Investigating the Inflammatory Link Between Vitamin D and Hidradenitis Suppurativa: A Systematic Review and Causal Inference Analysis
Jasmine Spiteri, Laura Grech, Dillon Mintoff, Nikolai P. Pace

TL;DR
This study explores the relationship between vitamin D levels and hidradenitis suppurativa, finding that low vitamin D is likely a marker of inflammation rather than a cause.
Contribution
The study uses Mendelian randomization to investigate causality, finding no direct causal link between vitamin D and HS.
Findings
Low vitamin D levels are common in HS patients and correlate with disease severity and inflammation.
Mendelian randomization found no causal effect of vitamin D on HS risk.
Vitamin D supplementation improves clinical outcomes, suggesting potential therapeutic value.
Abstract
An inverse correlation between serum vitamin D levels and hidradenitis suppurativa (HS) severity is frequently reported, yet the causal nature and direction of this association remain unresolved. A systematic review was conducted following PRISMA guidelines, identifying 12 relevant studies. A two-sample Mendelian randomization (MR) analysis using the inverse-variance weighted (IVW) method was subsequently performed using genetic instruments for vitamin D from the UK Biobank (n = 417,580) and HS summary statistics from FinnGen (n = 1420). The systematic review confirmed a high prevalence of vitamin D deficiency (<20 ng mL−1) among HS patients (weighted mean 17.90 ng mL−1) and identified inverse correlations between vitamin D levels and disease severity, active lesions, and C-reactive protein (CRP), while supplementation improved clinical outcomes. A null MR estimate consistent with the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
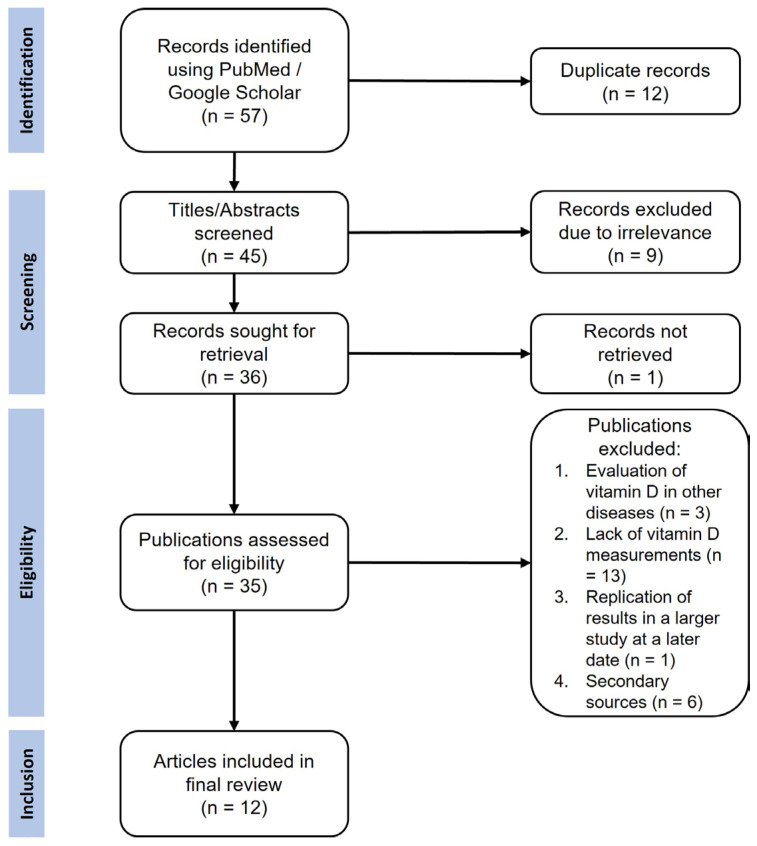 Figure 1
Figure 1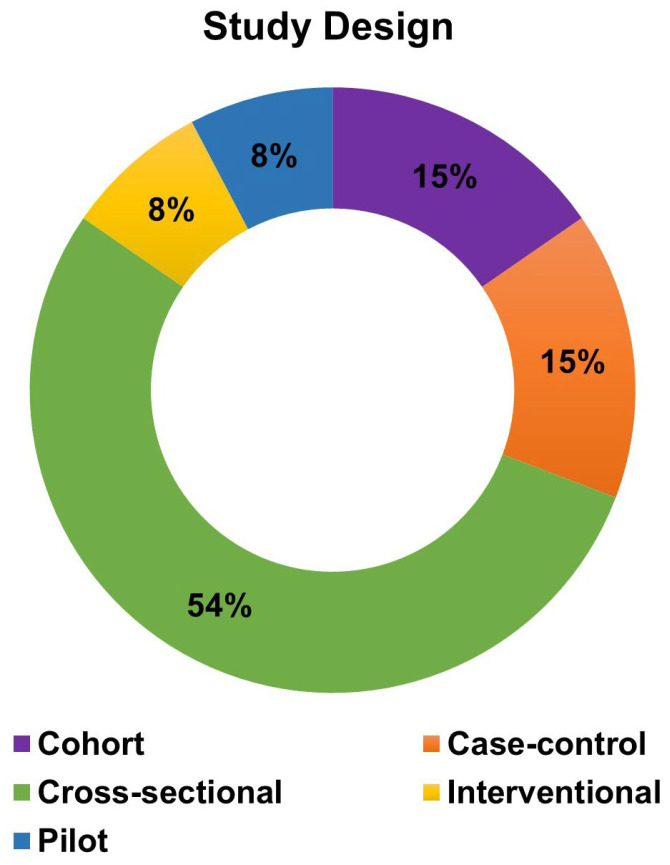 Figure 2
Figure 2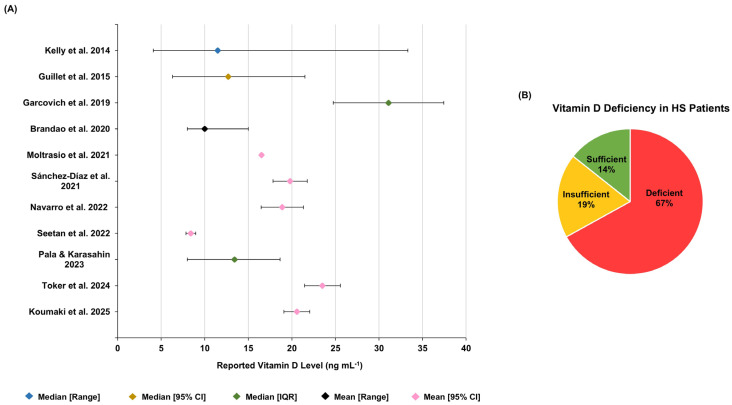 Figure 3
Figure 3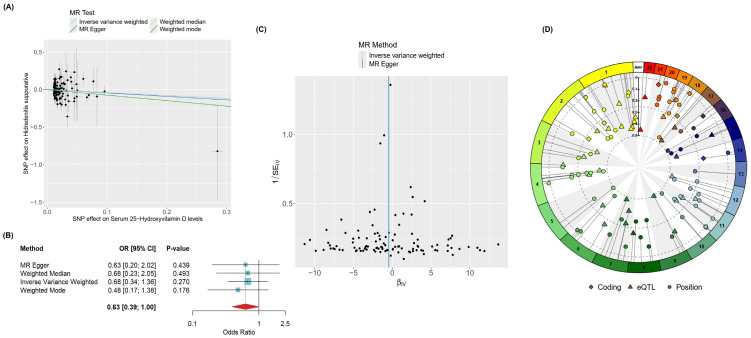 Figure 4
Figure 4- —Tertiary Education Scholarships Scheme (Malta)
- —HS-FUNOMICS
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHidradenitis Suppurativa and Treatments · Acne and Rosacea Treatments and Effects · Dermatological and COVID-19 studies
1. Introduction
Vitamin D is a secosteroid prohormone involved in numerous biological processes [1,2]. Following UV-dependent synthesis from 7-dehydrocholesterol in keratinocytes or uptake from dietary sources, vitamin D undergoes sequential hydroxylation (first at C25 in the liver yielding 25-hydroxyvitamin D (25(OH)D) and subsequently (but not exclusively) in the kidney to form its active metabolite, 1α,25-dihydroxyvitamin D (1,25(OH)_2_D)) [3,4,5]. The latter circulates to target tissues where it binds to vitamin D receptor (VDR)—a ligand-dependent transcription factor of the nuclear receptor superfamily. Upon ligand binding, VDR heterodimerizes with retinoid X receptor (RXR) isotypes and recruits coactivators and co-repressors to regulate the transcription of Vitamin D-response genes [2,4].
