Hypothermic Machine Perfusion Allows Safe Delay in Kidney Transplantation After Cold Storage
Michal Macech, Tadeusz R. Grochowiecki, Ewa Wojtaszek, Slawomir Nazarewski, Tomasz Glogowski, Andrii Mondryk, Michal S. Proczka, Milena N. Michalska, Jolanta Malyszko, Zbigniew Galazka

TL;DR
Using hypothermic machine perfusion after cold storage for kidney transplants reduces delayed graft function without harming long-term outcomes.
Contribution
Demonstrates that sequential hypothermic machine perfusion after cold storage is safe and reduces delayed graft function in kidney transplants.
Findings
Delayed graft function occurred less frequently in the SCS+HMP group (17.6%) compared to the SCS group (39.2%).
HMP was independently associated with lower odds of delayed graft function (OR 0.34; 95% CI 0.13–0.82).
Patient and death-censored graft survival and renal function were comparable between the two groups over 24 months.
Abstract
Background/Objectives: Static cold storage (SCS) remains the standard method of kidney preservation. As a referral transplant center, we frequently receive kidneys initially preserved with SCS and subsequently initiate prolonged hypothermic machine perfusion (HMP) to extend allocation time and optimize recipient matching. The clinical impact of this sequential preservation strategy remains incompletely defined. To compare outcomes between kidneys preserved with SCS followed by prolonged HMP (SCS+HMP) and SCS alone. Methods: This single-center retrospective study included 200 adult recipients of kidney transplants from brain-dead donors (67 SCS+HMP; 133 SCS). Outcomes were primary graft non-function (PNF), delayed graft function (DGF), patient and death-censored graft survival, and renal function over 24 months. Univariable and multivariable analyses identified predictors of DGF.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
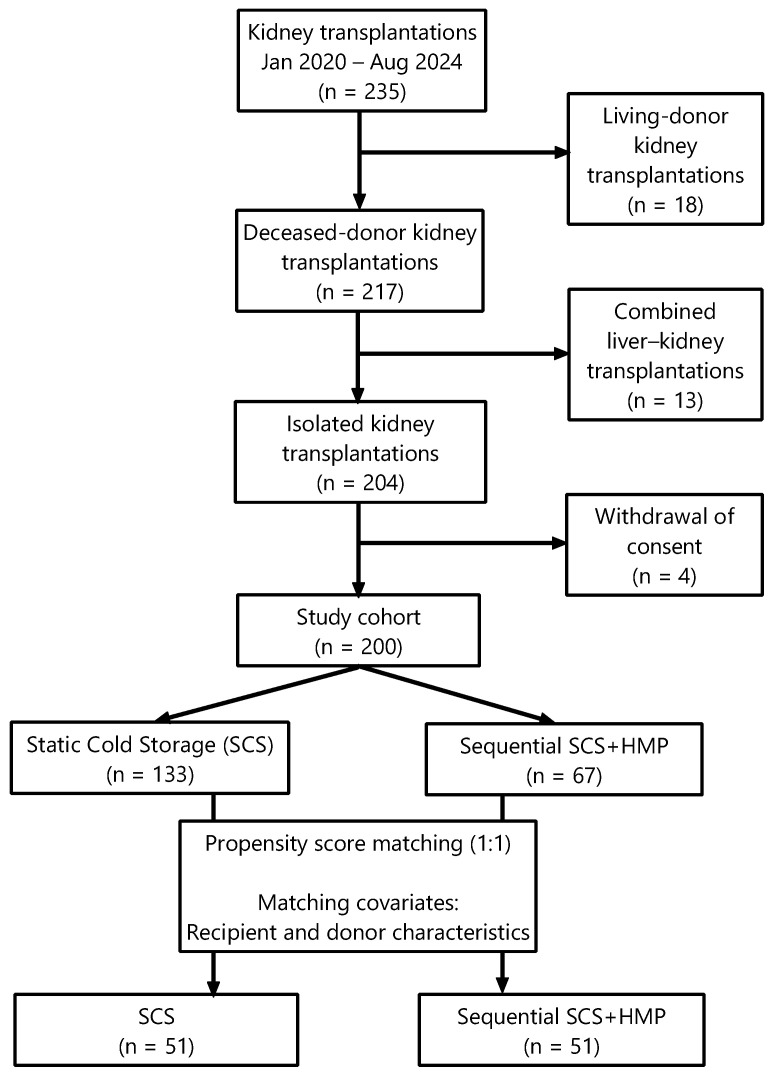 Figure 1
Figure 1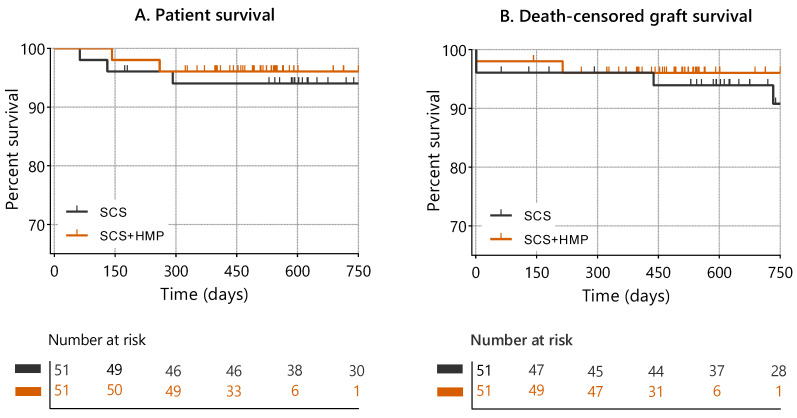 Figure 2
