The IBD-FITT Study—Moderate-Intensity Exercise for Patients with Active Inflammatory Bowel Disease: An Open-Label Randomized Controlled Trial
Ken Lund, Torben Knudsen, Jens Kjeldsen, Kate Lykke Lambertsen, Rasmus Gaardskær Nielsen, Carsten Bogh Juhl, Bente Mertz Nørgård

TL;DR
A study tested if moderate exercise improves quality of life for people with active IBD, but found no significant difference compared to standard care.
Contribution
This is the first randomized controlled trial to investigate the impact of a 12-week exercise program on quality of life in patients with active IBD.
Findings
No statistically significant difference in quality of life scores between the exercise and control groups.
Recruitment and adherence to exercise sessions were challenging, with only 11 participants completing more than half of the sessions.
No clinically significant differences were observed in secondary outcomes like disease activity or inflammatory markers.
Abstract
Background: Exercise has been suggested as a supplementary modality for Inflammatory Bowel Disease (IBD), but supporting evidence remains scarce. We aimed to assess whether a 12-week physical exercise intervention improves quality of life (QOL) in adults with active IBD. Methods: An open-labeled randomized controlled trial examining the efficacy of a 12-week physical exercise intervention on QOL in adults (18–65 years) with active IBD. Participants were randomized 1:1 into either an intervention group, with two weekly supervised exercise sessions and one home session, or a control group with standard care. QOL by the Inflammatory Bowel Disease Questionnaire (IBDQ) was the primary outcome. Secondary outcomes were the European Quality of Life 5 Dimensions (EQ5D), waist circumference, blood pressure, disease activity, and lipid status. Explorative outcomes were C-reactive protein, fecal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
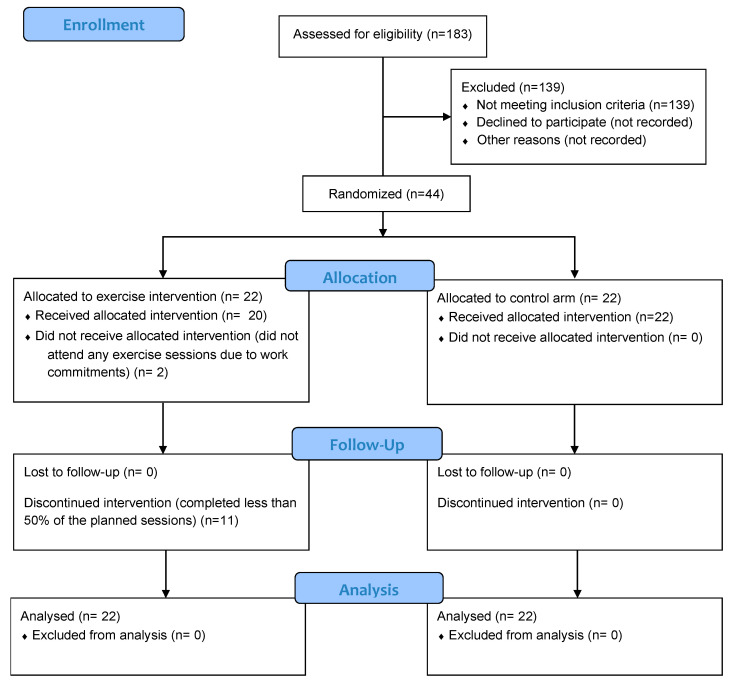 Figure 1
Figure 1- —Pfizer
- —Region of Southern Denmark
- —Louis-Hansen Foundation
- —Tryg Foundation
- —Danish Colitis Crohn’s Foundation
- —Chief Physician Association at Odense University Hospital–Region of Southern Denmark
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInflammatory Bowel Disease · Microscopic Colitis · Spondyloarthritis Studies and Treatments
1. Introduction
Inflammatory Bowel Diseases (IBD), Crohn’s disease (CD), and ulcerative colitis (UC) are chronic autoimmune diseases characterized by fluctuating disease activity. Complex medical therapies and surgical interventions are used to manage inflammation [1,2]. Disease control is important for maintaining quality of life (QOL), physical function, and study/work participation in an increasing population of IBD [3].
