Plasma CA125 as a Prognostic Marker in Very Elderly Patients Hospitalized for Acute Heart Failure
Javier Jaramillo-Hidalgo, Mónica Ramos, Maribel Quezada-Feijoó, Rocío Toro, Noemí García-Calderón, Francisco Javier Gómez-Pavón

TL;DR
This study shows that high CA125 levels in very elderly patients admitted for heart failure predict higher risk of death and readmission.
Contribution
The study is the first to demonstrate CA125's independent prognostic value in patients aged 80+ with acute heart failure.
Findings
Elevated CA125 levels independently predicted 12-month mortality in very elderly AHF patients.
CA125 ≥ 100 U/mL also predicted the composite outcome of mortality or heart failure readmission.
Functional dependence and frailty measures had better discriminative ability than biomarkers.
Abstract
Background/Objectives: Acute heart failure (AHF) is a leading cause of hospitalization and mortality among very old patients, yet this group is underrepresented in prognostic studies. Carbohydrate antigen 125 (CA125) has emerged as a potential biomarker of congestion and inflammation, but its value in patients aged 80 years and over remains unclear. We aimed to evaluate the prognostic value of plasma CA125 measured at admission for 12-month all-cause mortality and the composite outcome of mortality or heart failure (HF) readmission in very elderly patients hospitalized for AHF. Methods: We conducted a prospective observational study of patients aged ≥80 years admitted to an acute geriatric unit for AHF. CA125 and NT-proBNP were measured within 24 h of admission. Outcomes were assessed at 12 months. Survival analyses were performed using Kaplan–Meier curves, Cox regression models, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
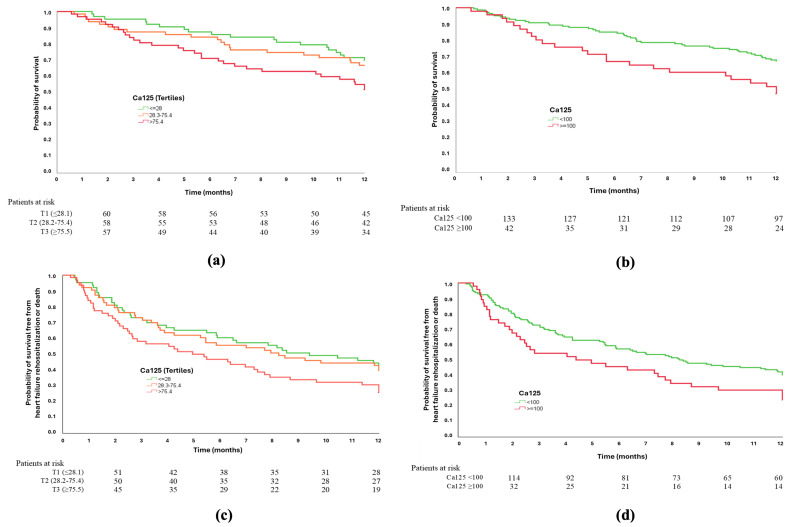 Figure 1
Figure 1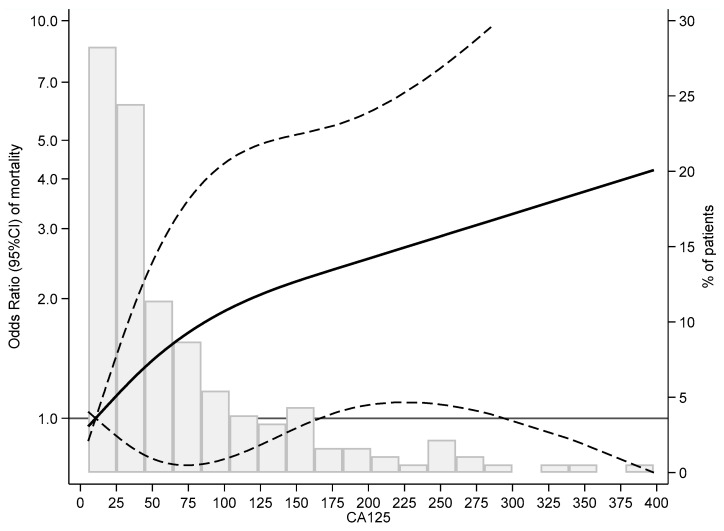 Figure 2
Figure 2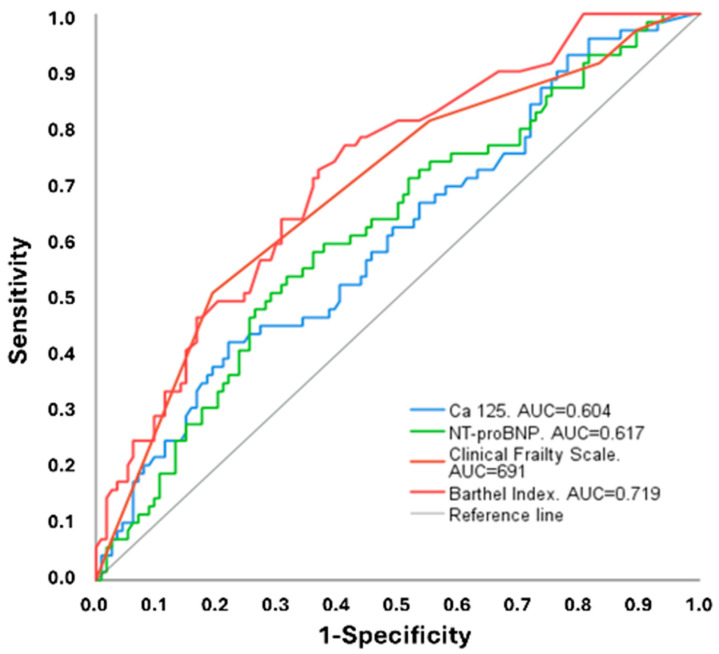 Figure 3
Figure 3- —Fundación Universidad Alfonso X el Sabio
- —Fundación Alfonso X el Sabio
