C-X-C Motif Chemokine Ligand 5 (CXCL5) Exhibits a U-Shaped Risk Profile for Mortality in Patients with Suspected Coronary Chest Pain
Dennis Winston T. Nilsen, Patrycja Anna Naesgaard, Volker Poenitz, Trygve Brugger-Andersen, Heidi Grundt, Annika Elisabet Michelsen, Pål Aukrust, Harry Staines, Thor Ueland

TL;DR
CXCL5, a platelet-derived chemokine, shows a U-shaped risk profile for mortality in patients with suspected coronary chest pain.
Contribution
This study identifies a U-shaped association between CXCL5 levels and mortality in coronary chest pain patients.
Findings
Both low and high CXCL5 levels are linked to increased mortality risk in patients with suspected coronary chest pain.
A U-shaped relationship was confirmed in both univariate and multivariable analyses.
The U-shaped risk profile was strengthened when including a composite endpoint of mortality, MI, or stroke.
Abstract
CXCL5 is a platelet-derived chemokine which promotes inflammatory responses in neutrophils and monocytes through CXCR2. Previous studies on CXCL5 in atherogenesis are to some degree conflicting, with scarce outcome data following acute coronary syndrome. This study aimed to assess the utility and risk profile of CXCL5 as a prognostic marker of all-cause mortality at 5-year follow-up in patients hospitalized for chest pain of suspected coronary origin. We measured CXCL5 levels in platelet-poor plasma in 826 consecutive patients included in the “Risk Markers in the Acute Coronary Syndrome” (RACS) study (ClinicalTrials.gov Identifier: NCT00521976). Stepwise