Usability Evaluation of a Central Monitoring System with AI-Based Cardiac Arrest Prediction in the ICU
Jiyoon Oh, Yourim Kim, Wonseuk Jang

TL;DR
This study evaluated how well ICU nurses can use a central monitoring system with AI to predict cardiac arrest, finding it generally acceptable but needing design improvements.
Contribution
A summative usability evaluation of an AI-based cardiac arrest prediction system in a simulated ICU environment.
Findings
The system achieved a 90% task success rate with critical tasks ranging from 73% to 100% success.
The System Usability Scale score was 67.3, indicating an 'OK' usability rating.
User satisfaction averaged 4.5, showing generally positive perception despite some design issues.
Abstract
Background/Objectives: The incidence of cardiac arrest among critically ill patients has been increasing, with many patients experiencing clinical exacerbation prior to the event. Early detection and rapid treatment are essential to reduce the risks associated with cardiac arrest; however, difficulties such as limited ICU resources and inadequate monitoring of vital signs reduce the effectiveness of treatment. Various cardiac arrest prediction systems have been developed to overcome these issues. This study performed a summative evaluation of a Central Monitoring System with AI-based Cardiac Arrest Prediction. Methods: A summative usability evaluation was conducted in a simulated ICU environment with 22 ICU nurses experienced in using patient monitoring devices. Participants completed tasks based on the device workflow and then filled out the System Usability Scale (SUS) and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
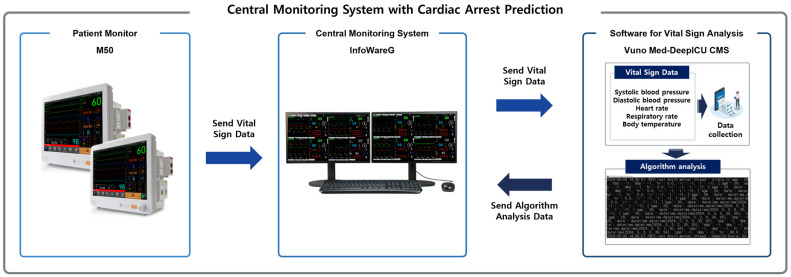 Figure 1
Figure 1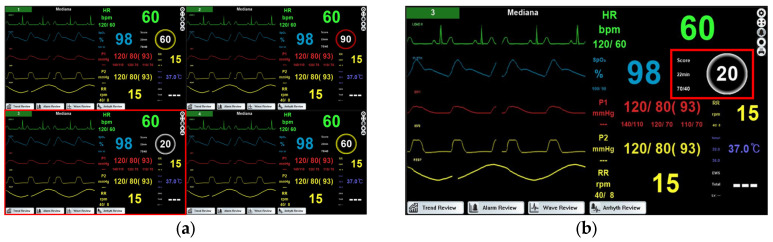 Figure 2
Figure 2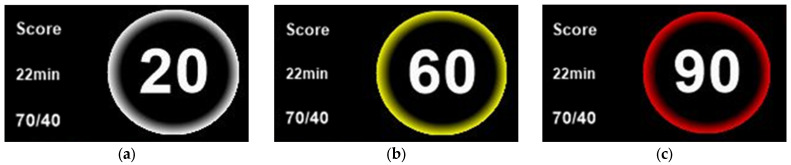 Figure 3
Figure 3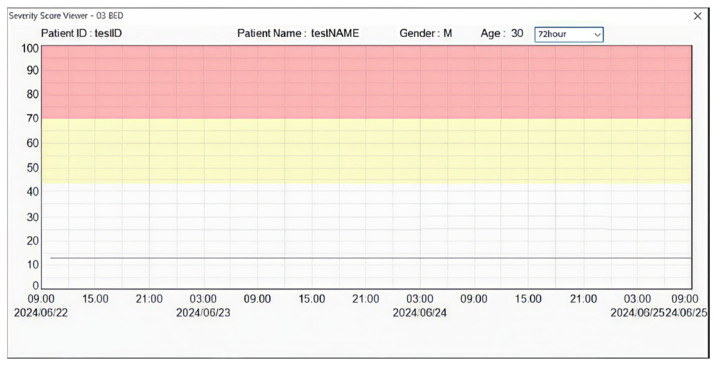 Figure 4
Figure 4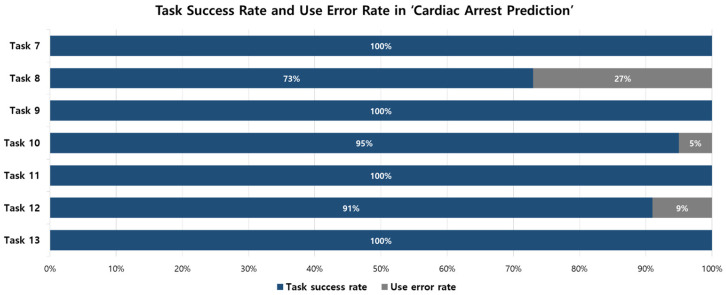 Figure 5
Figure 5- —Korean government Korea Medical Device Development Fund
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrest and Resuscitation · Sepsis Diagnosis and Treatment · Healthcare Technology and Patient Monitoring
1. Introduction
The incidence of cardiac arrest among patients admitted to the intensive care unit (ICU) has been increasing annually, and the mortality rate of patients who experience cardiac arrest is higher than that of those who do not [1,2]. Up to 80% of patients show signs of clinical exacerbation before experiencing cardiac arrest [3,4]. Early detection and rapid treatment are important to prevent further exacerbation following cardiac arrest. However, difficulties such as limited ICU resources, inadequate vital signs monitoring, and untimely corrective actions reduce the effectiveness of treatment [1,5]. To overcome these issues, various countries have investigated strategies such as the operation of Medical Emergency Teams, specialized training programs for managing critically ill patients, and the development of systems to predict patient exacerbation [1,6,7,8].
