Postoperative Ileus After Rectal Cancer Surgery: Assessing Incidence, Severity, and Impact Across Open, Laparoscopic, and Robotic Approaches
Michael Goldenshluger, Ofir Gruper, Yasmin Anderson, Tal Caller, Ephraim Katz, Alexander Lebedeyev, Ilan Kent, Edward Ram, Dean Lutrin, Lior Segev

TL;DR
Minimally invasive rectal cancer surgery reduces the chance of postoperative ileus compared to open surgery, but the severity of ileus is similar across all methods.
Contribution
The study compares ileus incidence and severity across open, laparoscopic, and robotic rectal cancer surgeries using consistent definitions.
Findings
Minimally invasive surgery had a 15.4% ileus rate compared to 31.1% in open surgery.
Robotic surgery showed a lower ileus rate (8.5%) than laparoscopic (17.6%), though not statistically significant.
Ileus severity was similar across all surgical approaches.
Abstract
Background/Objectives: Postoperative paralytic ileus (POI) is a common complication after rectal resections. Although it is often argued that laparoscopic or robotic surgery reduces ileus compared to open surgery, research indicates that the incidence rates remain considerably high after minimally invasive surgery (MIS), and it is unclear whether laparoscopy or robotic surgery confers lower ileus rates. Furthermore, the literature lacks consistency in defining ileus and does not adequately address the severity levels of this complication. This study aims to compare the incidence and severity of ileus after open, laparoscopic, and robotic oncologic rectal resections, using definitions established in the current literature. Methods: This is a retrospective cohort study including patients who underwent rectal resection in a single tertiary academic-affiliated hospital between the years…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
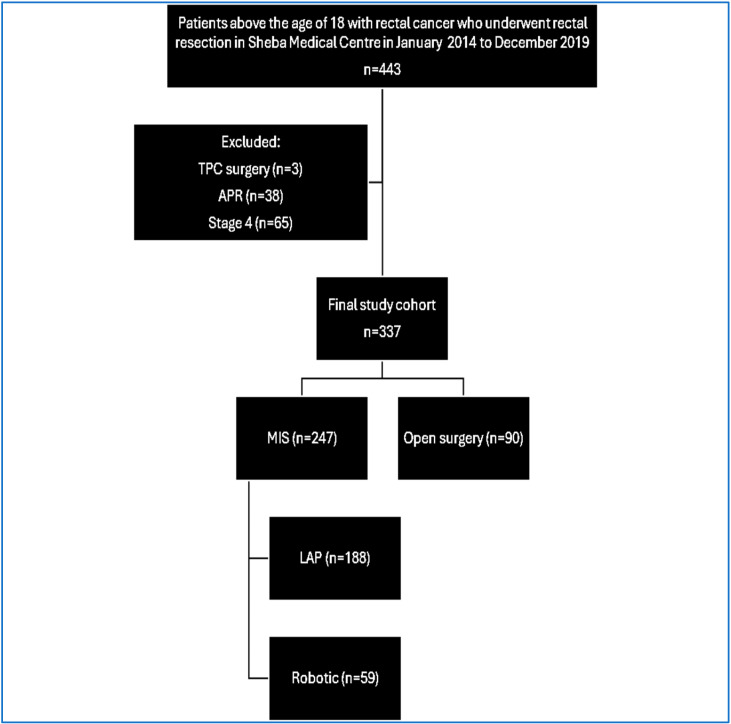 Figure 1
Figure 1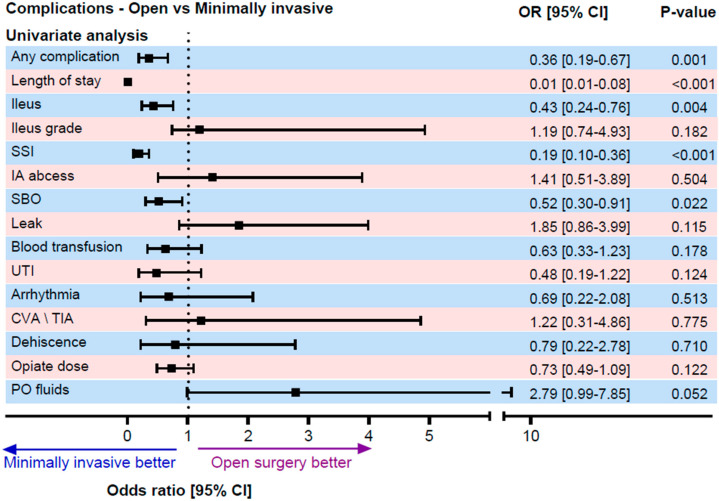 Figure 2
Figure 2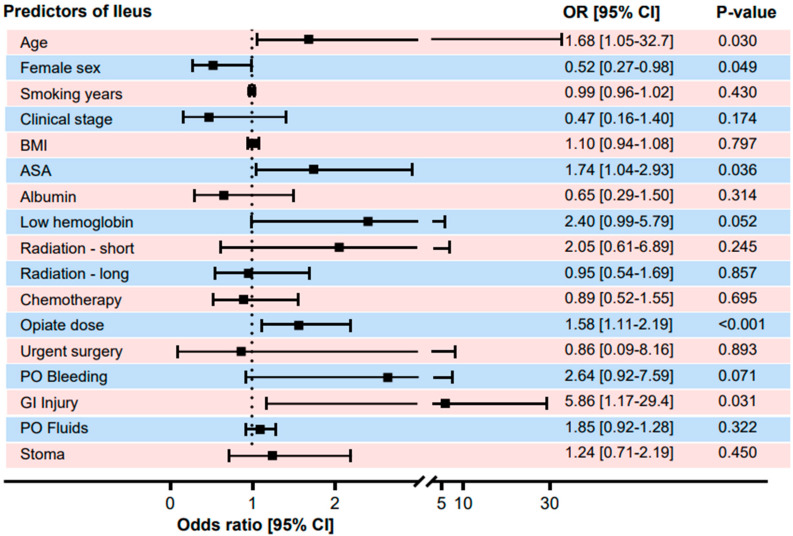 Figure 3
Figure 3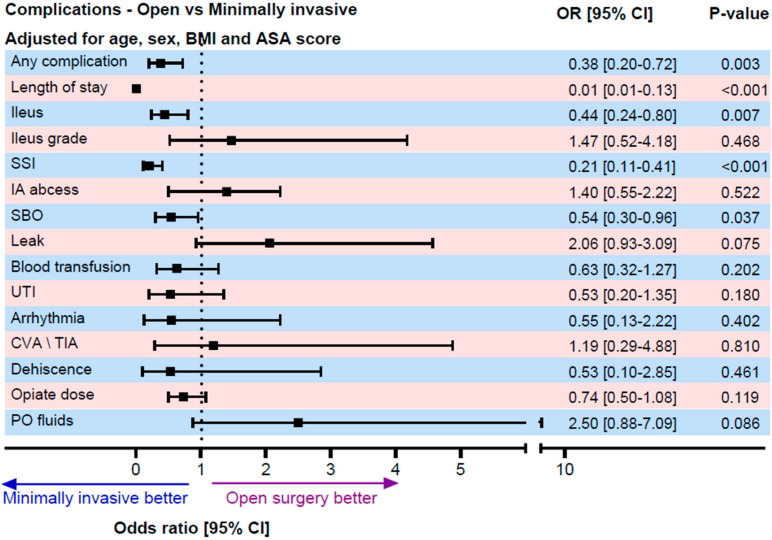 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEnhanced Recovery After Surgery · Colorectal Cancer Surgical Treatments · Stoma care and complications
1. Introduction
