Radiation Exposure in Robotic-Assisted Versus Conventional and Navigation-Assisted Spine Surgery: A Systematic Review, Meta-Analysis, and Meta-Regression of 3205 Patients
Víctor Rodríguez-Domínguez, Catalina Vivancos Sánchez, Mario Taravilla-Loma, María L. Gandía-González, Alberto Isla Guerrero

TL;DR
This study compared radiation exposure in robotic-assisted, conventional, and navigation-assisted spine surgeries, finding no significant overall reduction in radiation dose or fluoroscopy time with robotic techniques.
Contribution
The study provides a comprehensive meta-analysis and meta-regression of radiation exposure outcomes across different spine surgery techniques.
Findings
Robotic assistance did not significantly reduce radiation dose or fluoroscopy time compared to freehand surgery.
Subgroup analyses showed lower exposure with specific robotic systems and for certain surgical indications and levels.
Recent freehand studies showed increased fluoroscopy time and radiation dose, while robotic techniques remained stable.
Abstract
Objectives: This systematic review and meta-analysis compared freehand and navigation-assisted spine surgery with robot-assisted techniques, focusing on radiation dose, fluoroscopy time, and factors influencing these outcomes. Methods: Following the PRISMA and PROSPERO protocols, we searched major databases for comparative studies on radiation exposure or fluoroscopy duration. Non-comparative, cadaveric, and animal studies were excluded. Bias was assessed with RoB 2 and MINORS. The data were pooled using random-effects models, with subgroup, meta-regression, sensitivity, and publication-bias analyses. Results: Twenty-eight studies (3205 patients) were included. Compared with freehand