Investigating Tourists’ Emergency Healthcare Access Barriers: A Systematic Literature Review
Panagiota Peleka, Dimitra-Maria Aggelopoulou, Olga Siskou

TL;DR
This review identifies barriers tourists face when accessing emergency healthcare abroad, such as language issues and insurance problems.
Contribution
The study systematically reviews literature to highlight unaddressed challenges in emergency healthcare access for international tourists.
Findings
Language and cultural barriers were the most common challenges reported by tourists.
Financial and insurance coverage issues significantly hindered access to timely emergency care.
Most studies were conducted in Asian countries, highlighting regional variations in healthcare access for tourists.
Abstract
Background: Tourists often travel within their own country or abroad for business, leisure or to receive planned healthcare. However, they are often not prepared for unexpected medical emergencies that occur far from home. Seeking emergency healthcare during travel may pose various barriers and challenges to tourists. Aims: This systematic review aimed to identify the challenges and barriers tourists face while seeking emergency healthcare during travel. Methods: A comprehensive search was performed in PubMed, Scopus, Web of Science and ScienceDirect from 1st January 1995 to 31 October 2025. The review included studies focusing on tourists who sought emergency healthcare abroad. Due to the methodological heterogeneity of the studies making meta-analysis impossible, a narrative synthesis of the results was conducted. The review protocol was registered with PROSPERO (ID CRD420251156975).…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
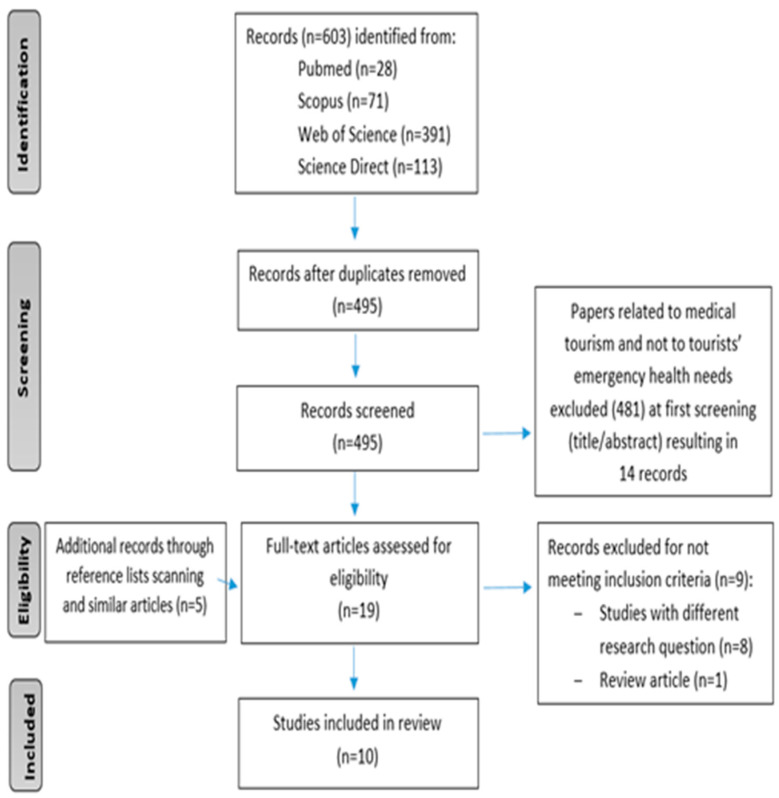 Figure 1
Figure 1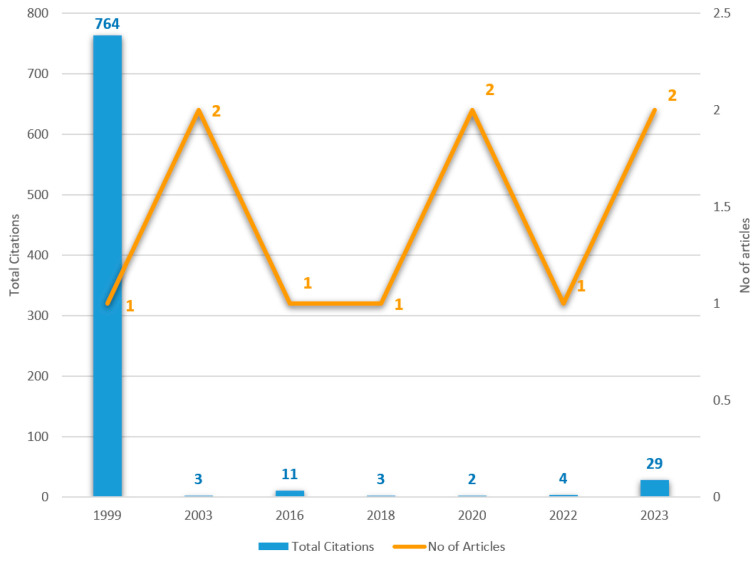 Figure 2
Figure 2 Figure 3
Figure 3- —Center for Health Services Management and Evaluation of the National and kapodistrian University of Athens
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTravel-related health issues · Global Healthcare and Medical Tourism · Trauma and Emergency Care Studies
1. Introduction
Τourists often travel within their own country or abroad for business, leisure or to receive planned healthcare. According to the United Nations World Tourism Organization (UNWTO) [1], approximately 1.4 billion international tourist arrivals were recorded in 2024, indicating an additional rise of between 3% and 5% throughout 2025. The UNWTO attributes this recovery to the “steady” demand from major markets and the rebound of tourism in Asia, which has seen significant growth after the COVID-19 pandemic restrictions.
However, tourists are often unprepared for unexpected medical emergencies encountered far from home. Although some health issues may be mild and resolve spontaneously, medical problems among travelers are not uncommon. Researchers have previously found that between 10,1% and 44,8% of travelers experience illness during international trips [2,3,4,5], but this percentage can rise to nearly 70% when visiting developing countries [6]. According to reports from the Bureau of Epidemiology, Ministry of Public Health of Thailand, the prevalence of the reported health