Cox regression models, applying quintiles, were fitted for the biomarker with all-cause mortality within 5 years as the dependent variable. At 5-year follow-up, 250 (30.3%) of the population had died; 34.5% in Quintile (Qt)-1, 32.1% in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
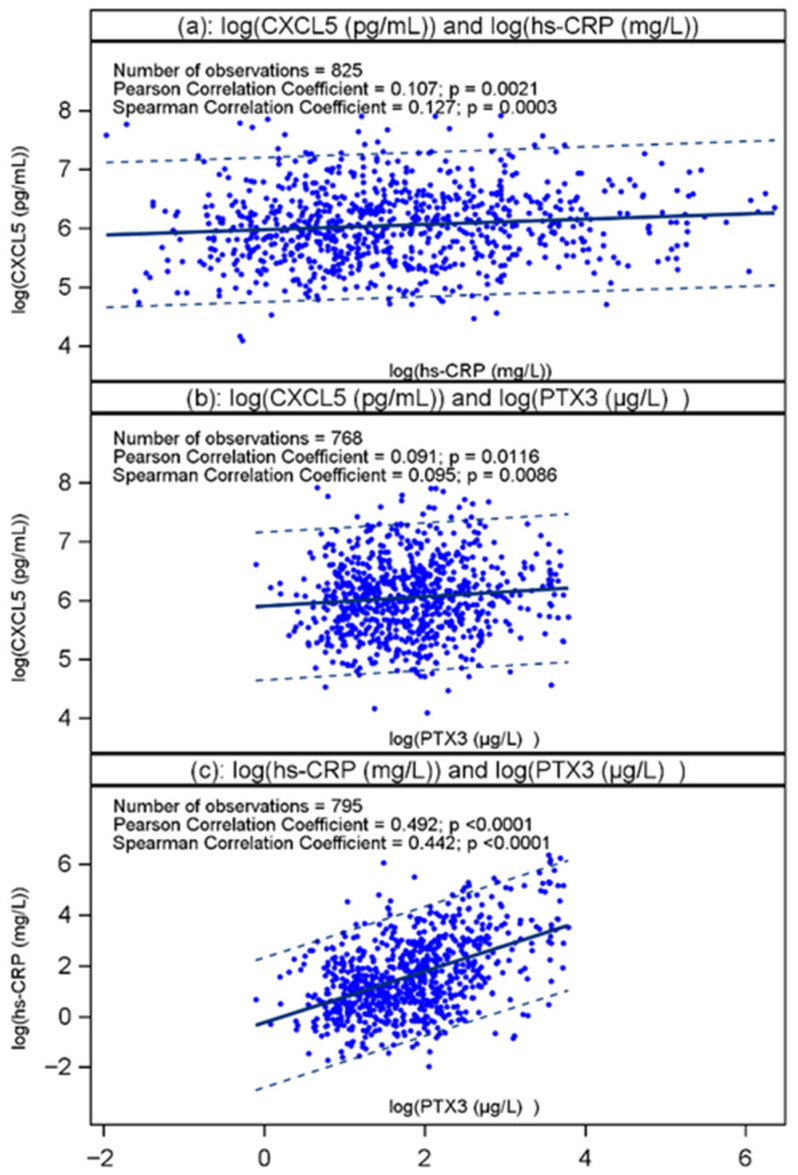 Figure 1
Figure 1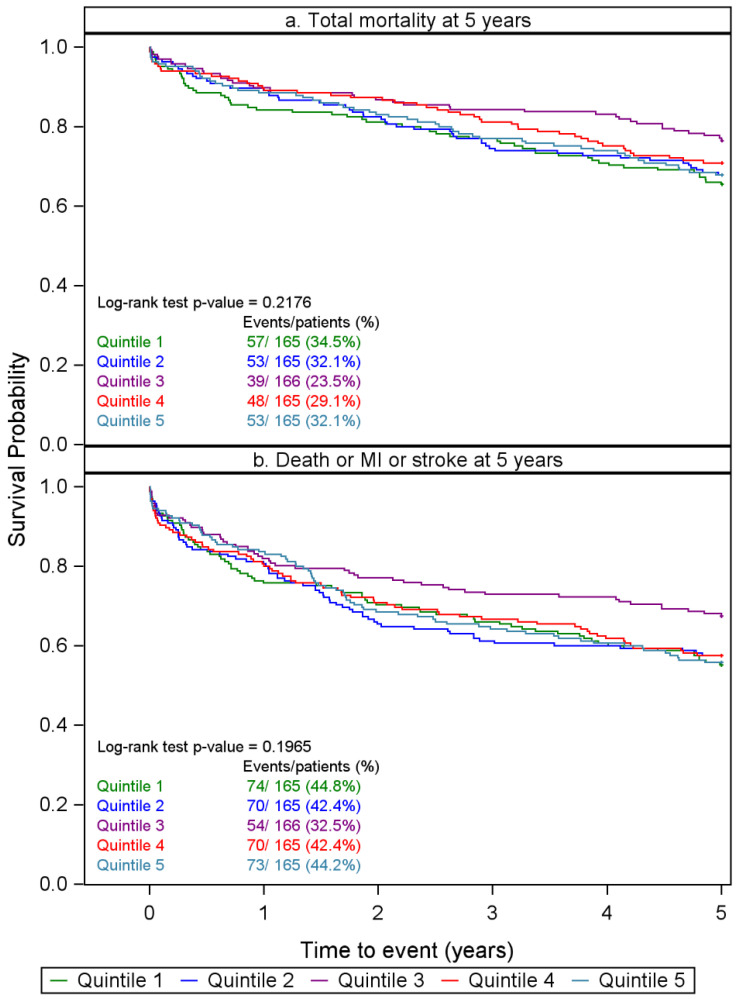 Figure 2
Figure 2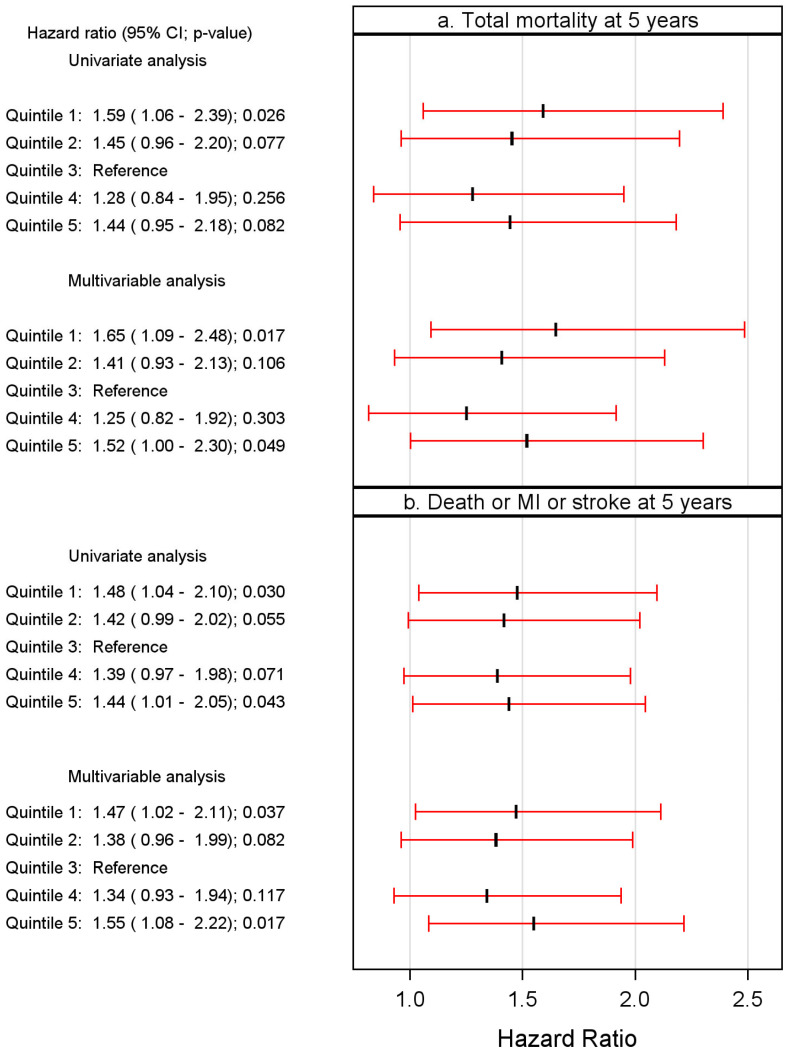 Figure 3
Figure 3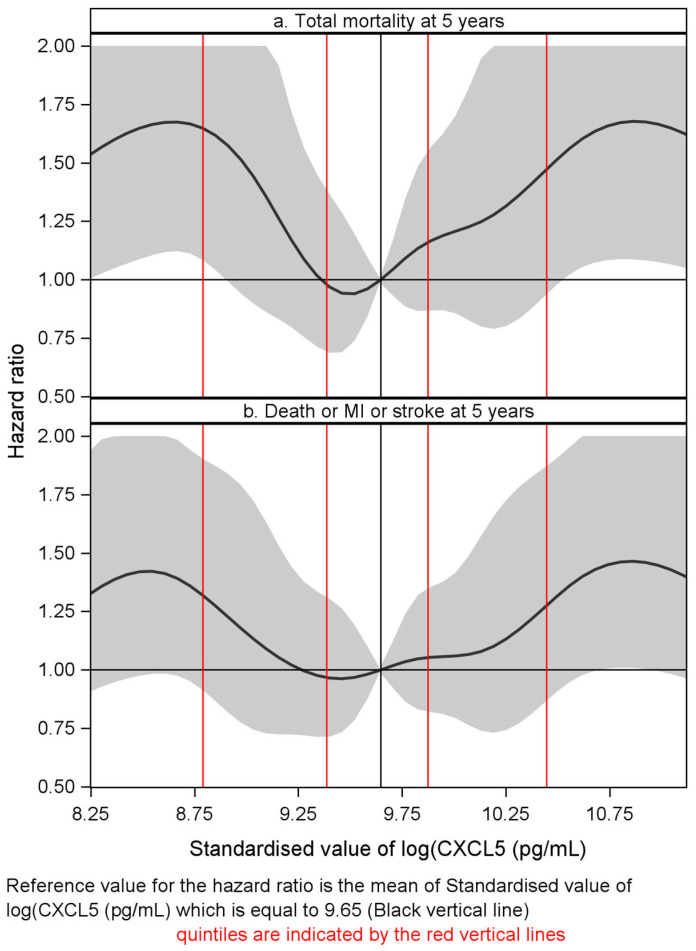 Figure 4
Figure 4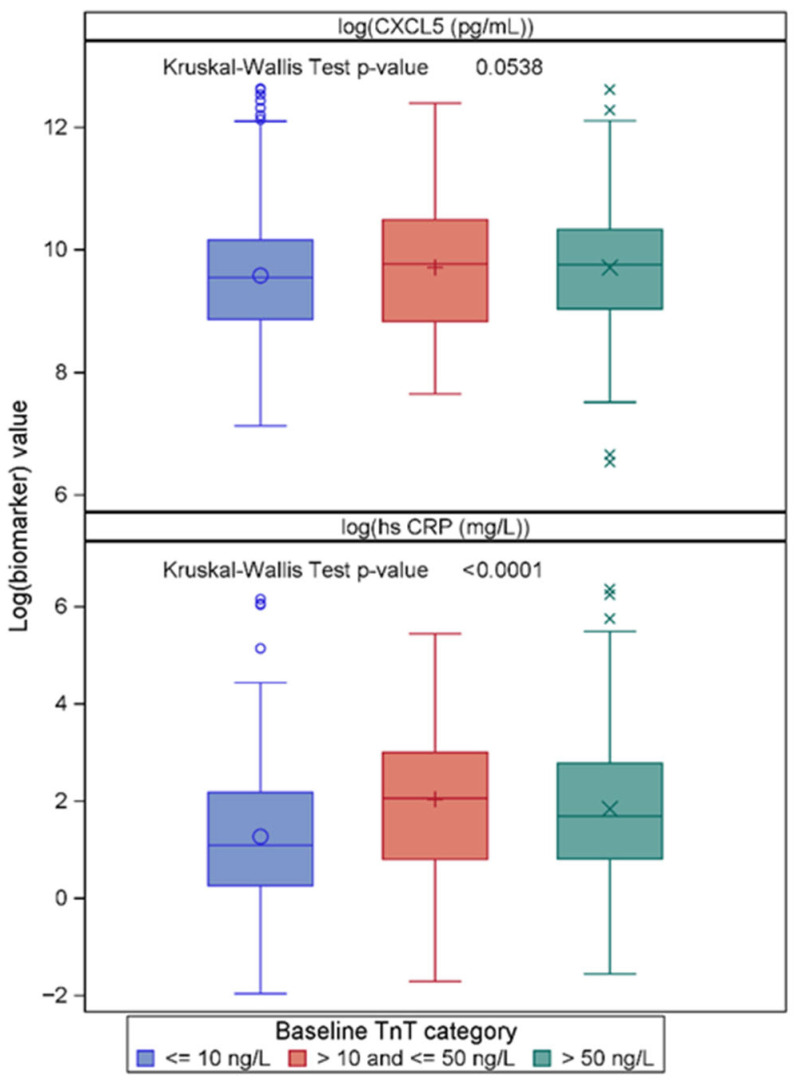 Figure 5
Figure 5- —Western Norway Regional Health Authority, Norway
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChemokine receptors and signaling · Cardiac Fibrosis and Remodeling · Acute Myocardial Infarction Research
1. Introduction
Chemokines are low-molecular-weight inflammatory cytokines that play a crucial role in innate and adaptive immune responses [1]. By attracting leukocytes into the atherosclerotic lesion and inducing activation of endothelial cells and different leukocyte subsets within the lesion, chemokines play an important role in plaque progression and destabilization [2]. Indeed, several studies have shown an association between circulating levels of certain chemokines (e.g., CXC motif chemokine ligand 8 [CXCL8], CXCL10, CXCL16 and CC motif chemokine ligand 2 [CCL2]) and cardiovascular risk [3]. These molecules could also represent novel targets for therapy in atherosclerotic disorders [4]. However, the chemokine family constitutes a wide range of molecules, and the role of these mediators in atherosclerosis and their clinical consequences are still not fully understood.