Beyond its well-established role as a key regulator of calcium and phosphate homeostasis, vitamin D exerts pleiotropic effects across a wide range of biological processes, having complex immunoregulatory, cell growth and differentiation, and cardiovascular functions. The endocrine effects of the 1,25(OH)_2_D-VDR interaction in different cells, include lipid and phosphate absorption in intestinal enterocytes, cell cycle regulation, and regulation of immune responses. Furthermore, the conversion to active 1,25(OH)_2_D can occur extra-renally in epithelial and immune cells, enabling paracrine and autocrine signaling [1,2,4].
Vitamin D signaling serves as a regulator of both innate and adaptive immunity. Its immunomodulatory effects include enhancing the innate antibacterial response via the induction of the anti-microbial peptide cathelicidin in monocytes and macrophages. Simultaneously, it promotes a more tolerogenic immune state by steering dendritic cell differentiation towards a phenotype that favors anti-inflammatory interleukin (IL) 10 secretion, while directly suppressing the production of pro-inflammatory cytokines like IL-17 and interferon (IFN) γ in T cells. These mechanisms enhance antimicrobial defense and help maintain immune tolerance, thereby reducing the risk of autoimmunity [1,4]. The clinical relevance of this immunoregulatory role is evident in several autoimmune and chronic inflammatory conditions, including familial Mediterranean fever (FMF) [6,7,8,9], rheumatoid arthritis (RA), axial spondyloarthritis [10,11,12,13,14], and inflammatory bowel disease (IBD) [15,16,17]. In these diseases, hypovitaminosis D is not only more prevalent than in healthy controls but also frequently correlates with increased disease severity and elevated levels of proinflammatory cytokines.
Beyond its systemic immunomodulatory effects, vitamin D signaling is a regulator of cutaneous homeostasis. In the skin, the 1,25(OH)_2_D-VDR complex suppresses keratinocyte hyperproliferation and promotes their normal differentiation and the formation of the protective cornified envelope. Furthermore, it regulates hair follicle cycling through its interaction with the hairless co-repressor [4,18]. Disruption of these processes—epidermal barrier integrity, cell growth, and follicular function—provides a direct pathophysiological link between impaired vitamin D signaling and the development of chronic inflammatory skin conditions, such as psoriasis, atopic dermatitis (AD), acne vulgaris (AV), and hidradenitis suppurativa (HS) [5]. Evidence of this link is provided via meta-analytical studies that consistently report lower vitamin D levels in patients with psoriasis [19,20,21], AD [22,23,24] and AV [25,26,27] across different ages, which are negatively correlated with disease severity.