problems was 2.1 per 1000 travelers, which is probably underestimated—including only those who sought medical care from healthcare facilities throughout Thailand [5]. Common health problems among travelers include diarrhea, dermatological conditions, respiratory tract infections, injuries, fever and abdominal pain [3,5,7]. Increased travel to countries with endemic diseases like rabies significantly raised the number of travelers requiring post-exposure prophylaxis at GeoSentinel clinics by fourfold from 2003 to 2012 [8]. Regarding in-flight medical emergencies, which are particularly challenging due to the limited medical resources on board, an incidence of approximately 1 emergency per 604 flights was reported [9].
Cruise tourism also presents several health risks, particularly when medical emergencies exceed onboard handling capacity. Outbreaks such as food poisoning can strain both onboard health services and local medical facilities at ports [10]. Elderly travelers, often managing chronic illnesses or multiple health comorbidities, require special attention due to their increased vulnerability to health complications [11]. Although fatal events during travel are rare, estimated at approximately 1 in 100,000 travelers, they remain a significant concern [12,13].
Findings from previous literature reviews (one systematic and one narrative review) have demonstrated that seeking unplanned healthcare in foreign countries or unfamiliar locations presents several challenges for individuals [14,15]. Language difficulties and limited interpretation services are common barriers for tourists, often preventing them from fully understanding their health condition or financial responsibilities related to treatment. Cultural differences can also add to anxiety and confusion, as visitors unfamiliar with the structure and functioning of local healthcare systems may experience delays in receiving care. Insurance coverage and payments issues can also arise, sometimes leading to significant unpaid medical expenses. Additionally, limited access to patients’ medical histories can result in diagnostic errors, treatment delays and unnecessary repetition of medical procedures. Challenges in continuity of care are also present, as receiving appropriate follow-up care after an emergency abroad can be difficult, potentially affecting the patient’s recovery.
Countries with challenging geography such as Greece [16] often face difficulties in providing emergency healthcare in remote areas. Some key issues are the significant shortage of formally trained emergency medicine professionals and the unequal distribution of healthcare providers, especially on smaller islands and other rural locations. Healthcare services in such areas may only be available from a newly graduated physician or a general practitioner [17]. Consequently, patients with acute conditions often require air transportation to hospitals, significantly increasing costs. Although these flights typically have a short duration, considerable delays can occur due to weather conditions [17]. The situation is further complicated by Greece’s popularity as a tourist destination, contributing to considerable seasonal population fluctuations.
