Oral Health Trends and Challenges in North and West Africa: A Systematic Review of Cross-Sectional Studies
Rocío Trinidad Velázquez-Cayón, Juliana Cassol Spanemberg, Ana del Toro Arencibia, Elena Sirumal, Susell Parra-Rojas

TL;DR
This review highlights poor oral health in North and West Africa, driven by inequality and reactive care, and calls for prevention-focused, integrated healthcare systems.
Contribution
The paper systematically reviews cross-sectional studies to reveal structural oral health challenges and proposes policy shifts for equitable care.
Findings
Localized caries prevalence in children reaches 74% in the region.
Adults show high levels of periodontal issues like calculus and gingival bleeding.
Low-SES populations rely on traditional remedies or emergency extractions due to access barriers.
Abstract
What are the implications of the main findings? There is a critical need to transition from current symptom-driven, extraction-oriented dental care models toward integrated, primary care systems focused on prevention and tooth-preserving interventions.Future public health policies must prioritize the standardization of epidemiological reporting and the inclusion of patient-centered metrics to effectively address structural inequalities and reduce the oral health burden in the region. There is a critical need to transition from current symptom-driven, extraction-oriented dental care models toward integrated, primary care systems focused on prevention and tooth-preserving interventions. Future public health policies must prioritize the standardization of epidemiological reporting and the inclusion of patient-centered metrics to effectively address structural inequalities and reduce the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
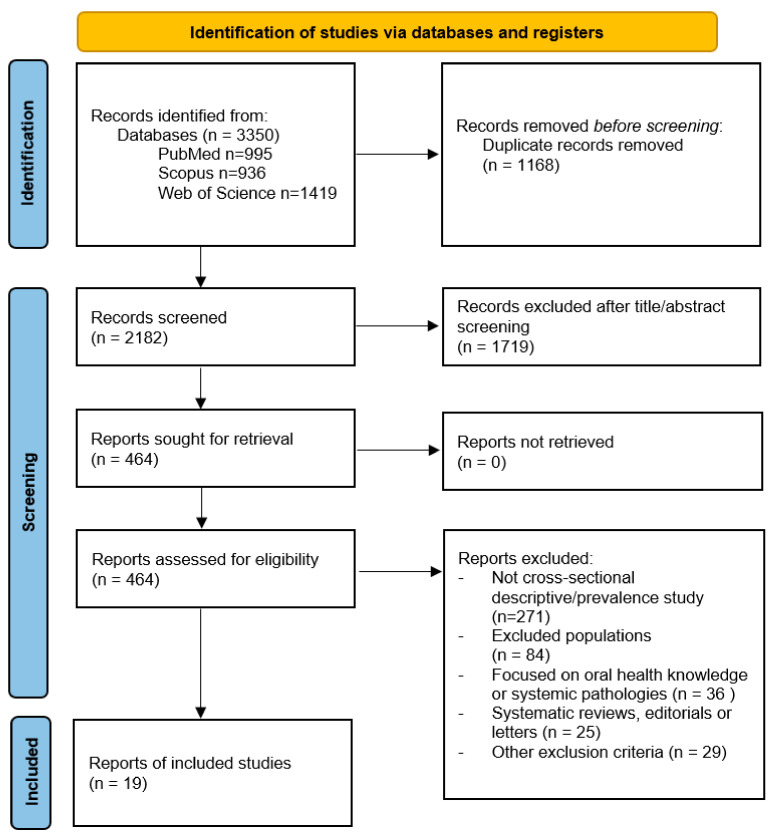 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental Health and Care Utilization · Oral microbiology and periodontitis research · HIV/AIDS oral health manifestations
1. Introduction
The World Health Organization (WHO) emphasizes the importance of oral health, as it not only contributes to the functional capacity of mastication and phonation but also constitutes an essential component of overall health and well-being [1]. Moreover, the implementation of appropriate preventive and therapeutic measures to address oral diseases is a determining factor, since it can prevent serious complications such as systemic infections, cardiovascular conditions, and potential complications during pregnancy [2]. Consequently, the promotion of oral health emerges as a priority within the field of public health. Currently, oral diseases pose a global public health challenge, as the high incidence of oral diseases contributes to a negative impact on individual’s quality of life [1,2,3,4]. The concept of oral health-related quality of life involves considering not only physical aspects such as pain or functional changes but also emotional and social dimensions associated with oral health. Its direct influence on quality of life is noteworthy, as it may lead to functional, aesthetic, nutritional, and psychological problems [5,6].
