The Limited Evidence Base for Multilevel Lumbar Interbody Fusion and Its Consequences for Clinical Conclusions: A Systematic Review
Evan R. Simpson, Casey Slattery, Kalyn Smith, Jesse Caballero, Michael Gordon, Gerald Alexander, Jon White, Jeffrey Deckey, Jeremy Smith, Vance Gardner

TL;DR
This systematic review finds limited evidence for multilevel lumbar interbody fusion techniques, highlighting the need for better studies to guide clinical decisions.
Contribution
The first systematic review of multilevel LIF literature, identifying publication bias and highlighting advantages of lateral and oblique approaches.
Findings
TLIF showed the shortest operative time and hospital stay with favorable pain and disability scores.
Lateral and oblique approaches provided better radiographic outcomes compared to posterior approaches.
Minimal clinical differences were found between minimally invasive and open TLIF techniques.
Abstract
Background/Objectives: Lumbar interbody fusion (LIF) is widely utilized to treat multilevel degenerative lumbar spine pathologies. This systematic review aimed to comprehensively review lateral and posterior multilevel LIF procedures and their clinical and radiographic outcomes. Methods: Following the PRISMA guidelines, a search of PubMed, Embase, Web of Science, and Cochrane identified eligible studies. Patient demographics, as well as clinical and radiographic outcomes were collected. Risk of bias was assessed using the MINORS criteria, while randomized trials were evaluated using the RoB-2 tool. An extensive subgroup analysis was completed when that was possible. Results: A total of 45 studies were included consisting of 5623 patients. The pooled outcomes indicated that TLIF demonstrated the lowest operative duration (198.7 ± 77.83 min) and LOS (5.09 ± 2.5 days), alongside favorable…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
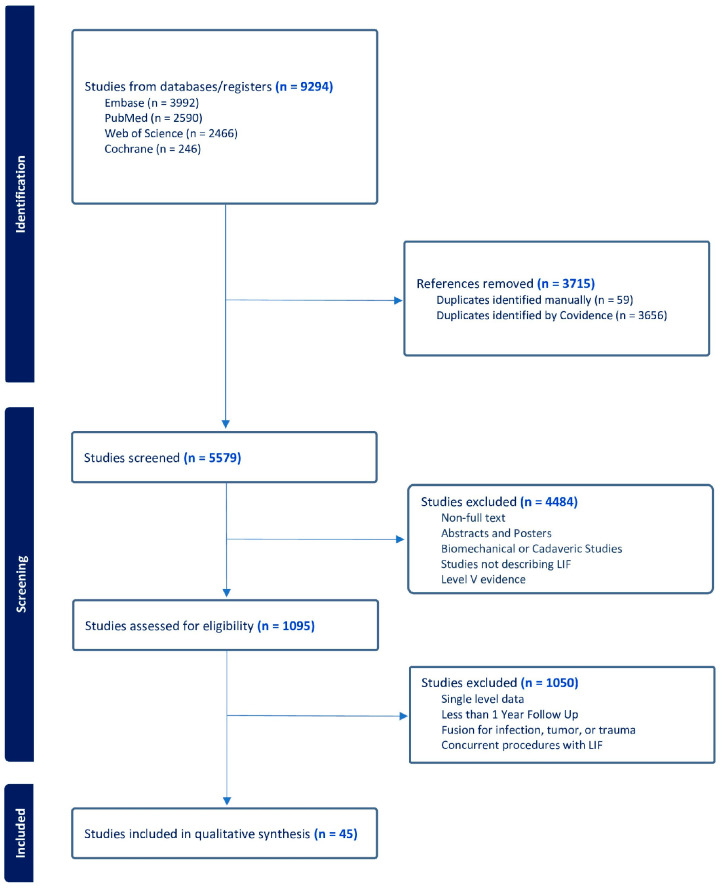 Figure 1
Figure 1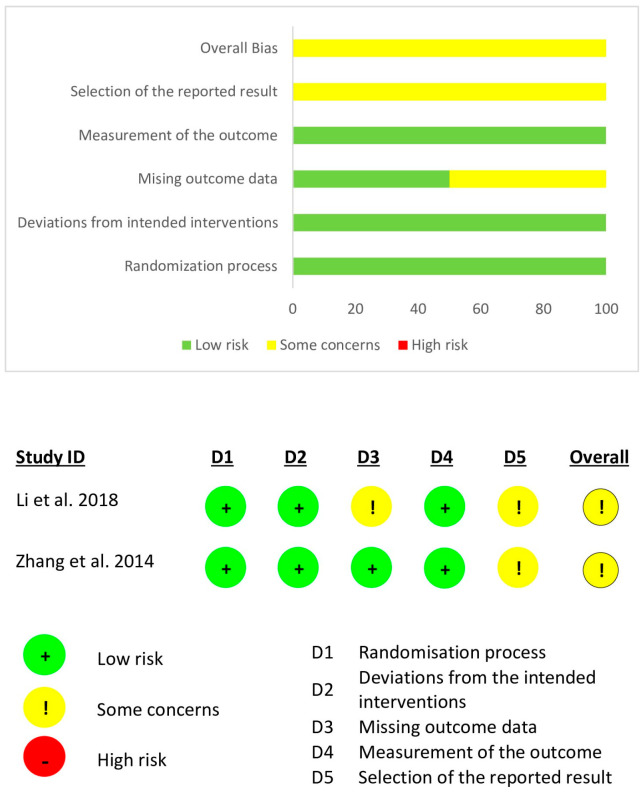 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpine and Intervertebral Disc Pathology · Cervical and Thoracic Myelopathy · Scoliosis diagnosis and treatment
1. Introduction
As a result of documented positive clinical outcome and advancements, the number of spinal fusion procedures has been steadily increasing within the United States [1,2,3]. Further evidenced by a 170.9% increase from 1998 to 2008, the incidence of lumbar fusion procedures grew at an accelerated rate [4]. Lumbar interbody fusion (LIF) specifically has seen increases from 13.6% to 32%, whereas other fusion options, such as posterolateral fusion (PLF), have decreased [5,6,7,8].