Several studies have been conducted on the development of cardiac arrest prediction systems for use in emergency departments and ICUs. Using databases such as MIMIC (Medical Information Mart for Intensive Care), eICU-CRD (eICU Collaborative Research Database), researchers have developed prediction algorithms based on patients’ electrocardiogram (ECG) data and vital signs [9,10]. These algorithms have demonstrated high predictive performance, with an AUC of 0.80 or higher, indicating their potential for real-time prediction of cardiac arrest in the ICU [9,10]. Despite the high predictive performance reported in previous studies, the real-world implementation of AI-based clinical decision support systems remains limited due to challenges related to workflow integration, interface usability, and clinician acceptance [11].
In this study, we developed a Central Monitoring System with Cardiac Arrest Prediction for use in ICUs to predict the risk of cardiac arrest in real time. Vital signs measured by the patient monitor are sent to the central monitoring system, and an artificial intelligence-based algorithm analyzes the data to estimate the patient’s risk of cardiac arrest. The estimated risk can be reviewed on the central monitoring system. The system was designed to generate predictions based on routinely collected vital signs and patient information in the ICU without requiring additional tests, enabling continuous and stable application in clinical environments [8].
ICUs are environments designed to provide treatment for critically ill patients and are equipped with various devices such as patient monitors and ventilators [12,13]. In particular, patient monitors are widely used for continuous monitoring, enabling the observation of parameters such as invasive blood pressure, electroencephalogram (EEG), electrocardiogram (ECG), carbon dioxide (CO_2_) levels, and transcutaneous oxygen saturation (SpO_2_) [14,15]. ICU nurses are responsible for providing care to critically ill patients and making decisions in critical situations, resulting in higher workload compared with other departments [12]. The demanding work environment and the quality of medical equipment contribute to ICU nurses’ occupational stress, which can negatively affect patient outcomes [16]. In addition, frequent alarms may lead to alarm fatigue, which can disrupt workflow and compromise patient safety [17]. In such high workload settings, use errors related to medical devices are more likely to occur [14]. Therefore, before implementing new technologies, particularly systems with alarm-based prediction functions, it is important to perform systematic usability testing to identify potential use errors and analyze their root causes [18,19].
A usability test focuses on evaluating whether users can complete tasks that are based on the device’s workflow [19]. Formative evaluation is conducted during the development process to evaluate the suitability of the user interface and to identify unexpected use errors [20]. Summative evaluation is performed to demonstrate that the medical device can be used safely and effectively without serious use errors [20]. While previous studies have mainly focused on the predictive performance of cardiac arrest algorithms, this study performed a summative evaluation of a Central Monitoring System with AI-based Cardiac Arrest Prediction in a simulated environment with 22 ICU nurses.