Growth in tourism may negatively impact the provision of local healthcare services, especially during peak seasons, limiting access to care for both tourists and local residents [18,19]. Emergency departments, in particular, face added pressures from handling non-urgent cases among tourists, potentially compromising the efficiency and speed of care delivery [18,19]. Importantly, many travel-related health problems can be mitigated through pre-travel consultations [7]. Furthermore, unexpected health situations can be managed more effectively if travelers are informed in advance about local healthcare resources, emergency procedures and important contacts [20]. However, pre-travel health consultations remain frequently neglected by international travelers. A study conducted by LaRocque et al. at Boston Logan International Airport (2010) [21] reported that nearly half of travelers heading to low- or low–middle-income countries did not seek any pre-travel advice.
Healthcare reimbursement is another critical issue. While European tourists typically utilize the European Health Insurance Card (EHIC) introduced in 2003 to streamline coverage [22], visitors from non-European countries often encounter administrative and insurance-related difficulties when accessing healthcare. Beyond these immediate challenges, socioeconomic factors also matter, as unexpected health problems may extend tourists’ stays abroad [5] and substantially increase their expenses.
This systematic review aims to summarize the current evidence regarding barriers that tourists face when seeking urgent medical care, as well as shedding light on the broader challenges posed by increased tourism on local healthcare systems. The ultimate goal of the current literature review is to contribute to redesigning tourism and health policy so that tourist destinations, in addition to being attractive and interesting, also become safer both for visitors and locals.
2. Materials and Methods
2.1. Design
A systematic review was conducted following the PRISMA guidelines, aiming to synthesize the current literature on barriers faced by tourists when accessing emergency healthcare services. The review protocol was registered with PROSPERO (ID CRD420251156975).
2.2. Search Strategy
In order to formulate a clear research question, the authors used the PICO model: patient or problem, intervention, comparison and outcome. In this study, the research question comprised three elements—PIO. Specifically (P) referred to tourists traveling to other regions; (I) the use of emergency healthcare; and (O) barriers, unmet healthcare needs and accessibility problems.
To address the research question, a literature search was conducted in the PubMed, Scopus, Web of Science and ScienceDirect databases, using the following search string: (tourist* OR traveler* OR visitor* OR tourism OR traveling OR visiting) AND (“healthcare services” OR “healthcare” OR “health care” OR “medical services” OR “seek* healthcare” OR “health services” OR “emergency medical care” OR “urgent health care” OR “emergency department visits” OR “rescue services”) AND (barrier* OR obstacle* OR challenge* OR limitation* OR issue* OR problem* OR delay* OR disparities* OR “unmet healthcare needs” OR inequality* OR “access” OR accessibility OR “healthcare availability” OR experiences OR “clinical outcomes” OR satisfaction).
The literature search was conducted from the end of September 2025 to the end of November 2025 using a title-specific search criterion, ensuring that only studies with a primary focus on the topic were retrieved. This title-based search approach was employed to increase the specificity and relevance of the articles assessed, to reduce false positive selections and finally to ensure a manageable number of articles. An additional filter was applied to include only articles published after the year 1995, aiming to capture literature from the last 30 years. Moreover, backward/forward citation searching was conducted.
Two independent researchers (P.P. and D.A.) screened all identified records for eligibility. The article selection procedure began with title screening, followed by abstract review, and concluded with full-text assessment for eligibility. Inter-rater agreement between the two independent researchers was reported for the majority of articles. However, any uncertainties regarding article inclusion were resolved through discussion with the principal investigator.
2.3. Inclusion/Exclusion Criteria
The inclusion criteria for this review were carefully defined to ensure the relevance of the selected studies. First of all, eligible studies had to focus on tourists (either national/domestic or international), with main purposes of travel, leisure, business, education, adventure and cultural experience. Therefore, studies focusing on travelers such as migrants, expatriates or routine cross-border visitors were excluded.
Secondly, the health services sought by these tourists had to be unplanned or emergency in nature, reflecting acute healthcare needs rather than scheduled medical interventions. Thirdly, only studies published in English or Greek were considered in order to align with the language capabilities of the research team. Finally, only studies published after 1995 were included to ensure that the review captured contemporary challenges in the field of tourist healthcare. However, studies were excluded if they focused primarily on medical tourism, spa or wellness tourism, planned healthcare interventions or traveling communities seeking routine care.