Africa exhibits profound disparities across its population segments in wealth levels, overall well-being, healthcare accessibility, and educational achievements. These contrasts are mirrored in the substantial economic heterogeneity across African nations, characterized by stark economic and tribal divides, alongside sparsely distributed rural communities juxtaposed against densely populated urban centers [7,8].
Widespread poverty remains a major challenge across many African countries, where high levels of undernutrition coexist with a substantial burden of endemic and water borne infectious diseases. Limited access to safely managed drinking water, inadequate sanitation and poor hygiene practices, including oral hygiene, further amplify the risk of preventable morbidity and mortality. These conditions are frequently aggravated by weak governance and episodes of political instability, which undermine health systems, disrupt education and constrain investments in basic infrastructure. Addressing these challenges requires integrated and collaborative, multisectoral strategies that simultaneously target poverty reduction, nutrition, water and sanitation, and health system strengthening to improve living conditions and population health in African settings [9,10].
The United Nations has utilized this division of Africa into geographical regions for statistical and organizational purposes since the creation of the United Nations Statistics Division (UNSD) in 1947. This classification has been maintained and periodically updated since then. The latest update to the United Nations geographical region map for Africa, which includes the division into regions such as Northern Africa, Western Africa, Eastern Africa, Central Africa, and Southern Africa, was carried out in 1999. It is responsible for collecting, processing, and disseminating statistical information for the UN. This geographical region map, created and updated in 2024, serves purposes of statistical analysis [11].
West Africa is widely recognized as one of the world’s poorest regions, concentrating a very high share of the global multidimensionally poor population despite representing only a fraction of the world’s inhabitants. Analyses based on the Global Multidimensional Poverty Index show that more than half of people in African countries are multidimensionally poor, with particularly high headcount ratios in West African settings, and that the vast majority of these poor individuals live in rural areas [9,10].
Although oral diseases are not commonly fatal, they represent a major public health problem due to their high incidence and significant impact on overall health. These conditions result from various modifiable risk factors common to many non-communicable diseases (NCDs), such as sugar consumption, tobacco and alcohol use, and poor oral hygiene, along with their underlying social and economic associated factors [12,13,14,15].
The WHO 2022 Global Oral Health Report estimates that approximately 3.5 billion people worldwide suffer from oral diseases, with three-quarters residing in middle-income countries. The prevalence of major oral diseases continues to rise globally due to increasing urbanization and changes in living conditions, primarily driven by lack of fluoride exposure, the availability and accessibility of sugar-rich foods, and limited access to community oral care services [1].
Dental caries is the most prevalent oral disorder, with observed increases in incidence across numerous African countries in recent years. Recent epidemiological studies in developing countries suggest that the prevalence and severity of dental caries have risen with industrialization and the adoption of Western diets. Income levels can indirectly influence caries susceptibility, as lack of economic resources, often linked to lower education levels and harmful health habits, as well as limited access to healthcare information, correlates with higher caries incidence. Additionally, low parental education can hinder access to and understanding of oral disease prevention importance [15,16].
To provide a comprehensive overview of oral health in North and West Africa, the following specific objectives were established:
- To determine the prevalence and severity of the most common oral conditions—dental caries, periodontal diseases, and tooth loss—among different age groups in the country.
- To analyze the association between oral health status and socioeconomic, behavioral, and contextual associated factors, such as education, urban–rural residence, and oral hygiene practices.
2. Materials and Methods
2.1. Protocol Recording
The review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [17] (Supplementary File S1: PRISMA checklist), and the study protocol has been registered in the PROSPERO database under identification number CRD420261283702.
2.2. Focused Question
“What is the oral health status in North and West Africa, and what are the most prevalent oral health conditions in this region?”
2.3. Eligibility Criteria
In this systematic review, the following inclusion and exclusion criteria were established, with included studies organized into two categories for presenting results: cross-sectional descriptive studies describing the most prevalent oral health conditions through intraoral and extraoral examinations and their relationship with socioeconomic and cultural factors, and studies evaluating or complementing oral health status information through self-perception surveys.