surgery, robotic assistance did not significantly reduce radiation dose (SMD −0.81; p = 0.07) or fluoroscopy time (SMD −0.56; p = 0.06), with substantial heterogeneity. Subgroup analyses revealed lower…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
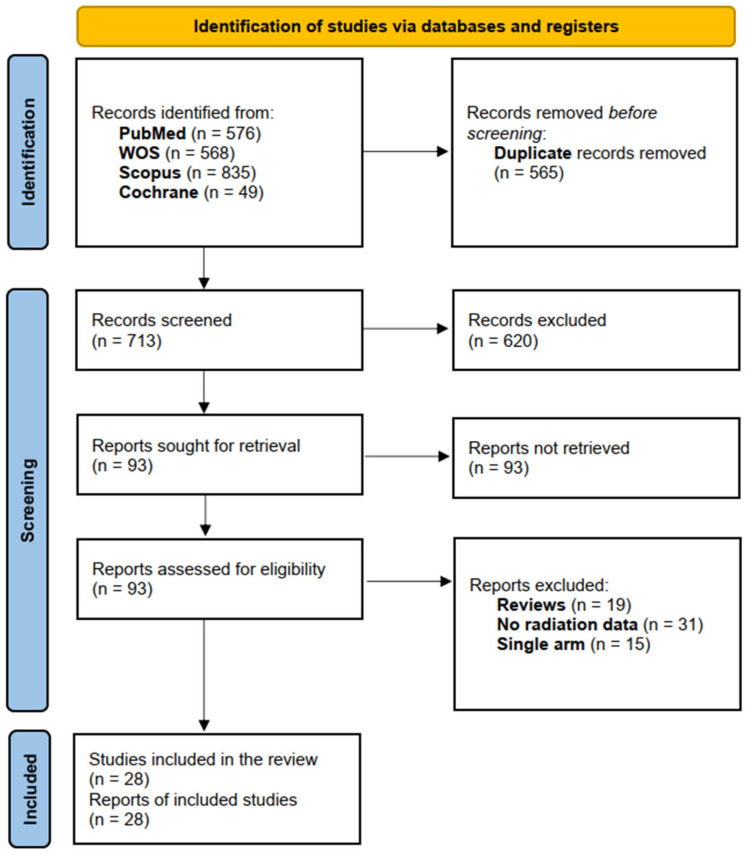 Figure 1
Figure 1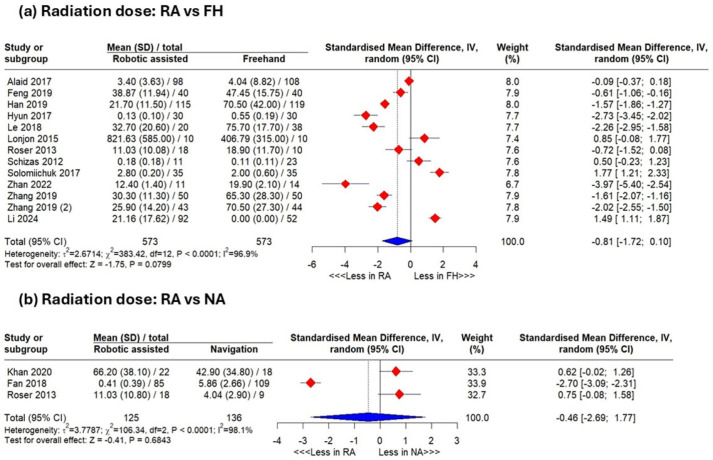 Figure 2
Figure 2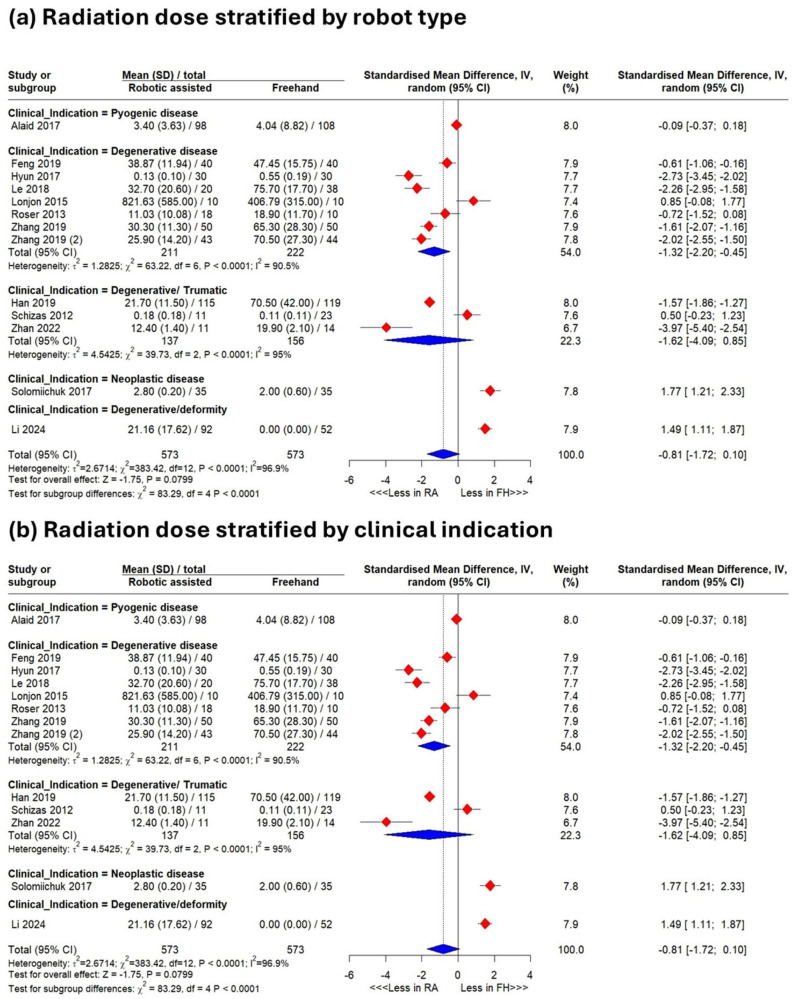 Figure 3
Figure 3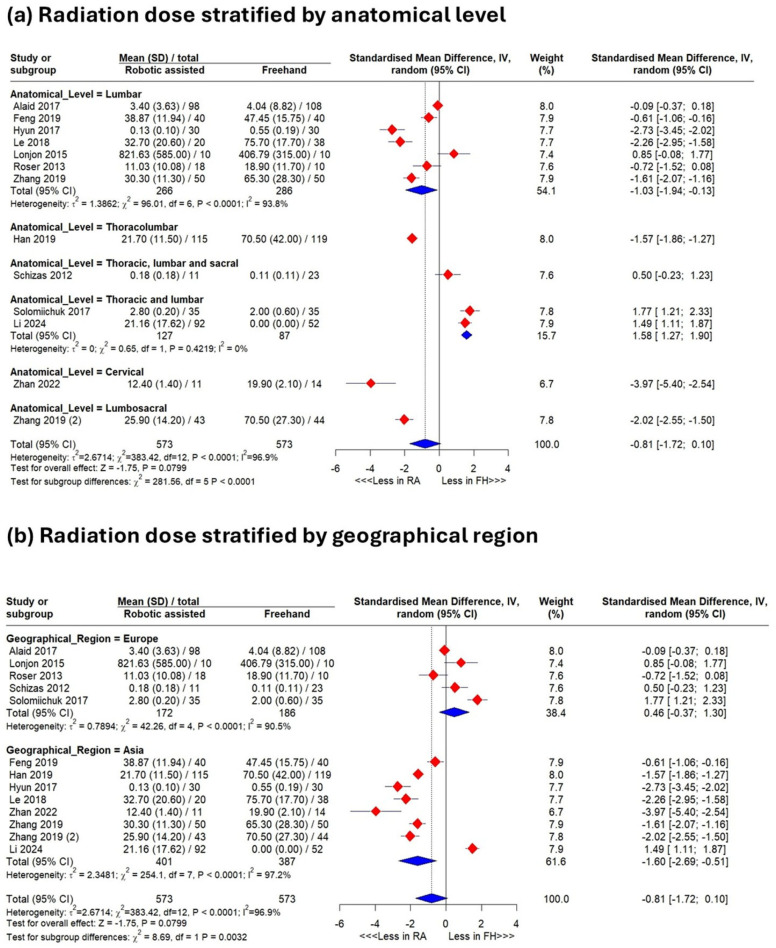 Figure 4
Figure 4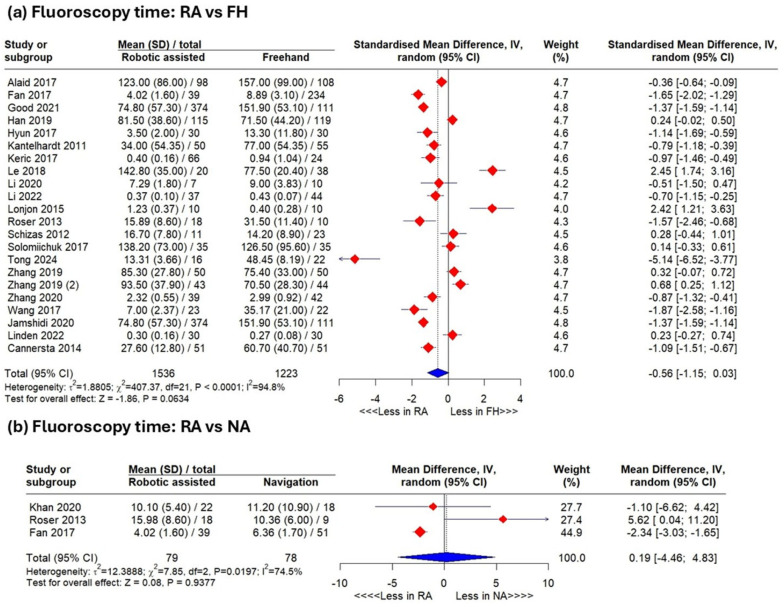 Figure 5
Figure 5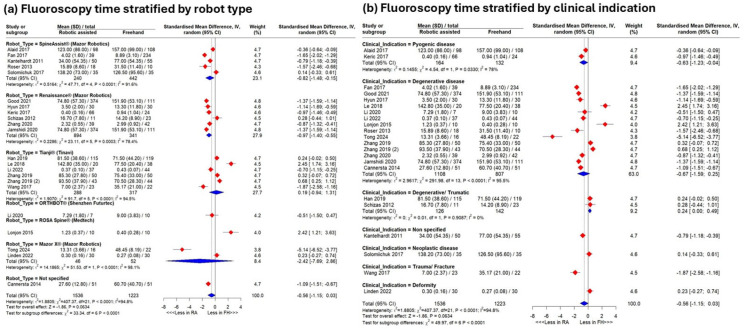 Figure 6
Figure 6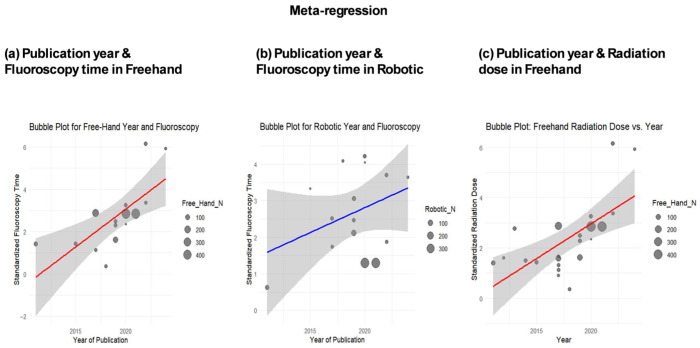 Figure 7
Figure 7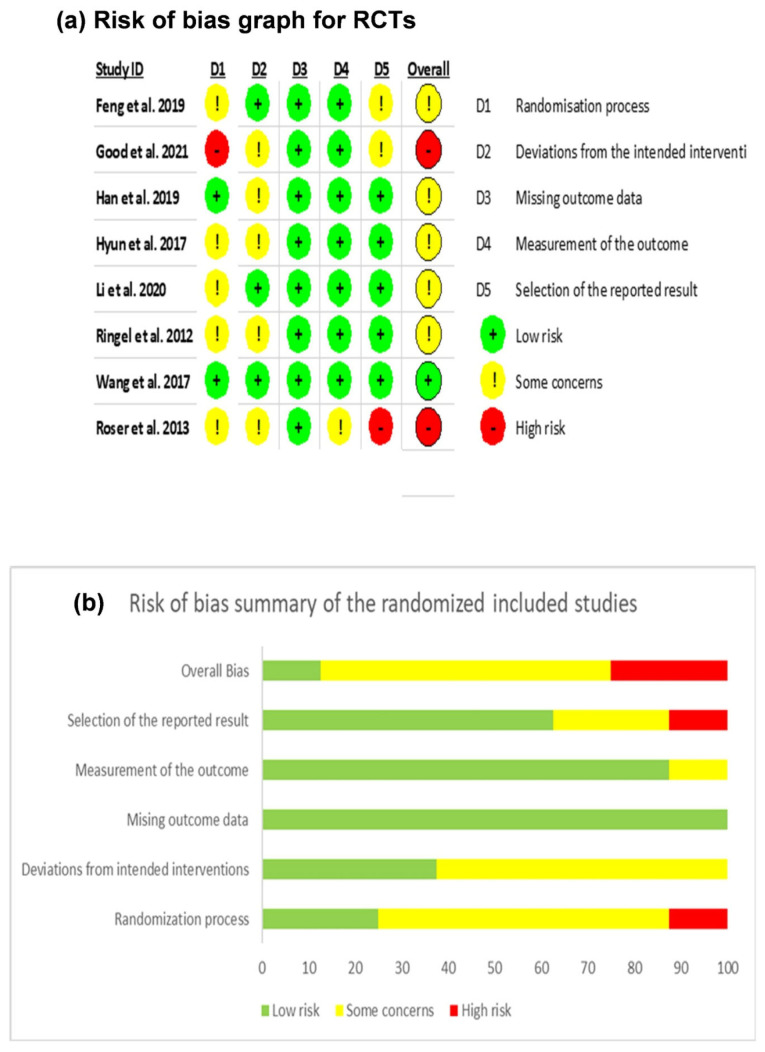 Figure 8
Figure 8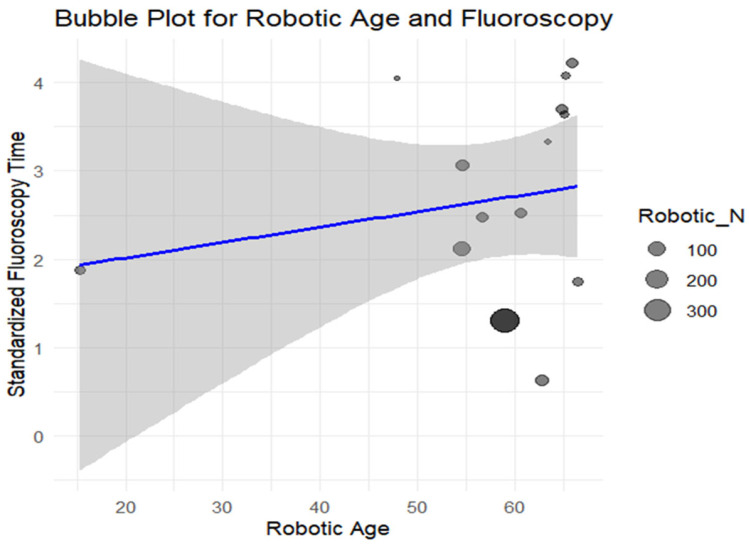 Figure 9
Figure 9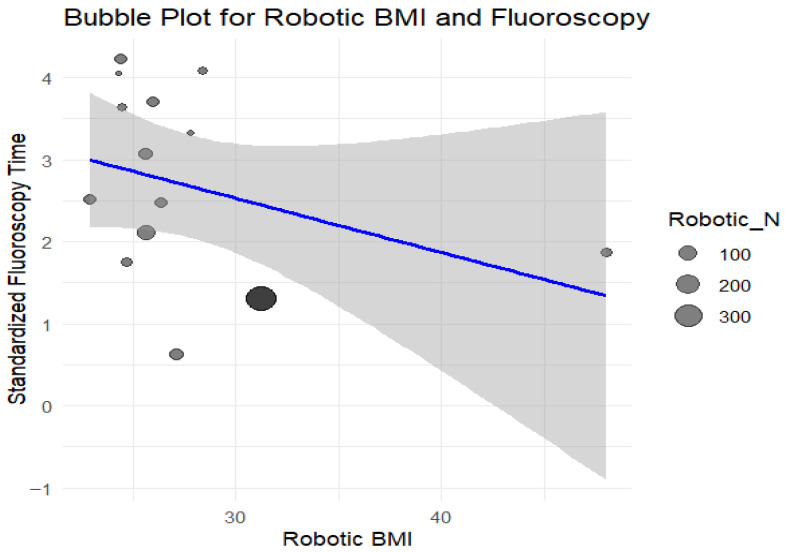 Figure 10
Figure 10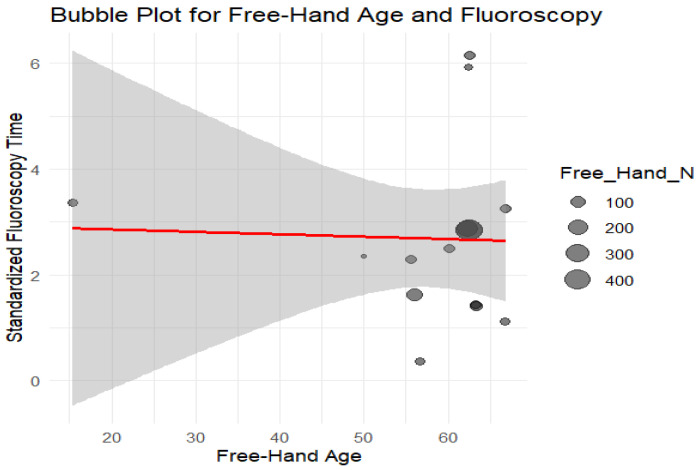 Figure 11