2.4. Study Selection and Outcome
A comprehensive search was performed in PubMed, Scopus, Web of Science and ScienceDirect from 1st January 1995 to 31 October 2025.
A total of 603 articles were identified through database searches, along with 5 additional studies found via reference list screening and supplementary searches of related articles. After removing 108 duplicate records, 500 unique entries remained. Following initial screening of titles and abstracts, 481 records were excluded, resulting in 19 potentially relevant articles; these were then independently assessed (by two researchers) for eligibility, and 9 records were excluded as they did not meet the inclusion criteria.
As a result, 10 studies were included in the final systematic review. The study selection process is illustrated in the PRISMA flowchart shown in Figure 1.
Moreover, Figure 2 presents the citation evolution of the reviewed articles.
2.5. Data Analysis and Synthesis
The following information was extracted from each study: year of publication, study location, study duration, sample size, sample characteristics (mean/median age, gender, and nationality), study type and key findings. Additionally, the methodological quality of each included study was assessed (see the following paragraph). A meta-analysis was not possible due to the methodological heterogeneity of the included studies (cross-sectional studies were analyzed along with retrospective reviews of medical records); therefore, a narrative synthesis of the results was conducted.
The results are organized based on the healthcare access model of Penchansky and Thomas [23]. Based on the National Academies of Sciences, Engineering and Medicine, access to healthcare is defined as “timely use of personal health services to achieve the best possible health outcomes”. However, some patients face barriers that limit access to necessary healthcare, creating inequalities that can potentially adversely affect health outcomes [24]. Therefore, it is necessary to analyze the distinct dimensions that make up the concept of access to healthcare and their connected impact on patients’ and health systems’ outcomes [24,25].
The accessibility dimensions are defined as follows [23]:
- Availability related to sufficiency of health services and professionals.
- Accessibility focused on geographic distance and time to access health services.
- Acceptability referring to match between patients’ and providers’ attitudes (including cultural and social norms).
- Affordability related to patients’ ability to pay for health services.
- Adequacy focused on effective and appropriate response to patients’ needs.
2.6. Quality Assessment
The quality assessment of the included studies was conducted using the Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies, developed by the National Institutes of Health [26]. This tool consists of 14 specific questions and provides a structured and consistent framework for identifying potential biases, evaluating the internal validity of each study and assessing the overall methodological quality of each study. It examines key elements such as the clarity of the research question, selection and definition of the study population, measurement of exposures and outcomes and handling of confounding variables. There are three possible answers: “yes”, “no” and “other” (i.e., cannot determine, not applicable or not reported). Based on the responses, each study is assigned a quality rating of either good, fair or poor, reflecting its overall risk of bias.
In general, five studies were assessed as good or fair, and key conclusions reported in the current literature review are based on these. Three could not be assigned a quality rating (due to limited information) and two were assessed as poor. In all reviewed studies, both the research question or objective and the population were clearly specified and defined. Moreover, in seven out of ten studies the outcome measures (dependent variables) were clearly defined, valid, reliable and implemented consistently across all study participants (while in the other three studies, this was not applicable). Finally, the exposure measures (independent variables) were clearly defined and implemented consistently across all study participants in six out of ten studies.
3. Results
Characteristics of the Studies
This review included 10 quantitative studies, of which 5 used a cross-sectional design and 5 a retrospective design. All studies were published between 1999 and 2023. Most (7/10) were conducted in Asian countries (Japan, Turkey, Saudi Arabia and Thailand), while the remaining three were conducted in Europe [27], the U.S.A. [28] and multiple countries [7]. The number of participants ranged from 37 to 2333. All studies included both genders, except for one that focused exclusively on obstetrical emergencies in pregnant women [29] (Table 1). Common health issues included gastrointestinal problems (diarrhea and abdominal pain), injuries, infectious diseases (dengue, malaria and rabies exposure) and pregnancy-related emergencies.
Figure 3 summarizes the most frequently reported barriers faced by tourists seeking emergency care.
Moreover, in Table 2, the results are classified based on the Penchansky and Thomas [23] framework.
