Personalized cardiovascular risk management for outdoor activities: a digital health application
Marco Vecchiato, Nicola Borasio, Sandro Savino

TL;DR
A new digital app called MOVE helps people manage cardiovascular risks while hiking by personalizing trail recommendations based on individual health and trail conditions.
Contribution
MOVE is a novel digital health system that integrates user-specific cardiovascular risk and trail features to provide personalized hiking predictions.
Findings
MOVE estimates cardiorespiratory fitness and classifies cardiovascular risk according to ESC guidelines.
The app was widely adopted, with over 3000 hikes recorded, including users with diverse cardiovascular risk profiles.
Nearly one-third of hikes were classified as high-effort, particularly for users with lower fitness or demanding trails.
Abstract
Hiking is a widely practiced outdoor activity with well-known cardiovascular and mental health benefits. However, its popularity among individuals with chronic conditions and across varying fitness levels raises safety concerns, especially in mountainous environments. Current trail planning tools typically rely on generic metrics, without considering individual cardiovascular risk or functional capacity. To address this gap, a novel digital system named MOVE was developed. Based on a patented algorithm, MOVE integrates user-specific characteristics, such as age, sex, body mass index, physical activity level, cardiovascular risk factors, and chronic conditions, with trail features, such as slope, elevation, and altitude. The system provides estimated cardiorespiratory fitness (eCRF), classifies cardiovascular risk according to ESC guidelines, and generates personalized predictions of…
Click any figure to enlarge with its caption.
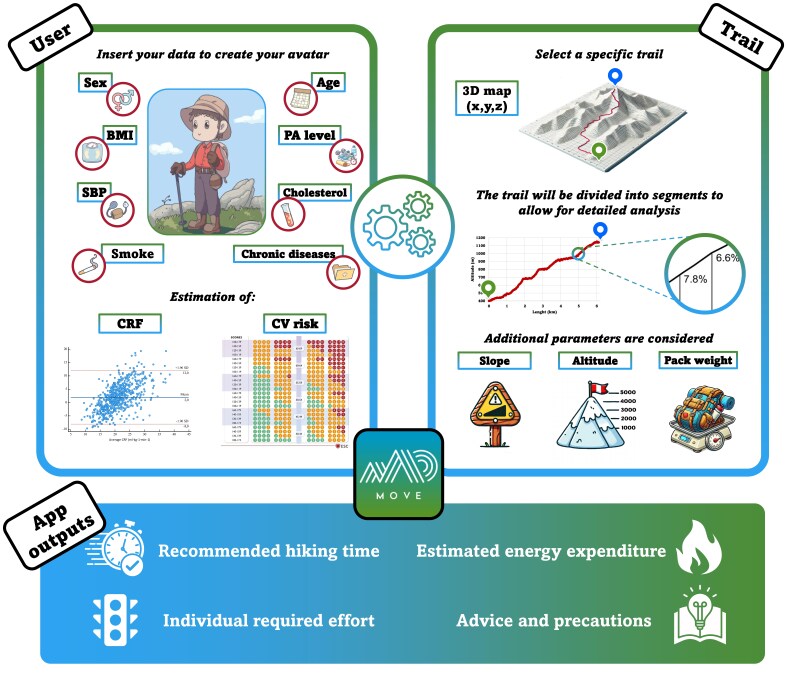 Figure 1
Figure 1| Variables | All | Women | Men | ||||
|---|---|---|---|---|---|---|---|
|
|
|
| |||||
|
|
|
|
|
|
|
|
|
| 48.17 | 14.64 | 44.60 | 12.15 | 49.54 | 15.27 | ||
|
|
|
|
|
|
| ||
|
| 884 | 29 | 283 | 34 | 601 | 28 | |
|
| 889 | 30 | 337 | 41 | 552 | 25 | |
|
| 1058 | 35 | 209 | 25 | 849 | 39 | |
|
| 173 | 6 | 3 | 0 | 170 | 8 | |
|
|
|
|
|
|
|
|
|
| 23.98 | 3.29 | 23.01 | 3.78 | 24.35 | 3.01 | ||
|
|
|
|
|
|
| ||
|
| 47 | 2 | 41 | 5 | 6 | 0.3 | |
|
| 2057 | 68 | 610 | 73 | 1447 | 67 | |
|
| 752 | 25 | 132 | 16 | 620 | 29 | |
|
| 148 | 5 | 49 | 6 | 99 | 4 | |