Structured physical exercise has been suggested as a supplementary treatment modality [4,5]. Exercise can potentially improve the immunological response, psychological health, and muscle and bone strength [5,6]. Furthermore, exercise may have a beneficial influence on patients’ well-being and QOL [4,5,7]. Although the mechanism is not fully understood, exercise increases cytokines, improving the regulation of inflammation and promoting an anti-inflammatory state that may reduce the disease activity in IBD [4,5]. However, evidence of its efficacy is limited, with a few empirical studies, mostly among patients in remission, which may have limited the measurable effect of exercise on inflammatory markers [4,5,6,7].
In adult patients with active IBD, we aimed to examine the efficacy of a 12-week physical exercise intervention on QOL, clinical disease activity, inflammatory markers, and immune response. For additional information, see the previously described protocol [8].
2. Materials and Methods
2.1. Study Design and Setting
This is an open-label randomized trial with two parallel groups randomized 1:1 in blocks of 4 after eligibility screening as previously described [8]. The intervention group received two supervised exercise sessions and one home session weekly, and the control group received standard care over 12 weeks. The study took place in gastroenterology outpatient clinics at two separate hospitals: The Department of Medical Gastrointestinal Diseases at Odense University Hospital and The Department of Medicine at Southwest Jutland Hospital. The intervention took place at an authorized physiotherapy clinic located in Odense and at the Department of Physiotherapy at Southwest Jutland Hospital.
2.2. Participants and Interventions
We included adults (18–65 years) with active IBD, indicated by a score of >5 points on the Harvey Bradshaw Index (HBI) for CD or on the Simple Clinical Colitis Activity Index (SCCAI) for UC, or a fecal calprotectin higher than 200 mg/g or C-reactive protein equal to or higher than 6 mg/L. Inclusion and exclusion criteria are detailed in the published protocol [8]. A 12-week moderate exercise program was designed to be accessible and adaptable regardless of prior exercise state [8]. Examples of exercises include biking, squats, and stepping. The intervention included two 60 min supervised exercise sessions per week and one home exercise session. A moderate exercise level was defined as 60–80% of maximum heart rate, and exercises were individually tailored by a physiotherapist, as described previously [8]. Adverse events were monitored during the exercise sessions [8]. Data were captured in paper diaries, entered into a database by a student worker, and controlled by the first author [8].
2.3. Outcomes
The primary outcome was QOL using the Inflammatory Bowel Disease Questionnaire (IBDQ) [8]. Secondary outcomes were European Quality of Life–5 Dimensions (EQ5D), body mass index, waist circumference, blood pressure, disease activity scores, lipid status, and explorative biomarkers for inflammation [8]. We analyzed the exploratory outcomes (cytokines) using the V-PLEX proinflammatory panel from Mesoscale Diagnostics (MSD, Rockville, MA, USA) on a SECTOR Imager 6000 Plate Reader (Mesoscale Discovery) according to the manufacturer’s instructions.
2.4. Statistics
Descriptively, categorical variables were presented using frequency, counts, median, and interquartile range (IQR). For continuous data, means with standard deviation (SD) were reported. Comparative analyses were conducted using an intention-to-treat approach, under the assumption of missing at random (MAR). To assess the validity of MAR, the baseline for participants who completed the study was compared to that of participants with missing outcome data. Multilevel mixed-effect linear and logistic regression models were employed for group comparisons, adjusting for age, sex, and type of disease as covariates when feasible, reporting means and 95% confidence intervals (95%CI). Additionally, a per-protocol subgroup analysis was performed to evaluate the change in VO_2_max (according to a Watt-max cycling test as previously described) [8] among participants who completed more than 50% of the sessions.
2.5. Ethical Approval
This study was approved by the Regional Ethics Committee of the Region of Southern Denmark (protocol code: S-20200003) on 27 February 2020 and registered at Clinicaltrials.gov (NCT04816812). This study was conducted in accordance with the Declaration of Helsinki. Informed consent was obtained from all subjects involved in the study.
3. Results
We screened 183 patients and included 44 participants, 22 in the intervention group and 22 in the control group. In the intervention group, 20 of 22 participants attended exercise sessions: 3 completed over 80% of supervised sessions, 11 over 50%, and 7 completed over 80% of home sessions. Recruitment and adherence to the exercise intervention were hindered by the time the exercise sessions were scheduled, which often conflicted with the participants’ work commitments. Figure 1 shows the consort flow diagram. Table 1 shows descriptive characteristics.