Hidradenitis suppurativa (HS) is a chronic inflammatory disease of the pilosebaceous unit that primarily affects apocrine gland-bearing regions, particularly the axillary, gluteal, and genital areas. It manifests with recurrent painful nodules that may progress into abscesses, sinus tracts, and scarring [28,29]. The etiology of HS, although incompletely understood, involves dysregulated immune responses, disruption of epidermal barrier function, cutaneous dysbiosis, and metabolic alterations as a result of the interaction between genetic and environmental factors [30].
Emerging epidemiological and clinical evidence supports a link between vitamin D deficiency and HS presentation and course. Multiple studies report an inverse association between hypovitaminosis D and HS disease severity [29,30,31,32,33,34,35]. Hypovitaminosis D has been associated with the presence of active lesions, increased levels of C-reactive protein (CRP), the co-occurrence of Crohn’s disease, and non-familial HS [29,30,32,34]. These relationships appear to be clinically relevant as continuous supplementation with vitamin D (ranging from 25,000 to 100,000 IU monthly according to the patients’ insufficiency/deficiency level) was shown to significantly improve the response to standard topical/systemic therapies as well as decrease the number of active nodules [29,31]. Nevertheless, the observational nature of these studies leaves the causal relationship between vitamin D and HS unresolved. It remains unknown whether hypovitaminosis D contributes to HS pathogenesis or if the inflammatory burden of HS leads to hypovitaminosis D.
Against this background, the present study aimed to systematically investigate the role of vitamin D in HS by: (1) reviewing and synthesizing published reports of serum vitamin D levels across different HS phenotypes and their association with demographic and clinical variables; (2) performing a two-sample Mendelian randomization (MR) analysis to determine the causal direction of the observed association; and (3) discussing the potential pathophysiological pathways linking vitamin D to HS by integrating evidence from other autoinflammatory conditions.
2. Materials and Methods
The study selection process followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, as detailed in Figure 1.
2.1. Study Selection and Inclusion Criteria
An electronic literature search was conducted to identify English-language studies investigating the relationship between vitamin D and HS. This search was conducted in the PubMed/MEDLINE and Google Scholar databases. The following combination of free text keywords and Medical Subject Headings terms was used for this search: “hidradenitis suppurativa”, “acne inversa”, “Verneuil’s disease”, “vitamin D”, and “25OHD”, together with the Boolean terms “AND” and “OR”. Original articles published between January 2014 and August 2025 that directly investigated the role of vitamin D in HS patients were considered eligible for inclusion. Studies that were not identified via the database search were selected through citation review and handsearching based on relevance.
2.2. Exclusion Criteria
Studies were excluded if they: (1) reported vitamin D levels in relation to conditions other than HS, (2) reported only observed effects of vitamin D supplementation or diet alterations in HS patients without vitamin D measurement, and (3) were conference proceedings, reviews, comments or editorial letters.
2.3. Data Extraction
Titles and abstracts were screened against the inclusion and exclusion criteria. Any discrepancies were resolved by consensus of the investigators. The following information was extracted from the selected articles: (1) study design, (2) measured metabolite of vitamin D and assay methodology, (3) HS phenotype, (4) patient demographic and clinical data, (5) any treatment or supplementation taken, (6) control group size (where relevant), and (7) main outcomes of the study specifically related to vitamin D.
Methodological quality of the included studies was appraised using the Mixed Methods Appraisal Tool (MMAT, version 2018), with study design-specific criteria applied to quantitative non-randomized and quantitative descriptive studies [36]. Rather than assigning an overall numeric score, we used the MMAT to identify recurrent sources of potential bias and methodological limitations relevant to interpretation of the evidence base.
2.4. Data Analysis
Study and patient characteristics were summarized descriptively using tables and plots. Categorical variables (sex, smoking status, and disease severity) are presented as percentages. For quantitative variables (age and BMI), a weighted mean ± weighted standard deviation was calculated, using the sample size of each individual study as the weight. This approach was applied to provide a more accurate aggregate estimate, as it assigns greater influence to studies with larger sample sizes, which are presumed to offer more precise parameter estimates.
To enable cross-study comparability, serum vitamin D levels reported in nmol L^−1^ were converted to ng mL^−1^ using the conversion factor of 2.5 (i.e., ng mL^−1^ = nmol L^−1^ ÷ 2.5). For studies reporting mean vitamin D levels with a standard deviation, the 95% confidence interval was calculated and used as the error bars in the forest plot to visually represent the precision of each study’s estimate Vitamin D deficiency/insufficiency categories were extracted as reported in the original studies, because threshold definitions varied (for example, <10, <20, and <30 ng/mL). Additionally, study-level reporting was insufficient for consistent reclassification thus no post hoc standardisation of categorical prevalence estimates was performed. Cross-study summaries of categorical vitamin D status were treated as descriptive and interpreted with caution [31]. A quantitative meta-analysis was not performed because serum vitamin D outcomes were reported using heterogeneous summary measures (for example, means with standard deviations or confidence intervals, and medians with ranges or interquartile ranges), and the parameters required to derive comparable effect estimates and variances were inconsistently available. In addition, individual participant data were unavailable and, in some studies, the measured vitamin D metabolite and/or assay methodology was not clearly specified, precluding reliable pooling across studies.