Figure 2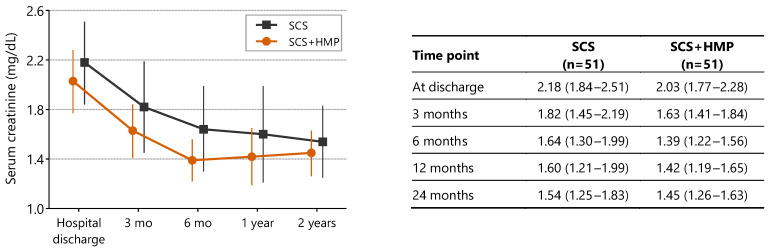 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrgan Transplantation Techniques and Outcomes · Renal Transplantation Outcomes and Treatments · Transplantation: Methods and Outcomes
1. Introduction
Although static cold storage (SCS) at approximately 4 °C remains the standard method of organ preservation, the past three decades have seen substantial technological advances in machine perfusion [1,2]. Numerous improvements in kidney preservation prior to transplantation have been reported. Studies have demonstrated that hypothermic machine perfusion (HMP) reduces the incidence of delayed graft function [3,4] and improves graft survival as well as creatinine clearance [5].
Furthermore, both continuous and pulsatile perfusion have been shown to protect graft cells from apoptosis [6], attenuate ischemia–reperfusion injury [7,8], and decrease the expression of inflammatory cytokines [9]. Several studies suggest that HMP may safely prolong cold ischemia time (CIT) without adversely affecting graft function [10]. However, most of these investigations were conducted in settings where HMP was initiated at the donor center or applied as end-ischemic machine perfusion [11].
As a referral center, we frequently receive kidneys that have initially been preserved using SCS. To allow time for completion of crossmatch testing, recipient optimization, and logistical coordination prior to transplantation, we routinely place the graft on HMP and typically perform transplantation the following morning.
The aim of this study was to evaluate the impact of short-term SCS followed by prolonged HMP on early and medium-term transplant outcomes.
2. Materials and Methods
2.1. Study Design and Population
This single-center retrospective cohort study reflects real-world kidney allocation practices in Poland and was conducted at a high-volume referral transplant center. The study included 200 consecutive adult patients who underwent kidney transplantation at the Department of General, Vascular, Endocrine and Transplant Surgery, Medical University of Warsaw, between January 2020 and December 2024.