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHeart Failure Treatment and Management · Sepsis Diagnosis and Treatment · Nutrition and Health in Aging
1. Introduction
Heart failure (HF) is a major public health problem in developed countries, with prevalence and incidence increasing markedly with age. Among patients aged 80 years and older, HF represents one of the leading causes of hospitalization and mortality. Despite its clinical relevance, this population remains underrepresented in most clinical trials and observational studies, especially those including patients with advanced frailty. Consequently, the applicability of existing evidence to routine geriatric practice is limited [1,2,3,4,5,6].
Older adults with HF differ substantially from younger cohorts. They typically present with a higher burden of comorbidities, polypharmacy, functional dependency, and frailty, which not only modify the clinical expression of HF but also influence prognosis and response to conventional therapies. In this setting, tools to improve risk stratification and support individualized management are urgently needed [6,7,8].
Biomarkers play a central role in HF diagnosis and prognosis. Natriuretic peptides are widely used, but their interpretation in very old patients is often challenging due to age-related physiological changes, renal dysfunction, and multimorbidity. In recent years, carbohydrate antigen 125 (CA125), a glycoprotein traditionally employed as a tumor marker in ovarian cancer, lung cancer, teratoma, and non-Hodgkin lymphoma, has emerged as a potential biomarker in HF. CA125 levels rise in response to serosal inflammation and systemic congestion, both hallmarks of acute heart failure (AHF). Several studies have demonstrated associations between elevated CA125 and congestion severity, longer hospital stays, and worse outcomes, including mortality and hospital readmissions. Moreover, CA125 is inexpensive, widely available, and less influenced by renal function than natriuretic peptides [9,10,11,12,13,14].
