.4. Statistical Analysis
The data are presented as mean and SD (standard deviation) or median and IQR (interquartile range) for continuous variables. Percentages were used for nominal variables. Comparison between survivor and non-survivor groups was assessed by a chi-square test in the case of categorial variables and the Mann–Whitney test for continuous variables. ROC (Receiver Operator Characteristic) curves were used to assess the prognostic ability of severity scores CURB-65, Pneumonia Severity Index, MuLBSTA, COVID-GRAM, and PADUA to predict mortality. Measures of diagnostic accuracy—SE (sensitivity), SP (specificity), PPV (positive predictive value), and NPV (negative predictive value)—for different cut-offs of severity scores are reported. Additionally, univariate and multivariate logistic regression models were built to assess mortality, with model 1 (M1) not adjusted for any variables, model 2 (M2) adjusted for vaccination, model 3 (M3) adjusted for tumor pathology, model 4 (M4) adjusted for ICU, model 5 (M5) adjusted for ICU and tumor pathology, model 6 (M6) adjusted for ICU, tumor pathology and vaccination, and model 7 (M7) adjusted for ICU, tumor pathology, vaccination and age. The statistical analysis was performed using R software (v. 4.5.2.) and SPSS (v. 19). The considered value for statistical significance was p < 0.05.
3. Results
Of the 173 patients included in the study, 56.06% were male, mainly from urban areas (73.41%), with the average age of 79.72 (SD = 6.55). There were 155 (89.60%) survivors and 18 (10.40%) patients died. The median age in the survivors group was 79.54 ± 6.51, and among deceased patients, it was 81.28 ± 6.9. Many patients had at least one comorbidity (93.06), 67.63% (117) patients with hypertension, 28.90% (50) with diabetes mellitus, 28.32% (49) with obesity and 41.61% (72) with previous neurological pathology. There were fewer patients with chronic kidney disease or tumor pathology. Tumor pathology was associated with a higher risk of death (p = 0.002). A total of 109 of the patients were vaccinated against COVID-19. Among them, 10 patients were vaccinated with a single dose, 25 with two doses and 74 patients had also received a booster shot. Admission to intensive care and initiation of mechanical ventilation were important factors in predicting mortality, being statistically significant (p < 0.05) (Table 1).
The central tendencies of the risk scores CURB-65, PSI, MuLBSTA, GRAM-COVID, and PADUA are presented in Table 1. The values of severity scores were significantly higher in the non-survivor group when compared to survivors (Table 2).
The ROC curve analysis was performed to assess the discrimination accuracy of the severity scores. The AUC for the PADUA score was 0.914 (95%CI: [0.856–0.971], p < 0.001), while the sensitivity associated with the cut-off value > 4 was 94.44% (95%CI: [72.71–99.86]) and a specificity of 61.94% (95%CI: [53.80–69.61]). The MuLBSTA score had the AUC of 0.854 (95%CI: [0.785–0.922], p < 0.001), with the sensitivity associated with the cut-off value > 12 of 66.67% (95%CI: [40.99–86.66]) and a specificity of 78.06% (95%CI: [70.72–84.31]). In case of PSI score the AUC was 0.831 (95%CI: [0.748–0.915], p < 0.001), with the sensitivity associated with the cut-off value > 4 of 100.00% (95%CI: [81.47–100.00]) and a specificity of 16.77% (95%CI: [11.26–23.60]). For the CURB-65 score, the AUC was 0.719 (95%CI: [0.571–0.867], p = 0.002) with the sensitivity associated with the cut-off value ≥ 3 of 55.56% (95%CI: [30.76–78.47]) and a specificity of 83.23% (95%CI: [76.40–88.74]). The COVID-GRAM score had the AUC of 0.703 (95%CI: [0.608–0.799], p = 0.005) with the sensitivity associated with the cut-off value ≥ 3 of 100.00% (95%CI: [81.47–100.00]) and a specificity of 40.65% (95%CI: [32.84–48.82]) (Table 3, Figure 2).
The results of unadjusted analysis, showed that all five scores were significantly associated with mortality. After adjusting for ICU admission, tumor pathology, and vaccination status, the PADUA (aOR 2.528), PSI (aOR 1.031), and MuLBSTA (aOR 1.365) scores remained independent predictors of death (Table 4).