Lateral procedures, such as lateral lumbar interbody fusion (LLIF), extreme lateral interbody fusion (XLIF, NuVasive, San Diego, CA, USA), and direct lateral interbody fusion (DLIF, Medtronic, Minneapolis, MN, USA), facilitate sagittal and coronal deformity correction through a lateral retroperitoneal transpsoas approach [9,10,11,12]. Through direct visualization, posterior lumbar interbody fusion (PLIF) can achieve decompression and restoration of interbody height with a single incision but can cause injury due to the retraction of muscles and nerves [10,13,14]. While transforaminal lumbar interbody fusion (TLIF) offers advantages such as reduced risk of injury and bilateral anterior column support via a single unilateral incision, lordosis restoration remains limited [15,16,17]. Oblique lateral interbody fusion (OLIF) proceeds anterior to the psoas but presents similar possibilities of vascular injury seen in the anterior approach [10,18,19,20,21]. While providing an array of tools for the surgeon, an informed consideration of benefits and risks for each LIF procedure is paramount. This is especially true in multilevel procedures, as revision risk increases with greater instrumentation length [22].
While consensus on a superior procedure remains in question, previous reviews have demonstrated the clinical success of varying LIF approaches [23,24,25]. This is limited to single-level procedures, and, to the authors’ knowledge, there is no prior study that has extensively reported on exclusively multilevel LIF procedures. Thus, this systematic review aims to thoroughly present all radiographic and clinical outcomes of lateral and posterior multilevel lumbar interbody fusion in the current literature.
2. Materials and Methods
2.1. Search Strategy and Eligibility Criteria
This systematic review was designed in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines [26] and was not prospectively registered in the International Prospective Register of Systematic reviews (PRISMA 2020 Checklist). A literature search was conducted by two authors using PubMed, Embase, Web of Science, and Cochrane Central Register of Controlled Trials (CENTRAL) from database inception to present. Any conflicts were resolved by the senior author. The literature search can be found in Table S1. Inclusion criteria consisted of level 1–4 studies evaluating outcomes of lateral and posterior LIF of two or more levels, follow-up of at least 1 year, one or more patient-reported outcome measures (PROM), radiographic measurements, postoperative complications, and fusion rates. Studies using LIF with posterior instrumentation were included. Exclusion criteria included any non-full-text articles, biomechanical or cadaver studies, editorial commentaries, review articles, studies reporting fusion for infection or tumor, studies reporting on the use of an additional procedure such as PLF, posterior, or three column osteotomy, and traumatic lumbar spondylolisthesis as defined by Konan et al. [5].
2.2. Data Extraction
The data was extracted from the included studies by two authors and transferred to a Microsoft Excel (Microsoft Corp, Redmond, WA, USA) spreadsheet. The following data was extracted from each study: author name, publication year, level of evidence, demographics, operative details, radiographic outcomes, clinical outcomes, complications, conclusions, and limitations. Complications were delineated as revisions/reoperations, dural tear, adjacent segment disease/degeneration (ASD), symptomatic hematoma, myocardial infarction, psoas weakness, delayed wound healing, deep wound infection, superficial wound infection, pseudoarthrosis, rod fracture/hardware failure, pulmonary embolism, deep vein thrombosis, neurological complications, adjacent disk herniation, urinary tract infection, and all-cause complications not previously listed. All data was reported as mean with standard deviation and range, when possible. When data was presented without a standard deviation, the previously published approaches were used to derive an estimate [27,28]. All radiographic outcomes and PROMs were reported as change values between preoperative and postoperative measurements to assess the effect of the intervention. Due to significant heterogeneity in study design, a meta-analysis was not performed.