2.5. Mendelian Randomization Analysis
The two-sample MR analysis was performed using summary-level data from GWAS of European ancestry subjects. Genetic instruments for serum vitamin D levels (the exposure) were obtained from the UK Biobank (dataset ID: ebi-a-GCST90000617; n = 417,580) [37]. Summary statistics for hidradenitis suppurativa (the outcome) were sourced from the FinnGen Biobank (dataset ID: finn-b-L12_HIDRADENITISSUP; n = 1420) [38]. The analysis was performed via the MR analysis two-sample Mendelian randomization R (version 4.5.1) shiny application (MRanalysis version 2.0.0), which uses the TwoSampleMR and MRPRESSO packages [39].
SNPs associated with vitamin D levels at genome-wide significance (p < 5 × 10^−8^) were selected as instrumental variables (IVs). To ensure genetic independence, linkage disequilibrium (LD) clumping was performed using a strict threshold (r^2^ < 0.001) within a 10,000 kb window. SNPs with an F-statistic greater than 10 were retained to ensure strong instrument strength and mitigate potential weak instrument bias.
The primary causal estimate was derived using the IVW method. To assess the robustness of this result, we performed sensitivity analyses using the MR-Egger, weighted median, and weighted mode methods. We evaluated the validity of the model assumptions by: (1) calculating Cochran’s Q statistic to test for heterogeneity among the instrumental variable estimates; (2) applying the MR-Egger intercept test and the MR-PRESSO global test (with its leave-one-out analysis) to detect and adjust for potential horizontal pleiotropy. Variant-gene mapping of the SNPs selected as instrumental variables was carried out using snpXplorer and presented as a Circos plot [40].
3. Results
3.1. Study Characteristics
The literature search identified 35 studies investigating the role of vitamin D in HS. Following the exclusion of studies involving other skin diseases (n = 3), descriptive studies investigating the role of diet and vitamin D supplementation without measurements in patients (n = 13), superseded studies that were later replicated in larger cohorts (n = 1), and review articles (n = 6), 12 primary studies were included for analysis (Table S1) [29,30,31,32,33,34,35,41,42,43,44,45]. The number of HS patients per study ranged from 5 to 250 (N_total_ = 956), with the majority of studies being cross-sectional and including patients with varying clinical phenotypes (Figure 2). Four studies have investigated the role of vitamin D in specific HS subpopulations, namely HS patients who have undergone bariatric surgery [41], patients with syndromic HS (Pyoderma gangrenosum, Acne, Suppurative Hidradenitis/PASH and Pyogenic Arthritis, Acne, Pyoderma gangrenosum, Suppurative Hidradenitis/PAPASH syndromes) [42], patients refractory to topical or systemic HS therapies [31], and patients diagnosed with severe HS (according to the Hurley stage and International Hidradenitis Suppurativa Severity Score System/IHS4) who are candidates for biologic therapy [43].
Among the studies that specified the methodology (n = 8), serum vitamin D was exclusively measured as 25-hydroxyvitamin D (25(OH)D). Electrochemiluminescence was the most common assay (n = 6), followed by chemiluminescence and enzyme-linked immunosorbent assay/ELISA (each n = 1). The remaining four studies, which were retrospective chart reviews or genomic analyses, did not specify the analyte measured and the assay used.
Demographic and clinical data were inconsistently reported across studies, with noticeable underreporting of ethnicity, the age of HS onset, disease duration, family history of HS, and the anatomical sites involved. Across the included cohorts, HS patients were predominantly adult females (mean age: 36.9 ± 4.8 years), active smokers, and with body mass indices in the obese range (mean body mass index/BMI ≥ 30 kg m^−2^) (Table 1). Most patients had moderate-severe disease (64%—combined value based on Hurley stage/IHS4/Hidradenitis Suppurativa Physician Global Assessment (HS-PGA) scoring systems), likely reflecting sampling in secondary care settings. The majority were receiving standard topical and systemic therapies for HS but had not received vitamin D supplementation for at least 6 months prior to assessment.
Information about control groups was limited. Most studies reported the inclusion of sex- and age-matched controls while only two studies accounted for smoking status and BMI. In the cohort study by Garcovich et al. (2019), HS patients without a history of bariatric surgery and exhibiting typical disease manifestations were selected as controls (according to the classification systems by Canoui-Poitrine et al. (2013) and van der Zee et al. (2015) [41,46,47]).
Structured appraisal using the Mixed Methods Appraisal Tool (MMAT) indicated that most included studies met the majority of design-specific quality criteria, particularly regarding the appropriateness of vitamin D-related measurements and the use of suitable statistical analyses for the study design (Table S2 Part I,II). Potential selection bias (single-center, retrospective, severe HS cohorts), variable control of confounding (BMI, smoking, adiposity/metabolic factors, and comorbidities), and the predominance of cross-sectional designs which limit temporal and causal inference, were identified.
3.2. Serum Vitamin D Level and Correlation Studies
A total of 11 studies reported mean or median serum vitamin D levels in patients with HS. Across these studies, the reported central tendency values were descriptively aggregated, yielding an overall weighted mean of 17.90 ± 20.34 ng mL^−1^. This summary should be interpreted cautiously in light of substantial between-study heterogeneity in reporting format (mean versus median), dispersion metrics, and study design. Overall, serum vitamin D levels were consistently low across HS cohorts, and multiple studies reported a high frequency of vitamin D deficiency (Figure 3A,B).