The IBDQ score showed no significant difference of 8 points between the intervention and control groups, with predicted mean scores of 172 (95%CI: 158–185) and 164 (95%CI: 151–178) at week 12. Five did not answer the IBDQ questionnaire completely at week 0 and week 12. Twelve had missing answers to the IBDQ questionnaire at week 0 or 12. Those who did not respond were not statistically significantly different in terms of age, sex, or type of disease. The EQ5D was divided into five subdomains plus the visual rating scale; none were statistically significantly different, except for the domain of pain and discomfort, which was significantly lower in the intervention group at week 12. No statistically significant differences were found in waist circumference and systolic blood pressure. Diastolic blood pressure and body mass index were statistically significantly lower and higher for the intervention group, respectively. For the clinical disease score, HBI, and SCCAI, a non-significant reduction in the score was observed at week 12. Lipid status and hemoglobin showed no significant difference and were generally within the normal range. Albumin was omitted due to missing data (only three measurements). No significant differences were found for explorative outcomes. Table 2 shows outcome measures.
In a per-protocol sub-analysis, participants who completed more than 50% showed a non-significant change in the relative VO_2_max (mL/kg/min) based on a bike Watt-max test from 30.25 (±SD: 4.41) to 31.60 (±SD: 3.54) at week 12. The mean of perceived exertion on the BORG scale [9] for all completed sessions was 12.5 points (±SD: 1.25). No adverse events were registered.
4. Discussion
In this randomized trial, we examined the efficacy of a 12-week supervised exercise program for patients with active IBD. We did not find a statistical difference between groups in the primary outcome of QOL or secondary outcomes, including disease activity and exploratory outcomes for inflammatory markers and immune response.
Structured exercise has been suggested for improving QOL and other outcomes in patients with IBD [4,5,7]. Still, evidence from randomized studies is limited, with varying results regarding efficacy, ranging from no changes to improvement for various outcomes based on various interventions [4,5,6,7]. Previously, improvement in QOL after exercise interventions has been shown [4], even though the studies are heterogeneous. We did not observe a significant difference in the QOL score, consistent with other studies, despite their use of different interventions and inclusion of patients in remission [4,6]. A recent systematic review including a meta-analysis has demonstrated a significant reduction in disease activity in exercise groups versus controls, but no significant changes for IBDQ scores or inflammatory markers [4]. The systematic review demonstrated the heterogeneity of the studies in changes to the IBDQ scores, with a mean difference ranging from 17.5 to −8.3 [4]. This variation may reflect differences in study populations, intervention types, and duration. Tew et al. [10] report a decline in IBDQ scores in their pilot randomized controlled trial of 36 adult patients with Crohn’s disease who undertook high-intensity and moderate-intensity continuous training over 6 months. Jones et al. [11] observed a mean of 4 points in the IBDQ score among 47 adults with stable Crohn’s disease following a 6-month intervention. Seeger et al. [6] observed a modest mean increase of 1 point in the short IBDQ score in their randomized trial of 45 patients with Crohn’s disease completing endurance and muscle training. These findings align with ours, showing no significant difference in the IBDQ score, even though our study has a shorter evaluation period of 3 months, differences in intervention types, and lower participant adherence. There are several important factors to consider when interpreting our results. Our study had a small sample size and low adherence to exercise sessions. The limited recruitment and adherence were hindered by several factors, even though regular screening was done. One factor could be that we were targeting participants with active disease, and another could be the scheduled time of day for the supervised exercise session or the length of 12 weeks. The exercise sessions were only offered at one morning hour (7–8 am) in Odense or during the daytime (between 9 am and 3 pm) in Esbjerg, which often conflicted with work commitments for most participants. Patients with IBD may also experience other barriers to participating in exercise, alone or in combination, such as fatigue, fear of increased toilet urgency, and abdominal pain [12].
Our study has several limitations. Recruitment was from November 2021 to May 2023, during which the coronavirus pandemic advanced in Denmark. To overcome this and to address the low number of participants, the inclusion period was extended by 6 months to approach our target of 150 participants [8]. Early in the project, the original inclusion criteria were revised to require either a disease score above 5 (HBI or SCCAI) or an increased clinical disease marker [8]. When assessing QOL scores, the minimal clinically important difference is important, and changes of 16 points in the IBDQ score are relevant [13], though the difference here was smaller. The treatment of active IBD may also contribute to the improvement in QOL in both groups. The open-label design in combination with self-reported QOL could be prone to an expectancy bias, which should be taken into consideration for these results. The limited adherence to the exercise intervention should be acknowledged, as this may limit adequate assessment of the efficacy. Lastly, some significant baseline differences, BMI and fecal calprotectin, may have influenced the results. Improving QOL in patients in remission remains a key focus for future studies.