However, most available evidence derives from middle-aged or younger-old patients, with a mean age in the early seventies. Data focusing especially on the old-old (≥85 years) remains scarce. Furthermore, the interplay between CA125 levels and geriatric features such as frailty, functional status, and multimorbidity has been insufficiently investigated, despite their well-established impact on HF prognosis [6,7,8,15,16,17].
To address this gap, we have conducted a prospective observational study in patients aged 80 years and older admitted with AHF. We hypothesized that elevated CA125 levels at admission would be independently associated with a higher risk of all-cause mortality and the combined endpoint of mortality or HF hospital readmissions at one-year follow-up. In addition, we aimed to compare the prognostic performance of CA125 with established biomarkers and geriatric variables related to frailty and functional status.
2. Materials and Methods
2.1. Study Design and Setting
We conducted a prospective, single-center observational study designed to evaluate the prognostic value of CA125 in very elderly patients hospitalized for AHF. Consecutive patients were recruited between 9 March 2023 and 1 March 2024 in the acute geriatric unit of Hospital Universitario Central de la Cruz Roja, Madrid (Spain). All patients were followed for 12 months after hospital discharge.
2.2. Study Population
Eligible participants were consecutive patients aged ≥80 years admitted with a primary diagnosis of AHF, as defined by the 2021 European Society of Cardiology criteria [1]. Exclusion criteria were age less than 80 years, lack of informed consent, or active malignancy.
2.3. Sample Size
The required sample size was calculated to detect a statistically significant hazard ratio (HR) between CA125 and time to mortality during follow-up. According to previous studies [18], an estimated HR of 1.78 for all-cause mortality and 1.58 for the composite outcome of mortality or AHF hospitalization was assumed. To obtain a conservative estimate, the lower HR (1.58) was used.
For a confidence interval (CI) 95% and 80% statistical power, a minimum sample size of 166 patients was required. Assuming a 20% follow-up loss rate, the final target sample size was 208 patients, rounded up to 210 participants.
2.4. Clinical Assessment and Data Collection
Within the first 24 h of admission, standardized data collection was performed. Sociodemographic variables included age, sex, and living situation (home or nursing facility). The burden of comorbidities was assessed using the Charlson comorbidity index [19], and the presence of hypertension, diabetes mellitus, chronic kidney disease, atrial fibrillation, and coronary artery disease was recorded. A comprehensive geriatric assessment (CGA) was conducted in all patients, including: (i) frailty using the clinical frailty scale (CFS) [20], (ii) the functional status through the Barthel index (BI) [21], (iii) a nutritional evaluation using mini-nutritional assessment short form, and (iv) polypharmacy defined as the use of ≥5 medications.
The physical examination focused on signs of congestion, including jugular venous distension, peripheral edema, hepatomegaly, and orthopnea. The imaging and cardiac evaluation were performed with chest radiography, a 12-lead ECG, and a bedside ultrasound, using the Philips Lumify S4-1 (Philips Ultrasound, Bothell, WA, USA) to assess the inferior vena cava diameter and the presence/absence of a pleural effusion. Additionally, a transthoracic echocardiogram was performed during hospitalization if no examination had been performed within the previous 6 months (Philips Affinity-70C model, Philips Ultrasound, Bothell, WA, USA), to assess the left ventricular function, considering reduced ejection fraction when it was <50% [1], and to identify significant pulmonary hypertension when present [22].
Routine laboratory testing included basic hemogram and biochemical variables, including hemoglobin, creatinine, estimated glomerular filtration rate (CKD-EPI), sodium, and potassium.
In the case of a patient with chronic HF therapy, this information was documented at the time of admission.
2.5. Biomarkers Measurement
Plasma concentrations of CA125 and NT-proBNP were determined within 24 h of admission. Blood samples were obtained under standardized conditions and processed according to the hospital laboratory protocols. CA125 concentrations were determined using a luminescence-based immunometric immunoassay (Vitros CA125; Ortho Clinical Diagnostics, Madrid, Spain). NT-proBNP levels were measured by a fluorescence immunoassay (VIDAS NT-proBNP2; bioMérieux, Marcy-l’Etoile, France). The results were expressed in U/mL for CA125 and pg/mL for NT-proBNP.