CXCL5/epithelial-derived neutrophil-activating peptide 78 (ENA-78), derived from a variety of cells including monocytes/macrophages, endothelial cells, epithelial cells and particularly platelets, is a potent chemoattractant for neutrophils, T cells and monocytes, and plays a major role in angiogenesis through interaction with the chemokine receptor CXCR2 [3,5,6,7,8,9,10]. We have previously reported enhanced release of CXCL5 from peripheral blood mononuclear cells (PBMCs) and platelets in patients with coronary artery disease (CAD) when exposed to oxidized low-density lipoprotein (oxLDL) [11]. Moreover, Chen et al. suggested that CXCL5 could be a marker of subclinical atherosclerosis in type 2 diabetes mellitus (T2DM) [12], supported by the findings in a report by Wang et al. [13]. On the other hand, a protective role of CXCL5 in atherosclerosis is also suggested, potentially involving the impairment of foam cell formation [14,15]. Thus, to this end, the role of CXCL5 in atherosclerosis and development of myocardial infarction (MI) is somewhat unclear, and data on CXCL5 in relation to outcomes following admission for chest pain of suspected coronary origin is, to the best of our knowledge, lacking.
To further elucidate the role of CXCL5 in atherosclerotic disorders, we have investigated the association between CXCL5 and clinical outcomes during 5 years of follow-up in a chest-pain population admitted to hospital with clinically suspected acute coronary syndrome (ACS).