The study protocol was approved by the Local Ethics Committee (AKBE/267/2025) and conducted in accordance with the Declaration of Helsinki and the Declaration of Istanbul.
All transplanted kidneys were procured from donation after brain death (DBD) donors. Detailed donor characteristics are provided in Table 1.
2.2. Preservation Protocols and Study Groups
Kidneys undergoing HMP were preserved using the LifePort^®^ Kidney Transporter (Organ Recovery Systems, Chicago, IL, USA) with PumpProtect^®^ preservation solution (Carnamedica, Warsaw, Poland). Static cold storage was performed using StoreProtect Plus^®^ preservation solution (Carnamedica, Warsaw, Poland).
Recipients were stratified according to graft preservation strategy. The SCS+HMP group consisted of 67 recipients who received kidneys initially preserved by SCS followed by HMP, whereas the SCS group included 133 recipients transplanted with kidneys preserved by SCS alone.
Recipient demographic and clinical data were retrospectively collected from institutional records. The study design, patient selection process, and propensity score matching are illustrated in Figure 1.
2.3. Immunosuppression
All recipients received a standardized maintenance immunosuppressive regimen consisting of tacrolimus, mycophenolate mofetil, and corticosteroids. Induction therapy with basiliximab or antithymocyte globulin was administered according to individual immunological risk.
2.4. Outcomes and Statistical Analysis
Outcomes of interest included delayed graft function (DGF), primary graft non-function (PNF), patient survival, death-censored graft survival, and renal function assessed by serum creatinine at discharge and at 3, 6, 12, and 24 months after transplantation.
2.4.1. Propensity Score Matching
To reduce selection bias and baseline imbalances between preservation groups, propensity score matching (PSM) was performed. Propensity scores were estimated using logistic regression including baseline donor characteristics (Table 1) and selected clinically relevant recipient variables considered potential confounders. Recipient covariates included recipient age, pretransplant dialysis duration, primary cause of end-stage renal disease, diabetes mellitus, coronary artery disease, heart failure, and recipient body mass index.
Cold ischemia time (CIT) was intentionally excluded from the propensity score model because it was considered a post-exposure variable and a potential mediator of the preservation strategy rather than a baseline confounder. CIT is partly determined by the preservation approach itself, particularly in the SCS+HMP group, where prolonged preservation represents an inherent component of the management pathway. Inclusion of CIT in the propensity score model could therefore result in overadjustment and attenuation of the estimated effect of the preservation strategy.
Recipients in the SCS+HMP group were matched 1:1 to SCS recipients using nearest-neighbor matching without replacement on the logit of the propensity score, with a caliper width of 0.2 times the standard deviation of the logit. Covariate balance was assessed using standardized mean differences (SMDs).
2.4.2. Other Analyses
Univariable and multivariable (Firth penalized) logistic regression analyses were performed to identify factors associated with delayed graft function (DGF). Multivariable models included preservation strategy, donor age, ECD status, and donor terminal serum creatinine. Results are presented as odds ratios (ORs) with 95% confidence intervals (CIs).
Patient survival was estimated using the Kaplan–Meier method and compared between groups using the log-rank test. Graft survival was evaluated using (i) a cause-specific Cox proportional hazards model with death treated as a censoring event and (ii) a competing-risk approach based on the Fine–Gray subdistribution hazards model. Hazard ratios (HRs) with corresponding 95% confidence intervals (CIs) are reported. Additionally, restricted mean survival time (RMST) was calculated over the 24-month follow-up period.
Statistical analyses were performed using Statistica version 13.3 (TIBCO Software Inc., Palo Alto, CA, USA) and R version 4.5.2 (R Foundation for Statistical Computing, Vienna, Austria). A p value < 0.05 was considered statistically significant.
3. Results
A total of 200 kidney transplant recipients were included in the study. Baseline recipient characteristics are presented in Table 2. Details of preservation strategy and ischemia times are summarized in Table 3.