|
|
|
|
|
|
|
|
|
| 37.13 | 8.13 | 32.83 | 7.49 | 39.07 | 7.65 | ||
|
|
|
|
|
|
|
| |
|
| 1871 | 62 | 567 | 68 | 1304 | 60 | |
|
| 605 | 20 | 97 | 12 | 508 | 23 | |
|
| 11 | 0.4 | 0 | 0.0 | 11 | 1 | |
|
| 89 | 3 | 2 | 0.2 | 87 | 4 | |
|
| 428 | 14 | 166 | 20 | 262 | 12 | |
|
|
| 1778 | 59 | 500 | 60 | 1278 | 59 |
|
| 277 | 9 | 63 | 8 | 214 | 10 | |
|
| 19 | 1 | 12 | 1 | 7 | 0.3 | |
|
| 299 | 10 | 10 | 1 | 289 | 13 | |
|
| 631 | 21 | 247 | 30 | 384 | 18 | |
|
|
| 428 | 14 | 51 | 6 | 377 | 17 |
|
| 2419 | 81 | 719 | 86 | 1700 | 78 | |
|
| 157 | 5 | 62 | 7 | 95 | 4 | |
|
|
| 967 | 32 | 296 | 36 | 671 | 31 |
|
| 324 | 11 | 83 | 10 | 241 | 11 | |
|
| 184 | 6 | 49 | 6 | 135 | 6 | |
|
| 15 | 0.5 | 0 | 0 | 15 | 1 | |
|
| 1514 | 50 | 404 | 49 | 1110 | 51 | |
|
|
| 1065 | 35 | 292 | 35 | 773 | 36 |
|
| 805 | 27 | 172 | 21 | 633 | 29 | |
|
| 544 | 18 | 175 | 21 | 369 | 17 | |
|
| 590 | 20 | 193 | 23 | 397 | 18 | |
|
|
| 490 | 16 | 35 | 4 | 455 | 21 |
|
| 2227 | 74 | 710 | 85 | 1517 | 70 | |
|
| 49 | 2 | 21 | 3 | 28 | 1 | |
|
| 79 | 3 | 38 | 5 | 41 | 2 | |
|
| 67 | 2 | 1 | 0.1 | 66 | 3 | |
|
| 79 | 3 | 29 | 3 | 50 | 2 | |
|
| 10 | 0.3 | 1 | 0.1 | 9 | 0.4 | |
|
| 7 | 0.2 | 2 | 0.2 | 5 | 0.2 | |
|
| 7 | 0.2 | 1 | 0.1 | 6 | 0.3 | |
|
| 2 | 0.1 | 1 | 0.1 | 1 | 0.0 | |
|
|
|
|
|
|
|
| |
|
| 10008 | 7972 | 9483 | 6690 | 10205 | 8394 | |
|
| 804 | 609 | 699 | 536 | 844 | 630 | |
|
|
|
|
|
|
| ||
|
|
| 740 | 25 | 282 | 34 | 458 | 21 |
|
| 1712 | 57 | 394 | 47 | 1318 | 61 | |
|
| 552 | 18 | 156 | 19 | 396 | 18 | |
|
|
| 1434 | 48 | 450 | 54 | 984 | 45 |
|
| 625 | 21 | 210 | 25 | 415 | 19 | |
|
| 945 | 31 | 172 | 21 | 773 | 36 | |
- —Monade srl team
- —Kick-Start Activity
- —European Space Agency10.13039/501100000844
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHigh Altitude and Hypoxia · Adventure Sports and Sensation Seeking · Physical Activity and Health
Introduction
Hiking is an increasingly popular outdoor recreational activity, especially during the summer season, with increasing accessibility due to available technical equipment and infrastructures. Outdoor activities are now practiced by a broad population, including individuals with chronic conditions or those seeking outdoor activities for their physical and mental well-being. Benefits include improved functional capacity, also affecting cardiorespiratory fitness, coordination, and reducing stress levels.