Despite the limitations, some strengths are apparent. We used a randomized design to examine the efficacy of an exercise intervention in participants with active IBD, focusing on QOL and changes in inflammatory markers and cytokines. However, recruiting participants and ensuring adherence to the exercise sessions turned out to be challenging in our setup. Focusing on patients in remission and offering flexible scheduling outside working hours might have increased recruitment and adherence. Among the participants who completed the exercise sessions, the overall tolerance was good.
5. Conclusions
We did not observe a statistically significant difference in QOL after 12 weeks of exercise sessions in patients with active IBD compared to a control group. The recruitment and adherence to exercise sessions were low, mostly hindered by the time of day for the exercise sessions conflicting with work commitments. The number of participants was limited, reducing the ability to truly assess the efficacy of exercise in patients with active IBD. The results must be interpreted with this in mind, and the time of day for an exercise session is important for future studies. Physical activity may play an important role for patients with IBD in remission, offering numerous benefits, from cardiovascular health to better mental health, or potentially helping to prevent future relapse, which may be explored further in future studies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Raine T. Bonovas S. Burisch J. Kucharzik T. Adamina M. Annese V. Bachmann O. Bettenworth D. Chaparro M. Czuber-Dochan W. ECCO Guidelines on Therapeutics in Ulcerative Colitis: Medical Treatment J. Crohn’s Colitis 20221621710.1093/ecco-jcc/jjab 17834635919 · doi ↗ · pubmed ↗
- 2Gordon H. Minozzi S. Kopylov U. Verstockt B. Chaparro M. Buskens C. Warusavitarne J. Agrawal M. Allocca M. Atreya R. ECCO Guidelines on Therapeutics in Crohn’s Disease: Medical Treatment J. Crohn’s Colitis 2024181531155510.1093/ecco-jcc/jjae 09138877997 · doi ↗ · pubmed ↗
- 3Hracs L. Windsor J.W. Gorospe J. Cummings M. Coward S. Buie M.J. Quan J. Goddard Q. Caplan L. Markovinovic A. Global evolution of inflammatory bowel disease across epidemiologic stages Nature 202564245846610.1038/s 41586-025-08940-040307548 PMC 12158780 · doi ↗ · pubmed ↗
- 4Jones K. Kimble R. Baker K. Tew G.A. Effects of structured exercise programmes on physiological and psychological outcomes in adults with inflammatory bowel disease (IBD): A systematic review and meta-analysis P Lo S ONE 202217 e 027848010.1371/journal.pone.027848036454911 PMC 9714897 · doi ↗ · pubmed ↗
- 5Mc Gettigan N. Allen K. Saeidi R. O′ Toole A. Boland K. A systematic review of the effect of structured exercise on inflammation and body composition in inflammatory bowel disease Int. J. Color. Dis.20233814310.1007/s 00384-023-04437-237227593 PMC 10212817 · doi ↗ · pubmed ↗
- 6Seeger W.A. Thieringer J. Esters P. Allmendinger B. Stein J. Schulze H. Dignass A. Moderate endurance and muscle training is beneficial and safe in patients with quiescent or mildly active Crohn’s disease United Eur. Gastroenterol. J.2020880481310.1177/205064062093638332580666 PMC 7434996 · doi ↗ · pubmed ↗
- 7Sabir G. Abdelhady H.A. Oumar Abakar A. Gangavarapu R.R. Mahmud S.A. Manandhar A. Malasevskaia I. The Potential Benefits of Exercise in Managing Inflammatory Bowel Disease: A Systematic Review Cureus 202416 e 6894810.7759/cureus.6894839381484 PMC 11461038 · doi ↗ · pubmed ↗
- 8Lund K. Knudsen T. Kjeldsen J. Nielsen R.G. Juhl C.B. Norgard B.M. The IBD-FITT study—Moderate-intensity exercise for patients with inflammatory bowel disease with moderate disease activity: An open-label randomized controlled trial Trials 20232474210.1186/s 13063-023-07781-437986021 PMC 10659067 · doi ↗ · pubmed ↗