For statistical analyses, CA125 was analyzed both as a continuous variable and in tertiles. Additionally, a predefined cut-off point was used (CA125 > 100 U/mL). To select this, different cut-off points were explored for the study event, and we chose the one that yielded the highest odds ratio (OR) and statistical significance in preliminary analyses at 6 months.
2.6. Outcomes
The primary endpoint was all-cause mortality within 12 months after hospital discharge. The secondary outcome was a composite of all-cause mortality or HF hospital readmissions within 12 months. In-hospital mortality was recorded but excluded from the survival analyses. Heart failure–related readmissions were defined as unplanned hospitalizations with heart failure as the primary discharge diagnosis from hospital administrative records. For analytical purposes, only the first readmission occurring during the follow-up period was considered. Follow-up data were obtained through review of electronic medical records and, when necessary, by telephone contact with patients or caregivers.
2.7. Statistical Analysis
Continuous variables are presented as mean ± standard deviation or median (interquartile range), according to data distribution. Categorical variables are expressed as counts and percentages. Group comparisons were performed using Student’s t-test or the Mann–Whitney U-test for continuous variables, and the χ^2^ test or Fisher’s exact test for categorical variables.
Time-to-event outcomes were analyzed using Kaplan–Meier survival curves, with log-rank comparisons performed. Follow-up time was calculated from hospital discharge to the event of interest or censoring at 12 months. Patients who died during the index admission were excluded from time-to-event analyses. Associations between CA125 levels and outcomes were evaluated using Cox proportional hazards regression models, and results are reported as hazard ratios (HRs) with 95% confidence intervals (CIs). The relationship between continuous CA125 levels and outcomes was further explored using restricted cubic spline regression. Prognostic discrimination was assessed using receiver operating characteristic (ROC) curves.
All statistical tests were two-sided, and p-values < 0.05 were considered statistically significant. Analyses were performed using SPSS version 28.0 (IBM Corp., Armonk, NY, USA) and Stata version 17.0 (StataCorp, College Station, TX, USA).
2.8. Ethical Considerations
The study protocol was reviewed and approved by the Institutional Ethics Committee of Universidad Alfonso X el Sabio (approval no. 2023_03/179). Written informed consent was obtained from all patients or their legal representatives. The study was conducted in accordance with the Declaration of Helsinki.
3. Results
3.1. Baseline Characteristics
A total of 210 patients aged 80 years and over were enrolled in the study. The mean age of the subjects was 89.8 ± 5.3 years, and 75.3% were females. Frailty was highly prevalent, with 88.1% of patients presenting a CFS score ≥ 5, and 37.6% showing moderate-to-severe functional dependence (BI < 60). HF with preserved ejection fraction (HFpEF) was the predominant phenotype (80.2%). In-hospital mortality occurred in 22 patients (10.5%), who were excluded from time-to-event analyses. Baseline clinical, functional, and laboratory characteristics are summarized in Table 1.
Median CA125 concentration at admission was 43 U/mL (IQR 22.3–96.6), and median NT-proBNP was 5424 pg/mL (IQR 2922–11,034).
3.2. Primary and Secondary Outcomes
The prognostic analyses were restricted to 188 patients discharged alive, after the index admission during which recruitment was performed, and followed for 12 months. Over a period of one year, 70 deaths (37.2%) were recorded, and 66 patients (36.1%) experienced at least one hospital readmission due to HF.
The baseline characteristics according to CA125 tertiles are shown in Table 2. Patients in the highest CA125 tertile did not differ significantly from those in the lower tertiles with respect to age, sex, living situation, degree of functional dependence, frailty status, or comorbidity burden. However, a trend towards higher atrial fibrillation prevalence was observed across increasing CA125 tertiles. A progressive increase in mortality was observed across the CA125 tertiles, with the highest tertile showing a higher one-year mortality rate than the lower two tertiles, with a trend toward statistical significance (p = 0.08).