Among the exclusion criteria are studies analyzing and/or comparing different oral health plans in North and West African countries, systematic reviews, editorials, letters to the editor, studies linking oral health with other systemic pathologies, studies specific to pregnant women, studies on institutionalized individuals such as those in orphanages or prisons, studies on cohorts in very isolated locations, studies analyzing the oral health status of migrant or refugee individuals in the host country, studies with samples consisting of health professionals or health science students, and studies focusing on evaluating the population’s level of knowledge regarding oral health.
2.4. The CoCoPop Strategy
The CoCoPop strategy was selected [18] as it is more appropriate for prevalence and population-level observational studies, allowing a comprehensive identification of relevant evidence by clearly defining the health condition of interest (Condition), the study setting or environment (Context), and the target population (Population):
- -Condition: Oral health outcomes included in the review.
- -Context: African countries included in the review.
- -Population: Adults, adolescents and children.
2.5. Information Sources and Search Strategy
The bibliographic search, conducted in October 2025, encompassed databases such as PubMed, Web of Science and Scopus. Employing Medical Subject Headings (MeSH) in combination with Boolean operators “AND” and “OR”, a tailored search strategy was adapted for each database (Supplementary File S2: Database search strategy).
2.6. Data Collection Processing and Data Items
Data collection was performed by two independent reviewers (A.T.A. and R.T.V.C.), using a piloted extraction form developed from the review objectives and CoCoPop framework, with a third reviewer (S.P.R) resolving discrepancies. The Kappa concordance test yielded a coefficient of 0.80, indicating considerable agreement and reinforcing the reliability of the study selection process. For each eligible study, data were extracted and organized into a standardized table covering: bibliographic information (author, year), study design, setting/country, population characteristics (age range, sample size), measurement instruments, clinical and self-reported outcomes, and socioeconomic status (SES) indicators. Clinical indices included the Decayed, Missing, and Filled Teeth index (dmft /DMFT), Community Periodontal Index of Treatment Needs (CPITN/CPI), and Oral Hygiene Index-Simplified (OHI-S).
In addition, information was collected on the main oral conditions and outcomes reported (prevalence and/or severity of dental caries, periodontal conditions, tooth loss and other relevant oral pathologies), indicators of socioeconomic position (education, occupation, asset based indices, social class, urban–rural residence) and behavioral or contextual variables (toothbrushing practices, use of fluoridated toothpaste, sugar consumption, tobacco use, dental attendance and type of provider). When available, measures of association between oral health outcomes and socioeconomic or behavioral factors, as well as key conclusions related to inequalities in oral health, were also recorded to facilitate the subsequent narrative synthesis.
2.7. Study Risk of Bias Assessment
The methodological quality of the studies followed the Joanna Briggs Institute (JBI) critical evaluation tool for checklist for cross sectional studies [18]. The following critical evaluation criteria were considered:
- Were the criteria for inclusion in the sample clearly defined?
- Were the study subjects and the setting described in detail?
- Was the exposure measured in a valid and reliable way?
- Were objective, standard criteria used for measurement of the condition?
- Were confounding factors identified?
- Were strategies to deal with confounding factors stated?
- Were the outcomes measured in a valid and reliable way?
- Was appropriate statistical analysis used?
Each study was independently assessed. For synthesis, an overall risk of bias category was assigned according to the pattern of JBI responses: studies with “yes” on most key items (particularly clear inclusion criteria, valid and reliable exposure and outcome measures, explicit identification and statistical control of confounders, and appropriate analyses) were classified as low risk of bias; studies with some concerns (for example, incomplete reporting or partial handling of confounding or measurement issues) were classified as moderate risk; and studies with multiple “no” or “unclear” ratings on core domains were classified as high risk of bias.
2.8. Effect Measures
Given the descriptive, cross-sectional design, effect measures focused on quantifying disease burden and characterizing the relationship between oral health and contextual factors.
Oral health status and the most prevalent conditions were described using clinical metrics such as the frequency and severity of dental caries (measured by dmft/DMFT/deft indices), periodontal conditions (including bleeding on probing, calculus, and periodontal pockets categorized via CPITN or CPI), and tooth loss (quantified by the number of missing teeth or the prevalence of partial and complete edentulism).