Figure 11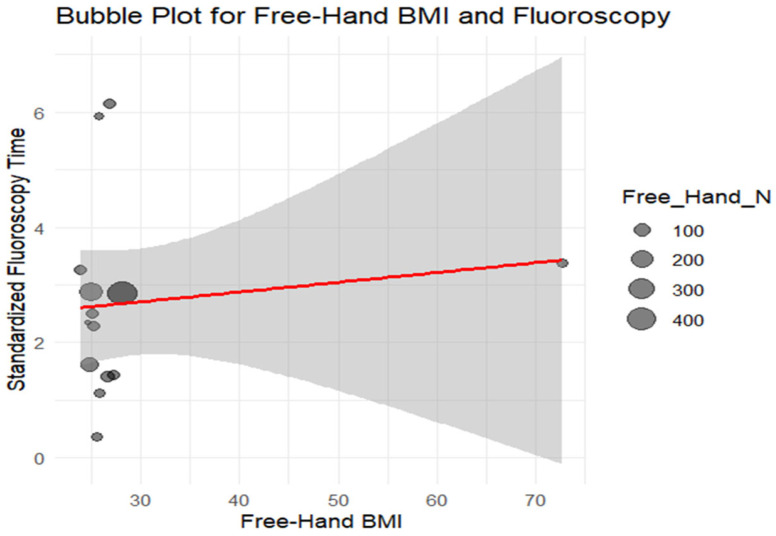 Figure 12
Figure 12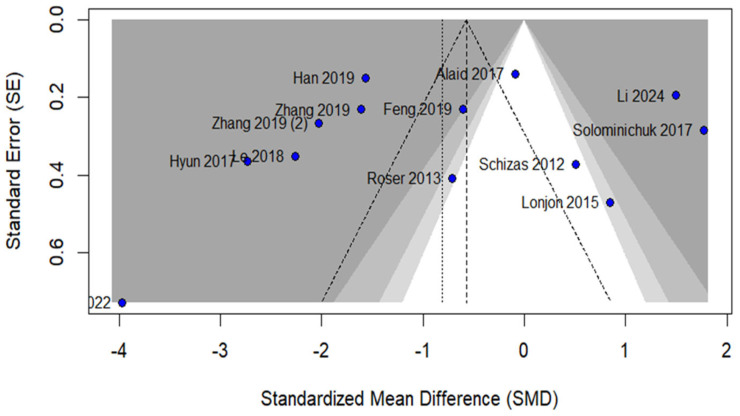 Figure 13
Figure 13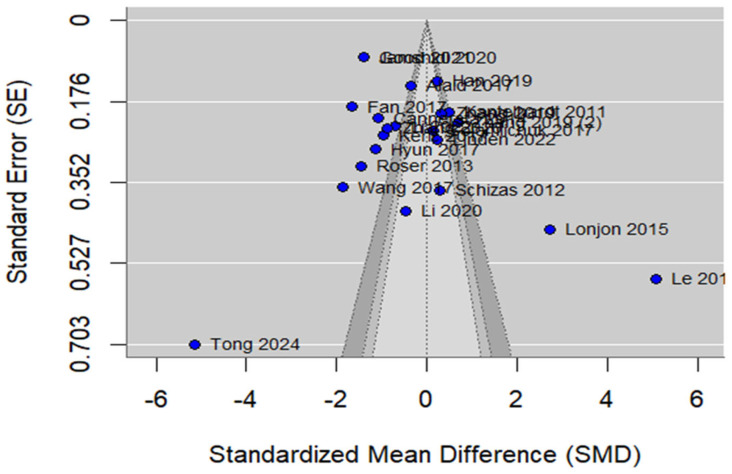 Figure 14
Figure 14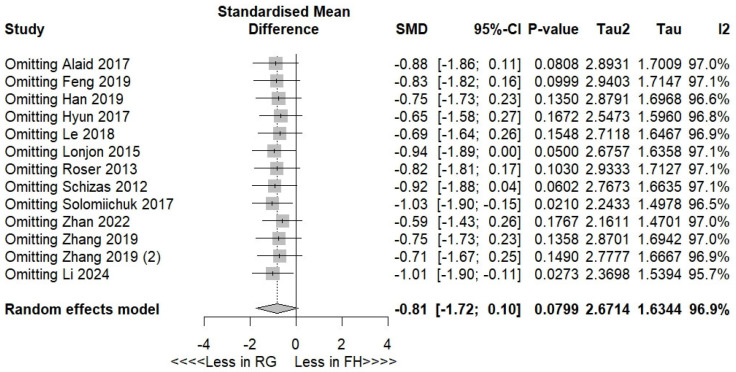 Figure 15
Figure 15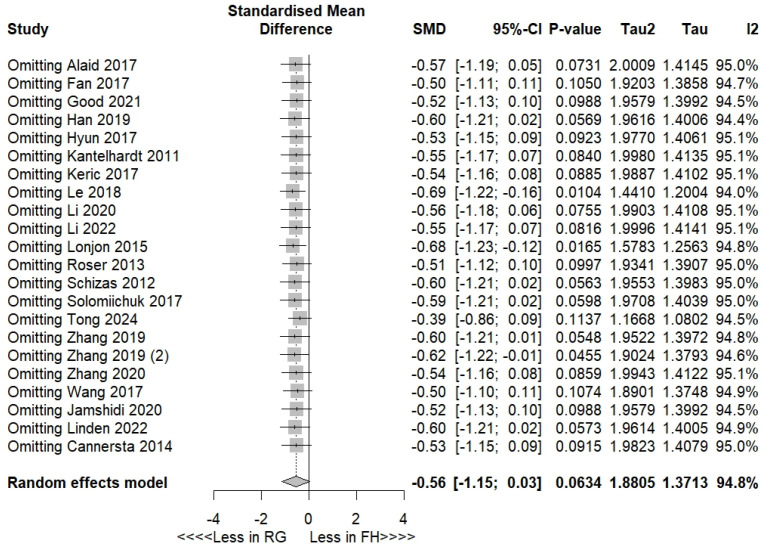 Figure 16
Figure 16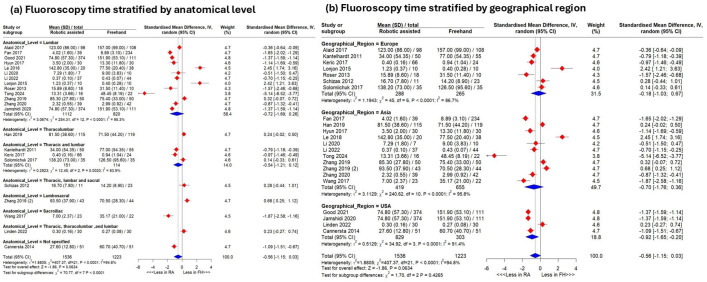 Figure 17
Figure 17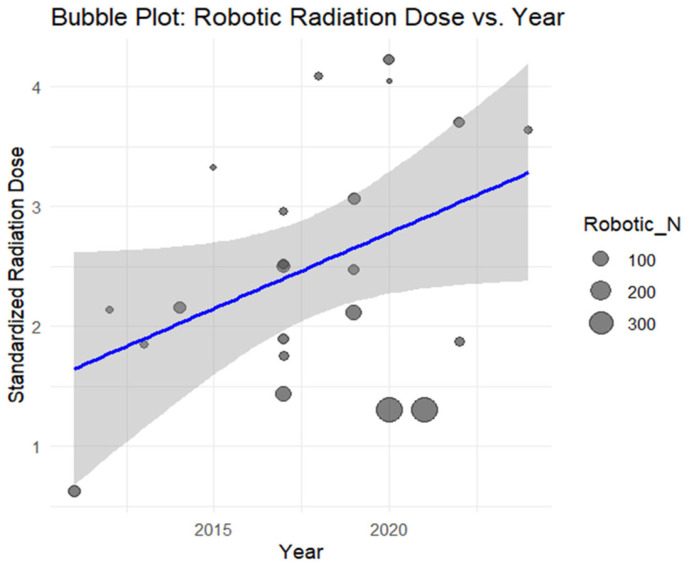 Figure 18
Figure 18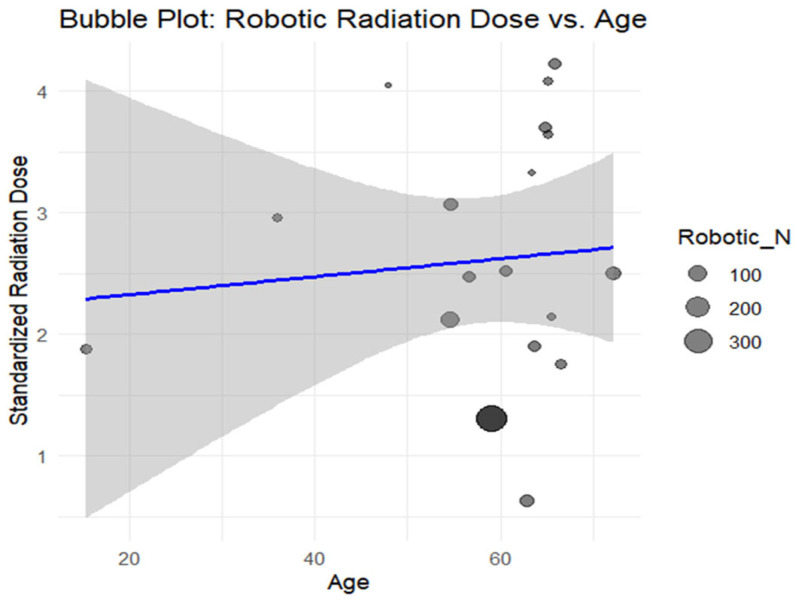 Figure 19
Figure 19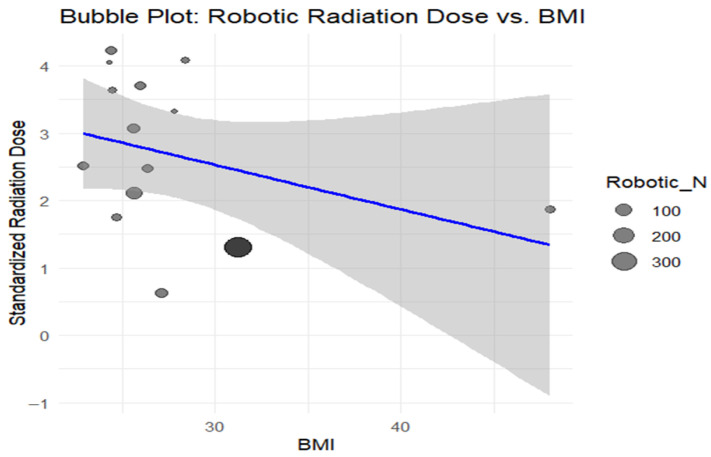 Figure 20
Figure 20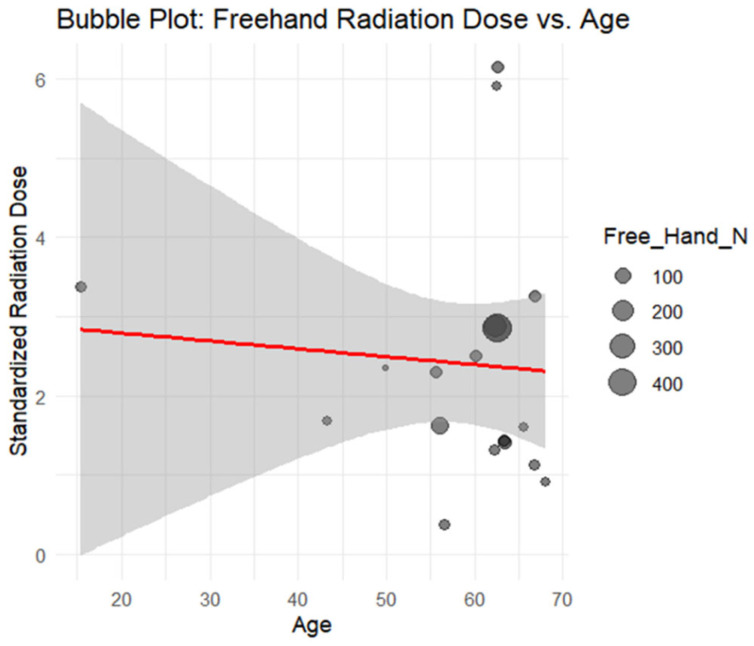 Figure 21
Figure 21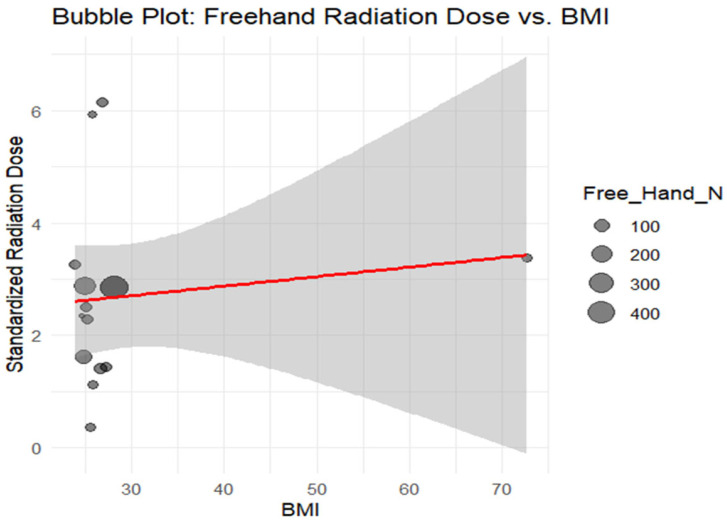 Figure 22
Figure 22Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpinal Fractures and Fixation Techniques · Radiation Dose and Imaging · Management of metastatic bone disease
1. Introduction
Surgical integration, particularly in robotics, is transforming multiple surgical domains and has gained relevance in spinal procedures [1]. Robotic systems offer precise control, minimally invasive approaches, and the potential for improved outcomes [2]. Nevertheless, their use in spine surgery remains debated, especially regarding radiation exposure [3,4]. Evidence suggests that robotic assistance may decrease radiation exposure for patients and operating room staff due to enhanced precision and potentially shorter operative times [5]. However, this assumption is not universally supported [6,7]. Several studies have questioned whether robotics truly reduces radiation, emphasizing the need for more rigorous evaluation [8]. While some publications report meaningful reductions in radiation levels [9], others describe no difference or even increased exposure [10].