Post-operative ileus (POI) is a non-mechanical bowel disturbance caused by impaired intestinal motility, resulting from inflammation, neural reflexes, and neuro-humoral peptides [1,2]. Typically, ileus resolves within one to three days with supportive treatment, though it may persist for weeks in some cases, occasionally requiring full parenteral nutrition [3]. POI has a significant impact on the postoperative course, increasing the risk of complications, causing substantial patient discomfort, hindering mobilization, and prolonging hospitalization, leading to increased costs. The onset and progression of POI are difficult to predict. POI is defined as the period following surgery during which gas or stool is not passed, and oral diet tolerance is not achieved [4]. When these events occur early in postoperative recovery, they are considered a normal physiological response of the gastrointestinal tract to surgery. ‘Postoperative ileus’ (POI) refers to persistent ileus extending beyond the ‘obligatory POI’ phase and is independently associated with more severe symptoms. Although POI is commonly observed, there is no international consensus on its exact clinical definition [5]. The reported incidence of ileus varies widely in the literature. Up to 25% of patients experience some degree of ileus after elective abdominal surgeries, while POI occurs in 5–30% of patients following colorectal surgeries. Recent studies indicate that even with the advent of minimally invasive techniques, the incidence of ileus has not decreased after major oncological abdominal and pelvic surgeries, and in some cases, it has increased, particularly after colon and rectal resections and other cancer surgeries involving abdominal organs [6,7]. Although minimally invasive surgery is generally considered a protective factor against ileus in colorectal procedures, randomized controlled trials have shown only a modest effect of laparoscopic surgery on its incidence. Studies using the standard definition of ileus in the literature report significant rates, as high as 21%, in patients after laparoscopic surgeries [2]. The role of robotic surgery in preventing POI remains uncertain when compared to laparoscopy [8]. Moreover, the lack of a standardized clinical definition of ileus in previous studies hinders accurate assessment and evaluation of prevention and treatment strategies. This study aims to assess the incidence and severity of postoperative ileus following oncologic rectal resection surgeries. A secondary objective is to compare the occurrence and severity of ileus among open, laparoscopic, and robotic approaches. Based on existing literature, it is expected that open surgery will have the highest incidence and severity of ileus, followed by laparoscopic surgery, with robotic surgery showing the lowest rates. Additionally, the study seeks to identify the risk factors that are associated with postoperative ileus. Using data from this study, future research can focus on evaluating the effectiveness of treatments and preventive strategies for POI.