2. Materials and Methods
2.1. Central Monitoring System with AI-Based Cardiac Arrest Prediction
2.1.1. Configuration
As illustrated in Figure 1, a Central Monitoring System with Cardiac Arrest Prediction consists of a patient monitor, a central monitoring system, and software for vital sign analysis.
The M50 (Mediana Co., Wonju-si, Gangwon-do, Republic of Korea) is a patient monitor (PM) designed to monitor patients by measuring vital signs such as electrocardiogram (ECG), heart rate (HR), non-invasive blood pressure (NIBP), oxygen saturation (SpO_2_), pulse rate (PR), respiration rate (RR), and body temperature.
InfoWareG (Mediana Co., Wonju-si, Gangwon-do, Republic of Korea) is a central monitoring system (CMS) that integrates data from multiple patient monitors and generates visual or auditory alarms when signs of patient exacerbation are detected.
VUNO Med-DeepICU CMS (v1.0.X; VUNO Inc., Seoul, Republic of Korea) is software for vital sign analysis designed to support diagnosis, analysis, and simulated treatment by integrating patients’ vital signs. It collects and analyzes systolic and diastolic blood pressure, pulse rate, respiratory rate, and body temperature to present a cardiac arrest prediction score ranging from 0 to 100. Previous study has demonstrated the high predictive performance of VUNO Med-DeepICU CMS for cardiac arrest prediction [8].
The patient monitor (M50) collects the patient’s vital signs and transmits the data to the central monitoring system (InfoWareG). The central monitoring system then forwards the data to the vital sign analysis software (VUNO Med-DeepICU CMS). The software analyzes the patient’s age, vital signs, and the timing of measurements to generate a cardiac arrest prediction score ranging from 0 to 100. The central monitoring system displays the cardiac arrest prediction score on the screen, enabling real-time monitoring.
2.1.2. GUI (Graphical User Interface)
Figure 2a shows the central monitoring system screen displaying multiple beds simultaneously. Figure 2b is an enlarged view of the area highlighted by the red box in Figure 2a, showing the main screen of the central monitoring system for a single bed. The cardiac arrest prediction score, generated by the software for vital sign analysis, is displayed on this screen. The area where the score appears is highlighted with a red box in Figure 2.
The cardiac arrest prediction score is represented as a number ranging from 0 to 100, with higher scores indicating an increased risk of cardiac arrest. By clicking the “score” area on Figure 3, users can view the scores generated over a defined interval. The “22 min” indicates the time since the score was generated, and the score is updated every 30 min. The “70/40” represents the severity step 2 limit (70, secondary alarm) and step 1 limit (40, primary alarm), defining the risk levels of cardiac arrest. According to the ANSI/AAMI HE75:2009 (R2018) standard, a white color is used to convey primary information on a black background, a yellow color indicates a medium or low priority alarm for medical purposes and caution for potential hazards, and a red color signals a high-priority alarm and danger [21]. In the central monitoring system, these colors are applied to the borders of the cardiac arrest prediction score circles to indicate the risk level to the user. A white border represents a score of 0–40, indicating a normal status (Figure 3a). A yellow border represents a score of 41–70, indicating a primary alarm that suggests an increased risk of cardiac arrest (Figure 3b). A red border represents a score of 71–100, indicating a secondary alarm that reflects a high risk of cardiac arrest (Figure 3c).
Figure 4 shows the screen displaying the cardiac arrest prediction scores generated within a 72-h period. Users can view the generated scores for 24-h or 48-h periods by selecting a period on the screen.
2.2. Study Design
In accordance with IEC 62366-1 recommendations, a total of 22 ICU nurses with prior experience using a patient monitor or a central monitoring system were recruited via email, exceeding the minimum of 15 participants required for a summative evaluation. All participants provided informed consent before participating in this study, and their demographic information, including sex, age, work experience, and user experience with similar devices, was recorded. They performed tasks based on predefined use scenarios and, following the usability test, completed the System Usability Scale (SUS) questionnaire and a satisfaction survey.
This study was approved by the Institutional Review Board (IRB) of Gangnam Severance Hospital (Approval No.: 3-2024-0212, approved on 25 July 2024) and conducted in the Medical Device Usability Research Center (Gangnam-gu, Seoul, Republic of Korea) from July 2024 to October 2024.