2.3. Quality Assessment
Each article underwent independent bias assessment by two authors. Non-randomized studies were assessed using the methodological index for non-randomized studies (MINORS) criteria [29]. Higher scores, indicating reduced bias, allow non-comparative studies to score up to 16 points and comparative studies up to 24 points. Non-comparative study scores were assessed as 0–4 (very low-quality evidence), 5–7 (low-quality evidence), 8–12 (fair-quality evidence), and greater than 13 (high-quality evidence). Comparative study scores were assessed as 0–6 (very low-quality evidence), 7–10 (low-quality evidence), 11–15 (fair-quality evidence), 16–20 (good-quality evidence), and greater than 21 (high-quality evidence). Randomized studies were assessed using the Cochrane risk-of-bias tool for randomized controlled trials (RoB-2) [30].
3. Results
3.1. Study Selection
A comprehensive search of all available lateral and posterior multilevel LIF literature was performed. The query of online databases identified 9294 studies. After initial screening, 1095 full texts were assessed for eligibility, leading to an inclusion of 45 studies (Figure 1).
3.2. Study Characteristics
Of the 45 included studies, two were randomized-controlled-trials (RCT) [31,32], three were prospective cohort studies [33,34,35], 19 were retrospective cohort studies [36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54], and 21 were case series [55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75]. A total of 25 studies reported on TLIF [32,33,34,35,36,37,38,41,42,43,44,52,53,54,58,61,62,63,64,67,68,69,72,73,74], 17 studies reported on PLIF [31,39,40,45,46,47,48,49,51,56,57,59,60,66,70,71,75], four studies reported on LLIF [36,46,55,65], and two studies reported on OLIF [50,52]. With 5623 total patients included, 4318 patients underwent TLIF, 1058 patients underwent PLIF, 110 patients underwent LLIF, and 137 patients underwent OLIF. PLIF reported the longest mean follow-up (48.80 ± 26.74 months), and TLIF followed (33.18 ± 5.67 months), while LLIF and OLIF had comparable shorter follow-up durations (21.40 ± 4.86 and 21.39 ± 12.47 months, respectively). Patients who underwent LLIF (68.63 ± 6.67 years) were slightly older compared to the other LIF cohorts, where mean ages were 61.21 ± 8.24 (PLIF), 61.22 ± 9.77 (TLIF), and 64.68 ± 10.6 (OLIF) years. The number of fused levels was relatively consistent across TLIF and PLIF (2.13 ± 0.33 and 2.13 ± 0.22, respectively), increasing slightly for LLIF (2.27 ± 0.25) and OLIF (2.64 ± 0.6). A detailed summary of reported study and patient characteristics can be found in Table 1. All individual study indications for surgery, surgical details, author conclusions, and limitations can be found in Table S2.
3.3. Pooled Outcomes
3.3.1. Operative Details
The majority of studies reported using PSF to augment the LIF procedure; two studies were exceptions [40,55]. PSF varied significantly with unilateral/bilateral and open/percutaneous placement (Table S2). Similarly, studies used autograft or allograft, with or without the use of bone morphogenic protein (BMP) to aid in arthrodesis. When weighted pooled mean values were analyzed, TLIF demonstrated the shortest operative duration at 198.7 ± 77.83 min and the shortest LOS at 5.09 ± 2.5 days. The LLIF procedure was associated with the lowest reported intraoperative blood loss of 229 ± 125.6 mL despite this value reflecting the total time of the combined LLIF and posterior instrumentation (Table 2).
3.3.2. Patient-Reported Outcome Measures
Three PROMs were reported by a large margin: Oswestry disability index (ODI), visual analog scale (VAS) leg pain, and VAS back pain. The collected TLIF data reported the greatest score improvement across ODI (33.68 ± 6.43), VAS leg pain (5.39 ± 0.66), and VAS back pain (4.67 ± 0.79). A summary of collected PROMs can be found in Table 3; however, no OLIF PROM data was available.
3.3.3. Radiographic Outcomes
Reviewing the pooled radiographic outcome data, the TLIF procedure had the greatest reported changes in thoracic kyphosis (TK) (3.56 ± 3.78°) and sacral slope (SS) (4.67 ± 2.55°). The PLIF procedure had the largest reported changes in pelvic incidence (PI) (1.79 ± 1.4°). The LLIF procedure had the largest reported changes in segmental lordosis (SL) (4.3 ± 1.2°), pelvic tilt (PT) (3.95 ± 0.41°), and pelvic incidence–lumbar lordosis (PI–LL) mismatch (8.01 ± 3.09°). The OLIF procedure had the greatest reported fusion rate (96.7%), as well as the largest lumbar lordosis (LL) (8.1 ± 2.4°) and sagittal vertical axis (SVA) (30.4 ± 32.2°) change; however, only a single OLIF study reported radiographic outcomes (Table 4). The data on the pooled disk height (DH) or foraminal height (FH) restoration was not available by procedure.