We examined the association between admission CA125 and all-cause mortality. When patients were stratified into three groups based on their CA125 tertiles, the Kaplan–Meier curves demonstrated a progressive separation, with a higher cumulative mortality observed in the top tertile (log-rank p = 0.061) (Figure 1a). When the pre-specified threshold of 100 U/mL was applied, survival differences became more evident: individuals with CA125 concentrations of 100 U/mL and over had significantly lower 12-month survival rates compared to those with lower concentrations (log-rank p = 0.011) (Figure 1b). In Cox univariate models, CA125 in the highest tertile (vs. the lowest) was associated with an almost twofold increase in the hazard of death (HR 1.89, 95% CI 1.06–3.35; p = 0.031). Dichotomization at 100 U/mL yielded a similar effect size (HR 1.88, 95% CI 1.15–3.09; p = 0.012), supporting the clinical relevance of this pragmatic cut-off (Table 3).
We then evaluated the composite of all-cause mortality or HF rehospitalization at 12 months. The Kaplan–Meier analysis once again revealed a graded risk across the CA125 tertiles, with a tendency towards higher event rates in the upper tertile (log-rank p = 0.069) (Figure 1c). The 100 U/mL threshold identified a subgroup with clearly higher cumulative risk for the combined endpoint (log-rank p = 0.029) (Figure 1d). Consistently, Cox univariate regression demonstrated increased hazards for patients in the top tertile (HR 1.60, 95% CI 1.03–2.48; p = 0.035) and for those with CA125 ≥ 100 U/mL (HR 1.54, 95% CI 1.04–2.29; p = 0.031) (Table 3). Next, to characterize the stability of these associations across parameterizations, we compared tertile-based and cut-off-based analyses. In addition, multivariable Cox regression analyses further adjusted for geriatric assessment variables—including the Barthel Index, Charlson Comorbidity Index, and MNA-SF, selected to represent key domains of geriatric vulnerability (functional status, comorbidity burden, and nutritional status)—the association between CA125 and the study outcomes remained consistent in both magnitude and direction. Effect estimates were not substantially attenuated after this adjustment, supporting the independent prognostic value of CA125 beyond these clinically relevant markers of frailty and overall health status.
We performed a logistic regression using cubic splines. This revealed a direct, increasing, and almost linear relationship between CA125 and one-year mortality. There was a rapid increase up to CA125 values of 100 U/mL, followed by a less pronounced rise at higher levels. Moreover, the association reached statistical significance only at very high values, specifically above 150 U/mL (Figure 2).
When comparing prognostic discrimination, ROC curve analysis highlighted the superior performance of geriatric variables over biomarkers. The BI showed the strongest predictive capacity for one-year mortality (AUC 0.719, 95% CI 0.645–0.794), followed by the CFS (AUC 0.691, 95% CI 0.611–0.770). In contrast, NT-proBNP (AUC 0.617, 95% CI 0.533–0.701) and CA125 (AUC 0.604, 95% CI 0.520–0.689) displayed lower discriminative power (Figure 3). These findings suggest that functional dependence and frailty, as measured by the BI and CFS, were more effective predictors of mortality than the cardiac biomarkers in this very elderly cohort.
4. Discussion
This study, conducted in a cohort of hospitalized seniors with AHF, shows that CA125 measured at admission is a consistent prognostic marker for 12-month all-cause mortality and for the composite outcome of mortality or HF hospital readmissions. Our results, for the very first time, demonstrate the usefulness of this biomarker for early risk stratification in a population with a mean age close to 90 years. This population is typically belittled in AHF research studies but is exposed to the highest burden of adverse outcomes.