2. Methods
2.1. Patient Population
The study includes all patients who underwent rectal resection for cancer at a single tertiary referral center between January 2014 and December 2019. The exclusion criteria consisted of individuals under the age of 18, patients with metastatic disease, and those who underwent abdominoperineal resection (APR) or total proctocolectomy (TPC).
2.2. Variables
The variables in this study include both dependent and independent factors, as well as potential confounders.
The primary endpoint was postoperative ileus (POI). POI was defined as the occurrence of at least two gastrointestinal symptoms that started on postoperative day four or later, including nausea or vomiting, inability to tolerate oral intake for more than 24 h, absence of flatus or bowel movement for over 24 h, abdominal distension, or radiologic findings consistent with ileus.
This definition, initially described in the systematic review and global survey by Vather et al. [4], demonstrated ≥75% concordance among international experts and has since been widely adopted to standardize reporting. Accordingly, waiting until postoperative day 4 allows for a differentiation between the expected physiological postoperative gastrointestinal recovery and the clinically significant prolonged ileus. POI is classified as primary when no underlying cause, such as peritonitis or intra-abdominal bleeding, is identified, or secondary when it arises due to a complication like an anastomotic leak.
Ileus severity was categorized using the classification proposed by Venara et al. [9], which stratifies postoperative ileus according to clinical consequences, ranging from grade A (prolonged hospitalization only) to grade E (death). Grade B involves the need for symptomatic treatment or diagnostic procedures, including laxatives, prokinetic drugs, anti-spasmodic medications, and anti-nausea drugs. Grade C includes the requirement for nasogastric tube insertion or readmission after discharge, particularly if the tube is removed and reinserted. Grade D refers to severe complications, with D1 indicating renal dysfunction and D2 representing ICU admission or reoperation. The independent variables include the type of surgery, with a comparison between laparoscopic or robotic surgeries and open surgery.
