Association of Gene Variants in Matrix Metalloproteinases and Their Tissue Inhibitors with Intraventricular Haemorrhage in Preterm Infants
Dawid Szpecht, Karolina Żyto, Gabriela Ciszek, Karolina Duczmal, Zofia Kowal, Kornelia Kręciszewska, Zuzanna Słowińska, Grażyna Kurzawińska, Anna Sowińska, Agnieszka Seremak-Mrozikiewicz

TL;DR
This study investigates how gene variants in matrix metalloproteinases and their inhibitors relate to brain bleeding in preterm infants.
Contribution
The study explores novel associations between specific MMP and TIMP gene variants and intraventricular hemorrhage in premature neonates.
Findings
Most gene variants in MMP-1, MMP-9, TIMP-1, and TIMP-2 were not statistically linked to IVH.
The T allele of TIMP1 rs4898 showed a potential association with IVH.
Further research is needed to clarify the role of MMP/TIMP polymorphisms in IVH.
Abstract
The objective of the present study is to examine the association between the presence of various forms of matrix metalloproteinase genes (MMP-1, MMP-9, TIMP-1 and TIMP-2) and their tissue inhibitors, and the incidence of intraventricular haemorrhage (IVH) in premature neonates. The data for this study were obtained from samples of peripheral venous blood, which were collected and stored post-delivery. The techniques employed for the purpose of genotyping were polymerase chain reaction (PCR) and restriction fragment length polymorphism (RFLP). The population that was examined comprised 100 patients with a gestational age (GA) ranging from 22 to 33 weeks and birth weight (BW) ranging from 432 to 2100 g. In the cohort of enrolled patients, 48 cases of IVH were observed. As indicated by the findings of this study, the majority of observed correlations between MMP-1, MMP-9, TIMP-1, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
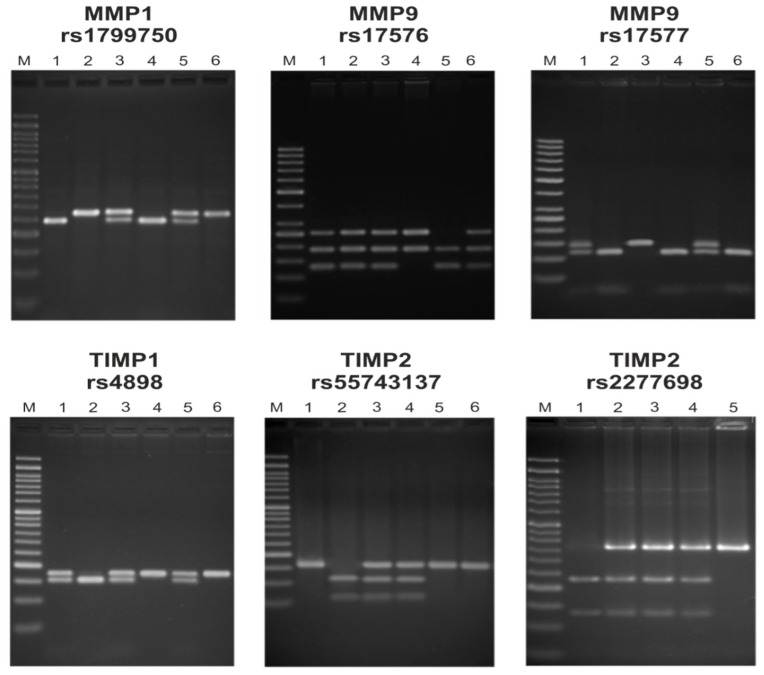 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBlood Coagulation and Thrombosis Mechanisms · Neonatal and fetal brain pathology · Preterm Birth and Chorioamnionitis
1. Introduction
Intraventricular haemorrhage (IVH) is one of the most common complications of preterm birth. The condition is characterised by the occurrence of bleeding within the germinal matrix, as defined by the first author. The germinal matrix is a brain region that is characterised by its high cellularity and vascularisation. During gestation, it is located beneath the lower vault of the lateral ventricles [1,2]. This region has been observed to regress during the process of brain development [3]. IVH is a common occurrence among premature infants. However, it is also rarely diagnosed among full-term newborns, usually due to the presence of the persistent germinal matrix or vascular malformations [1]. The incidence of this pathology has been shown to be inversely proportional to gestational age (GA) [4,5,6]. The potential for the identification of multiple risk factors associated with IVH in a group of preterm infants is a notable observation. It is an irrefutable fact that low birth weight (BW) and low GA are the underlying causes of many complications of prematurity, including IVH [7,8,9]. In the extant literature, a preponderance of authors draw attention to the genetic underpinnings of this condition. To date, the influence of polymorphism in the gene encoding vitamin K metabolism, as well as transportation, endothelial nitric oxide synthase and fibronectin 1, has been explored [9]. A number of studies have previously investigated the association between single nucleotide polymorphisms in the vitamin D receptor gene and IVH. However, these studies did not identify a significant relationship [10]. Furthermore, the impact of mutant genes implicated in inflammation has the potential to be substantial [11]. In the present study, the influence of genetic variability in the matrix metalloproteinase encoding genes is investigated. Metalloproteinases (MMPs) are zinc and calcium-dependent enzymes. A total of 23 MMP proteins are encoded by 24 distinct genes. A categorisation of these enzymes could be proposed, distinguishing between three collagenases, two gelatinases, three stromelysins, matrilysin, macrophage elastase and four membrane-type MMPs. MMPs are secreted as inactive proenzymes and are inhibited by tissue inhibitors of metalloproteinases (TIMPs). The function of these cells is subject to regulation by cytokines, growth factors and extracellular matrix (ECM) components. The function of matrix MMPs is the degradation of ECM proteins. This process is of crucial importance during the developmental phases, the growth stages, the phases of uterine cycling and angiogenesis. Degradation of ECM proteins can induce inflammation because of their chemotactic abilities [12,13]. As demonstrated by the study that analysed the activity of MMPs during hypoxic–ischemic brain damage in the immature rat, increased MMP activity was associated with damage to the blood–brain barrier (BBB) [14]. A breakdown of the BBB can result in increased penetration of toxic substances into brain cells and a heightened risk of bleeding in this area. It is imperative to emphasise that MMPs play a pivotal role in the degradation of collagen [13], a process that has been shown to stabilise blood vessels [15]. This finding suggests the potential involvement of MMPs in the pathogenesis of IVH. The present study employs the same patient cohort and methodological framework described by Choręziak-Michalak et al. (2023) [16]; however, while the previous work investigated retinopathy of prematurity (ROP), this analysis focuses specifically on IVH.