4. Discussion
Our study compares five severity scores in a cohort of patients with SARS-CoV-2 infection in terms of in hospital mortality. To our knowledge, the predictive value of the CURB-65 score has been evaluated before in the Romanian population; however, it has not been evaluated for Pneumonia Severity Index, MuLBSTA, COVID-GRAM, and PADUA. This study is a retrospective, observational study that evaluates the predictability of those scores among patients over 70 years old with the COVID-19 infection and admitted to the Infectious Diseases Department of the Academic Emergency Hospital Sibiu. A mortality rate of 10.4% was obtained, which is lower than in previous reports that analyzed all age groups [12,13,14]. The antiviral therapies and vaccination of patients could decrease the fatality rate. However, a significant number of patients, representing 36.99% of the study group, did not opt for vaccination, most of them coming from urban areas, which leads to a continued vulnerability in this group. Males remain the most affected, correlating with data from the literature [15,16,17,18,19]. Furthermore, studies showed that the use of antibiotics did not significantly improve the risk of death, independently of the timing of patients’ referral [20]. Previous exposure to antibiotics causes disturbances in the gut microbiota, as well as disruptions in the immune response to vaccination. McAlister et al. concluded that patients who received antibiotics in the last three months developed severe forms of the disease with poor 30-day outcomes after the patient was diagnosed with the COVID-19 infection [21,22].
The patients included in the study presented various pathologies, hypertension (67.63%), neurological pathology (41.61%), diabetes mellitus (28.90%) and obesity (28.32%). Hypertension was also the most common comorbidity identified in patients with COVID-19 [23]. Tumor pathology and chronic kidney disease were identified in a lower proportion, which is in accordance with the literature on this subject [24,25,26,27,28]. Among patients with tumor pathology, almost half died, which emphasizes the fact that immunodeficiency is a negative prognostic factor. Rodriguez-Nava et al. highlight, in a cohort of 313 patients, that 85% of the patients analyzed had at least two significant comorbidities, a finding that was also observed in our study [29]. Furthermore, admission to the intensive care unit (77.77% vs. 5.80%) and mechanical ventilation were negative prognostic factors and were also associated with an increased risk of mortality.
In our study, the CURB-65 score achieved an AUC of 0.719 (95% CI: [0.571–0.867], p = 0.002), a high specificity of 83.2% at a cut-off point of 3, but the lowest sensitivity of 55.5%. Our results are in line with those obtained by Su et al. This could be explained by the fact that although it includes age as a risk factor, it does not assess comorbidities. Although it has the lowest sensitivity, the CURB-65 score has the benefit of including a single laboratory parameter, which makes it easier to calculate [30]. A similar AUROC value was observed in the study conducted by Knight et al. on a cohort of 35,463 patients with a mean age of 73 years [31]. Citu et al. demonstrated good predictability of the CURB-65 score (AUC: 0.801; 95% CI: [0.681–0.922], p < 0.001) [32] regarding mortality, with a similar result obtained by Amr Elmoheen et al. in a study involving 1181 patients [8,33]. Its mortality predictive value is also preserved at 30 days, as highlighted by Lucijanić et al. [34].
In a study conducted on a cohort of 10,238 patients, comparing the CURB-65, PSI, MuLBSTA, and qSOFA scores, Arturo et al. highlighted the superiority of the PSI score in predicting mortality, which can also be observed in our study [33,35]. The performance of the PSI score in relation to the CURB-65 score was also highlighted in the study performed by Bradley et al. on a group of 8081 patients in 2022, also achieving slightly better ROC curve by associating d-dimers and procalcitonin [36,37]. Felippe Lazar Neto et al. in 2021 also highlighted, in a comparative analysis of PSI, CURB, CURB-65, COVID-GRAM, IDSA/ATS Minor Criteria, qSOFA, SCAP, SMART-COP, REA-ICU, CALL, and 4C scores, the superiority of PSI (AUC: 0.79; 95% CI: [0.77–0.82]) with a sensitivity of 0.90 (95% CI: [0.86–0.93]) and a specificity of 0.49 (95% CI: [0.46–0.52]). This could be a future direction to explore and verify the predictability of these scores beyond 30 days, at six months or one year. He also emphasized that the presence of comorbidities and age remain two strong independent risk factors for mortality in SARS-CoV-2 infection [38].