Data on opioid use were collected from the medical team’s follow-up reports, summarizing the doses administered to each patient and standardized to the morphine equivalents. The opioid dose was treated as a continuous variable, allowing assessment of the dose–response relationship with the risk of postoperative ileus. Fluid administration volumes during the first four days post-surgery (up to post-operative day 4) were also documented in the medical records. Intraoperative bowel injury was defined based on the surgeon’s report, including any serosal injury, abrasion, partial serosal disruption, deeper bowel wall penetration, or perforation.
2.3. Surgical Technique
The type of surgery, either a low anterior resection of the rectum (LAR) or an anterior resection of the rectum (AR), was categorized based on the surgeon’s operative report. LAR was defined as a proctectomy with a total mesorectal excision (TME) down to the pelvic floor, while AR only involved a partial TME. Tumor height was measured in centimeters using rigid rectoscopy, with a classification as follows: a low rectal tumor (within 5 cm of the anal verge), a middle rectal tumor (5–10 cm), and an upper rectal tumor (10–20 cm).
2.4. Statistical Methods
Continuous variables were first assessed for distribution using the Kolmogorov–Smirnov test. Because most variables were not normally distributed, comparisons between groups were performed using the Mann–Whitney U test. Categorical variables were compared using the χ^2^ test. Continuous variables were presented as means with standard deviations, while dichotomous and categorical variables were presented as absolute numbers and percentages within each group. Ordinal and binary regression analyses were conducted to identify predictors of postoperative ileus and to assess its severity, both with and without adjustments for risk factors. Propensity scores were calculated for each patient, accounting for characteristics such as age at surgery, gender, BMI, smoking history, minimally invasive surgery status, and preoperative measures like albumin, hemoglobin, clinical staging, and cancer markers (CEA, CA19-9). The patients were matched based on these characteristics, which resulted in a matched cohort of 63 patients who underwent open surgery and 126 patients who underwent minimally invasive surgery. All of the statistical analyses were two-sided, with a significance level set at p < 0.05. The statistical analyses were performed using SPSS version 25.0 (SPSS Inc., Chicago, IL, USA), while the propensity score calculation and matching were performed using STATA BE V17 (StataCorp, College Station, TX, USA).
2.5. Ethics
This study was approved by the Helsinki Committee of Sheba Medical Center under the proposal number SMC-9618-22.
3. Results
3.1. Patient Characteristics
From January 2014 to December 2019, a total of 443 patients underwent anterior resection or low anterior resection at a single tertiary institution for rectal carcinoma treatment. After excluding 106 patients due to metastatic disease or additional colectomy or abdominoperineal resection, the final cohort comprised 337 rectal cancer patients. Among them, 188 underwent laparoscopic surgery, 59 had robotic surgery, and 90 underwent open surgery.
The cohort’s baseline characteristics are summarized in Table 1. The mean age of patients in the cohort was 63.6 years, with 56.4% (n = 190) being men. The tumor location varied, with 62.3% in the upper rectum, 31.5% in the middle rectum, and 6.2% in the lower rectum.
3.2. Incidence and Risk Factors for POI
The overall incidence of POI was 19.6% (n = 66). Open surgery had a higher POI rate of 31.1% (n = 28) compared to the minimally invasive group at 15.4% (n = 38). The laparoscopic and robotic surgeries were associated with a 57% lower risk of ileus (OR 0.43, 95% CI 0.24–0.76, p = 0.004) (Table 2). While robotic surgery showed a lower ileus rate compared to laparoscopic surgery (8.5% vs. 17.6%, p = 0.092), the difference was not statistically significant. The mean preoperative hemoglobin (Hb) level was significantly lower among patients who developed POI compared to those who did not. Specifically, the mean Hb was 11.95 g/dL in the POI group versus 12.78 g/dL in the non-POI group, corresponding to a mean difference of 0.83 g/dL (p < 0.05).