2. Results
We measured CXCL5 in plasma from 826 patients admitted with chest pain of suspected coronary origin, applying its log_e_-transformed value. A flow-chart is displayed in Supplemental Figure S1, and a histogram showing the distribution of the transformed values is depicted in Supplemental Figure S2. Table 1 shows the baseline characteristics of the study population according to quintiles of CXCL5. There was a gradual almost-5-times increase in CXCL5 from the lowest to the highest quintile, whereas eGFR, BNP and Pentraxin 3 (PTX3), the last being found to predict outcome in this cohort in males [16], were similar in all quintiles. There was, however, a significant increase in hsCRP and total cholesterol across the quintiles from Qt-1 to Qt-5. The proportion of patients with a negative TnT decreased significantly and a borderline increase in patients with detectable TnT was noted from the lowest to highest quintile. Comparing the extreme quintiles (Qt-1 vs. Qt-5), statin (38.8 vs. 24.9%) and beta-blocker (40% vs. 27.7%) use occurred more frequently in the lowest as compared to the highest quintile. As shown in Figure 1, CXCL5 correlated weakly with hsCRP and PTX3, respectively. Supplemental Figure S3 shows a scatter plot based on the Pearson correlation coefficient between log_e_-transformed CXCL5 and log_e_-transformed BNP. Neither the Pearson nor the Spearman correlation coefficient was significant at the 5% level, suggesting that CXCL5 does not reflect myocardial wall stress.