3.3.4. Complications
To facilitate comparison, complications were stratified and reported as both total event count and weighted rate (Table S3). From the pooled complication data, the LLIF procedure had the greatest weighted rate of complications (71.11%) and, the PLIF procedure had the lowest weighted rate of complications (13.91%); however the LLIF procedure had substantially less data (patient N = 45). TLIF had a weighted complication rate of 24.83%, and OLIF had a weighted complication rate of 15.33%. All complications in the “Other” category are fully listed with their individual N in Table S4.
3.4. Comparative Outcomes
3.4.1. Procedural Comparison
Chong et al. [36] assessed two-level MIS LLIF and MIS TLIF, finding no differences in operative duration, LOS, or 2-year PROM improvement. The authors found LLIF to be superior for blood loss (229.0 ± 125.6 vs. 302.4 ± 97.1 mL), DH restoration at L3–L4 (4.1 ± 2.4 vs. 1.2 ± 1.9 mm), DH restoration at L4–L5 (3.0 ± 3.5 vs. −0.1 ± 4.4 mm), FH restoration at L3–L4 (3.5 ± 3.6 vs. 1.0 ± 3.6 mm), FH restoration at L4–5 (3.0 ± 3.5 vs. −0.1 ± 4.4 mm), SL (4.1 ± 6.4 vs. −2.1 ± 8.1°), LL (4.1 ± 7.0 vs. −2.3 ± 12.6°) and PI–LL mismatch (4.1 ± 7.0 vs. 2.3 ± 12.6°). Fusion, migration, subsidence, and ASD incidence were not significantly different; however, neurological deficits were more common in LLIF (9 vs. 3).
Nakashima et al. [46] assessed 2-year SL angle, DH, LL, PT, C7 SVA, and TK of PLIF and LLIF. In two-level fusions, LLIF produced greater changes in SL angle (4.8 ± 4.0 vs. 2.6 ± 3.2°), DH (4.0 ± 1.5 vs. 2.4 ± 1.9 mm), LL (8.4 ± 7.0 vs. 2.1 ± 6.7°), and PI–LL (−9.0 ± 7.3 vs. −3.4 ± 7.4). In three-level fusions, LLIF had greater improvement in LL (12.1 ± 11.1 vs. 4.2 ± 9.1°), PI–LL (−11.2 ± 11.3 vs. −3.0 ± 9.3), PT (−6.4 ± 4.9 vs. −2.5 ± 5.3°), and TK (7.8 ± 11.8 vs. −0.3 ± 9.7°).
Yoon et al. [52] assessed radiographic parameters of OLIF and TLIF. The authors found that the OLIF group had greater postoperative cage height (14.3 ± 1.5 vs. 11.5 ± 1.2 mm), cage angle (16.0 ± 5.6 vs. 5.6 ± 2.1), change in anterior DH (6.9 ± 3.2 vs. 4.7 ± 2.9 mm), correction of SL (−13.8 ± 7.5 vs. −7.4 ± 9.1°), and change in disk angle (−9.2 ± 5.2 vs. −5.1 ± 5.1°). The TLIF group had greater changes in posterior DH (2.4 ± 2.6 vs. 1.0 ± 2.4 mm) and FH (1.1 ± 2.8 vs. 0.2 ± 2.9 mm). There were no differences in PI, LL, PI–LL mismatch, PT, SVA correction, or complication rates.
3.4.2. Procedural Techniques
Song et al. [49] assessed PLIF with a cage vs. autogenous bone alone. The authors found no significant differences in leg pain, back pain, ODI, DH, LL correction, fusion rate, instrumentation failure, or subsidence between the two fusion techniques. Li et al. [43] matched TLIF patients with a n-HA/PA66 cage to PEEK cages. The authors reported that the n-HA/PA66 cage had a lower incidence of ASD (14.58% vs. 33.33%); however there were no differences in fusion rate, intervertebral space height, segmental angle, LL, VAS, ODI, or complication rates. Zhao et al. [54] assessed a unilateral vs. bilateral incision for open and percutaneous PSF in the TLIF procedure. Despite increased operative time (163.07 ± 37.94 vs. 147.15 ± 37.96, minutes), estimated blood loss (235.61 ± 88.77 vs. 190.57 ± 73.04, mL), and radiation exposure time (24.13 ± 1.74 vs. 17.71 ± 1.99 s) in the unilateral incision cohort, there were no differences in length of stay or clinical outcomes.