However, outdoor activities inherently carry risks. Following the COVID-19 pandemic, there has been a substantial rise in nature-based tourism all around the world with a parallel increase in accidents, primarily due to limited awareness of environment-specific risks.^1^ While climbing or alpine mountaineering could be expected as high-risk sports, hiking ranks first among outdoor activities requiring rescue operations, accounting for about 50% of all mountain rescue calls.^2^ The most frequent causes include falls, slips, fatigue, and acute medical events, often due to an underestimation of the required effort or inappropriate planning and trail selection. Notably, sudden cardiac death remains the leading cause of death among men over 34 years of age during mountain excursions.^3^
Although traditional hiking signage and online platforms provide useful data on trail length, altitude, elevation profile, and technical difficulty, they generally do not consider individual pathophysiological characteristics and lifestyle. Hiking times are typically estimated based on average users, with no personalized adjustment for physical activity and fitness level, health status, or cardiovascular risk profile. Despite the availability of national and international standards for trail classification (e.g. Swiss and Italian Alpine associations), most hikers must still rely on generic information. Moreover, such route signage typically estimates that an average person gains about 350 m per hour of ascent and 500 m per hour of descent, also considering changes in altitude. These values are helpful but fail to account for the high inter-individual variability regarding cardiorespiratory fitness, exercise tolerance, and relative cardiovascular demand.
MOVE: a novel digital tool for risk-stratified and fitness-based hiking guidance
In recent years, the fitness and digital health sectors have increasingly incorporated individual physiological and cardiovascular data into physical activity and exercise planning. Numerous commercial applications and devices now provide training recommendations tailored to parameters, such as age, heart rate, or estimated cardiorespiratory fitness (eCRF) reflecting a broader trend towards data-driven personalization in physical activity and sports.^4^ This approach appears particularly relevant for outdoor activities such as hiking, when considering the heterogeneous fitness levels and clinical conditions for a potentially demanding cardiorespiratory effort in an uncontrolled mountain environment. Nonetheless, most route-planning tools currently available on the market for outdoor use, continue to rely on generic metrics, without accounting for individual health status or cardiovascular risk.^5^
To address this implementation gap and to promote the health benefits for outdoor physical activities in natural environments, a patented algorithm has been developed integrating user-specific characteristics, such as age, sex, body mass index (BMI), physical activity level, cardiovascular risk factors, and possible chronic conditions, into the planning of hiking itineraries (Graphical Abstract). The system employs scientifically validated equations to estimate eCRF and uses cardiovascular risk classification according to the most recent ESC guidelines.^6,7^ The algorithm dynamically selects the most appropriate eCRF equation according to the individual user profile (age, sex, BMI, and physical activity level), based on reported performance metrics of validated models. eCRF is used exclusively for relative effort stratification and preventive guidance, and not for clinical fitness diagnosis or performance prescription. Based on these outputs, the system defines a recommended physical effort threshold, expressed as a percentage of eCRF, in accordance with the ESC guidelines on physical activity and cardiovascular disease prevention.^8^
This digital model has been implemented in a prototype application, called MOVE (publicly available as MOVE – hike and bike), which analyses trail features such as altitude, elevation change and slope in association with the user profile to provide personalized estimates of recommended hiking time, energy expenditure, heart rate intensity ranges, and relative physical effort.^9^ These outputs support informed trail selection based on an individual’s functional capacity and risk profile.^5^
Besides providing specific qualitative recommendations for different pathologies, the algorithm also considers other real-world variables such as load carriage and altitude to refine eCRF estimates and effort prediction. Carrying a backpack increases oxygen consumption, thus significantly affecting aerobic capacity with an impact of about ∼20% per 10% additional load relative to body weight. The algorithm takes this information and adjusts the outputs based on backpack weight. Similarly, altitude exposure reduces aerobic capacity by ∼1% per 100 m above 1500 m; thus, an approximately 20% reduction is expected at 3500 m. These adjustments aim to provide more realistic and tailored estimates aligned with the physiological demands of hiking.^10^
Real-world implementation: participant characteristics and trail data
Since its public release on online platforms in autumn 2024, MOVE has been broadly adopted, particularly during the spring-summer 2025 season, following partnerships with selected Italian Alpine tourist regions. Dedicated trail signage was installed, including vertical QR codes linking to the app interface. Between April and September 2025, 3004 hiking records were collected through the app, providing insight into its practical application and user demographics (Table 1).