Recent systematic reviews and meta-analyses provide inconsistent findings. Luengo-Matos [11] included only four studies addressing radiation reduction, and Li et al. [12] found no significant differences in fluoroscopy time between robotic and freehand techniques, based on merely two studies. Similarly, Guan et al. [13] reported no differences in overall radiation exposure, though subgroup analysis with six studies suggested lower doses in robotic-assisted TLIF compared with MIS-TLIF. Al-Naseem et al. [14] also detected no significant differences, relying on only three studies.
Given these limitations, a more comprehensive systematic review and meta-analysis is required to clarify whether robotic assistance meaningfully affects radiation exposure and how potential confounders influence reported outcomes.
2. Materials and Methods
2.1. Protocol Registration
This systematic review and meta-analysis adhered to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement [15] (Supplementary Table S1) and the recommendations of the Cochrane Handbook for Systematic Reviews and Meta-Analyses [16]. The protocol for this review was published and registered in PROSPERO with ID CRD42024608425.
2.2. Data Sources and Search Strategy
We searched the Cochrane Central Register of Controlled Trials (CENTRAL), PubMed (MEDLINE), Web of Science (WoS), and SCOPUS databases from inception until October 2024, with a reminder in all databases turned on to identify peer-reviewed eligible studies using search terms with Boolean operators. ClinicalTrials.gov was also searched for trial registration (Table A1).
2.3. Eligibility Criteria
The PICO criteria guided study selection: population (patients undergoing spinal surgery, including minimally invasive pedicle screw placement and spinal fusions), intervention (robotic-assisted technique), comparison (freehand or navigation-assisted), and outcomes (radiation dose and fluoroscopy time). We excluded reviews, editorials, book chapters, cadaveric/animal studies, and non-comparative studies without radiation data.
2.4. Study Selection
The Rayyan tool was used for screening. All retrieved records were imported into Rayyan (Version 1.7, [Computer software]. (2026). Rayyan Systems, Inc., Doha, Qatar) for de-duplication and screening. After removing the duplicates, two authors independently assessed all records using the blinding feature and then screened the full texts of potentially relevant studies. Rayyan labels/tags were used to record exclusion reasons and key notes; filters were used to track decisions by stage and reviewer and to export a reproducible decision log. Disagreements were resolved by consensus. Forward and backward citation tracking was also performed for the included studies.
2.5. Data Extraction
The study data were exported to Excel and organized by study characteristics, patient demographics, and outcomes (radiation dose and fluoroscopy time). The variables included the study design, indication, robot type, sample size, screws used, age, sex, and BMI. The radiation dose reflected cumulative ionizing exposure; fluoroscopy time captured X-ray duration. Radiation exposure and fluoroscopy time were extracted exactly as reported in each eligible study. Because radiation exposure was reported using different dosimetry measures and units (e.g., dose–area product, air kerma, effective dose, or occupational dose), and fluoroscopy time was reported with different time bases (e.g., per procedure, per screw, or during instrumentation) and units (seconds/minutes), we synthesized outcomes using standardized mean differences (SMD). To improve transparency and reproducibility, we summarized each study’s radiation dose measure/unit and fluoroscopy time basis in Table A3; when a study did not report a field, it was coded as “NA”.
2.6. Risk of Bias
The RCTs were assessed with the Cochrane RoB 2 tool [17] across six bias domains. Observational studies were evaluated using MINORS (0–24 scale: 0–6 is deficient, 7–10 is low, 11–15 is fair, 16–24 is high-quality) [18]. Two authors independently rated all studies, resolving disagreements through discussion with the senior author.
2.7. Statistical Analysis
All analyses were performed in R 4.3 using “meta,” “metafor,” and “dmetar.” the Standardized mean differences with 95% CIs were pooled using a DerSimonian–Laird random-effects model, with heterogeneity assessed via Chi-square and I^2^ following Cochrane criteria [16]. The comparisons included RA vs. FH and RA vs. NA. The subgroup and random-effects meta-regression analyses evaluated moderators. Meta-regression was conducted to formally explore potential sources of heterogeneity (e.g., publication year and other study-level moderators where available). Given the limited number of studies contributing to some moderators and the presence of residual heterogeneity, these analyses were considered exploratory. The sensitivity (leave-one-out) and Egger’s tests assessed robustness and publication bias [19].
3. Results
3.1. Search Results and Study Selection
By searching databases, 1278 records were retrieved. After duplicate removal, 713 references were left for primary screening by title and abstract. After screening by title and abstract, ninety-four articles were available to be assessed for our eligibility criteria. Finally, we included 28 studies enrolling 3205 patients in this systematic review and meta-analysis. The PRISMA flow chart of the selection process is shown in Figure 1.
3.2. Characteristics of the Included Studies
Most of the included studies were single-center studies, except for three that were multi-center [20,21,22]. Fourteen studies were conducted in China [20,23,24,25,26,27,28,29,30,31,32,33,34,35], five in the USA [21,22,36,37,38], six in Germany [10,39,40,41,42,43], one in Korea [44], one in Switzerland [45], and another in France [46]. Table 1 and Table 2 summarize the included studies and the baseline characteristics, respectively.
3.3. Risk of Bias
Methodological quality was evaluated using RoB 2 for randomized trials (n = 8) and MINORS for non-randomized studies (n = 20). Most RCTs showed some concerns, with one low-risk study (Wang et al., 2017) [26] and two high-risk studies (Roser et al., 2013; Good et al., 2021) [10,22]. The MINORS scores (17–20/24) indicated high quality despite prospective-data limitations (Table A2, Figure A1).
3.4. Outcomes
3.4.1. Radiation Dose
Robotic-assisted versus Freehand
With a high heterogeneity (I^2^ = 96.9%), the pooled results showed no significant radiation-dose difference between the robotic-assisted and freehand groups (SMD −0.81, 95% CI −1.83–0.21, p = 0.07) (Figure 2a). Sensitivity analyses excluding Solomiichuk et al. [43] or Li et al. [25] yielded significant reductions favoring robotics (p = 0.02) (Figure A2).