Acceptability issues related to language, cultural and religious differences, as well as issues related to communication with the healthcare providers (e.g., unanswered questions), proved to be the most frequently reported difficulties on behalf of tourists [28,29,31,32,33]. Tourists often reported difficulties in understanding healthcare staff and insufficient explanations regarding their condition or treatment [3]. A large proportion of them also reported that they needed professional interpretation services (up to 54%) [31,33], but in some cases there was a complete lack of access [28]. Even when interpretation was provided, interpreters usually lacked formal training [28] or they had limited specialization in different languages [33]. In addition, based on the results of Taguchi et al.’s study [32] conducted in Japan, some issues arose due to the lack of consideration for religious customs and the location where the tourist wished to receive treatment. Consistent with previous results, Nakazawa et al. [29] found that two of the main challenges tourists faced were language and cultural barriers.
In addition, financial consequences and insurance coverage issues (related to affordability) were investigated in three out of ten articles. A study conducted in two German travel clinics by Saffar et al. [27] identified that one in three participants (32%) had to spend more than €100 after potential rabies exposure. Interestingly, almost half of the participating travelers (48%) were unaware at the time of the study whether their costs could be reimbursed by their health insurance. Nakazawa et al. [29] similarly reported that differences in health insurance systems were among the main challenges faced by tourists. In another study by Mansanguan et al. [5] on adult backpackers who visited Thailand, one in five participants with health problems (20%) reported that they had to buy over-the-counter medication.
Moreover, availability and accessibility barriers were also identified. A study conducted in Saudi Arabia by Alsharif A.I. and Al-Khaldi Y.M [30] suggested that participants without Saudi nationality, compared to Saudis, indicated that the primary healthcare centers’ working hours were inappropriate. Approximately one in four tourists (22.4%) in the same study suggested establishing a 24-h duty service. The accessibility of emergency healthcare services was also problematic for tourists after a possible rabies exposure [27]. In this study, approximately half of the participants (52%) reported being able to reach a healthcare facility within one hour, while almost all (92%) could do so within 24 h, highlighting possible geographical constraints and reduced availability of healthcare facilities.
Finally, adequacy problems were also identified. Saffar et al. [27] found that one in five individuals who sought medical care abroad (20%) did not receive any vaccination, despite its necessity, highlighting that tourists did not receive the appropriate care abroad. Among those who were vaccinated and provided detailed information, about one in four (26%) received the vaccine only after visiting at least a second healthcare facility. Furthermore, Piyaphanee et al. [7] conducted a study using data from travelers evaluated at GeoSentinel network sites, which are specialized travel and tropical medicine clinics in 28 countries. The investigators suggested that travelers were more likely to receive complete reports on their trip-related healthcare exposure when evaluated at GeoSentinel clinics after returning home (92%), rather than during travel, emphasizing gaps in the continuity of care and quality of medical documentation during travel.
4. Discussion
This systematic review highlights that tourists seeking emergency healthcare abroad may face significant challenges impacting both the quality of care received and their overall travel, as well as the health system.
4.1. Impact on Patient
Language barriers proved to be the biggest obstacle in patient–provider communication [28,29,31,32,33]. As a result, some patients were unable to communicate with medical staff. Carrasquillo et al. [28] investigated the impact of language differences on patients’ experience in the emergency department and found that only half of non-English-speaking patients (52%) experienced satisfaction with the care provided, compared with 71% of English-speaking patients. Specifically, non-English-speaking patients were more likely to experience difficulties with communication, diagnostic testing, the use of medication and follow-up care, ultimately reducing the overall quality of healthcare.
Insurance and payment-related issues are also substantial challenges, especially for uninsured patients [10,15]. Limited or absent coverage and generally complex reimbursement procedures can delay access to necessary treatment. In emergency settings, where prompt intervention is critical, any delays caused by insurance verification may compromise patient outcomes. These challenges can be particularly important for tourists requiring extended hospitalization, as prolonged stays significantly increase total travel costs [10,15], e.g., due to the cancelation of return tickets and purchase of new ones.
Cooperation with external organizations such as embassies or transportation services was also reported as challenging, further complicating the patient journey [33]. Τhese barriers may also have indirect consequences on overall tourists’ travel experience, as health problems frequently prolonged the duration of stay abroad and led to postponements of planned activities or, in some cases, cancelations [5,27]. Such outcomes not only reflect the medical burden, but also highlight the social and economic implications of seeking emergency care while traveling.