3.4.3. MIS vs. Open TLIF
Gu et al. [33] (248.4 ± 94.3 vs. 576.3 ± 176.2), Lee et al. [42] (527.41 ± 219.66 vs. 865.81 ± 525.09), and Zhang et al. [53] (254.1 ± 23.97 vs. 450.7 ± 36.23) reported that MIS TLIF had less intraoperative blood loss (mL). Gu et al. [33] (9.3 ± 3.7 vs. 12.1 ± 3.6) and Zhang et al. [53] (6 ± 0.92 vs. 8 ± 2.2) reported a shorter length of stay (days) in the MIS cohort, but Lee et al. [42] found no difference. Lee et al. [42] (167.33 ± 37.54 vs. 216.58 ± 40.41) and Zhang et al. [53] (136.3 ± 27 vs. 148.4 ± 32.99) reported shorter operative time (minutes) in MIS, but Gu et al. [33] reported no difference. All authors found no difference in improvement of back pain, leg pain, ODI, fusion, improvement of sagittal parameters, pelvic parameters, or PROMs. Zhang et al. [53] reported that MIS TLIF had a lower complication rate (0% vs. 24.32%).
3.4.4. Unilateral vs. Bilateral Pedicle Screw Fixation Within TLIF
Gu et al. [34] (154.6 ± 22.1 vs. 185.9 ± 27.2), Liu et al. [44] (126.8 ± 25.9 vs. 198.1 ± 36.0), and Zhang et al. [32] (208 ± 36.51 vs. 257 ± 34.79) reported a shorter operative duration (minutes) when using unilateral fixation. Similarly, Gu et al. [34] (190.9 ± 61.0 vs. 256.2 ± 96.8), Liu et al. [44] (247.5 ± 96.4 vs. 345.6 ± 154.9), and Zhang et al. [32] (391 ± 134.75 vs. 546 ± 161.150) reported less blood loss (mL) when using unilateral fixation. Liu et al. [44] and Zhang et al. [32] reported no differences in radiographic or clinical outcomes, whereas Gu et al. [34] found greater improvements in cobb angle of the whole lumbar (2.05 ± 1.15 vs. 1.96 ± 0.81) and lower improvement in whole lumbar lordosis (7.26 ± 2.37 vs. 8.46 ± 2.74) through unilateral fixation.
3.5. Risk of Bias
All non-randomized studies underwent appraisal using the MINORS criteria (Table 1). Five studies were rated as low-quality evidence [57,59,69,72,75], 25 studies were rated as fair-quality evidence [37,38,39,40,45,48,50,51,52,55,56,58,60,61,62,63,64,65,66,67,68,70,71,73,74], and 13 studies were rated as good-quality evidence [33,34,35,36,40,42,43,44,46,47,49,53,54]. All individual MINORS scores can be found in Table 1. Two randomized studies assessed by the Cochrane RoB-2 tool indicated some concerns of bias (Figure 2).
4. Discussion
4.1. Summary of Analysis
The findings of this systematic review provide a comprehensive resource of operative details, as well as radiographic and clinical outcomes within lateral and posterior multilevel LIF techniques, namely the LLIF, OLIF, TLIF, and PLIF procedures. Quantitative procedural comparison of clinical outcomes was not conducted due to significant heterogeneity; therefore, the reported data was aggregated to qualitatively present the current multilevel LIF literature.
4.2. Operative Details
Surgical details were found to be highly heterogeneous. While posterior instrumentation was common, there was significant variation in the placement and decision for unilateral or bilateral fixation, similarly applying to the use of grafts and BMP (Table S2). LLIF was found to have the greatest mean operative duration of 272.8 min, with the lowest being TLIF at 198.7 min; however, limited LLIF data undermines the accuracy of this finding. For example, LLIF operative time may be inflated, as this measurement came from a single study utilizing a lateral-to-prone repositioning for PSF [36]. PLIF had the greatest intraoperative blood loss of 584.67 mL, whereas LLIF had the lowest intraoperative blood loss of 229 mL. While still subject to bias as a result of the low LLIF patient population, this finding aligns with LLIF’s percutaneous approach and minimal extradiscal dissection [76]. However, a lack of control and inherent variability of factors contributing to blood loss must be considered [77]. The reported LOS was found to cluster at extreme values. TLIF (5.09 days) was similar to LLIF (5.5 days), whereas OLIF (12.9 days) and PLIF (14.25 days) had a much longer LOS. While OLIF has limited evidence, the data on the predominantly open PLIF group correlates with recent evidence of increased LOS in non-MIS techniques [78]. The collected operative duration, blood loss, and LOS values resemble data trends from a recently published meta-analysis on LLIF vs. alternatives for treating degenerative spinal conditions [24].