The relationship between oral health status and socioeconomic, behavioral, or contextual variables was described through measures of association reported by the original studies. This included comparisons across categories of education, parental occupation, asset-based indices, and urban–rural residence, as well as oral health behaviors (e.g., toothbrushing frequency, sugar consumption) and care-seeking patterns. Due to the substantial heterogeneity in study populations, age groups, and diagnostic criteria, these measures were synthesized narratively and organized by life stage (children, adolescents, and adults) and type of outcome (clinical versus self-perceived) to ensure clinical relevance.
2.9. Synthesis Methods
A narrative synthesis of the selected studies was conducted. The qualitative synthesis was conducted in a structured manner using the study characteristics and outcomes summarized in the extraction table. First, the included studies were grouped according to the two prespecified categories: clinical findings and disease burden and self-reported oral health and behaviors.
Due to the significant heterogeneity observed in study populations, age groups, and diagnostic criteria across the included studies, findings were structured and compared by life stage (categorizing results into children, adolescents, and adults) to ensure clinical relevance and facilitate the identification of age-specific oral health patterns in the region.
3. Results
3.1. Literature Search and Selection
A total of 3350 records were identified through database searches: 995 from PubMed, 936 from Scopus, and 1419 from Web of Science. After removing 1168 duplicate records, 2182 unique titles and abstracts were screened, resulting in the exclusion of 1719 records that did not meet the initial eligibility criteria.
Of the 464 reports sought for retrieval, all were successfully retrieved and assessed for eligibility. During this phase, 445 reports were excluded for the following reasons: 271 were not cross-sectional descriptive or prevalence studies; 84 involved excluded populations; 36 focused on oral health knowledge or systemic pathologies; 25 were systematic reviews, editorials, or letters; and 29 met other specific exclusion criteria. Following this rigorous selection process, a total of 19 studies were included in the systematic review (Figure 1).
3.2. Characteristics of Included Studies
The 19 included cross-sectional studies (Table 1) were published between 1999 and 2023 [19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37], providing a comprehensive overview of oral health trends over more than two decades in North and West Africa. The geographical distribution encompassed several low- and middle-income countries, specifically Algeria, Burkina Faso, Egypt, Ghana, Niger, Nigeria, and Tunisia.
Most investigations were school-based surveys focusing on the pediatric and adolescent population. Others utilized community-based population surveys or household-based cross-sectional designs to assess adults and families in their natural living environments. A smaller but significant proportion of the evidence was derived from secondary analyses of national data, such as the WHO STEPwise approach to surveillance (STEPS) and national oral health surveys. Additionally, clinic-based series were employed to analyze specific treatment-seeking patterns, while national pathfinder surveys were used to provide a broad diagnostic overview of oral health status. Sample sizes showed significant heterogeneity, reflecting both local and national scopes. These ranged from smaller, localized cohorts, such as 369 Egyptian children and 496 Nigerian adults, to large-scale national representative samples, including 4677 Burkinabe adults, 5954 Egyptian adults, and 6989 Algerian adults.
Regarding assessment methodologies, oral health conditions were predominantly measured using standard clinical indices established by the World Health Organization (WHO). The dmft/DMFT was the primary measure for dental caries, while periodontal status was assessed through the Community Periodontal Index of Treatment Needs (CPITN/CPI) and oral hygiene through the Simplified Oral Hygiene Index (OHI-S).
The primary exposures and contextual factors analyzed across the studies included socioeconomic position (attained education, parental occupation, and urban–rural residence), health behaviors (frequency of toothbrushing, use of fluoridated toothpaste, and tobacco use), and healthcare-seeking patterns, frequently highlighting a predominance of emergency-driven, extraction-oriented care over preventive dental visits.
3.3. Clinical Findings and Disease Burden
In studies based on clinical examination [19,20,21,22,23,25,26,27,28,29,30,32,33,35,36], caries experience in children showed a wide range of prevalence, with a substantially higher burden in the primary dentition compared to low-to-moderate mean dmft/DMFT scores in the permanent teeth. National and local surveys revealed that approximately half of the schoolchildren were affected by dental caries, with a high proportion of lesions remaining untreated. Specifically, localized studies in Egypt and Nigeria reported caries prevalence rates of 74% and 24.6% among children and adolescents, respectively, reflecting significant regional variations.