2.3. Study Procedure
One participant was involved per test session. The facilitator introduced the test procedure and obtained informed consent forms from each participant. A training moderator conducted a 15-min training session covering device operation, GUI navigation, and the cardiac arrest prediction score, and participants were allowed to interact with the device. To minimize the influence of training on task performance, the usability test was conducted 10 min after the training session [20]. The test environment was arranged to resemble an actual ICU nurse station. Each session was observed in real time using monitoring equipment capable of recording.
Participants conducted 4 use scenarios (consisting of 18 tasks) for 20 min. The scenarios were designed to reflect clinical workflows and included Basic Settings (initial device setup), Cardiac Arrest Prediction (review of patient risk indicators), Patient Review (review of patient data), and Patient Discharge (patient discharge procedures). A risk analysis was conducted to identify tasks where use errors could potentially lead to harm, defined as injury or damage to the health of people, or damage to property or the environment. Tasks that could result in serious outcomes, such as death or permanent injury, were defined as critical tasks. Risk for each task was calculated according to ISO 14971 as the combination of harm probability and severity [22]. All tasks for each scenario are listed in Table 1. After completion of the usability test, participants completed the SUS survey and a satisfaction survey.
2.4. Analysis
2.4.1. Usability Test
Participants’ task performance was observed in real time using recording-capable monitoring equipment, and use errors were analyzed based on the recorded data. Task outcomes were categorized as Completed (C), Completed with Issues (CI), or Did Not Complete (NC). C indicates successful task completion without any observed or reported errors; CI refers to cases where errors occurred but were self-corrected (close call) or where difficulties were encountered, yet the task was completed (difficulty); NC includes a task that was not completed, completed incorrectly or required assistance from the moderator [20].
Task success rate was defined as the proportion of participants who achieved either C or CI, relative to the total number of participants. Use error rate was defined as the proportion of participants with NC outcomes. In this study, the goal was to achieve a task success rate of at least 70% and a use error rate below 30%, which was set considering the characteristics of the device and the actual clinical environment.
2.4.2. SUS (System Usability Scale) Survey
The SUS survey is widely used to evaluate the usability of systems across various fields [23]. As shown in Table 2, the SUS consists of 10 items, with odd-numbered items using positive statements and even-numbered items using negative statements [24]. Each item is rated on a 5-point Likert scale. For odd-numbered items, a score of 1 indicates “strongly disagree,” and a score of 5 indicates “strongly agree” [25]. For even-numbered items, a score of 1 indicates “strongly agree,” and a score of 5 indicates “strongly disagree” [25]. To calculate the SUS score, which ranges from 0 to 100, odd-numbered items are scored by subtracting 1 from the user response, and even-numbered items are scored by subtracting the user response from 5. The total sum is then multiplied by 2.5 to determine the SUS score [26]. The SUS score can be interpreted as Worst Imaginable (≤12.5), Poor (12.5–50.8), OK (50.9–71.3), Good (71.4–85.4), Excellent (85.5–90.8), and Best Imaginable (≥90.9) [27].
2.4.3. Satisfaction Survey
A satisfaction survey was conducted after the usability test to evaluate satisfaction with the device. As shown in Table 3, the satisfaction survey consisted of 9 items rated on a 5-point scale. A score of 5 indicated a very positive response, and a score of 1 indicated a very negative response. The satisfaction score was calculated as the average of the participants’ responses across all items.
3. Results
3.1. Demographic Characteristics
This study was conducted with 22 nurses who had experience using a patient monitor or central monitoring system. The participants had an average age of 38.0 years and an average clinical experience of 13.8 years. Demographic characteristics are shown in Table 4. All participants completed the usability test, SUS survey, and satisfaction survey.
3.2. Usability Test
Participants performed four use scenarios consisting of 18 tasks. The overall task success rate was 90%, with a mean success rate of 88% across the three critical tasks, meeting the pre-established goal. Task success rates and use error rates for each scenario are shown in Table 5. The task success rate was 89% for the “Basic Settings” scenario and 94% for “Cardiac Arrest Prediction”. The task success rates were 89% for ‘Basic Settings,’ 94% for ‘Cardiac Arrest Prediction,’ 81% for ‘Patient Review,’ and 100% for ‘Patient Discharge.’
In the ‘Basic Setting’ scenario (Tasks 1–6), all tasks except Task 4 achieved success rates above 90%. Task 4, which involves setting the severity limit, had a success rate of 45%, below the goal of 70%. The low success rate was due to a use error resulting from poor visibility of the setting button.