2.1. CXCL5 in Relation to All-Cause Mortality During 5 Years’ Follow-Up
In this long-term follow-up study, all patients were assessed during a period of 5 years during which 250 patients had died. The risk of all-cause mortality was found to be U-shaped, employing cubic spline hazard ratios. The associations between CXCL5 quintiles and all-cause mortality during 5 years of follow-up are demonstrated in a Kaplan–Meier plot (Figure 2a). The log-rank test was non-significant (p = 0.218). In univariate analysis, however, the risk of all-cause mortality in Qt-1 was significantly higher (p = 0.026) than that of the Qt-3 reference and was also increased with borderline significance (p = 0.082) in Qt-5 as compared to Qt-3. Accordingly, we performed a quintile analysis of risk and chose the third quintile (Qt-3) as reference.
There were four confounders in the multivariable analysis (age, BNP quartile, history of chronic heart failure and TnT > 10 ng/L). However, neither of the inflammatory markers (hsCRP nor PTX3) was selected in the stepwise algorithm. In the multivariable analysis, the U-shaped risk pattern was maintained, in which the CXCL5 levels in both the lowest (p = 0.017) and the highest quintile (p = 0.049) were significantly and independently associated with all-cause mortality as compared to the reference quintile (Qt-3). This is clearly demonstrated in a forest plot (Figure 3a). The risk of all-cause mortality remained U-shaped in a cubic spline plot adjusted for the covariates in the corresponding MVA model (Figure 4a).
2.2. CXCL5 in Relation to the Composite Endpoint During 5 Years’ Follow-Up
By 5 years, 341 patients had either died or suffered an MI or a stroke. The risk of the composite endpoint was also U-shaped, and the third quintile (Qt-3) was chosen as reference. Quintiles of CXCL5-associated risk for the composite endpoint are demonstrated in the Kaplan–Meier curves shown in Figure 2b. The log-rank test was non-significant, with a p-value of 0.197. In univariate analysis, the risk of the composite endpoint was significantly higher in Qt-1 (p = 0.030) and in Qt-5 (p = 0.043) as compared to the Qt-3 reference, whereas both Qt-2 (p = 0.055) and Qt-4 (p = 0.071) demonstrated a borderline significant increase.
In relation to long-time follow-up, six confounders emerged in the multivariable analysis (age, BNP quartile, history of chronic heart failure and TnT > 10 ng/L, plus smoking history and taking ACE inhibitors or ARBs). In the multivariable analysis, again, a U-shaped risk pattern was maintained, in which CXCL5 levels in both the lowest (p = 0.037) and the highest quintile (p = 0.017) were significantly and independently associated with the combined endpoint as compared to the third reference quintile. This is clearly demonstrated in a Forest plot (Figure 3b). The risk of all-cause mortality remained U-shaped in a cubic spline plot adjusted for the covariates in the corresponding MVA model (Figure 4b). We did not conduct a specific analysis related to MI or stroke, as their individual numbers were considered too small for conclusive results.
2.3. CXCL5 in Relation to TnT Groups
The patient numbers and events in the TnT subgroups were considered statistically too low for the assessment of CXCL5-related risk. However, its levels across these subgroups were compared, together with those of hsCRP, to assess their discriminatory utility in relation to (1) suspected coronary chest pain with TnT < 10 ng/L [n = 381], (2) unstable angina with TnT values between 10 ng/L and up to 50 ng/L [n = 90], and (3) an acute MI with TnT levels > 50 ng/L [n = 355]. The results are shown in Figure 5. There was a statistically non-significant increase in CXCL5 (p = 0.054) along with increasing TnT levels, applying the Kruskal-Wallace test, whereas hsCRP increased significantly. Furthermore, a box plot by index diagnosis demonstrated no difference between patient groups, as shown in Supplemental Figure S4.
To further characterize our patients who displayed normal TnT values using the second-generation TnT assay and primarily classified as non-ACS, we measured high-sensitivity TnT in 29 randomly picked patients from this subgroup. Accepting an hsTnT level of <5 ng/L as negative, only nine patients in this subsample fulfilled the criteria of being negative, whereas those with elevated levels had values ranging from 5 to 35 ng/L, with a median of 14 ng/L. Thus, approximately 70% of patients originally defined as TnT-negative may have experienced an acute coronary event, and approximately 30% presented hsTnT values ≥ 14 ng/L, indicating the presence of an acute MI, defined according to hsTnT criteria [17].