Across adolescent and adult populations, clinical data consistently demonstrated a combination of untreated caries, high levels of calculus, and gingival bleeding. There was a considerable prevalence of periodontitis and clinical attachment loss, particularly among older adults. Furthermore, clinic-based samples highlighted a clear predominance of symptom-driven, extraction-oriented care, indicating a lack of preventive or restorative focus. These clinical patterns were documented in both urban and rural settings and were frequently associated with a limited oral health workforce and poor service availability, underscoring substantial unmet treatment needs in the region.
3.4. Self-Reported Oral Health and Behaviors
In studies primarily based on self-reported measures [20,24,31,34,37], a significant proportion of adolescents and adults rated their oral health as poor or very poor.
Regarding oral hygiene practices, while daily toothbrushing was common, the frequency and quality of these habits varied. Participants frequently reported chewing difficulties and impaired. For instance, although 69.1% of adults in certain West African urban settings reported brushing twice daily, consistent use of fluoridated toothpaste and regular dental attendance remained infrequent across the region. In children, hygiene habits were strongly influenced by parental education and SES; lower parental education was directly associated with decreased brushing frequency and a higher burden of caries. Furthermore, a notable reliance on traditional cleaning methods persists, such as the use of chewing sticks (miswak), which are still preferred by a sizeable portion of the population for their perceived antibacterial properties and cultural relevance.
Self-reported data on healthcare-seeking patterns further revealed profound inequalities. Households with lower-SES were more likely to rely on home remedies, traditional healers, or non-dentist providers, often resulting in extractions as the primary solution for advanced caries. Conversely, more advantaged groups reported higher attendance at private dental clinics and access to a broader range of restorative treatment options. These disparities underline a clear social gradient where education, income, and urban–rural residence act as major associated factors of oral health outcomes in North and West Africa.
3.5. Socioeconomic Determinants and Oral Health Inequalities
Clinical patterns of untreated caries and periodontal disease were documented in both urban and rural settings, yet they were frequently exacerbated in contexts of limited oral health workforce and service scarcity, as noted in studies from Nigeria and Burkina Faso [25,34].
Social gradients were clearly visible through indicators such as education, income, and urban–rural residence [30,33]. In children, lower parental education was a significant predictor of higher caries prevalence and poorer hygiene habits [30]. Furthermore, self-reported data on care-seeking revealed that lower-SES households were more likely to rely on traditional remedies, such as chewing sticks or “miswak”, non-dentist providers, or emergency extractions to manage pain [25,36]. In contrast, more advantaged groups reported more frequent attendance at private dental clinics and access to a wider range of tooth-preserving treatment options [27,28]. These findings underscore substantial unmet treatment needs and the persistent challenge of shifting from emergency-driven models to preventive, equity-oriented care in the region.
3.6. Risk of Bias Assessment
Identification and handling of confounding factors (items 5 and 6) was the main methodological limitation identified across the included studies. Recent national surveys and studies employing robust multivariable analyses, such as Hewlett et al. 2022 [36], Aly et al. 2020 [30], Diendéré et al. 2022 [34], Abou El Fadl et al. 2021 [33], Uguru et al. 2021 [31], Pengpid et al. 2023 [37], and Varenne et al. 2011 [26], explicitly pre-specified sociodemographic and behavioral confounders and adjusted for them, leading to a Yes rating on both items and an overall low risk of bias (Table 2).
In contrast, older descriptive surveys, clinic-based series, or studies focusing primarily on bivariate correlations—including Agbelusi et al. 2007 [25], Abbass et al. 2019 [29], Abid et al. 2004 [22], Bruce et al. 2002 [21], Varenne et al. 2005 [23], Petersen et al. 1999 et al. [19], and Ojofeitimi et al. 2007 [24]—often reported sociodemographic variables without formally defining them as confounders or systematically adjusting for them in the final analysis. Consequently, these were rated Unclear for items 5 and 6 and judged to have a moderate risk of bias. Statistical analyses (item 8) were generally appropriate across the board, as most studies utilized regression models or stratified analyses aligned with their specific objectives (Table 2).