The cohort included 2172 men and 832 women, with a mean age of 48.17 ± 14.64 years. Most users were aged between 40 and 70 years (65%) and had a normal BMI (23.98 ± 3.29 kg/m^2^). Based on self-reported values and SCORE2/SCORE2-OP classifications, the cardiovascular risk profile included 967 individuals at low-to-moderate risk (32%), 324 at high risk (11%), and 184 at very high risk (6%), while 15 users <40 years old showed high risk based on medical history.
The mean eCRF was 37.1 ± 8.1 mL/kg/min, with significantly lower values in women. Blood pressure and cholesterol levels were reported as normal or well controlled in over 70% of participants, though 14% and 21% of users were unaware of their respective values. Notably, 14% were active smokers.
The most common trails selected had a mean length of ∼10 km and an average elevation gain of ∼800 m, with technical classifications of E (Hiking, 57%) and EE (Expert Hiking, 18%) being the most represented. Despite a wide range of physical fitness and clinical status, 31% of the hikes were classified by the algorithm as high effort, particularly among those with lower eCRF and/or greater elevation gain.
Limitations and future directions
This study does not report clinical outcomes such as adverse cardiovascular events or demonstrated safety improvements. The analysis is descriptive and exploratory, focusing on feasibility, implementation, and real-world usage patterns. Prospective studies evaluating clinical outcomes and safety endpoints are planned.
A key limitation of the current dataset is the reliance on self-reported health and lifestyle data, including blood pressure, cholesterol levels, and physical activity habits. As expected in a non-clinical, population-based setting, a substantial proportion of users were unable to report exact values for these parameters. To mitigate this issue, health variables were collected using predefined categories rather than continuous values, and missing information was explicitly classified as ‘unknown’. In cases where cardiovascular risk could not be calculated using risk charts due to incomplete data, a conservative risk classification strategy was adopted, assigning the highest plausible risk category based on the available information in order to avoid risk underestimation. This precautionary approach prioritizes user safety but may lead to overestimation of cardiovascular risk in some individuals.
Although directly measured CRF values are not available in the MOVE real-world dataset, we previously conducted controlled laboratory and field-based physiological testing using CPET and portable breath-by-breath gas analysis during hiking to objectively characterize the cardiorespiratory demands of hiking and the inter-individual variability in relative exercise intensity.^11^ These findings support the physiological rationale underlying MOVE’s effort modelling approach. Dedicated studies directly comparing eCRF and directly measured CRF values are planned as part of future research.
The current application processes the GPX file of the selected route, considering the associated user parameters and provides an overall trail-level assessment. However, future developments will offer more precise analyses, through segment-based breakdowns of trails and real-time tracking of the user position and speed, with adaptive recommendations and timely feedback along the trail.
Processing current and past tracking data of a single user with machine learning algorithms will allow better predictions of the user’s fitness level and expected performance; on the other hand, multi user data will be used to detect and offset errors in the route (e.g. accounting for a constant or seasonal bias due to the terrain type) to improve the algorithm outputs. Integration with wearable devices is expected to further improve the accuracy of the system due to live monitoring and processing of physiological data such as step cadence, heart rate, ventilation or oxygen saturation. In this evolving digital health landscape, applications designed for outdoor activities should move towards evidence-based personalization, particularly for populations at increased cardiovascular risk. The incorporation of artificial intelligence could further enhance these systems, enabling methods for user profiling, real-time data analysis, predictive modelling, and tailored feedback based on user trends and biometric feedback loops.