Our findings contribute to a growing body of evidence recognizing CA125, traditionally considered an oncological sign, as a marker of systemic congestion [18,23,24,25,26] and serosal inflammation with prognostic implications in HF. Prior studies, mostly in AHF but also in chronic stable HF [14], have shown that elevated CA125 levels correlate with congestion severity and increased risk of mortality and rehospitalization [27,28,29,30,31,32,33,34,35]. It is worth highlighting a systematic review published by Li et al. [31], which demonstrated that elevated CA125 levels were associated with a 68% increase in all-cause mortality (HR 1.68, 95% CI 1.36–2.07; p < 0.0001; I^2^ = 74%) and a 77% increase in HF–related readmissions (HR 1.77, 95% CI 1.22–2.59; p < 0.01; I^2^ = 73%). A more recently published systematic review also revealed CA125 as a significant prognostic factor for mortality and hospitalization risks in the acute and chronic HF population [36]. In 2025, Garcia et al. [37] confirmed that high C-reactive protein (CRP) levels, when coexisting with high CA125 levels, were associated with a higher mortality risk in a cohort of AHF with preserved EF. Concurrently, Miñana et al. [34], in a large cohort of patients with HFpEF, concluded that CA125 predicted the long-term burden of total HF admissions and was associated with the risk of long-term all-cause mortality. Agreeing with these authors, NT-ProBNP shows a lack of predictivity in AHF readmission due to the involvement of right HF, renal dysfunction, elderly patients, critical illness, and obesity; but also causes that provoke myocardial end-diastolic stress, such as pulmonary embolism or pneumonia. As proposed by the European Society of Cardiology, this marker needs to be supported by dyspnea and interpreted as a continuous variable [9]. The key contribution of our study is to confirm CA125’s prognostic value in an extremely old population characterized by advanced frailty, multimorbidity, and functional dependence.
A particularly practical finding is the identification of a clinically meaningful threshold. While some previous studies have focused on low CA125 levels to identify low-risk patients (e.g., <23 U/mL in the series by Núñez et al. [11]. In our cohort, elevated values (≥100 U/mL) identified a subgroup at substantially higher risk of both mortality and the composite endpoint at 12 months. These results highlight the potential usefulness of CA125 as a simple, widely accessible tool for prioritizing follow-up and the intensity of post-discharge care. Despite these findings, the proposed cutoff should be interpreted cautiously, given that it was derived from exploratory analyses within the same cohort and has not yet been validated in an independent population. Exploratory modelling using splines yielded a similar dose–response pattern, reinforcing the internal consistency of the association.
The composite endpoint of HF rehospitalization or mortality is particularly relevant in the geriatric scenario, as it reflects the care burden and morbidity that condition quality of life and resource use. In our cohort, elevated CA125 was significantly associated with increased risk of the composite at 12 months, consistent with previous large studies reporting that higher concentrations of the biomarker are accompanied by a progressive increase in the risk of death or HF hospitalization [18,30,31,34,38,39]. Our results are consistent with those reported by Nuñez et al. [18] in a cohort of 2356 patients hospitalized for AHF, where increasing CA125 quartiles independently predicted the combined outcome, with the highest risk observed in the upper quartile (HR = 1.72, 95% CI: 1.36–2.20; p < 0.001). Similar associations have been described by Miñana et al. [34], who observed a non-linear relationship between higher CA125 levels and HF readmission in 2369 patients with HFpEF. Also, Li et al. [31] reported an increased risk of HF hospitalization in patients with elevated CA125 levels (HR = 1.51, 95% CI: 1.11–2.04; p < 0.01). However, Llácer et al. [35] reported a weaker and non-significant association in a very elderly HFpEF cohort, more comparable to ours. This aligns with our preliminary 6-month analysis, in which CA125 did not significantly predict HF readmission, although a trend was observed in the highest tertile. Taken together, these data suggest that in older adults with HFpEF, the prognostic performance of CA125 may be attenuated when hospitalization is analyzed as an isolated outcome, rather than as part of a composite endpoint.