4.2. Impact on Health System
Language and cultural differences can also be critical barriers to the delivery of efficient emergency care. Communication difficulties and cultural differences can also lead to delays in decision-making, reduced adherence to care plans and additional strain on already limited ED resources [15]. Moreover, language barriers were linked to longer emergency department stays (up to approximately 50 min) [31] and in some cases to unpaid medical bills due to tourists misunderstanding [32].
Limited access to a patient’s medical history is also a significant challenge during emergency visits, hindering both diagnostic accuracy and treatment efficiency. When healthcare providers are unable to receive essential clinical information, informed decision-making is difficult and the provision of care may be delayed. The absence of medical records may also lead to repetition of diagnostic tests, driving up healthcare costs and extending ED length of stay [10,15].
Emergency departments (EDs) face significant challenges during peak vacation periods [18,19,34,35]. EDs in tourist areas often lack the resources to handle the high number of admissions, a portion of which are non-urgent [19,36]. Especially during the summer, when staff availability may be reduced due to their scheduled vacations, increased tourism can overwhelm existing resources and influence treatment speed, leading to prolonged wait times, delays in diagnosis and an overall decline in the quality of care [10,15,18,19,36]. This can be particularly important in geographically isolated or resource-limited settings, such as islands. A study conducted in Corfu (Greece, 2022) indicated that injury admissions during peak tourist season (summer months) have led to more frequent patient transfers to other healthcare facilities, particularly when injuries occur outside the hospital’s full working schedule [34]. Similar patterns have been observed in winter sports destinations like Switzerland, where hospital admission rates with orthopedic patients can be up to four times higher in winter compared to other seasons, largely due to non-local residents [35]. Another study conducted in Sorrento (Italy, 2021) indicated that tourists may receive faster ED treatment than local residents, potentially limiting their timely access to emergency care [18]. Additionally, unpredicted events such as mass food poisoning on cruise ships can sharply increase demand on the nearest healthcare facilities, placing additional stress on local health systems [10].
4.3. Limitations
One of the primary limitations of this study is the inclusion of literature published exclusively in English and Greek, which may have resulted in the exclusion of relevant studies available in other languages. Moreover, this language restriction may raise bias issues toward destinations and health systems more represented in English language publishing. Furthermore, by limiting the search to publications after 1995, earlier and potentially significant literature might have been overlooked. On the other hand, searching for papers published in previous decades led to the inclusion (in the current literature) of a few articles considered as old. Therefore, some of the barriers mentioned in these articles may have been mitigated, for example, through the use of telemedicine and translation applications. Although efforts were made to identify comprehensive and relevant sources, gray literature was not systematically explored; this raises the possibility that important data may have been missed. In addition, the initial search was conducted based on titles, resulting in a manageable number of 608 articles. However, it is recognized that a title-based search is likely to miss a few relevant studies.
Another notable limitation is the absence of a meta-analysis. This decision was based on the considerable methodological heterogeneity among the included studies, which made quantitative synthesis unfeasible. As a result, the strength and generalizability of the study’s conclusions are limited and there is a greater dependence on qualitative interpretation, which carries a degree of subjectivity.
In addition, the findings may be influenced by publication bias, where studies with positive or statistically significant outcomes are more likely to be published, while those with negative results remain unpublished, potentially affecting the representativeness and accuracy of the overall conclusions. Lastly, database selection bias may have played a role, as the search was confined to four major databases, potentially excluding relevant studies published in less prominent or regional repositories.
5. Conclusions and Recommendations
Based on the evidence to date (given that the literature search was completed in November 2025) and taking into consideration the limited number (n = 10) of specialized manuscripts focused on an emerging nature topic, which come mainly from Asia, we can conclude that tourists face multiple barriers when seeking emergency healthcare abroad: linguistic, financial, organizational and cultural. Addressing these issues requires systemic changes, while several targeted strategies can be implemented before, during and after travel to mitigate the aforementioned impacts at both the patient and health system levels.