Categorical vitamin D status was defined using non-uniform thresholds, with variable criteria for deficiency/sufficiency across studies. For this reason, category counts and proportions were retained according to each study’s original cut-off definitions and presented as a descriptive summary rather than directly comparable prevalence estimates to preserve fidelity to the source data and avoid introducing additional bias through post hoc reclassification. Despite these discrepancies, in the study by Koumaki et al. (2025), (where a sufficiency threshold of 20 ng mL^−1^ was applied resulting in a greater proportion of patients being classified as sufficient relative to studies using higher thresholds), the mean vitamin D level in their HS cohort remained significantly lower than in controls, consistent with the findings of four other studies [29,30,34,44,45]. The genetic landscape of syndromic HS, particularly in PASH and PAPASH phenotypes, further implicates vitamin D metabolism as a key disrupted pathway. Brandao et al. (2020) report a whole-exome sequencing study of PASH and PAPASH patients [42]. They show that approximately 45% of genes involved in vitamin D metabolism carry deleterious variants, which may significantly impair pathway functionality [42]. These genetic findings are corroborated by the consistent finding of low serum vitamin D levels, suggesting that dysregulated vitamin D signaling may also contribute to the shared pathophysiology of syndromic HS. These observations position vitamin D not merely as a nutritional correlate but as a component of a dysregulated metabolic and immunomodulatory axis in these severe, autoinflammatory forms of the disease.
Furthermore, a reduction in the number of nodules and improved response to HS therapeutics following 6 months of vitamin D supplementation, has been reported in intervention studies [29,31]. Despite the significant decrease in vitamin D levels in patients that discontinued supplementation after month 3, a statistically significant negative correlation between the number of lesions and vitamin D was observed at month 6. Additionally, the number of flare-ups was also noted to decrease after the supplementation period, highlighting the clinical relevance of vitamin D [29].
Analysis of phenotypic correlation yielded conflicting results, with some studies reporting a significant negative correlation between vitamin D levels and HS severity [30,31,32,33,34,43], and others noting no significant association between the 2 variables [29,44,45]. The presence of active lesions irrespective of anatomical site was also correlated with lower vitamin D levels [30]. Other variables, including CRP, smoking status, and BMI have also been negatively correlated with the difference in vitamin D levels in HS patients as well as the patients’ sex [32,45], but the results were not replicated by other studies [34,35]. Additionally, bariatric surgery did not influence vitamin D levels or the frequency of hypovitaminosis D in HS patients [41].
3.3. MR Analysis
Given the observational nature of the findings identified in the systematic review, we employed a two-sample Mendelian randomization (MR) analysis to assess causality. This method leverages genetically predisposed variation in 25(OH)D levels to infer causal relationships, largely free from reverse causation and confounding. A total of 106 instrumental variables (IVs) were included in the MR analysis. Inverse-variance weighted (IVW) analysis does not support a linear causal effect of genetically predicted 25(OH)D on HS (β = −0.390, SE = 0.35, p = 0.270). Concordant results were obtained using other MR methods, as shown in Figure 4A,B. This does not exclude the possibility of non-linear, threshold-dependent, context-specific, or mediated effects that were not evaluated in the present study.
Sensitivity analyses were conducted to assess the robustness and validity of the MR findings. Cochran’s Q statistic indicated no significant heterogeneity among the variant-specific estimates (Q_IVW_ = 126.45, degrees of freedom = 105, p_IVW_ = 0.078), supporting the consistency of the genetic instruments. Furthermore, tests for horizontal pleiotropy were non-significant. Both the MR-PRESSO global test (p = 0.076) and the MR-Egger intercept test (p = 0.880) found no strong statistical evidence of pleiotropic bias. It is noteworthy, however, that the funnel plot (Figure 4C) showed an asymmetry concentrated among weaker genetic instruments, a pattern that can sometimes indicate undetected pleiotropy; nevertheless, the formal statistical tests did not confirm this.
The genetic architecture of the instrumental variables was further characterized through variant-to-gene mapping (Figure 4D). This analysis revealed that a relatively small proportion of the vitamin D-associated single nucleotide polymorphisms (SNPs) were linked to protein-coding genes, a pattern that typifies findings from genome-wide association studies (GWAS), where many trait-associated variants reside in non-coding regions such as introns or intergenic regulatory elements. This underscores the requirement for fine mapping of GWAS-identified loci to distinguish causal regulatory signals and thereby elucidate the specific biological pathways involved.
The instrumental variables demonstrated a wide genomic distribution across multiple chromosomes. This dispersion is methodologically favorable, as it reduces the likelihood of linkage disequilibrium between variants and supports the key MR assumption of genetic independence, thereby strengthening the validity of our causal inference.
An assessment of reverse causality, i.e., whether HS itself influences vitamin D levels, was not feasible. This analysis was precluded by the relatively limited sample size of the HS GWAS and the consequent lack of sufficiently strong genetic instruments to robustly test this reverse direction.
4. Discussion
In this study, we reconcile the well-established observational association between low vitamin D levels and HS, with MR findings that do not support a detectable linear causal effect of genetically predicted 25(OH)D levels on disease risk. Importantly, this inference is specific to the causal model tested, namely the average linear effect of lifelong genetically influenced 25(OH)D variation in a predominantly European-ancestry context, and should not be interpreted as excluding all possible causal involvement of vitamin D in HS. Rather, the findings suggest that, within this analytical framework, hypovitaminosis D may function more often as a correlate of disease phenotype, comorbidity burden, and/or shared determinants (including confounding or mediating factors), rather than as a primary etiological driver. Additionally, the estimated effect may not be directly transferable to non-European populations, where differences in allele frequencies, linkage disequilibrium structure, vitamin D distributions, and HS risk determinants could alter both instrument performance and causal estimates. Similar discrepancies between observational and genetic associations have been reported in cardiovascular disorders and inflammatory bowel disease, where the observational signal has likewise been interpreted cautiously in light of confounding, reverse causation, mediation, or non-linear/context-dependent effects [48,49,50,51].