CA125 showed modest ability to predict mortality in our cohort, with performance notably lower than previously reported in larger studies, as Chen et al. reported (AUC: 0.845 for CA125) [33]. This may reflect the smaller sample size, the advanced age, the comorbidity burden, and the functional impairment of our population. By contrast, measures of functional dependence, using BI, and frailty demonstrated stronger discriminative value. These data may suggest that geriatric vulnerability overestimates biomarker-based risk in the old-old adults hospitalized for AHF. This observation is consistent with previous publications showing that higher BI scores at discharge were associated with lower mortality and reduced readmission risk, whereas poor functional status was associated with worse outcomes [16,40,41]. Frailty has also been repeatedly shown to predict adverse outcomes, independent of age and left ventricular function. Yuguchi et al. [42] recently reported a significant association between higher CFS scores and increased mortality risk (HR: 3.39, 95% CI: 1.32–8.72; p = 0.011), with an AUC of 0.74 for mortality prediction. Sunaga et al. [15] reported similar findings (HR: 2.54, 95% CI: 1.39–4.66; p = 0.003). The combination of frailty with elevated CA 125 appears to define the subgroup with the poorest prognosis, whereas individuals with preserved physical function and low CA125 demonstrated comparatively favorable outcomes [35,43]. This supports a dual approach to risk stratification—integrating biomarkers reflecting congestion and systemic inflammation with measures of functional capacity and frailty. Based on our results and the recommendations proposed by Jiménez-Méndez et al. [44], an optimal risk-stratification approach in the senior population may combine functional and frailty scales with blood-based biomarkers, such as CA125, to identify patients at high risk who may benefit from intensified management and closer follow-up.
Compared with previous evidence, our study broadens the field of application of the biomarker: it confirms that prognostic value is preserved when analyzing very elderly patients, with predominant HFpEF and high multimorbidity, and when using a high threshold (≥75–100 U/mL) that concentrates the most clinically relevant risk in this profile. In contrast to studies proposing low thresholds to define low risk [11,35], our data provides the necessary counterpart for practice: a high cut-off, operational for detecting high risk and guiding follow-up and treatment decisions.
In clinical application terms, the most directly transferable finding is that measuring CA125 at admission allows classification of elderly AHF patients into risk levels and identification of those with a substantially higher likelihood of dying or being re-hospitalized within one year. More recent studies have further suggested that serial measurement of this biomarker at discharge (in patients with a length of hospital stay >10 days) may have prognostic implications in terms of mortality [45]. This information can help prioritize resources (discharge planning, education, telemonitoring), adjust therapeutic thresholds (e.g., diuresis intensity with close monitoring of renal function), and structure follow-up (early visits, coordination with primary care). In this context, clinical trials have been published demonstrating the usefulness of CA-125–guided diuretic treatment strategy compared with standard management [46]. In addition, given its low cost, its use could be generalized without requiring additional infrastructure.
Several limitations materially constrain the interpretation of CA125 in this study. First, this was a single-center observational cohort with a relatively small sample size, which may limit statistical power and the generalizability of the findings. Furthermore, residual confounding cannot be excluded, and the external validity of the results should therefore be interpreted cautiously. Second, the modest sample size substantially reduced statistical power—particularly for interaction analyses—raising the likelihood of false-negative findings. Third, echocardiographic evaluation was not standardized, and key parameters (including pulmonary pressures and right ventricular function) were not systematically collected. Fourth, biomarkers were obtained within 48 h of admission; although acceptable for CA125 given its long half-life, this sampling window is likely suboptimal for NT-proBNP, which may be more informative when measured closer to discharge. Fifth, post-discharge CA125 trajectories were not captured, precluding assessment of dynamic risk stratification and longitudinal response. Sixth, the CA 125 threshold of 100 U/mL was derived from exploratory analyses within the same study cohort and was not externally validated, which may limit its generalizability and should be confirmed in independent populations. Finally, these results pertain to acute heart failure and should not be generalized to stable heart failure populations.