Pre-Travel Recommendations: Preparation plays a critical role in reducing travel-related health risks. Tourists should have a pre-travel medical consultation, especially those traveling to developing countries or those with chronic illnesses [11,27]. They should be informed according to the destination and the length of their trip about preventive strategies such as necessary vaccinations, guidance on managing potential health issues and advice on when and how to seek and access timely medical help in case of emergency [11]. Travelers with known health conditions are recommended to obtain a letter of referral from their personal physician before departure [20]. Moreover, tourists should be encouraged to prepare a comprehensive health record with their updated medical information such as vaccination certifications, potential allergies, blood type, insurance and emergency contact information [11]. They should also conduct appropriate research regarding the available health services and the proximity of medical facilities. For individuals who take regular medication, renewing prescriptions and ensuring an adequate supply is essential [20].
Recommendations During Travel: In case of facing a language barrier, using professional interpretation services or designing an app for interpretation can help to reduce communication difficulties and ensure proper treatment [18,37]. Understanding the local emergency system is also essential. Tourists should learn the emergency telephone number of the host country as soon as they arrive, or ideally before departure [20]. Furthermore, the availability of ambulance services may vary widely between urban and rural areas. Knowing the transportation availability and the distance to the nearest healthcare facility is very important, especially for families traveling with children or those traveling to areas with limited emergency care. In such cases, tourists are also advised to carry a basic first aid kit and essential over-the-counter medications, and even be prepared to apply basic emergency procedures like CPR [20]. In regard to highly visited tourist areas, particularly during peak seasons, increasing healthcare staff availability becomes crucial [3,10].
Moreover, in order to mitigate financial uncertainty and reimbursement confusion, destinations and insurers can co-develop standardized tourist billing explanations and upfront cost disclosure protocols.
Post-Travel Recommendations: Even after returning home, continuity of care remains important. Tourists should be given a detailed summary or referral letter from the foreign healthcare facility they have visited. This document should include the medical interventions performed and provide recommendations for follow-up care [11].
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1United Nations World Tourism Organization (UNWTO) International Tourism Recovers Pre-Pandemic Levels in 2024 Available online: https://www.unwto.org/news/international-tourism-recovers-pre-pandemic-levels-in-2024(accessed on 25 June 2025)
- 2Reed J.M. Mc Intosh I.B. Powers K. Travel illness and the family practitioner: A retrospective assessment of travel-induced illness in general practice and the effect of a travel illness clinic J. Travel Med.1994119219810.1111/j.1708-8305.1994.tb 00594.x 9815338 · doi ↗ · pubmed ↗
- 3Tekin Y. Turistik Bölgelere Gelen Turistlerin Aldıkları Sağlık Hizmetlerinden Memnun Kalma Düzeyleri (The Levels of Satisfaction Which Tourists Gain From Health Services in Tourist Regions)Doctoral Dissertation Marmara University Istanbul, Turkey 2003
- 4Fleck S. Jäger H. Zeeb H. Travel and health status: A survey follow-up study Eur. J. Public Health 2006169610010.1093/eurpub/cki 14416030132 · doi ↗ · pubmed ↗
- 5Mansanguan C. Matsee W. Petchprapakorn P. Kuhakasemsin N. Chinnarat N. Olanwijitwong J. Piyaphanee W. Health problems and health care seeking behavior among adult backpackers while traveling in Thailand Trop. Dis. Travel Med. Vaccines 201621510.1186/s 40794-016-0026-928883953 PMC 5530955 · doi ↗ · pubmed ↗
- 6Winer L. Alkan M. Incidence and precipitating factors of morbidity among Israeli travelers abroad J. Travel Med.2002922723210.2310/7060.2002.2420212962594 · doi ↗ · pubmed ↗
- 7Piyaphanee W. Stoney R.J. Asgeirsson H. Appiah G.D. Díaz-Menéndez M. Barnett E.D. Chen L.H. Healthcare seeking during travel: An analysis by the Geo Sentinel surveillance network of travel medicine providers J. Travel Med.202330 taad 00210.1093/jtm/taad 00236637429 PMC 10979637 · doi ↗ · pubmed ↗
- 8Gautret P. Harvey K. Pandey P. Lim P.L. Leder K. Piyaphanee W. Geo Sentinel Surveillance Network Animal-associated exposure to rabies virus among travelers, 1997–2012 Emerg. Infect. Dis.20152156910.3201/eid 2104.14147925811076 PMC 4378464 · doi ↗ · pubmed ↗