4.3. Patient-Reported Outcome Measures
The collection of PROMs varied significantly, with no apparent standardization. The ODI and VAS pain scales were the greatest reported by a considerable margin; however, all collected PROMs were included for visualization (Table S5). The ODI scores were only reported for TLIF, PLIF, and LLIF, with TLIF having the greatest ODI score gain of 33.68 and LLIF having the lowest score gain of 21.04. Postoperative VAS leg pain score gain was the greatest for TLIF at 5.39, whereas LLIF had the lowest score gain, 1.62. The reported VAS back pain followed a similar trend, with TLIF having the greatest score gain, 4.67, and LLIF having the lowest score gain, 3.58. Interestingly, all score gain differences between LLIF and TLIF either approached or surpassed the MCID of 12.8, 1.6, and 1.2 for ODI, leg pain, and back pain, respectively [79]. However, a lack of statistical analysis precludes conclusions on this difference. These values differ from a meta-analysis finding that LLIF had favorable postoperative ODI scores resistant to change when using meta-regression to assess the influence of operated level [24].
4.4. Radiographic Outcomes
Radiographic outcomes can be further segmented into fusion rates and alignment results. Fusion rates were the greatest for OLIF, 96.7%, and the lowest for TLIF, 92.95%. However, the OLIF results came from one study. The data within this review found that the sagittal alignment parameters showed improvement for all fusion approaches, including lumbar lordosis, pelvic incidence, and SVA (Table 4). While there is currently some literature questioning the correlation of solid arthrodesis with desirable outcomes, the ample data within this review and the PRO score gains surpassing the MCID appeared to support this correlation [80,81,82].
4.5. Complications
As a result of small cohort size, LLIF had a skewed complication rate much higher than other procedures. The complication rates of the OLIF procedure closely resembled those of TLIF and PLIF, for which standard deviations overlapped substantially. As expected, dural tears were more common for PLIF (4.04%) than TLIF (2.91%), and psoas weakness occurred at the greatest rate with LLIF (42.86%). Neurologic complications, defined as weakness or numbness, were much more common in LLIF (33%) and to a lesser extent in PLIF (9.8%). These events were all described as transient episodes with no permanent sequelae, with the exception of one LLIF patient with motor deficits (L2 deficit, MRC grade 4) at the 2-year follow up [36]. Previous research has presented conflicting results. An et al. conducted a meta-analysis on OLIF and PLIF, finding that complications rates were significantly lower in the OLIF than in the PLIF group [23]. In a meta-analysis comparing OLIF and MIS TLIF, Zhang et al. found no differences [25]. When LLIF was compared against posterior alternatives, there was a significant risk reduction in the lateral procedure, which was resistant to meta-regression [24]. Currently, the most high-evidence analyses comparing lateral and posterior LIF procedures contain primarily single-level data with a combination of procedures, which can introduce confounding effects and limit our ability to contextualize multilevel LIF results.
4.6. Procedural Comparison
Within comparative evidence assessing LIF procedures, all three produced similar conclusions of optimal clinical performance through a lateral approach. When comparing MIS LLIF to MIS TLIF, Chong et al. [36] noted lower blood loss, DH, and FH restoration at the cost of increased neurological deficits in the LLIF procedure. The authors state that these results are somewhat expected, as LLIF facilitates disk distraction at the midline, with cages spanning the epiphyseal ring [83]. Notably, LLIF was performed on L3–L5, which could be the cause of the observed favorable LL restoration, although favorable sagittal parameters did not result in an improvement of clinical outcomes.
Assessing 2-year radiographic outcomes, Nakashima et al. [46] found that, in addition to DH, the LLIF procedure outperformed PLIF in both two- and three-level fusions for many radiographic parameters. Similar to Chong et al. [36], the authors agreed that this may be as a result of advantages inherent to LLIF such as access to disk space and endplate preparation. The authors added that LLIF interbody cages are unique in that they provide an extension–distraction moment, permitting the enlargement of the interbody space and DH; however, a 2-year follow up may be too short to see a manifestation of this advantage [84].
Yoon et al. [52] analyzed the OLIF procedure against TLIF; the authors found these results were largely limited to DH, angle, and SL, with no difference in sagittal alignment or complication rates. Despite affirming previously documented findings of increased cage and DH through a lateral approach such as the OLIF procedure, the authors noted no differences in sagittal alignment, attributing this finding to the use of bilateral facetectomies within TLIF, which achieved posterior column shortening and lordosis by rod assembly with compressive force.
4.7. Procedural Techniques
Three studies assessed differences in techniques within multilevel LIF. In PLIF, for two-level isthmic-spondylolisthesis, Song et al. [49] assessed the advantages of a single PEEK cage against the use of autogenous bone in procedures using posterior instrumentation. The authors concluded that despite prior literature indicating the necessity of an interbody cage to restore disk height and supply structural support [85], the use of autogenous bone obtained during decompression performed equally. Li et al. [43] conducted a 6-year minimum follow-up study of n-HA/PA66 vs. PEEK cages for multilevel degenerative disease. The cohorts were matched for demographics, including body mass index (BMI), Charlson comorbidity index (CCI), bone mineral density (via T-score), and excluded patients with preoperative Pfirrmann grades above 3. The authors reported that outcomes remained homogenous; however, the incidence of ASD was twice as high in the PEEK cage cohort, likely as a result of n-HA/PA66’s advantages at the material–tissue interface. Lastly, Zhao et al. [54] assessed the impact of unilateral long or bilateral short decompression incisions when using open and percutaneous pedicle screw fixation within TLIF. The authors reported that a unilateral long incision resulted in a longer operative duration and blood loss with no advantages in LOS or clinical outcomes.