The study also has notable strengths: we studied one of the oldest cohorts reported (predominantly nonagenarians), captured an exhaustive CGA (frailty, functional status, and geriatric syndromes), achieved high data completeness, and completed 12-month follow-up despite logistical challenges. These features enhance real-world relevance and underscore the value of geriatric–cardiology collaboration for risk stratification in very old patients with AHF.
5. Conclusions
In very elderly patients hospitalized for AHF, CA125 measured at admission was independently associated with 12-month mortality and with the composite of mortality or HF rehospitalization. A pragmatic threshold of ≥100 U/mL identified a high-risk subgroup with clearly worse outcomes. CA125 is simple, inexpensive, and widely available, and provides complementary prognostic information to cardiogeriatric assessment. Routine incorporation of CA125 into the evaluation of very old patients with AHF may support individualized care planning and prioritization of post-discharge follow-up. Further multicenter studies should evaluate whether CA125-guided strategies can improve outcomes in this highly vulnerable population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mc Donagh T.A. Metra M. Adamo M. Baumbach A. Böhm M. Burri H. Čelutkiene J. Chioncel O. Cleland J.G.F. Coats A.J.S. 2021 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure Eur. Heart J.2021423599372610.1093/eurheartj/ehab 36834447992 · doi ↗ · pubmed ↗
- 2Roger V.L. Go A.S. Lloyd-Jones D.M. Benjamin E.J. Berry J.D. Borden W.B. Bravata D.M. Dai S. Ford E.S. Fox C.S. Heart Disease and Stroke Statistics-2012 Update: A Report from the American Heart Association Circulation 2012125 e 2e 22010.1161/CIR.0b 013e 31823 ac 04622179539 PMC 4440543 · doi ↗ · pubmed ↗
- 3Dharmarajan K. Rich M.W. Epidemiology, Pathophysiology, and Prognosis of Heart Failure in Older Adults Heart Fail. Clin.20171341742610.1016/j.hfc.2017.02.00128602363 · doi ↗ · pubmed ↗
- 4Mozaffarian D. Benjamin E.J. Go A.S. Arnett D.K. Blaha M.J. Cushman M. Das S.R. de Ferranti S. Després J.-P. Fullerton H.J. Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association Circulation 2016133 e 38e 36010.1161/CIR.000000000000035026673558 · doi ↗ · pubmed ↗
- 5GBD 2017 Disease and Injury Incidence and Prevalence Collaborators Global, Regional, and National Incidence, Prevalence, and Years Lived with Disability for 354 Diseases and Injuries for 195 Countries and Territories, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017 Lancet 20183921789185810.1016/S 0140-6736(18)32279-730496104 PMC 6227754 · doi ↗ · pubmed ↗
- 6Lazzarini V. Mentz R.J. Fiuzat M. Metra M. O’Connor C.M. Heart Failure in Elderly Patients: Distinctive Features and Unresolved Issues Eur. J. Heart Fail.20131571772310.1093/eurjhf/hft 02823429975 PMC 4176107 · doi ↗ · pubmed ↗
- 7Yang M. Kondo T. Anand I.S. de Boer R.A. Campbell R.T. Køber L. Lam C.S.P. Maggioni A.P. Martinez F.A. O’Meara E. Clinical Characteristics and Outcomes of Patients Aged 80 Years and over with Heart Failure: Need for Better Treatment Eur. J. Heart Fail.2024271403141710.1002/ejhf.341739169481 · doi ↗ · pubmed ↗
- 8Boureau A.S. Annweiler C. Belmin J. Bouleti C. Chacornac M. Chuzeville M. David J.P. Jourdain P. Krolak-Salmon P. Lamblin N. Practical Management of Frailty in Older Patients with Heart Failure: Statement from a Panel of Multidisciplinary Experts on Behalf the Heart Failure Working Group of the French Society of Cardiology and on Behalf French Society of Geriatrics and Gerontology ESC Heart Fail.202294053406310.1002/ehf 2.1404036039817 PMC 9773761 · doi ↗ · pubmed ↗