4. Discussion
This systematic review aimed to comprehensively analyze the oral health status across North and West African regions by identifying the most prevalent oral diseases and their associated socioeconomic and cultural factors. In addition, it sought to examine the main barriers limiting access to oral healthcare services, the available resources for prevention and treatment, and the methodological approaches adopted in studies conducted within these settings. Our findings, derived from 19 cross-sectional studies published between 1999 and 2023 (no eligible studies were identified for 2024–2025), reveal a substantial burden of unmet dental needs and structural inequalities.
In studies based on clinical examination, a substantial burden of oral disease was evident from early ages, characterized primarily by high proportions of dental caries in the primary dentition, with prevalence reaching 74% in localized samples, and a low therapeutic index that leaves many lesions untreated in both dentitions. Furthermore, periodontal health was consistently compromised across adolescents and adults, who exhibited frequent calculus deposits, gingival bleeding, and clinical attachment loss, alongside a considerable prevalence of tooth loss and a predominance of symptom-driven, extraction-focused treatment patterns. Across several settings, the distribution of these oral conditions was closely linked to structural and social disadvantage, including rural poverty and marked imbalances in the oral health workforce.
Regarding self-reported oral health and behaviors, the evidence highlighted recurring patterns of poor self-rated oral health and impaired quality of life, particularly among older adults. Although basic daily hygiene was commonly reported, the recommended twice-daily brushing and the consistent use of fluoridated toothpaste remained infrequent, showing clear social gradients by education and income. Moreover, recent dental attendance was uncommon due to economic and geographic barriers, leading lower-SES households to rely frequently on traditional remedies, such as chewing sticks (miswak), or non-dental providers to manage caries episodes. These findings underscore a persistent challenge in shifting from emergency-driven responses toward preventive and equity-oriented models of care in the region.
An international web-based survey by John MK et al. [38] involving 1580 dentists reinforced that effective interventions should be evaluated not only on clinical indicators but also on their impact on function, pain, aesthetics, and psychosocial well-being. The assessment of oral health-related quality of life has established itself as a valid tool for diagnosis and treatment planning, allowing for the prediction of patient adherence based on individual perceptions and expectations [39].
The scoping review by Carrasco-Labra et al. [40] examined the barriers and facilitators for oral health policies in the WHO African region, emphasizing that understanding these factors is crucial for improving the efficiency of health systems and the quality of health outcomes. Access to oral health services varies considerably between countries and is largely demand-driven rather than a result of rigorous planning. Globally, oral health care is primarily provided by private professionals, covering only a small portion of health needs [41,42]. In low-income countries, professionals tend to concentrate in urban areas, leaving a significant part of the population with limited access to primary care. Cost remains a major obstacle to accessing these services [43].
Health programs play a crucial role in population well-being. Ghotane et al. [44] conducted a program in Sierra Leone that revealed a lack of qualified personnel, estimating a need for 27 to 163 dental therapists to satisfy population requirements. Adeniyi et al. [45] examined the Nigerian oral health system, demonstrating that it did not respond effectively to population needs due to poor management. Furthermore, Folayan et al. [46] addressed the prevalence and consequences of dental caries in Nigerian children, finding that limited access due to economic and structural barriers resulted in low service utilization.
Only 54% of the African population utilizes dental and preventive services [11]. Due to the lack of resources and medical facilities, the population has minimal access to oral care, leading to high levels of preventable diseases [13,47]. Understanding the situation in their home countries is essential to evaluate how oral health conditions interfere with the quality of life of individuals in a continuous migration environment [40]. The urban–rural asymmetry and high costs associated with dental care represent significant barriers, often resulting in unaffordable out-of-pocket expenses [43,48,49].
Across the available studies, consistent trends emerged of a substantial burden of untreated caries and periodontal conditions from childhood into adulthood, accompanied by low therapeutic indices and care patterns dominated by pain-driven, extraction-oriented treatment.