3. Discussion
Data on the prognostic value of CXCL5 in relation to outcomes following admission for chest pain of suspected coronary origin are scarce. In the present study, the adjusted risk for all-cause mortality and the composite endpoint, respectively, showed a dual pattern of plasma CXCL5 levels in relation to outcome in the total population. Thus, the risk of all-cause mortality was increased in both the lowest and the highest quintile of CXCL5, using the third quintile as reference. Both extremes of the quintiles were independently associated with risk of death, suggesting a dual role of CXCL5 in atherosclerotic-related disease. This pattern may potentially reflect some previous studies describing both protective, i.e., modulation of macrophage phenotype and enhancement of cholesterol efflux [14], and harmful, i.e., enhancing neutrophil recruitment and plaque destabilization [18], effects of CXCL5, respectively. Moreover, whereas hsCRP and PTX3 are highly correlated, CXCL5 is only weakly correlated with hsCRP and PTX3, and can hardly be characterized as an acute-phase reactant.
Our findings of a positive relationship between the third and fifth quintiles of CXCL5 and all-cause mortality may support a previous report demonstrating a positive association between CXCL5 and the extent of CAD, potentially also reflecting a local accumulation of CXCL5 in coronary plaques [13]. Moreover, previous findings of an oxLDL-induced release of CXCL5 in PBMCs and platelets in patients with CAD could further support such a notion [11]. Furthermore, Zineh et al. identified a −156 G > C (rs352046) single-nucleotide polymorphism in the CXCL5 promoter that was associated with elevated plasma CXCL5 levels, and notably, this genotype was associated with increased mortality following ACS [19].
On the other hand, it has also previously been reported that increased CXCL5 expression in a mouse model did not increase neutrophil infiltration, whereas inhibition of CXCL5 expression induced a significant macrophage foam accumulation in murine atherosclerotic plaques [14]. Those findings would suggest a protective role of CXCL5 in atherosclerosis, as also claimed in a clinical report demonstrating a negative association between CXCL5 and CAD severity in 200 patients undergoing diagnostic coronary angiography [15].
The U-shaped association between CXCL5 and all-cause mortality requires further attention, and this is the first clinical outcome study that supports previous preclinical studies suggesting both protective and harmful effects of CXCL5 in relation to CAD and its clinical outcome. As the observed associations in the current report may reflect complex or unmeasured confounding, reverse causality, or unrelated biological processes, only assumptions can be made when comparing our data with those of previous reports.
The reasons for these dual effects are at present not clear. CXCL5 competes with other CXC chemokines in its class for their common receptor, CXCR2 [7,20]. Their affinities differ, not only in relation to the individual chemokine, but also in relation to whether the chemokines appear as monomers or dimers/oligomers, the latter being more strongly bound to the receptor [7]. Theoretically, considering dimers as blockers and monomers as activators of CXCR2, receptor accessibility may be increased at low concentrations of CXCL5 depending on the status of other chemokines and general immune response. At higher concentrations of CXCL5, more of its dimers are formed. This may result in less receptor availability, which could explain reports suggesting a protective role of CXCL5 [15]. However, at present, these issues are far from clear and need to be further investigated. Nonetheless, while previous studies on the dual role of CXCL5 are mainly based on preclinical models and in vitro experiments, the present study is, to the best of our knowledge, the first clinical study to support the double-edged role of CXCL5 in atherosclerosis, i.e., showing harmful associations of both low and high levels in the same patient cohort.
Limitations
Patients with coronary suspected chest pain were selected clinically for this study, irrespective of troponin values. Inclusions and blood sampling were performed immediately after admission. All patients presented with anginal pain at admission, compatible with a coronary origin. For support of myocardial damage, we employed a modified “second-generation” TnT assay [16], known to be less sensitive than more up-to-date assays [20]. However, not only the AMI population, but also a large number of non-AMI patients presented with a history of established coronary heart disease. Furthermore, our use of hsTnT in a subsample of randomly picked patients from the group of patients classified as non-ACS demonstrated minor myocardial injury in approximately 70% of these patients. Nevertheless, the lack of a definite clinical diagnosis related to this group of patients should be regarded as a study limitation. Blood sampling for the measurement of the biomarkers was limited to one draw at hospital admission, and the association found will have to be related to the time of admission. Further studies would have to be done to investigate whether the association is affected by measurements in blood samples harvested during the course of hospital stays. Moreover, as BNP was found to be a confounder, heart failure may influence outcome and presumably also the CXCL5 levels, and the lack of left ventricular ejection fraction and other data on myocardial function is a limitation of the study. Furthermore, all subjects were recruited from a Norwegian population, and the management of these patients in 2002–2003 differs somewhat from the standard of care today, although all patients received both aspirin and a statin, and also revascularization by either percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG) when clinically required according to national recommendations at the time of this study [16]. Moreover, demonstrating the ability of a biomarker to predict an outcome in clinical research may not apply to clinical practice due to the lack of automated instruments and assays with established reference ranges. Therefore, our results may not necessarily be generalizable and should be regarded as hypothesis-generating.