4.8. MIS vs. Open
We examined three studies that compared MIS vs. open TLIF procedure [33,42,53]. All three studies reported a reduction in intraoperative blood loss as a result of MIS, whereas only two studies, respectively, found a difference in length of stay [33,53] and operative time [42,53], favoring MIS TLIF. In all three studies, no operative details favoring MIS translated into an improvement of PROM scores, fusion rates, or radiographic parameters. Zhang et al. [53] found a lower complication rate in the MIS TLIF cohort, stemming from less retraction. This finding may also be attributable to the increased follow-up length of 5 years, in comparison to the 2-year follow up and 1-year follow up in Gu et al. [33] and Lee et al. [42], respectively. When investigating study methodology, all MIS procedures used a single interbody cage compared to two cages in Open TLIF, a disadvantage of MIS TLIF that may affect fusion over a longer follow-up [86,87]. Fusion was homogenously determined by Bridwell’s scale [88], and despite varying this interbody cage difference, both MIS and open groups demonstrated a high fusion rate with a minimal non-significant difference.
4.9. Unilateral vs. Bilateral Pedicle Screw Fixation
We examined three studies comparing unilateral vs. bilateral PSF within the TLIF procedure [32,34,44]. These studies reported a reduction in operative time and blood loss when using unilateral PSF. This finding seems intuitive, as placing more screws and a second rod would require greater operative time and result in increased blood loss. Gu et al. [34] found that the unilateral fixation cohort produced favorable improvements in the whole lumbar cobb angle and unfavorable results in lumbar lordosis; however, the differences in clinical outcomes were strongly non-significant. While fusion rates were non-significant, the assessment methods were found to be somewhat heterogenous: Gu et al. [34] assessed with plain X-rays at 12 months, Liu et al. [44] assessed with assistance of flexion-extension X-rays and CT scans, and Zhang et al. [32] assessed with annual CT scans. While previous literature on LIF has found that flexion–extension X-rays can be a valuable tool in identifying lumbar instability, a lack of standardization and inconsistent use of CT scans limit robust evidence for true differences in fusion rate [89,90].
4.10. Bias Within the Literature
The review process revealed a concerning aspect within the multilevel LIF literature. A vast majority of the literature focused on posterior approaches, with 42 studies, while LLIF and OLIF were only discussed in six. This may be due to the technical nature of LLIF and OLIF in addressing complex multilevel pathology; however, LLIF publications are increasing at an accelerating rate [91]. Additionally, 21 of the included studies were level 4 evidence. Individual study bias analysis with the MINORS tool found that most included studies were low- or fair-quality evidence, whereas a minority were classified as good-quality. Similarly, some concerns of bias were found in both included RCTs. Beyond an apparent publication bias favoring the posterior LIF approaches, the assessment of study quality further highlights the deficiencies within the available evidence. While a few outcomes indicated favorable results through lateral approaches, there is a lack of evidence to definitively claim a broadly superior procedure between LIF alternatives. Furthermore, as operative level is often pooled, the literature limits subgroup analysis to determine optimal clinical benefit within a specified lumbar segment.
4.11. Cost
If heterogeneity of outcomes continues to limit the ability to determine a broadly favorable LIF procedure, attention can be shifted towards cost reduction. At a 2-year time horizon, TLIF had a favorable cost–utility metric (lower cost/QALY) when considering direct costs of the procedure; however, LLIF became more favorable when indirect costs such as productivity loss were included [92]. A subgroup analysis was conducted on MIS vs. open procedures finding that at a time horizon of 1 year, MIS was favorable, but when the time horizon was extended to 2 years, the costs approached similarity [93,94]. This suggests that there is an immediate quality-of-life benefit as a result of reduced blood loss or LOS, findings that were applicable to the multilevel LIF literature.