Despite inconsistencies among MR analyses, several studies have reported inverse associations between vitamin D levels and the risk of cardiometabolic and autoimmune diseases, including hypertension, coronary heart disease, type 2 diabetes, obesity, multiple sclerosis, psoriasis, and systemic lupus erythematosus [51,52,53,54,55,56,57,58]. Several of these metabolic conditions, particularly obesity, have been linked to the development of HS, that in turn increase the risk of CVDs and metabolic syndrome in HS patients [59,60,61]. Hence, the MR studies between vitamin D and these disorders suggest a role for vitamin D in HS pathophysiology. Moreover, studies leveraging GWAS data have identified variants related to human leukocyte antigen class II molecules, which are invariably associated with autoimmune conditions and therefore imply that HS may also have an autoimmune etiology [62,63]. Thus, the involvement of vitamin D in HS merits further discussion.
4.1. Patient Characteristics Associated with Vitamin D
Across the reviewed studies, most HS patients were females, overweight and smokers—characteristics of the typical HS phenotype that also tend to associate with increased risk of hypovitaminosis D.
The inverse relationship between BMI or adiposity and vitamin D has been reported in several observational and MR studies [41,64,65,66,67,68]. Although individuals with a higher body surface area theoretically have a greater potential for UV-mediated 7-dehydrocholesterol photosynthesis, individuals with obesity tend to be less exposed to the sun due to the reduced outdoor activity and the use of clothing habits that cover more skin [65,66]. This tendency may be accentuated in individuals with HS, who may limit sun exposure due to visible lesions.
Apart from UVB exposure, other physiological factors influencing vitamin D levels in individuals with obesity include: (1) the increased sequestration of the lipid-soluble vitamin D in adipose tissue, (2) lower production of 25-hydroxylase due to CYP2R1 downregulation and thus reduced formation of 25(OH)D, (3) enhanced hydroxylation of 25(OH)D in response to intact parathyroid hormone (iPTH) stimulation, and (4) VDR and vitamin D binding protein (DBP) gene polymorphisms [64,65,66,68,69,70]. The inverse causal relationship, i.e., vitamin D as a determinant of obesity could not be confirmed, mainly due to its role in the inhibition of adipogenesis and reduced accumulation of triglycerides, adipocyte apoptosis via activation of Ca^2+^-dependent signaling, regulation of lipogenesis and lipolysis, and reduction in insulin resistance [66,69,70,71,72].
Obesity and vitamin D deficiency also tend to be more prevalent in females. The significantly higher lipid levels in women have been attributed to the inhibition of HMG-CoA reductase activity by estrogen [68]. Coupled with the increased concentration of DBP and/or expression of VDR as well as the upregulated hepatic hydroxylation of vitamin D, this results in the reduced availability of biologically active vitamin [68,73,74,75,76]. Nonetheless, the results vary between studies and associations between vitamin D and testosterone have also been described, suggesting that other factors (ethnicity, diet, and health awareness) may be responsible for the discrepancy [77,78,79,80,81].
Hypovitaminosis D is also prominent in both active and passive smokers, showing decreased levels of 25(OH)D and its active metabolite 1,25(OH)_2_D. It has been suggested that the inhibition of parathyroid hormone (PTH) by smoking leads to vitamin D deficiency due to nicotine-induced hypoparathyroidism [82,83]. More research is required into the influence of smoking on vitamin D but several processes have been implicated, including: (1) impaired 1-α-hydroxylation in the kidneys, (2) increased activity of liver enzymes, (3) direct alteration of vitamin D catabolism, or (4) damage or delayed skin healing due to enhanced expression of cyclooxygenase 2 and inducible nitric oxide synthase [82,84,85,86].
Taken together, these findings suggest that vitamin D deficiency in patients with HS may largely reflect shared lifestyle with physiological characteristics rather than being disease-specific. While variation in sun exposure, BMI and smoking may exacerbate these differences, HS itself may not be a primary determinant of hypovitaminosis D.
4.2. Plausible Mechanistic Pathways Linking Vitamin D and Hidradenitis Suppurativa
While direct mechanistic evidence linking vitamin D to HS remains limited, existing immunologic and epithelial biology supports several plausible hypotheses. In particular, vitamin D may influence HS-relevant processes involving IL-1β/T_H_17 signaling, innate immune sensing (including NOD2-related pathways), and follicular differentiation networks. We next review potential mechanistic hypotheses linking vitamin D status to HS-relevant immune and epithelial processes.
Although the influence of sex or smoking status on HS risk remains uncertain, obesity is a well-established predisposing factor. Excess weight exacerbates HS not only through mechanical friction but also through meta-inflammation driven by adipocyte hypertrophy and macrophage infiltration, resulting in increased IL-1β, IL-6, IL-8, tumor necrosis factor (TNF) α levels via toll-like receptor (TLR) mediated NF-κB activation [69,70,73,87,88,89,90]. Both 25(OH)D and 1,25(OH)_2_D have been shown to attenuate these inflammatory pathways, reducing TNF-α and IL-6 expression in adipose tissue [73,87]. This suggests that vitamin D supplementation might hinder the inflammatory response in individuals with HS and obesity and that inflammatory mediators may be involved in the observed relationship between vitamin D and other HS phenotypes.