Univariate analysis identified significant risk factors for POI, including older age (OR 1.68, p = 0.03), male gender (OR 1.92, p = 0.049), higher ASA score (OR 1.74, p = 0.036), and low preoperative hemoglobin (OR 2.4, p = 0.052). Surgical factors like intraoperative bowel injury (OR 5.86, p = 0.031) and high-dose opioid use (OR 1.58, p < 0.001) were also associated with increased POI risk.
We compared the differences in the severity of ileus between the definition found in the literature (occurrence of two or more symptoms starting from postoperative day 4: vomiting; inability to tolerate oral nutrition for more than 24 h; absence of gas passage for more than 24 h; abdominal distension; and a characteristic radiographic image) and the clinical diagnosis. Among the 337 patients in the study, 66 patients (19.6%) met the literature-based criteria for ileus diagnosis, although only 33 (9.8%) were clinically diagnosed with POI by the medical team. Of the patients who met the literature-based definition for POI, 31 (47%) were also identified by the medical team, while 35 patients (53%) were not clinically diagnosed despite meeting the literature-defined criteria. Only 2 patients (0.7%) who were clinically diagnosed with ileus did not meet the literature-based criteria.
3.3. Complications and Surgical Outcomes
The binary logistic regression that was adjusted for age, gender, BMI, and ASA score confirmed that open surgery was an independent risk factor for ileus (OR 0.44, 95% CI 0.24–0.8, p = 0.007). A per-protocol analysis comparing planned open surgeries to converted minimally invasive surgeries showed no significant difference in ileus risk (OR 0.99, p = 0.985). Secondary analysis using propensity score matching (63 open surgeries vs. 126 minimally invasive surgeries) confirmed lower ileus rates in the minimally invasive group (17.5% vs. 35%, OR 0.39, p = 0.008). We specifically examined whether the conversion from minimally invasive to open surgery was associated with an increased risk of POI using a per-protocol analysis comparing planned open procedures with cases that were initiated minimally invasively and converted to open. In this analysis, conversion was not associated with an increased risk of POI (OR 0.99, 95% CI 0.47–2.08, p = 0.985), suggesting that the surgical approach that was ultimately performed is the primary determinant of POI risk.
3.4. Ileus Severity and Management
Among the 66 patients who developed ileus, severity classifications included 32% as grade A, 15% as grade B, and 47% as grade C. Severe cases were less frequent, with 4.5% in grade D and 1.5% in grade E. Ordinal logistic regression showed no significant difference in ileus severity between open and minimally invasive surgery (OR 1.19, p = 0.182).
3.5. Additional Clinical Benefits
Minimally invasive surgery demonstrated several additional benefits, including a 62% reduction in overall complications, halving the hospital stay duration, an 81% reduction in surgical site infections, and a 46% reduction in small bowel obstruction. After adjusting for confounders, the only statistically significant benefit that remained was the reduced hospital stay duration. No significant correlation was found between the surgery type and the complications, such as postoperative fluid collections, intra-abdominal abscesses, blood transfusion requirements, and opioid use (Figure 1, Figure 2, Figure 3 and Figure 4).
4. Discussion
The key findings of this study indicate a significantly lower incidence of ileus in minimally invasive rectal resections, with a trend suggesting a potential advantage of using robotic surgery over laparoscopy. Notably, anemia was identified as a major risk factor for ileus, a factor not previously reported in the literature.
This study confirms, through multivariate analysis and propensity score matching, that minimally invasive techniques act as a protective factor against POI. While non-randomized studies have linked robotic surgery to a significantly lower risk of ileus compared to the laparoscopic approach, a meta-analysis of randomized controlled trials did not reveal a significant difference between the two methods [10,11]. Our findings indicate a trend toward reduced ileus in the robotic surgery group. Notably, patients in the robotic group underwent more low resections and had higher rates of preoperative radiation—both factors that increase surgical complexity—further reinforcing the protective effect of robotic surgery against POI.