3.4.2. Subgroup Analyses
Subgroup analyses showed that Tianji^®^ (Tinavi) significantly reduced radiation dose (SMD −1.44, 95% CI −2.64–−0.25; p = 0.023) (Figure 3a). Grouped by indication, robotics reduced the dose in degenerative disease (SMD −1.32, 95% CI −2.20–−0.45), whereas neoplastic and degenerative/deformity clinical indications favored freehand techniques (1.77 [1.21–2.33]; 1.49 [1.11–1.87]; p < 0.0001) (Figure 3b).
Grouped by anatomical level, several regions favored robotics, but lumbar/thoracic-level procedures favored the freehand technique (SMD 1.58 [1.27–1.90]; p < 0.0001) (Figure 4a). Asian studies favored robotics (SMD −1.60 [−2.93–−0.28]; p = 0.003) (Figure 4b).
3.4.3. Robotic-Assisted Versus Navigation-Assisted
Including heterogeneous studies (I^2^ = 98.1), the pooled analysis showed no significant difference between the robotic-assisted and navigation-assisted groups (SMD: −0.46 with 95% CI [−2.96, 1.77], p = 0.72) (Figure 2b).
3.4.4. Fluoroscopy Time
Robotic-assisted versus Freehand
Including heterogeneous studies (I^2^ = 94.9%), the pooled analysis showed a trend toward lower fluoroscopy time in the robotic-assisted group versus freehand group (SMD −0.56, 95% CI −1.15–0.03; p = 0.06) (Figure 5a). Leave-one-out sensitivity analyses excluding Le et al. [29], Lonjon et al. [46], or Zhang et al. [34] demonstrated significantly reduced fluoroscopy time favoring robotics (Figure A3).
3.4.5. Subgroup Analyses
Subgroup analysis by robot type showed significantly lower fluoroscopy time for the Renaissance^®^ (SMD −0.97, 95% CI −1.40–−0.55) and Spine Assist^®^ (SMD −0.82, 95% CI −1.48–−0.15), whereas studies using the ROSA Spine^®^ favored freehand techniques (SMD 2.42, 95% CI 1.21–3.63; p < 0.0001) (Figure 6a). By clinical indication, pyogenic disease and trauma/fracture favored robotics (SMD −0.63 [−1.23–−0.04]; −1.87 [−2.58–−1.16]; p < 0.0001) (Figure 6b). Grouping by anatomical level showed a lower fluoroscopy time for procedures at a sacroiliac level (SMD −1.87 [−2.58–−1.16]), but a greater time for lumbosacral-level procedures (SMD 0.68 [0.25–1.12]; p < 0.0001) (Figure A4a). Regionally, USA studies favored robotics (SMD −0.92 [−1.65–−0.20]; p = 0.4) (Figure A4b).
3.4.6. Robotic-Assisted Versus Navigation-Assisted
Including heterogeneous studies (I^2^ = 74.5%), the pooled analysis revealed no significant difference between the robotic-assisted and navigation-assisted groups (SMD: 0.19 with 95% CI [−4.64, 4.83], p = 0.93) (Figure 5b).
3.4.7. Meta-Regression
Publication year significantly increased fluoroscopy time in the freehand group (β = 0.3897, p = 0.0001) (Figure 7a) and showed a non-significant upward trend in the robotic group (β = 0.1715, p = 0.06) (Figure 7b). Radiation dose increased with freehand (β = 0.3930, p = 0.014) but not robotics techniques. Age and BMI were non-significant (Figure A5, Figure A6, Figure A7, Figure A8, Figure A9, Figure A10, Figure A11, Figure A12 and Figure A13).
3.4.8. Publication Bias
By inspecting the funnel plots and Egger’s test results, there was no significant publication bias regarding the radiation dose (Z = −1.3444, p = 0.1788) (Figure A14) or fluoroscopy time (Z= 0.3019, p = 0.7627) (Figure A15).
4. Discussion
Radiation exposure during spinal surgery poses risks to patients and OR staff, with recommended limits of 5 rem for total-body radiation and 50 rem for extremities per year [47]. Exposure varies with surgeon and technician experience, and safe fluoroscopy practices keep annual doses below recommended limits [48]. Transitioning from freehand to robot-assisted pedicle screw placement enhances precision, reduces complications, and improves outcomes [23,25,26,35,36,37]. Early studies, including that of Kantelhardt and Devito (2011) [40], demonstrated feasibility and accuracy, highlighting robotic surgery’s potential to lower radiation exposure and prevent screw misplacement [49].
4.1. Summary of Results and Justifications
The pooled analysis revealed no significant difference in radiation dose between the robotic-assisted (RA) and freehand (FH) groups (p = 0.07; I^2^ = 96.9%), though the high heterogeneity likely arose from differences in anatomical level, surgical setting, and robot type. The effect direction (SMD −0.81) suggested a potential RA advantage. Leave-one-out sensitivity analyses excluding Solomiichuk et al. [43] or Li et al. [25] demonstrated a significant RA reduction, indicating that specific studies may mask robotic benefits.
Subgroup analyses identified robot type, clinical indication, anatomical level, and region as key determinants. The Tianji^®^ system (Tinavi) showed significantly lower radiation exposure than FH (SMD −1.44; 95% CI −2.64–−0.25), consistent with advanced Chinese robotic systems optimizing workflow and minimizing intraoperative imaging [50]. RA techniques reduced radiation in degenerative disease, while FH was favored in deformity/degenerative and neoplastic cases, likely due to increased fluoroscopic confirmation in complex anatomy. Robotic benefits are greatest in typical degenerative patients with standard anatomy [11]. Zhang et al. (2019) [34] reported FH radiation to be 2.16 times higher than that of RA techniques during lumbar pedicle screw placement (65.3 ± 28.3 vs. 30.3 ± 11.3 μSv).
Anatomical stratification showed robotic assistance significantly reduced radiation exposure in the cervical, lumbar, lumbosacral, and thoracolumbar regions, especially in deeper or junctional zones. Conversely, a FH technique was favored in thoracic regions, possibly due to study limitations grouping the thoracic and lumbar levels, surgical inexperience, or less-frequent procedures in these areas. These findings highlight that RA benefits vary with anatomy, surgeon experience, and case selection. Robotic precision improves outcomes in complex regions, but workflow delays may offset radiation dose advantages [42].
Regional analysis showed lower radiation in Asian studies, particularly China, where high surgical volume and rapid learning curves may reduce exposure [28]. RA and navigation-assisted techniques showed no significant dose difference. Villard et al. (2014) [51] found that surgeon exposure was nearly tenfold higher with 2D fluoroscopy versus navigation. Bratschitsch et al. (2019) [52] demonstrated navigation significantly reduced team radiation exposure (49 ± 19 vs. 566 ± 560 μSv), allowing surgeons to perform up to tenfold more procedures before reaching annual limits.
Overall, RA reduces radiation exposure variably depending on robot type, anatomical complexity, clinical indication, surgeon experience, and regional practice patterns, while navigation also offers substantial protection compared with freehand techniques.