4. Materials and Methods
4.1. Study Design and Patient Population
Patients admitted to the emergency department with chest pain of suspected coronary origin were included consecutively in “Risk Markers in the Acute Coronary Syndrome (RACS)” (ClinicalTrials.gov Identifier: NCT00521976; approval date: 27 August 2007) [16]. The study was performed at Stavanger University Hospital, Norway, and included 871 patients recruited from November 2002 until September 2003.
The exclusion criteria were age < 18 years, unwillingness or incapacity to consent, and prior inclusion. An acute MI was defined by a Troponin-T (TnT) cut-off value of 50 ng/L, employing a rule-in-rule-out MI protocol based on blood samples harvested at baseline and 6–7 h after admission, and additional information from ECG readings was collected for further classification of the MI, as previously described [16]. Clinical follow-up data were based on hospital and public registries and by telephone interview at 30 days and 6, 12, 24 and up to 84 months, and any additional information was obtained from general practitioners and nursing homes [16]. Mortality beyond 2 years was essentially provided from death registries and limited to all-cause mortality [16]. Baseline data including demographics, smoking habits, clinical history, and general laboratory characteristics were collected at hospital admission.
4.2. Ethics
Written informed consent was required for participation. The study was approved by the Regional Board of Research Ethics and by the Norwegian Health Authorities, approval code: 118.02. The latest approval was by the Regional Board of Research Ethics, approval code 5764; approval date: 7 November 2024. It was conducted in accordance with the Helsinki Declaration of 1971, as revised in 1983.
4.3. Blood Sampling and Laboratory Measurements
Blood samples were collected by direct puncture of an antecubital vein immediately following hospital admission, applying a minimum of stasis, and an additional sample for measurement of TnT was drawn 6–7 h later. Centrifugation was performed for 15 min at 2000 g at 20 °C to obtain platelet-poor plasma, which was stored in aliquots as ethylene diamine tetra-acetic acid (EDTA) plasma and citrated plasma, respectively, at −80 °C. Routine tests, including for high-sensitivity C-reactive protein (hsCRP), TnT, brain natriuretic peptide (BNP) and estimated glomerular filtration rate (eGFR), were analyzed by the Medical Biochemistry Department at Stavanger University Hospital. TnT was measured with a modified second-generation assay. To obtain additional information with regard to myocardial injury in patients with TnT levels ≤ 10 ng/L, we randomly picked a subsample for measurement of high-sensitivity troponin-T (hsTnT), which was analyzed at the Medical Biochemistry Department at the National Hospital, Rikshospitalet, Oslo, by an electrochemiluminescence immunoassay (Elecsys 2010 analyzer, Roche Diagnostics, Basel, Switzerland).
4.4. Measurement of CXC Motif Chemokine Ligand 5 (CXCL5)
CXCL5 (pg/mL) was analyzed in duplicate in plasma from 826 patients, using an enzyme-linked immunosorbent assay (ELISA) with antibodies from R&D Systems (Catalog #: DY254, Minneapolis, MN, USA), and applying a 384-well format with a combination of a SELMA (Jena, Germany) pipetting robot and a BioTek (Winooski, VT, USA) dispenser/washer. An ELISA plate reader (BioTek) was used to measure absorption at 450 nm with wavelength correction to 540 nm. The intra- and inter-assay coefficients were <10%.