4.12. Limitations and Future Research
This study is not without limitations. Although this study utilized strict exclusion criteria, multilevel LIF literature is inherently heterogenous. This limited our ability to quantitatively compare the LLIF, OLIF, TLIF, and PLIF procedures. Furthermore, inconsistent reporting and a publication bias within the literature increases the difficulty of reporting accurate values on LLIF and OLIF. This is especially apparent within the OLIF literature, where reported procedural characteristics and outcome values come from a very limited dataset. Limited reporting of consistent clinical outcomes is a substantial limitation of the multilevel LIF literature and present study, substantially weakening conclusions regarding the clinical effectiveness of the procedures. This was notable for PROMs, where almost the entirety of the evidence was within the TLIF and PLIF cohorts. Clinical heterogeneity within surgical techniques, assessment of radiographic outcomes, and level 4 evidence introduced bias into the reported pooled outcomes. Heterogeneity of included studies limited the ability for further subgroup analysis by study quality beyond the stratification completed within the present study. Additionally, there was significant variation in clinical indications across the included studies and further stratification by indication was not methodologically feasible. This significantly limits the ability to draw meaningful conclusions by surgical approach or indication. It is important to note that a lack of intersection between level 3 or higher evidence across the collected outcomes necessitated the inclusive nature of the pooled outcomes. As higher-level of evidence studies did not consistently report on the same variables, a reliance on level 4 evidence was required to provide a comprehensive overview of the current clinical landscape.
Future studies should prioritize quantitative procedural comparison on a subset of high-level evidence to ensure that conclusions can remain robust by employing study designs such as randomized controlled trials or multicenter prospective cohorts. These studies should leverage the comprehensive data gaps identified through our exhaustive search and grouping of the available literature as a roadmap to target specific approaches and indications, thereby providing the high-level evidence necessary to impact clinical decision-making. Similarly, future studies can expand their investigation to the anterior procedure (ALIF) or segment analysis by operated levels. Future reviews can prioritize high-quality evidence of lateral procedures to reduce bias or confounding effects. As future studies look to iterate on the limitations of the present data and study, emergent technology within lumbar interbody fusion can be considered in conjunction. Recent literature has investigated the use of robotic assistance within lumbar procedures, finding that robot guidance can outperform freehand and CT-guided placement of pedicle screws [95,96], with evidence indicating a reduction in surgical revision due to screw mispositioning [95]. Both meta-analyses call for high-level evidence to further confirm the benefits of robotic assistance.
5. Conclusions
While this comprehensive review identified significant heterogeneity, it is the first to consolidate all reported outcomes in the current multilevel LIF literature. Despite pooled outcome measures favoring the TLIF procedure, a publication bias towards posterior LIF approaches was observed. Conversely, available comparative evidence contradicted these pooled findings, reporting advantages for the LLIF and OLIF procedures over their posterior counterparts. Given the inconsistent evidence, results should be interpreted with caution. It is essential that future research utilizes robust study design to provide data and render insight to aid clinical decision-making of lumbar interbody fusion for multilevel pathology.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ilyas H. Udo-Inyang I. Savage J. Lumbar Spinal Stenosis and Degenerative Spondylolisthesis: A Review of the SPORT Literature Clin. Spine Surg.20193227227810.1097/BSD.000000000000084131145150 · doi ↗ · pubmed ↗
- 2Bae H.W. Rajaee S.S. Kanim L.E. Nationwide trends in the surgical management of lumbar spinal stenosis Spine 20133891692610.1097/BRS.0b 013e 3182833 e 7c 23324922 · doi ↗ · pubmed ↗
- 3Sheikh S.R. Thompson N.R. Benzel E. Steinmetz M. Mroz T. Tomic D. Machado A. Jehi L. Can We Justify It? Trends in the Utilization of Spinal Fusions and Associated Reimbursement Neurosurgery 202086 E 193E 20210.1093/neuros/nyz 40031574148 · doi ↗ · pubmed ↗
- 4Rajaee S.S. Bae H.W. Kanim L.E. Delamarter R.B. Spinal fusion in the United States: Analysis of trends from 1998 to 2008 Spine 201237677610.1097/BRS.0b 013e 31820 cccfb 21311399 · doi ↗ · pubmed ↗
- 5Konan L.M. Davis D.D. Mesfin F.B. Traumatic Lumbar Spondylolisthesis Stat Pearls Stat Pearls Publishing Treasure Island, FL, USA 202528846300 · pubmed ↗
- 6Resnick D.K. Choudhri T.F. Dailey A.T. Groff M.W. Khoo L. Matz P.G. Mummaneni P. Watters W.C. Wang J. Walters B.C. Guidelines for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 7: Intractable low-back pain without stenosis or spondylolisthesis J. Neurosurg. Spine 2005267067210.3171/spi.2005.2.6.067016028735 · doi ↗ · pubmed ↗
- 7Briggs H. Milligan P.R. Chip fusion of the low back following exploration of the spinal canal J. Bone Jt. Surg. Am.194426125130
- 8Kepler C.K. Vaccaro A.R. Hilibrand A.S. Anderson D.G. Rihn J.A. Albert T.J. Radcliff K.E. National trends in the use of fusion techniques to treat degenerative spondylolisthesis Spine 2014391584158910.1097/BRS.000000000000048624979276 · doi ↗ · pubmed ↗