The task success rates for ‘Cardiac Arrest Prediction’ (Tasks 7–13) are shown in Figure 5. Critical tasks that were pre-defined (Tasks 8, 9, and 12) also met the goal. Tasks 8 and 12, which involved confirming the severity of alarms and the patient’s respiration and heart rates, achieved success rates of 73% and 91%. Task 9, which involved pausing the alarm, achieved a 100% success rate.
Tasks 7 and 13 are tasks for checking the patient’s cardiac arrest prediction score, both achieving a success rate of 100%. A difference in the method of displaying alarm severity between InfoWareG (CMS) and the previously used system was identified as a cause of use errors. The previously used system displayed the severity of the alarm using red, yellow, and cyan, whereas InfoWareG (CMS) used red, flashing yellow, and yellow. This difference is expected to lead to a reduction in the user error rate through user training and continued use. Task 9 is a task for pausing the alarm, which achieved a task success rate of 100%. Tasks 10 and 11 are tasks for operating the monitoring screen. Task 10 achieved a task success rate of 95%, and Task 11 achieved 100%.
In the ‘Patient Review’ scenario, Tasks 15 and 16 both achieved 100% success rates. However, Task 14, for checking the patient’s alarm history, and Task 17, for reviewing the cardiac arrest prediction score trends, achieved 68% and 55%, respectively, falling below the 70% goal. The use errors observed in these two tasks were caused by the participants’ inability to locate the required information on the screen, with the root cause being their unfamiliarity with the device.
In the ‘Patient Discharge’ scenario, the task for processing patient discharge achieved a 100% success rate.
3.3. SUS (System Usability Scale) Survey
The SUS survey was conducted with 22 ICU nurses who participated in the usability test. The results for each SUS item are shown in Table 6. The SUS score was 67.3 (95% CI 62.6–72.0), which corresponds to an “OK” level.
Odd-numbered items are interpreted as such that higher scores indicate greater user satisfaction. The items related to frequency of use (SUS 1) and ease of learning (SUS 7) received scores of 4.2 and 4.0. These results suggest that users are willing to use the system and can learn how to use it quickly. Even-numbered items are interpreted as such that lower scores indicate greater user satisfaction. The items related to system consistency (SUS 6) and system complexity (SUS 8) received relatively low scores of 2.2 and 2.3. These results indicate that the system is consistent and not overly complex to use.
3.4. Satisfaction Survey
A satisfaction survey was conducted with 22 ICU nurses who participated in the usability test. The results for each item of the satisfaction survey are shown in Table 7. The average score of the satisfaction survey was 4.5.
The average satisfaction scores for items 3 and 9, related to the cardiac arrest prediction function, were 4.2 and 4.3. These results indicate that participants were highly satisfied with the system’s ability to predict cardiac arrest. Participants’ feedback indicated that presenting the cardiac arrest prediction score as a numerical value enables intuitive monitoring, thereby increasing its perceived usefulness in clinical practice.
4. Discussion
This study performed a summative evaluation of a Central Monitoring System with AI-based Cardiac Arrest Prediction in a simulated environment with 22 ICU nurses to assess whether it can be used safely and effectively. ICUs are designed to provide treatment for critically ill patients, which makes rapid treatment essential, while nurses face high workloads as they must make rapid decisions in critical situations [12]. In addition, frequent alarms and the potential for use errors related to medical devices may affect patient safety, highlighting the need for systematic usability testing before introducing new devices into clinical settings [17,18,19]. The usability test included tasks based on the device workflow, the System Usability Scale (SUS) survey, and a satisfaction survey, and was performed in a simulated environment designed to resemble an ICU to reflect actual clinical environments.
The task success rate in the usability test was 90%, meeting the predefined goal. By scenario, the success rates were 89% for Basic Settings, 94% for Cardiac Arrest Prediction, 81% for Patient Review, and 100% for Patient Discharge. For critical tasks (Tasks 8, 9, and 12), success rates ranged from 73% to 100%. In contrast, Task 4, which involved setting the severity limit, had a success rate of 45%, falling below the goal of 70%. This low success rate was due to poor visibility of the setting button, highlighting a potential use error in a task. Addressing this design issue may improve task success in future device iterations. Additionally, Task 14, for reviewing patient alarm records, and Task 17, for checking the trend of cardiac arrest prediction scores, achieved success rates of 68% and 55%, respectively. These use errors were analyzed to have resulted from poor button visibility, difficulty locating required information on the screen, and participants’ unfamiliarity with the device, as observed during task performance.