3.1. Risk Factors for Delayed Graft Function
Univariate logistic regression analysis was performed to identify donor- and recipient-related risk factors for delayed graft function (DGF) in the entire study cohort (n = 200). Only variables demonstrating statistically significant associations are presented in Table 4. Recipient dialysis duration, coronary artery disease, and heart failure, as well as donor age, terminal donor serum creatinine, and expanded criteria donor (ECD) status, were significantly associated with an increased risk of DGF.
3.2. Propensity Score-Matched Analysis
Propensity score matching yielded 51 well-balanced pairs (n = 102). Covariate balance after matching was adequate, with all standardized mean differences <0.12 (Supplementary Table S1; Supplementary Figure S1).
In the matched cohort, hypothermic machine perfusion was associated with a lower odds of delayed graft function in multivariable Firth penalized logistic regression analysis (OR 0.34; 95% CI 0.13–0.82).
Delayed graft function occurred in 9 of 51 recipients (17.6%) in the SCS+HMP group and 20 of 51 recipients (39.2%) in the SCS group; p = 0.027 (absolute difference, 21.6 percentage points; 95% CI 4.0–39.1 percentage points). The incidence of primary graft non-function was comparable between groups (SCS+HMP: 2 patients [3.9%] vs. SCS: 3 patients [5.9%]; p = 1.0).
3.3. Survival Outcomes
Cumulative patient survival and death-censored graft survival did not differ significantly between preservation strategies (log-rank p = 0.63 and p = 0.68, respectively) (Figure 2). Survival probabilities at 3, 6, 12, and 24 months are presented in Table 5.
In Cox proportional hazards regression analysis, preservation strategy was not significantly associated with patient survival (HR 0.66; 95% CI 0.19–2.35; p = 0.52).
For death-censored graft survival, cause-specific Cox regression similarly showed no significant association between preservation strategy and graft failure (HR 0.69; 95% CI 0.12–4.08; p = 0.68).
In competing-risk analysis using the Fine–Gray subdistribution hazard model, hypothermic machine perfusion was likewise not significantly associated with graft failure when death was treated as a competing event (sHR 0.65; 95% CI 0.11–3.70 p = 0.62).
Restricted mean survival time (RMST) analysis over 24 months demonstrated no statistically significant differences between groups. The RMST for graft survival was 725 days in the SCS+HMP group versus 713 days in the SCS group (absolute difference, 11.2 days; 95% CI −43.1 to 65.5; p = 0.69). For patient survival, the RMST was 703 days versus 679 days, respectively (absolute difference, 24.2 days; 95% CI −46.6 to 94.9; p = 0.50).
3.4. Renal Function and Ischemia Time Analyses
Serum creatinine levels did not differ significantly between preservation strategies over the 24-month follow-up (repeated-measures ANOVA, p = 0.19). In both groups, serum creatinine levels improved significantly within the first 6 months after transplantation compared with discharge values (p < 0.001; Figure 3).
Cold ischemia time (CIT) was significantly longer in the SCS+HMP group (1545 min; 95% CI 1431–1660) than in the SCS group (1104 min; 95% CI 1008–1200; p < 0.001). After propensity score matching, CIT remained longer in the SCS+HMP group (1516 vs. 1105 min; p = 0.005), reflecting intrinsic characteristics of the preservation strategies. The distribution of CIT before and after matching is shown in Supplementary Figure S2.
In multivariable analysis, CIT analyzed as a continuous variable was not independently associated with DGF (OR per minute 1.0001; 95% CI 0.9995–1.0008; p = 0.68).
Similarly, hypothermic machine perfusion duration was not significantly associated with DGF when analyzed either as a continuous variable or according to quartiles.
4. Discussion
This study evaluated the clinical impact of a sequential kidney graft preservation strategy consisting of short static cold storage followed by prolonged hypothermic machine perfusion (SCS+HMP), compared with static cold storage (SCS) alone in a tertiary referral-center setting. The key finding is that sequential preservation was associated with a lower incidence of delayed graft function. Importantly, this effect was observed despite longer total preservation time in the SCS+HMP group.