With a good prediction of 90-day mortality [9,27] at a cut-off point of 12 [39], among patients with the COVID-19 infection and aged over 70 years old from our study, the MuLBSTA score proved to be a good predictor of mortality with statistical significance and an AUC of 0.854 (95%CI: [0.785–0.922], p < 0.001). This score additionally quantifies multilobar involvement and the bacterial co-infections, the elderly patients being more susceptible to severe pulmonary involvement. Also, among the cardiac comorbidities, the presence of hypertension is an individually quantified parameter, this condition being the most common in the studied cohort. Cheng et al. reported similar outcomes, concluding that this score is a highly effective tool for assessing mortality risk, providing superior results than CURB-65 and APACHE II score, which is also a reliable tool for assessing disease severity [40]. Furthermore, Preti et al. highlight that the MuLBSTA score preserves its predictive value [41] in a study conducted on a group of 431 patients regarding 28-day mortality prediction using PSI, MuLBSTA, and CURB-65 scores,.
The COVID-GRAM score proved to be a good predictor of mortality among elderly patients, assessing from 0 to 5 comorbidities, including hypertension and diabetes, two important groups of comorbidities in our study, as well as an LDH assessment, which is an important marker for quantifying severity. Thus, in our study, at a cut-off point of 89 corresponding to the high-risk group, the COVID-GRAM score shows 100% sensitivity for mortality (95%CI: [81.47–100.00]). Esteban Ronda et al. also obtained good predictability of this score in a group of 208 patients with a median age of 63 years, reporting high sensitivities for CURB-65, COVID-GRAM and PSI [10]. Moreover, high AUC for the Pneumonia Severity Index score and MuLBSTA score (0.831 and 0.853) was obtained, but a similar sensitivity to COVID-GRAM. The accuracy of the COVID-GRAM score was also highlighted by Martha A. Mendoza-Hernandez et al., in a study of 514 patients, who analyzed seven severity scores in a center with high mortality due to COVID-19 infection, applied at baseline and at two, four, six, and eight days of hospitalization. It was also pointed out that the COVID-GRAM and MuLBSTA scores maintained their predictive capacity regardless of when they were applied, which gives these scores predictive stability. The predictive value of the PSI score increased, which can be explained by the variability of the clinical parameters used, which change depending on the time of hospitalization. Thus, the temporal variability of clinical parameters can significantly influence the predictive effectiveness of each score [42].
Regarding procoagulant status, the PADUA score achieved good results, being a good predictor of mortality due to possible thrombotic events, achieving, in our study a good sensitivity of 94.4% at a cut-off point ≥ 4 and an AUC of 0.914 (95%CI: [0.856–0.971], p < 0.001). The literature reports an increased mortality at this cut-off point at a rate up to 63% and highlights the importance of prophylactic anticoagulation in patients with severe/critical forms of the disease, who are at high risk of developing thrombotic events [43]. Furthermore, using the PADUA score helped to achieve lower risk of venous thromboembolism through effective anticoagulation, which has decreased the number of deaths caused by thrombotic events, especially during the cytokine storm that induces a coagulation cascade, through insufficient control of anti-inflammatory factors over pro-inflammatory cytokines, leading to thrombosis events [44,45,46].
However, our study has several limitations. First, it is a retrospective study conducted in a single center with a relatively small number of patients enrolled. The small number of events (18 deaths) limit the robustness of the conclusions. Although the scores had good discriminative ability (PADUA AUC: 0.914, MuLBSTA AUC: 0.854, PSI AUC: 0.831, CURB-65 AUC: 0.719, COVID-GRAM AUC: 0.703), and the optimism-corrected AUC results of bootstrapping analysis (internal validation with 1000 bootstrap resamples) remained high (corrected AUC for PADUA: 0.915, MuLBSTA: 0.854, PSI: 0.832, CURB-65 AUC: 0.718, COVID-GRAM AUC: 0.703) indicating internal stability, the score’s performance should be confirmed in larger, multicenter cohort with different patient populations and varying mortality risks. Also, due to the small number of events, the identified cut-off may lack stability across different clinical cohorts. The high sensitivity and relatively poor specificity of several models (PSI, COVID-GRAM) introduce a substantial risk of false-positive stratification. While these tools are valuable for identifying patients requiring increased clinical vigilance, their use in the geriatric population should be adjunctive adjuvant. Clinical decision-making should integrate these numerical scores with bedside clinical judgment, individual goals of care, multidisciplinary assessment of the patient’s overall prognosis. Another limitation is that these scores were calculated only at the baseline, which does not provide a perspective on the effectiveness of these scores over time. Last but not least, the lack of comparison with pandemic waves and highlighting the predictability of these scores based on the circulating variant of the virus in order to identify possible differences in the predictive accuracy of these scores represents another limitation.