The SUS score was 67.3, corresponding to an “OK” level [27], and the satisfaction survey showed an average of 4.5. These results indicate that participants generally found the system acceptable, while use errors arising from differences compared with previously used devices are expected to decrease through user training and continued use.
Although some usability failures were observed during the summative evaluation, their direct impact on patient safety could not be assessed within the simulated environment. Since this study was conducted in a simulated environment, further research is needed to evaluate the system’s effectiveness and user experience in a real clinical environment. Future studies should assess the actual incidence of cardiac arrest events, the time required to initiate interventions, and the extent to which the cardiac arrest prediction score contributes to clinical decision making and timely response. Such research would help clarify how effectively the system supports early detection of cardiac arrest risk and the timely initiation of interventions in a real clinical environment.
5. Conclusions
This study evaluated the usability of a Central Monitoring System with Cardiac Arrest Prediction through a usability test, SUS survey, and satisfaction survey. Some tasks showed lower performance due to design issues such as poor button visibility and unfamiliarity with the device, highlighting potential areas for design improvement. As the evaluation was performed in a simulated setting, further studies in real clinical environments are needed to assess effectiveness, user experience, and the system’s contribution to timely detection of cardiac arrest events.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lee H. Yang H.L. Ryu H.G. Jung C.W. Cho Y.J. Yoon S.B. Yoon H.K. Lee H.C. Real-Time Machine Learning Model to Predict in-Hospital Cardiac Arrest Using Heart Rate Variability in IC Unpj Digit. Med.2023621510.1038/s 41746-023-00960-237993540 PMC 10665411 · doi ↗ · pubmed ↗
- 2Armstrong R.A. Kane C. Oglesby F. Barnard K. Soar J. Thomas M. The Incidence of Cardiac Arrest in the Intensive Care Unit: A Systematic Review and Meta-Analysis J. Intensive Care Soc.20192014415410.1177/175114371877471331037107 PMC 6475987 · doi ↗ · pubmed ↗
- 3Kwon J.M. Kim K.H. Jeon K.H. Lee S.Y. Park J. Oh B.H. Artificial Intelligence Algorithm for Predicting Cardiac Arrest Using Electrocardiography Scand. J. Trauma Resusc. Emerg. Med.2020289810.1186/s 13049-020-00791-033023615 PMC 7541213 · doi ↗ · pubmed ↗
- 4Hillman K.M. Bristow P.J. Chey T. Daffurn K. Jacques T. Norman S.L. Bishop G.F. Simmons G. Duration of Life-Threatening Antecedents Prior to Intensive Care Admission Intensive Care Med.2002281629163410.1007/s 00134-002-1496-y 12415452 · doi ↗ · pubmed ↗
- 5Elvekjaer M. Aasvang E.K. Olsen R.M. Sørensen H.B.D. Porsbjerg C.M. Jensen J.U. Haahr-Raunkjær C. Meyhoff C.S. Physiological Abnormalities in Patients Admitted with Acute Exacerbation of COPD: An Observational Study with Continuous Monitoring J. Clin. Monit. Comput.2020341051106010.1007/s 10877-019-00415-831713013 · doi ↗ · pubmed ↗
- 6Lee A. Bishop G. Hillman K.M. Daffurn K. The Medical Emergency Team Anaesth. Intensive Care 19952318318610.1177/0310057 X 95023002107793590 · doi ↗ · pubmed ↗
- 7Smith G.B. Osgood V.M. Crane S. ALERT—A Multiprofessional Training Course in the Care of the Acutely Ill Adult Patient Resuscitation 20025228128610.1016/S 0300-9572(01)00477-411886734 · doi ↗ · pubmed ↗
- 8Shin Y. Cho K.-j. Chang M. Youk H. Kim Y.J. Park J.Y. Yoo D. The Development and Validation of a Novel Deep-Learning Algorithm to Predict in-Hospital Cardiac Arrest in ED-ICU (Emergency Department-Based Intensive Care Units): A Single Center Retrospective Cohort Study Signa Vitae 202420839810.22514/sv.2024.045 · doi ↗