Delayed graft function remains one of the most relevant early complications after kidney transplantation. Even short-term dysfunction may influence hospital stay, immunosuppressive management, and early graft assessment. Therefore, strategies that reduce DGF are clinically meaningful.
Static cold storage, which is regarded as the standard preservation method, reduces metabolic demand but does not provide active metabolic support. Even under hypothermic conditions, residual cellular metabolism persists, leading to depletion of energy stores, disruption of ion homeostasis, and accumulation of metabolic byproducts [12]. In addition, cessation of flow during static storage promotes endothelial dysfunction and increases susceptibility to ischemia–reperfusion injury [13,14]. In contrast, hypothermic machine perfusion maintains continuous circulation of preservation solution, supports microvascular flow, and facilitates removal of metabolic waste. Experimental and clinical studies suggest that this may limit ischemic injury and improve early graft function [15,16]. Consistent with the above mechanisms, we observed a 66% reduction in the odds of delayed graft function in our cohort (odds ratio, 0.34).
Notably, the benefit in early graft function occurred even though total cold ischemia time was substantially longer in the SCS+HMP group. Traditionally, prolonged preservation time is considered a major risk factor for DGF [17,18,19]. Our findings suggest that the method of preservation may be at least as important as its duration. When dynamic perfusion is applied, longer preservation time does not necessarily translate into worse early outcomes.
Importantly, the benefit observed in early graft function did not come at the expense of later outcomes. Patient survival, death-censored graft survival, and longitudinal renal function were comparable between groups. These findings indicate that extending preservation time in combination with hypothermic machine perfusion does not compromise overall transplant outcomes.
At the time of its introduction at our center, the sequential preservation strategy was adopted primarily for logistical reasons. During the COVID-19 pandemic, national transplant policy required recipients to undergo COVID-19 testing and high-resolution chest computed tomography prior to transplantation. In approximately 20% of cases, newly detected abnormalities led to recipient disqualification and necessitated additional time for recipient reassignment [20], thereby prolonging the pre-implantation interval. In this setting, sequential static cold storage (SCS) followed by hypothermic machine perfusion (HMP) provided a practical solution to maintain graft viability during unavoidable delays. Over time, however, the rationale for this approach evolved. HMP was increasingly applied not only to facilitate scheduling but also to improve graft condition prior to implantation, unless technical constraints prevented its use (e.g., inability to cannulate the renal artery) or the anticipated time to revascularization was less than 6 h. The present findings support this evolution in practice.
The preservation protocol evaluated here differs from strategies predominantly investigated in randomized controlled trials and more closely reflects real-world practice. Most trials have assessed continuous HMP initiated at the donor center [3,4,21,22,23] or short end-ischemic perfusion [24,25,26]. In contrast, our study examined prolonged HMP initiated after an initial phase of SCS, typically after organ arrival at a referral transplant center.
Preservation approaches similar to ours have been described. Adani et al. reported that delayed initiation of HMP after static cold storage may improve graft hemodynamics and attenuate ischemic injury accumulated during SCS [27]. Likewise, Patel et al. evaluated donation after circulatory death kidneys undergoing HMP following static cold storage and reported a reduction in delayed graft function from approximately 39% with SCS alone to 28% with sequential HMP, corresponding to a relative reduction of about 30% [28]. Importantly, this benefit was achieved without adverse effects on graft survival. These data provide quantitative support for the concept that initiation of machine perfusion after transportation may still confer measurable clinical benefit and are directionally consistent with our findings.
Several limitations should, however, be acknowledged. As a retrospective observational study, treatment allocation was not randomized, introducing potential selection bias and logistic confounding. Kidneys assigned to HMP were selected based on clinical judgment and anticipated logistical delays. Although propensity score matching reduced imbalances in measured variables, residual confounding from unmeasured factors cannot be excluded. An additional consideration pertains to the number-at-risk distributions in the Kaplan–Meier analyses. A marked decline in the SCS+HMP group beyond the first post-transplant year reflects administrative censoring rather than an excess of events. Because SCS+HMP became routine practice in our clinic from 2023 onward and the database was closed in 2025, many patients in this group had not yet reached two years of follow-up at the time of analysis. In contrast, most patients in the SCS group were transplanted earlier and therefore had longer available follow-up. Accordingly, the comparison partly reflects a newer institutional standard versus an earlier treatment period, and survival estimates at later time points in the SCS+HMP group should be interpreted with appropriate caution.