Parallels are provided from studies investigating the role of vitamin D in other inflammatory diseases such as rheumatological and dermatological conditions which share pathogenic pathways with HS. In psoriatic plaques and AV inflammatory lesions, treatment with vitamin D or its analogues resulted in reduced T_H_17-mediated immunity in keratinocytes via inhibition of T-cell recruitment and NF-κB signaling [91,92,93]. Similar observations were also made in patients with RA, where low levels of vitamin D are associated with increased formation of reactive oxygen species (ROS) that ultimately activates NF-κB and elevates the T_H_17-related cytokine IL-21 [14]. Despite the lack of a dominant T_H_ axis in HS, IL-17 signaling is a major contributor to the development of the inflammatory cascade, through immune cell infiltration of both uninvolved and lesional skin and the upregulation of antimicrobial peptides (AMPs) like psoriasin [94,95,96,97,98]. The development of T_H_17 cells and hence release of IL-17 cytokine is enhanced by the increased levels of the upstream regulator IL-1β [98,99]. This has also been targeted by topical vitamin D treatment in acne vulgaris, suggesting that vitamin D treatment could mitigate the pro-inflammatory milieu resulting from the IL-1β-T_H_17 cell cytokine axis in HS [100]. Other pro-inflammatory markers such as IFN-γ and TNF-α, which are also upregulated in HS patients and associated with keratinocyte hyperproliferation, have also been downregulated in AD and IBD most likely through VDR signaling [97,101,102,103,104,105]. Additionally, an increase in AMPs, such as psoriasin (S100A7) and cathelicidin (LL-37) in keratinocytes and sebocytes was also noted in psoriasis and AV [91,92,93]. The keratinocytic induction of cathelicidin in response to vitamin D as opposed to its release from neutrophils in HS patients, would prevent microbial infections of lesional skin without aggravating inflammation [91,106]. Vitamin D may thus influence inflammatory pathways relevant to HS through effects on innate and adaptive immune responses, although direct HS-specific mechanistic evidence remains limited.
Conversely, vitamin D positively regulates Notch signaling in the intestinal barrier, preserving the integrity of tight junctions [107]. Differentially expressed genes related to the Notch pathway that are regulated by VDR have also been identified in HS lesions, but enhanced Notch signaling has been associated with keratinocyte hyperproliferation and innate immunity activation which would lead to inflammation [108,109]. Similarly, 1,25(OH)_2_D stimulates the pathogen-recognition receptor NOD2 in IBD, triggering inflammation and innate immunity dysregulation. NOD2 has also been identified in the HS inflammasome, particularly in syndromic HS, and thus treatment with vitamin D could exacerbate inflammation [110,111,112]. Plausibly, NOD2-linked innate immune dysregulation represents a potential pathway for vitamin D-related inflammatory variation in HS, but this remains speculative and hypothesis-generating.
The metabolite 1,25(OH)_2_D has also been associated with hair follicle cycle regulation. This involves shortening of the anagen phase potentially through the Wnt/β-catenin pathway to promote hair regeneration and enhancing proliferation and migration of follicular cells [113]. These processes are VDR-dependent and likely involve downregulation of the HIF-1α and NLRP3, both being overexpressed in HS patients [113,114,115]. Since HIF-1α promotes glycolytic metabolism, angiogenesis and IL-1β/IL-17 [114], and NLRP3 mediates IL-1β and IL-18 maturation, vitamin D-mediated suppression of these factors may mitigate inflammation and follicular occlusion, the hallmarks of HS pathogenesis [98,113,114,115]. Nonetheless, these mechanistic pathways should be interpreted as hypothesis-generating models that may help contextualize the observed clinical associations between vitamin D status and HS, rather than as directly causal mechanisms.
The observed clinical improvements in HS (reduction in the number of nodules and frequency of flare-ups, and enhanced response to therapy following vitamin D supplementation) collectively support a modulatory rather than causal role for Vitamin D in HS [29,31]. However, further interventional trials are warranted to determine the usefulness, dosage and formulation of vitamin D as an adjuvant therapeutic in the management of HS.
4.3. Methodological Variations in Serum Vitamin D Measurements
The measurement of the same metabolite (25(OH)D) in at least 8 of the reviewed studies using similar analysis methods, yielded different mean values of vitamin D even in patient groups of similar ethnicities. Aside from methodological limitations (variability in sample size and patient demographic/clinical characteristics), other confounding factors may be implicated. These include factors involving UVB exposure such as melanin pigmentation or religious customs, changes in 7-dehydrocholesterol levels with age, gene polymorphisms, liver/kidney disease, and interfering medication [29,30,45,116]. Numerous articles have reviewed the issues related to vitamin D measurements, not only those pertaining to physiological aspects, but also inter-laboratory and inter-assay variations [116,117,118].