4.5. Statistics
Descriptive statistics are presented as medians with interquartile ranges (25th–75th percentiles) for continuous data and as numbers and percentages for categorical data. Differences in baseline characteristics were assessed by the Kruskal–Wallis test for continuous data and the Chi-squared test for categorical data. Due to a skewed distribution, Pearson’s and Spearman’s rank correlation coefficients were calculated between the log_e_-transformed values of biomarkers. For the cubic spline and Cox models, the log_e_-transformed CXCL5 value was normalized by dividing by the standard deviation (SD). Hence, the hazard ratios presented in the Results section are 1-SD on the log scale. The lack of prior knowledge on the nature of the CXCL5 effect suggested using a reasonable number of knots to add flexibility. The cubic split plot supported the use of quintiles and quintile-3 as the reference. Thus, restricted cubic splines were fitted at eight knots located at percentiles; 2.5, 97.5 and six equally spaced values in between. The hazard ratios, using the mean value of the normalized log (CXCL5) as the reference, were plotted to visualize the shape of the hazard associated with CXCL5. For the composite endpoint, the times to the first death, MI and stroke were used. No patients were lost to follow-up, and patients without an event were censored at five years. The Kaplan–Meier product limits were used for plotting the times to events, and the log-rank test was used to test for the equality of the survival curves. Cox regression models, using CXCL5 quintiles, with quintile-3 as the reference level, were fitted using the clinical endpoint as the dependent variable. The Cox model was based on quintiles alone and not on cubic splines. Results are shown separately for the univariate (UVA) and multivariable analysis (MVA), respectively. The multivariable model included potential covariables [shown by an asterisk in the baseline table (Table 1)] selected using a stepwise algorithm added to the model containing CXCL5 quintiles, applying a p-value threshold of 0.05 for entry and 0.10 for removal. Statistics were performed using the statistical package SPSS version 25 (IBM Corp. Armonk, NY, USA). All tests were 2-sided with a significance level of 5% without multiplicity adjustment.
5. Conclusions
The present study is the first to support a dual role of CXCL5 in relation to clinical outcome in patients with chest pain of suspected coronary origin, with both low and high levels demonstrating a significant association with all-cause mortality or a composite endpoint consisting of all-cause mortality, MI or stroke at 5-year follow-up. These findings demonstrate a double-edged sword nature of CXCL5 where both high and low levels may be harmful. Its negative association with events at low levels is of particular interest, as this supports previous reports claiming beneficial anti-atherosclerotic effects in murine experiments and in patients undergoing diagnostic coronary angiography, in conflict with other studies claiming the opposite, which is more in accordance with a traditional point of view.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Murphy P.M. Chemokines and Chemokine Receptors Clinical Immunology 5th ed.Principles and Practice Elsevier Amsterdam, The Netherlands 201910.1016/B 978-0-7020-6896-6.00010-7 · doi ↗
- 2Ajoolabady A. Pratico D. Lin L. Mantzoros C.S. Bahijri S. Tuomilehto J. Ren J. Inflammation in atherosclerosis: Pathophysiology and mechanisms Cell Death Dis.20241581710.1038/s 41419-024-07166-839528464 PMC 11555284 · doi ↗ · pubmed ↗
- 3Aukrust P. Halvorsen B. Yndestad A. Ueland T. Øie E. Otterdal K. Gullestad L. Damås J.K. Chemokines and cardiovascular risk Arterioscler. Thromb. Vasc. Biol.2008281909191910.1161/ATVBAHA.107.16124018669888 · doi ↗ · pubmed ↗
- 4Noels H. Weber C. Koenen R.R. Chemokines as therapeutic targets in cardiovascular disease Arterioscler. Thromb. Vasc. Biol.20193958359210.1161/ATVBAHA.118.31203730760014 · doi ↗ · pubmed ↗
- 5Damås J.K. Gullestad L. Ueland T. Solum N.O. Simonsen S. Frøland S.S. Aukrust P. CXC-chemokines, a new group of cytokines in congestive heart failure—Possible role of platelets and monocytes Cardiovasc. Res.20004542843610.1016/S 0008-6363(99)00262-X 10728363 · doi ↗ · pubmed ↗
- 6Guo L. Li N. Yang Z. Li H. Zheng H. Yang J. Chen Y. Zhao X. Mei J. Shi H. Role of CXCL 5 in regulating chemotaxis of innate and adaptive leukocytes in infected lungs upon pulmonary influenza infection Front. Immunol.20211278545710.3389/fimmu.2021.78545734868067 PMC 8637413 · doi ↗ · pubmed ↗
- 7Sepuru K.M. Nagarajan B. Desai U.R. Rajaratham K. Molecular basis of CXCL 5-glycosaminoglycan interactions J. Biol. Chem.2016291205392055010.1074/jbc.M 116.74526527471273 PMC 5034048 · doi ↗ · pubmed ↗
- 8Saha S. Sano F.K. Sharma S. Ganguly M. Mshra S. Dalal A. Akasaka H. Kobayashi T.A. Zaidi N. Tiwari D. Molecular basis of promiscuous chemokine binding and structural mimicry at the C-X-C chemokine receptor, CXCR 2Mol. Cell 20258597698810.1016/j.molcel.2025.01.02439978339 PMC 7617694 · doi ↗ · pubmed ↗