5. Conclusions
All scores analyzed in this study proved to be effective in the study group. However, the Pneumonia Severity Index, MuLBSTA and PADUA scores revealed acceptable prediction ability for mortality among patients hospitalized with COVID-19 and aged over 70 years old. The complexity of the parameters assessed by the scores analyzed led to greater accuracy in predicting mortality. However, the simplicity and short time required to complete these scores are important factors that influence their use in clinical practice. Future research should focus on the prospective multi-center validation of the scores in larger (geriatric) cohorts to establish more accurate clinical cut-offs. Additionally, incorporating viral sequencing, additional measures, and longitudinal data through machine learning algorithms (to develop dynamic risk models that update based on laboratory trends) may enhance the specificity of these models, and may reduce the risks of complications while improving personalized care for the patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Xie J. Wu W. Li S. Hu Y. Hu M. Li J. Yang Y. Huang T. Zheng K. Wang Y. Clinical characteristics and outcomes of critically ill patients with novel coronavirus infectious disease (COVID-19) in China: A retrospective multicenter study Intensive Care Med.2020461863187210.1007/s 00134-020-06211-232816098 PMC 7439240 · doi ↗ · pubmed ↗
- 2Huang C. Wang Y. Li X. Ren L. Zhao J. Hu Y. Zhang L. Fan G. Xu J. Gu X. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China Lancet 202039549750610.1016/S 0140-6736(20)30183-531986264 PMC 7159299 · doi ↗ · pubmed ↗
- 3WHO WHO Coronavirus Disease (COVID-19) Dashboard Available online: https://covid 19.who.int(accessed on 1 December 2025)
- 4Bradley P. Frost F. Tharmaratnam K. Wootton D.G. NW Collaborative Organization for Respiratory Research Utility of established prognostic scores in COVID-19 hospital admissions: Multicenter prospective evaluation of CURB-65, NEWS 2 and q SOFABMJ Open Respir. Res.20207 e 00072910.1136/bmjresp-2020-00072933293361 PMC 7722817 · doi ↗ · pubmed ↗
- 5Lombardi Y. Azoyan L. Szychowiak P. Bellamine A. Lemaitre G. Bernaux M. Daniel C. Leblanc J. Riller Q. Steichen O. External Validation of Prognostic Scores for COVID-19: A Multicenter Cohort Study of Patients Hospitalized in Greater Paris University Hospitals Intensive Care Med.2021471426143910.1007/s 00134-021-06524-w 34585270 PMC 8478265 · doi ↗ · pubmed ↗
- 6Hokenek H.D. Julide S.K. Comparison of scoring systems’ mortality prediction ability in COVID-19 intensive care patients over 80 years of age Ann. Clin. Anal. Med.20231427628010.4328/ACAM.21611 · doi ↗
- 7Oliva A. Borrazzo C. Mascellino M.T. Curtolo A. Al Ismail D. Cancelli F. Galardo G. Bucci T. Ceccarelli G. d’Ettorre G. CURB-65 plus hypoalbuminemia: A new score system for prediction of the in-hospital mortality risk in patients with SARS-Co V-2 pneumonia Infez. Med.20212940841510.53854/liim-2903-1235146346 PMC 8805501 · doi ↗ · pubmed ↗
- 8Elmoheen A. Abdelhafez I. Salem W. Bahgat M. Elkandow A. Tarig A. Arshad N. Mohamed K. Al-Hitmi M. Saad M. External Validation and Recalibration of the CURB-65 and PSI for Predicting 30-Day Mortality and Critical Care Intervention in Multiethnic Patients with COVID-19Int. J. Infect. Dis.202111110811610.1016/j.ijid.2021.08.02734416403 PMC 8372428 · doi ↗ · pubmed ↗