From a laboratory perspective, the accurate quantification of vitamin D status is hampered by significant methodological heterogeneity. Commonly employed immunoassays are susceptible to variable cross-reactivity with different vitamin D metabolites and epimers which have differing affinity constants to binding proteins. Additionally, these assays are biased by sample matrix interference, particularly in the presence of lipids. Despite the increased specificity of chromatographic methods, their application is limited to research purposes while clinical settings favor automated and rapid immunoassays [116,118,119,120]. The lack of agreement on the utilized assay influences the interpretation of serum 25(OH)D levels across studies, particularly in cases where cut-off values are specified according to the kit used or a specific condition (usually musculoskeletal) being studied, without taking into consideration the different roles of vitamin D and general health [118,121,122]. Furthermore, the sole reliance on total 25(OH)D as a biomarker is potentially limiting, as it does not reflect the bioavailable fraction or the influence of other relevant metabolites whose concentrations may be differentially detected by various assays. [118,121,123]. The measurement of active free metabolites may thus inform the definition of the physiological ranges of vitamin D, provided methods are developed to accurately measure these unstable molecules. The absence of measurements of additional laboratory parameters, such as serum PTH, in most clinical cohorts presents an additional limitation, as the PTH-25(OH)D relationship is a key dynamic regulator of calcium homeostasis and its omission prevents a more integrated physiological assessment of functional vitamin D status [124]. This data would help inform more holistic guidelines that take into consideration the broader role and benefits of vitamin D beyond bone health, as well as variations in its metabolism in different individuals, to ensure adequate dosaging [125,126].
These limitations can greatly impact the outcomes of the studies included in this review, as shown through their conflicting correlation analyses. Furthermore, the influence of these confounding factors indicates that the use of genetic instruments in a linear MR analysis may not be representative of the true biological association between serum 25(OH)D and HS. The non-linear relationship between vitamin D and other biomarkers suggests that applying a stratified, non-linear MR model or the application of mediation analysis could better explain the role of vitamin D in HS. Other limitations include: (1) the GWAS data is based on European participants and therefore the results cannot be extrapolated to other populations; (2) residual bias cannot be excluded since the exact biological function of the IVs is not known; (3) canalization or compensatory developmental processes may dampen the effect of genetically dysregulated 25(OH)D, favoring a null result. Additional limitations merit consideration. Primarily, no formal meta-analysis of serum vitamin D levels was performed due to substantial methodological and reporting heterogeneity across studies, incomplete variance data, and inconsistent specification of the vitamin D analyte/assay in some reports. These factors limit validity and interpretability of a pooled estimate. Furthermore, the reported heterogeneity in vitamin D threshold definitions across studies introduces potential classification bias and constrains direct comparison of deficiency/insufficiency prevalence. In the absence of sufficiently granular published data, post hoc harmonization of categories was not consistently possible. The observational evidence base is also subject to methodological limitations identified on MMAT appraisal including potential selection bias, inconsistent adjustment for important confounders (notably BMI and smoking), and predominantly cross-sectional study designs, all of which may influence the observed association between vitamin D status and HS.
5. Conclusions
Overall, the low vitamin D levels in HS patients identified by previous studies cannot be confirmed to cause HS by linear MR analysis; reverse causality also cannot be ascertained. Nonetheless, the modulation of immune and inflammatory responses, specifically the IL-1β-T_H_17 cell cytokine axis, as well as the regulation of the hair cycle and keratinocyte proliferation, highlight possible mechanistic avenues through which vitamin D may improve HS symptoms. Further understanding of HS pathophysiology, the interplay between vitamin D supplements and administered HS therapeutics as well as other confounders is necessary, prior to inclusion of vitamin D in a treatment regimen.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Verstuyf A. Carmeliet G. Bouillon R. Mathieu C. Vitamin D: A Pleiotropic Hormone Kidney Int.20107814014510.1038/ki.2010.1720182414 · doi ↗ · pubmed ↗
- 2Rochel N. Vitamin D and Its Receptor from a Structural Perspective Nutrients 202214284710.3390/nu 1414284735889804 PMC 9325172 · doi ↗ · pubmed ↗
- 3De Luca H.F. Zierold C. Mechanisms and Functions of Vitamin D Nutr. Rev.200956 S 4S 1010.1111/j.1753-4887.1998.tb 01686.x 9564171 · doi ↗ · pubmed ↗
- 4Haussler M.R. Whitfield G.K. Kaneko I. Haussler C.A. Hsieh D. Hsieh J.-C. Jurutka P.W. Molecular Mechanisms of Vitamin D Action Calcif. Tissue Int.201392779810.1007/s 00223-012-9619-022782502 · doi ↗ · pubmed ↗
- 5Bukvić Mokos Z. Tomić Krsnik L. Harak K. Marojević TomićD. Tešanović PerkovićD. VukojevićM. Vitamin D in the Prevention and Treatment of Inflammatory Skin Diseases Int. J. Mol. Sci.202526500510.3390/ijms 2611500540507817 PMC 12154430 · doi ↗ · pubmed ↗
- 6ErtenŞ. Altunoğlu A. Ceylan G.G. MaraşY. Koca C. Yüksel A. Low Plasma Vitamin D Levels in Patients with Familial Mediterranean Fever Rheumatol. Int.2012323845384910.1007/s 00296-011-2281-422193220 · doi ↗ · pubmed ↗
- 7Kisacik B. Kaya S.U. Pehlivan Y. Tasliyurt T. Sayarlioglu M. Onat A.M. Decreased Vitamin D Levels in Patients with Familial Mediterranean Fever Rheumatol. Int.2013331355135710.1007/s 00296-011-2278-z 22187059 · doi ↗ · pubmed ↗
- 8Turhan T. Doğan H.O. Boğdaycioğlu N. Eyerci N. Omma A. Sariİ. Yeşilyurt A. Karaaslan Y. Vitamin D Status, Serum Lipid Concentrations, and Vitamin D Receptor (VDR) Gene Polymorphisms in Familial Mediterranean Fever Bosn. J. Basic Med. Sci.201818212810.17305/bjbms.2017.225928926322 PMC 5826670 · doi ↗ · pubmed ↗