Our analysis of other risk factors for POI confirmed that age is a significant predictor, aligning with the existing literature [7]. Our study demonstrated that among middle-aged patients, the risk of developing ileus increased by 70% with each additional decade of life. Other established risk factors, including male sex, high American Society of Anesthesiologists (ASA) scores, and elevated postoperative opioid use, were also corroborated [12,13].
Notably, this study identified low preoperative hemoglobin levels as a previously unrecognized risk factor for POI. However, preoperative anemia is well-documented as a predictor of postoperative complications, increased 30-day morbidity, and prolonged hospital stay. Several pathophysiological mechanisms may underlie the association between preoperative anemia and ileus. Chronic inflammation, particularly in cases of iron deficiency anemia, may amplify the postoperative inflammatory response, while tissue hypoxia can impair wound healing and bowel motility. Additionally, perioperative blood transfusions, which are often required in anemic patients, have been independently associated with an increased risk of ileus.
Although prior studies have identified diverting stomas, particularly ileostomies, as a risk factor for POI^11^, we did not observe this association in our cohort. This may suggest that other factors influencing postoperative recovery in our population have had a greater impact than the presence of a stoma itself.
In this study, we report a relatively high POI incidence of almost 20% in a large cohort of oncologic proctectomy patients. This rate is higher than that reported for colorectal surgeries (9.4–14.2%) but lower than what is observed in randomized controlled trials that focus solely on rectal resection (30.9%) [13].
A potential explanation for the higher incidence of POI in this study is the definition applied. When classified based on the medical teams’ assessment, the incidence was 9.8%, whereas it increased to 19.6% when defined strictly according to the literature criteria. Notably, 53% of patients meeting the formal literature-based definition of ileus were not recognized as having the condition by the medical team. The study findings indicate that most of these additional cases identified by the literature definition were of mild severity. These included cases where ileus resulted solely in prolonged hospitalization (grade A) or required symptomatic management or a diagnostic evaluation (grade B). It appears that the medical team, when assessing these mild cases, attributed the symptoms to physiological POI—an expected postoperative occurrence that typically resolves without significant consequences. The predominance of mild cases among those diagnosed using the literature definition suggests that exclusive reliance on this criterion could lead to an overdiagnosis of clinically insignificant cases. These findings underscore the necessity for a more refined diagnostic approach to ileus, where clinical judgment plays a role in distinguishing mild cases from those with meaningful clinical implications.
Meta-analyses conducted by Vather et al. (2013) have highlighted inconsistencies in the terminology used across POI studies [4]. Specifically, the differentiation between “physiological” ileus and POI, which is more likely to have significant clinical consequences, is often unclear [4].
Another factor to consider is that during the period in which this study was conducted, an enhanced recovery after surgery (ERAS) protocol had not yet been fully implemented in our practice, which may have contributed to the higher frequency of postoperative ileus that was observed in this cohort.
This study is limited by its retrospective observational nature, which could introduce secondary biases due to confounding factors. Additionally, this is a single-center study, which reduces its external validity. In this context, there may have been a loss to follow-up for patients who received treatment at other hospitals due to complications. Moreover, the study relies on medical records that were written for clinical purposes, not research purposes, and thus some data were missing, potentially affecting the results. For example, there were no records on surgical time or blood loss during surgery, both of which are known risk factors for postoperative ileus. Furthermore, in the earlier years of the study (2014), there was no systematic documentation of the opioid doses given after surgery, meaning the true effect of opioid administration on ileus development may have been underestimated.
Regarding the analysis demonstrating a lower rate of POI in the robotic group compared with the open surgery group, this finding should be interpreted with caution, as the analysis may be underpowered. The sample size within the robotic subgroup may have been insufficient to detect a statistically significant difference.