The pooled analysis indicated a marginal trend favoring robotic-assisted (RA) surgery in fluoroscopy time (SMD −0.56; 95% CI −1.15–0.03; p = 0.06), which became significant after excluding Le et al., Lonjon et al., or Zhang et al., suggesting RA may improve intraoperative efficiency despite high heterogeneity [21]. Jamshidi et al. (2021) [21] reported a 78.3% reduction in total fluoroscopy time and a 79.8% reduction per screw with RA, corresponding to a 50.8% reduction in overall operative fluoroscopy.
The subgroup analyses highlighted differences by robot type. Renaissance^®^ and SpineAssist^®^ significantly reduced fluoroscopy time due to advanced preoperative planning and percutaneous workflows [53,54], likely reflecting their longer market presence and accumulated surgical experience. Conversely, ROSA^®^ favored freehand techniques, potentially due to workflow complexity or operator learning curves. Clinical indications such as trauma and pyogenic disease showed substantial RA benefits, as robotic precision expedites urgent fixation and reduces repositioning errors. Anatomically, RA techniques decreased fluoroscopy in sacroiliac regions but increased it at the lumbosacral junction, likely reflecting registration challenges in transitional zones. Despite more extensive instrumentation, RA techniques required fewer fluoroscopic spot checks than freehand procedures.
Good et al. (2021) [22] reported per-screw fluoroscopy times of 3.6 ± 3.9 s with Mazor versus 17.8 ± 9.0 s in freehand procedures, an 80% reduction (p < 0.001), and the total intraoperative exposure was less than half that of the freehand group (74.8 ± 57.3 vs. 151.9 ± 53.1 s, p < 0.001). Wang et al. (2017) [26] similarly reported reduced radiation with RA sacroiliac screw fixation. Regionally, USA studies showed significant RA reductions, likely due to advanced systems and institutional experience, though subgroup differences were not significant (p = 0.4).
Meta-regression indicated increasing fluoroscopy time and radiation exposure over time for freehand procedures, reflecting more complex cases, increased 3D imaging use, or higher accuracy demands. RA techniques showed a non-significant rising trend, suggesting workflow improvements mitigate exposure increases. Comparisons between RA and navigation-assisted groups showed no significant differences, consistent with Roser et al. (2013) [10] and Fan et al. (2018) [27].
Overall, robotic assistance provides significant benefits in degenerative cases and specific anatomical regions, such as the cervical and lumbosacral levels. Renaissance^®^ demonstrates the greatest reduction in fluoroscopy time, corroborating Kantelhardt et al. [10,40] and Roser et al. [10]. Meta-regression revealed radiation exposure has increased over time in freehand procedures but remained more consistent with RA procedures, highlighting the impact of robotic precision, technical maturation, and experience [11,50,51]. Across most subgroup strata, the heterogeneity remained substantial, indicating that subgrouping did not fully explain between-study variability; therefore, these subgroup findings should be interpreted as exploratory and hypothesis-generating rather than definitive.
4.2. Limitations
Despite its rigorous methodology, this study has notable limitations. First, outcome measurement was not uniform across studies: radiation was reported using different dose metrics/units, and fluoroscopy time was reported using different bases (e.g., per screw vs. per procedure), which likely contributed to substantial heterogeneity and may introduce detection bias. Second, imaging workflows and operative protocols (e.g., use of 2D fluoroscopy vs. 3D imaging, institutional radiation practices) varied across settings and were not consistently reported. Third, many of the included studies were retrospective, increasing susceptibility to selection bias and residual confounding (e.g., surgeon experience and learning-curve effects, case complexity, and center-specific protocols). Finally, the persistence of heterogeneity reduces certainty and limits generalizability, supporting the need for prospective studies with standardized radiation and fluoroscopy reporting.
5. Conclusions
In pooled analyses, robotic-assisted surgery was not associated with a statistically significant reduction in overall radiation dose or fluoroscopy time compared with freehand techniques. Exploratory subgroup and sensitivity analyses suggested possible differences across robotic platforms and clinical contexts; however, substantial heterogeneity and variable outcome reporting limit generalizability. Standardized prospective comparative studies are needed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1De Jesus Encarnacion Ramirez M. Chmutin G. Nurmukhametov R. Soto G.R. Kannan S. Piavchenko G. Nikolenko V. Efe I.E. Ramirez Romero A. Mukengeshay J.N. Integrating Augmented Reality in Spine Surgery: Redefining Precision with New Technologies Brain Sci.20241464510.3390/brainsci 1407064539061386 PMC 11274952 · doi ↗ · pubmed ↗
- 2Regmi M. Liu W. Liu S. Dai Y. Xiong Y. Yang J. Yang C. The evolution and integration of technology in spinal neurosurgery: A scoping review J. Clin. Neurosci.202412911085310.1016/j.jocn.2024.11085339348790 · doi ↗ · pubmed ↗
- 3Shahi P. Vaishnav A. Araghi K. Shinn D. Song J. Dalal S. Melissaridou D. Mai E. Dupont M. Sheha E. Robotics Reduces Radiation Exposure in Minimally Invasive Lumbar Fusion Compared With Navigation Spine 2022471279128610.1097/BRS.000000000000438135791068 · doi ↗ · pubmed ↗
- 4Buchan G. Ong C. Hecht C. Tanous T.J. Peterson B. Hasegawa A. Kamath A.F. Equivalent radiation exposure with robotic total hip replacement using a novel, fluoroscopic-guided (CT-free) system: Case–control study versus manual technique J. Robot. Surg.2023171561156710.1007/s 11701-023-01554-636913058 · doi ↗ · pubmed ↗
- 5Xu D. Lou W. Li M. Xiao J. Wu H. Chen J. Current status of robot-assisted surgery in the clinical application of trauma orthopedics in China: A systematic review Health Sci. Rep.20225 e 93010.1002/hsr 2.93036381405 PMC 9642816 · doi ↗ · pubmed ↗
- 6Mc Kenzie D.M. Westrup A.M. O’Neal C.M. Lee B.J. Shi H.H. Dunn I.F. Snyder L.A. Smith Z.A. Robotics in spine surgery: A systematic review J. Clin. Neurosci.2021891710.1016/j.jocn.2021.04.00534119250 · doi ↗ · pubmed ↗
- 7Lopez I.B. Benzakour A. Mavrogenis A. Benzakour T. Ahmad A. Lemée J.M. Robotics in spine surgery: Systematic review of literature Int. Orthop.20234744745610.1007/s 00264-022-05508-935849162 · doi ↗ · pubmed ↗
- 8Zawar A. Chhabra H.S. Mundra A. Sharma S. Kalidindi K.K.V. Robotics and navigation in spine surgery: A narrative review J. Orthop.202344364610.1016/j.jor.2023.08.00737664556 PMC 10470401 · doi ↗ · pubmed ↗