On the other hand, the growing presence of digital platforms, outdoor-specific social media and route-sharing websites has increased visibility and accessibility to mountain tourism, without adjusting for the related risks with specific target initiatives. Non-personalized recommendations may inadvertently promote overexertion or unsafe behaviour, particularly among less experienced or higher-risk individuals. The potential for these platforms to support individualized planning based on fitness and risk profiling represents a valuable direction and opportunity for public health initiatives and health tourism by promoting safe and salutary physical activity in nature mountain environment.
Conclusions
While outdoor activities like hiking offer significant cardiovascular and psychological benefits, they must be approached with a greater degree of individualized planning, especially as participation expands across age and risk spectrums. Digital health tools integrating cardiovascular risk assessment, pathophysiological profiling, physical activity, and fitness evaluations as well as hiking trail analysis may serve as valuable allies in this effort. A patented algorithm currently implemented in an early-phase digital application suggests the feasibility and first promising outcomes of this approach. In the near future, the incorporation of artificial intelligence and wearable technology may further support hikers in making informed, health-conscious and thus safe decisions before and during such outdoor activities.
Ethical considerations
No identifiable personal data were collected through the MOVE - hike and bike application. All data analysed in this study were fully anonymized and aggregated. According to European data protection regulations, the analysis of fully anonymized data does not involve the processing of personal data. Therefore, in accordance with institutional policies, this study did not require formal ethics committee approval.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Van Veelen MJ, Voegele A, Rauch S, Kaufmann M, Brugger H, Strapazzon G. COVID-19 pandemic in mountainous areas: impact, mitigation strategies, and new technologies in search and rescue operations. High Alt Med Biol 2021;22:335–341.34319777 10.1089/ham.2020.0216 PMC 8558066 · doi ↗ · pubmed ↗
- 2Ciesa M, Grigolato S, Cavalli R. Retrospective study on search and rescue operations in two prealps areas of Italy. Wilderness Environ Med 2015;26:150–158.25698181 10.1016/j.wem.2014.10.008 · doi ↗ · pubmed ↗
- 3Burtscher M . Risk of cardiovascular events during mountain activities. Adv Exp Med Biol 2007;618:1–11.18269184 10.1007/978-0-387-75434-5_1 · doi ↗ · pubmed ↗
- 4Javed A, Kim DS, Hershman SG, Shcherbina A, Johnson A, Tolas A, et al Personalized digital behaviour interventions increase short-term physical activity: a randomized control crossover trial substudy of the My Heart counts cardiovascular health study. Eur Heart J Digit Health 2023;4:411–419.37794870 10.1093/ehjdh/ztad 047PMC 10545510 · doi ↗ · pubmed ↗
- 5Vecchiato M, Borasio N, Scettri E, Franzoi V, Duregon F, Savino S, et al Are suggested hiking times accurate? A validation of hiking time estimations for preventive measures in mountains. Medicina (Lithuania) 2025;61:115.10.3390/medicina 61010115 PMC 1176685939859097 · doi ↗ · pubmed ↗
- 6Visseren F, Mach F, Smulders YM, Carballo D, Koskinas KC, Bäck M, et al 2021 ESC guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J 2021;42:3227–3337.34458905 10.1093/eurheartj/ehab 484 · doi ↗ · pubmed ↗
- 7Peterman JE, Harber MP, Imboden MT, Whaley MH, Fleenor BS, Myers J, et al Accuracy of exercise-based equations for estimating cardiorespiratory fitness. Med Sci Sports Exerc 2021;53:74–82.32694370 10.1249/MSS.0000000000002435 · doi ↗ · pubmed ↗
- 8Pelliccia A, Sharma S, Gati S, Bäck M, Börjesson M, Caselli S, et al 2020 ESC guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur Heart J 2021;42:17–96.32860412 10.1093/eurheartj/ehaa 605 · doi ↗ · pubmed ↗