These findings highlight key challenges for oral health systems, including persistent inequalities and the difficulty of shifting toward preventive, person-centered models of care. These oral health systems are characterized by a lack of rigorous planning and a predominantly demand-driven approach. Access is severely limited by a marked urban–rural asymmetry, where professionals and services are concentrated in metropolitan areas, leaving rural populations with minimal access to primary care. Furthermore, systemic issues such as poor management and a critical shortage of qualified personnel—as evidenced in countries like Nigeria and Sierra Leone [44,45]—hinder the necessary transition from emergency-driven extractions toward effective, preventive models. Overcoming these structural barriers and high out-of-pocket costs is essential to ensure that oral health is integrated into general health equity. At the policy level, there is an urgent need to integrate oral health into general primary healthcare frameworks and to prioritize the standardization of epidemiological reporting to effectively monitor and address structural inequalities. Furthermore, national health agendas must focus on improving the distribution of the oral health workforce and reducing out-of-pocket costs to ensure access for the most vulnerable populations. Regarding clinical practice, dental professionals and health systems should transition from a reactive, extraction-oriented culture toward preventive and tooth-preserving interventions.
5. Limitations
Notwithstanding these constraints, this review provides a comprehensive synthesis of the contemporary oral health landscape in a region characterized by rapid demographic and social transitions. By focusing on evidence published since the late 1990s, the findings offer a reliable baseline for understanding current disease trends and the structural barriers to care. However, the identified gaps in standardized reporting and longitudinal data call for a more harmonized approach in future epidemiological research. The methodology of this study was designed to assess the oral health status of representative national populations across various age groups, noting that studies prior to 1999 were difficult to access and highlighting a lack of research meeting these criteria since 2023. A significant limitation identified in the analyzed evidence is the inconsistent identification and handling of confounding factors, particularly in older descriptive and clinic-based studies. Many of these investigations failed to formally define or systematically adjust for sociodemographic variables in their analyses, which may affect the robustness of the observed associations. To guide future research and improve the quality of evidence for public health policy, it is imperative to adopt harmonized epidemiological approaches that utilize longitudinal designs and standardized reporting metrics, such as Oral Health-Related Quality of Life (OHRQoL).
6. Conclusions
These findings highlight a critical paradox in the North and West African regions: while basic oral hygiene is a recognized social norm, the clinical reality is dominated by advanced, untreated pathology and a persistent reliance on emergency extractions. The deep-seated inequalities identified, driven by geography, education, and economic status, underscore that current oral health systems are failing to reach the most vulnerable populations. Consequently, the fundamental challenge for the region lies in dismantling the existing symptom-driven culture.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization Global Oral Health Status Report 2022 World Health Organization Geneva, Switzerland 2022
- 2Fiorillo L. Oral Health: The First Step to Well-Being Medicina 20195567610.3390/medicina 5510067631591341 PMC 6843908 · doi ↗ · pubmed ↗
- 3World Health Organization Global Strategy and Action Plan on Oral Health 2023–2030 World Health Organization Geneva, Switzerland 2023
- 4World Health Organization The World Health Organization Quality of Life assessment (WHOQOL): Position paper from the World Health Organization Soc. Sci. Med.1995411403140910.1016/0277-9536(95)00112-K 8560308 · doi ↗ · pubmed ↗
- 5Sischo L. Broder H.L. Oral health-related quality of life: What, why, how, and future implications J. Dent. Res.2011901264127010.1177/002203451139991821422477 PMC 3318061 · doi ↗ · pubmed ↗
- 6Slade G.D. Oral health-related quality of life is important for patients, but what about populations?Community Dent. Oral Epidemiol.201240394310.1111/j.1600-0528.2012.00718.x 22998303 PMC 3652582 · doi ↗ · pubmed ↗
- 7Oke G.I. Sibomana O. Understanding Health Inequality, Disparity and Inequity in Africa: A Rapid Review of Concepts, Root Causes, and Strategic Solutions Public Health Chall.20254 e 7004010.1002/puh 2.7004040496105 PMC 12039359 · doi ↗ · pubmed ↗
- 8Caleyachetty R. Kumar N.S. Bekele H. Manaseki-Holland S. Socioeconomic and Urban–Rural Inequalities in the Population-Level Double Burden of Child Malnutrition in the East and Southern African Region P Lo S Glob. Public Health 20233 e 000039710.1371/journal.pgph.000039737097991 PMC 10128925 · doi ↗ · pubmed ↗