Despite these limitations, the study has notable strengths. The cohort reflects contemporary transplant activity in a high-volume tertiary referral center managing marginal donors and medically complex recipients. The preservation strategy evaluated addresses practical logistical challenges encountered in routine transplantation. Furthermore, clinically meaningful endpoints—including DGF, primary non-function, survival, and longitudinal renal function—were systematically assessed.
In summary, sequential preservation using static cold storage followed by prolonged hypothermic machine perfusion reduces the incidence of delayed graft function. Importantly, this improvement in early graft performance occurs despite extended preservation time and without compromising patient survival, graft survival, or renal function, supporting its role in contemporary transplant practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ozgur O.S. Namsrai B.E. Pruett T.L. Bischof J.C. Toner M. Finger E.B. Uygun K. Current practice and novel approaches in organ preservation Front. Transplant.20232115684510.3389/frtra.2023.115684538993842 PMC 11235303 · doi ↗ · pubmed ↗
- 2Fallon J. Sagar A. Elzawahry M. Sadik H. Gyoten K. Abbas S.H. Dumbill R. Friend P. The Hitchhiker’s guide to isolated organ perfusion: A journey to 2040 Front. Transplant.20254164272410.3389/frtra.2025.164272440881386 PMC 12381836 · doi ↗ · pubmed ↗
- 3Moers C. Smits J.M. Maathuis M.H. Treckmann J. van Gelder F. Napieralski B.P. van Kasterop-Kutz M. van der Heide J.J.H. Squifflet J.-P. van Heurn E. Machine perfusion or cold storage in deceased-donor kidney transplantation N. Engl. J. Med.200936071910.1056/NEJ Moa 080228919118301 · doi ↗ · pubmed ↗
- 4Tedesco-Silva H. Mello Offerni J.C. Ayres Carneiro V. de Paula M.I. Neto E.D. Lemos F.B.C. Moura L.R.R. Filho A.P.E.S. Cunha M.D.F.D.M. da Silva E.F. Randomized Trial of Machine Perfusion Versus Cold Storage in Recipients of Deceased Donor Kidney Transplants with High Incidence of Delayed Graft Function Transplant. Direct.20173 e 15510.1097/TXD.000000000000067228573190 PMC 5441986 · doi ↗ · pubmed ↗
- 5Jochmans I. O’Callaghan J.M. Pirenne J. Ploeg R.J. Hypothermic machine perfusion of kidneys retrieved from standard and high-risk donors Transpl. Int.20152866567610.1111/tri.1253025630347 · doi ↗ · pubmed ↗
- 6Zhang Y. Fu Z. Zhong Z. Wang R. Hu L. Xiong Y. Wang Y. Ye Q. Hypothermic Machine Perfusion Decreases Renal Cell Apoptosis During Ischemia/Reperfusion Injury via the Ezrin/AKT Pathway Artif. Organs.20164012913510.1111/aor.1253426263023 · doi ↗ · pubmed ↗
- 7Knijff L.W.D. van Kooten C. Ploeg R.J. The Effect of Hypothermic Machine Perfusion to Ameliorate Ischemia-Reperfusion Injury in Donor Organs Front. Immunol.20221384835210.3389/fimmu.2022.84835235572574 PMC 9099247 · doi ↗ · pubmed ↗
- 8Hosgood S.A. Yang B. Bagul A. Mohamed I.H. Nicholson M.L. A comparison of hypothermic machine perfusion versus static cold storage in an experimental model of renal ischemia reperfusion injury Transplantation 20108983083710.1097/TP.0b 013e 3181 cfa 1d 220098357 · doi ↗ · pubmed ↗