Finally, our multivariable model may not have accounted for all potential risk factors and confounders, which is a common limitation in observational studies. In particular, operative complexity variables such as the extent of mesorectal excision were not included and may have influenced surgical difficulty and postoperative recovery.
Nonetheless, the study has several strengths. First, we employed multiple statistical methods for both primary and secondary analyses to validate the findings. Although it appeared that patients in the minimally invasive surgery (MIS) group were younger compared to those in the open surgery group, after adjusting and matching for confounders, we were able to demonstrate that MIS is associated with a lower incidence of ileus. Second, all participants included in the study underwent blinded adjudication. The chart review was manual, ensuring that data and diagnoses were accurate. Third, the fact that the study focused solely on rectal resection is a strength. Many studies examining the incidence of ileus combine rectal and colon surgeries, which could lower the reported incidence.
5. Conclusions
In conclusion, MIS for rectal cancer is associated with a significantly lower risk of postoperative ileus compared to open surgery, with a notable trend suggesting that robotic surgery may offer further advantages over laparoscopy. However, when ileus occurs, its severity remains comparable between the two techniques. It is important to note that this study identified preoperative anemia as a previously unrecognized risk factor for postoperative ileus, emphasizing the need for preoperative optimization to mitigate this risk.
Furthermore, the discrepancy between clinically diagnosed ileus and cases identified using literature-based criteria highlights the potential for overdiagnosis when relying solely on rigid definitions. Incorporating clinical judgment into the diagnostic process is essential to distinguish mild, self-resolving cases from those with meaningful clinical consequences.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hussain Z. Park H. Words K. Inflammation and Impaired Gut Physiology in Post-operative Ileus: Mechanisms and the Treatment Options J. Neurogastroenterol. Motil.20222851753010.5056/jnm 2210036250359 PMC 9577567 · doi ↗ · pubmed ↗
- 2Wattchow D. Heitmann P. Smolilo D. Spencer N.J. Parker D. Hibberd T. Brookes S.S.J. Dinning P.G. Costa M. Postoperative ileus—An ongoing conundrum Neurogastroenterol. Motil.202133 e 1404610.1111/nmo.1404633252179 · doi ↗ · pubmed ↗
- 3Buchanan L. Tuma F. Postoperative Ileus Stat Pearls Stat Pearls Publishing Treasure Island, FL, USA 202532809615 · pubmed ↗
- 4Vather R. Trivedi S. Bissett I. Defining Postoperative Ileus: Results of a Systematic Review and Global Survey J. Gastrointest. Surg.20131796297210.1007/s 11605-013-2148-y 23377782 · doi ↗ · pubmed ↗
- 5Wells C.I. Milne T.G.E. Seo S.H.B. Chapman S.J. Vather R. Bissett I.P. O’G Rady G. Post-operative ileus: Definitions, mechanisms and controversies ANZ J. Surg.202192626810.1111/ans.1729734676664 · doi ↗ · pubmed ↗
- 6Moghadamyeghaneh Z. Hwang G.S. Hanna M.H. Phelan M. Carmichael J.C. Mills S. Pigazzi A. Stamos M.J. Risk factors for prolonged ileus following colon surgery Surg. Endosc.20163060360910.1007/s 00464-015-4247-126017914 · doi ↗ · pubmed ↗
- 7Pozios I. Seeliger H. Lauscher J.C. Stroux A. Weixler B. Kamphues C. Beyer K. Kreis M.E. Lehmann K.S. Seifarth C. Risk factors for upper and lower type prolonged postoperative ileus following surgery for Crohn’s disease Int. J. Color. Dis.2021362165217510.1007/s 00384-021-03969-9PMC 842623634142229 · doi ↗ · pubmed ↗
- 8Christofi F.L. Impact of Minimal Invasive Robotic Surgery on Recovery From Postoperative Ileus and Postoperative Gastrointestinal Tract Dysfunction Am. J. Biomed. Sci. Res.2020853553810.34297/AJBSR.2020.08.00133538516381 PMC 10956729 · doi ↗ · pubmed ↗