2. Results
2.1. Clinical Data
Demographic and clinical features of patients enrolled in the study trial are presented in Table 1. The study population consisted of 100 patients (47 female, 53 male) with median GA of 28 weeks (range 22–33 weeks) and median BW of 1080 g (range 432–2100 g). IVH was diagnosed in 48 patients (22 female, 26 male), including one patient with I grade IVH, 21 patients with II grade IVH, 22 patients with III grade IVH and four patients with IV grade IVH.
As shown in Table 1, the relationship between development of IVH and GA, BW, Apgar score, presence of birth asphyxia, infections (intrauterine, early, and late-onset), ROP, bronchopulmonary dysplasia (BPD) and mechanical ventilation therapy was observed. Grade of IVH correlated with GA, BW, the 5 min Apgar score, the use of mechanical ventilation and presence of BPD and ROP.
The reported p-values were adjusted for multiple testing correction using the False Discovery Rate (FDR) method (Supplementary Tables S1–S6). For a detailed comparison of nominal and adjusted values, please refer to the Supplementary Materials, which aligns with the significant results highlighted in the main text and tables.
2.2. Association Studies
Table 2 presents association between preterm infants affected by IVH as well as those without this complication and frequencies of studied gene variants. Only one variant proved to be statistically significant. No deviation from the Hardy–Weinberg equilibrium (HWE) was detected in both groups. The TIMP1 rs4898T allele occurred at a higher frequency in IVH cases in comparison to no-IVH cases (66% vs. 50%; OR 0.524 95% CI: 0.296–0.926; p = 0.026). Due to this allele’s linkage to the X chromosome, we conducted separate tests depending on sex, which showed the correlation for male newborns. The TIMP1 rs4898T allele occurred significantly more often in male neonates with IVH than in those without the condition (69% vs. 48%), suggesting a potential association (OR 0.413; 95% CI: 0.186–0.914; p = 0.029). No other statistically significant differences were observed. The MMP9 rs17576G allele was slightly less frequent in the IVH group relative to the no-IVH group. On the other hand, TIMP2 rs2277698T appeared more common in neonates with IVH in contrast to the other group. The significant results were put in bold whilst the other observations are presented in Table 2.
The association between the occurrence of IVH and studied variants was analysed with the use of logistic regression. The findings are illustrated in Table 3. Calculations included crude OR and adjusted OR (AOR) for BW, GA, mechanical ventilation, ROP, APGAR 5′, BPD. The analysis was performed for males and females separately in the TIMP1 gene, as it is linked to the X chromosome. No statistically significant variations were found. A trend was found in male neonates for CC homozygotes in the TIMP1 rs4898 gene (crude p = 0.06; OR 0.260; 95% CI: 0.064–1.056), although this association further lost significance after adjustment (AOR 0.305; 95% CI: 0.060–1.556; p = 0.153). The current results provide a foundation for future testing on a larger scale to confirm these preliminary observations. Other non-significant trends were observed for the MMP9 rs17576 gene in the whole group (result borderline; AOR 0.348; 95% CI: 0.121–1.000; p = 0.05). The discussed results are presented in Table 3.
For Table 2 and Table 3, correction for multiple testing using the FDR approach (Holm–Bonferroni) was applied to the tested genetic models. After adjustment for multiple comparisons, none of the associations remained statistically significant. The initially significant associations observed for the TIMP1 rs4898 variant (p = 0.026) in male newborns were no longer significant (FDR-adjusted p = 0.208). Similarly, a borderline association noted for the MMP9 rs17576 variant (p = 0.05) after FDR correction did not remain significant (FDR-adjusted p = 0.250).
Table 4 presents a comparison between patients with I + II grade IVH and III + IV grade IVH and frequencies of MMPs and TIMPs alleles and genotypes. No deviation from the HWE in the genotype distribution was detected. Table 5 shows the association between grade of IVH and studied variants, analysed using logistic regression. Crude OR and AOR for BW, GA, 5 min Apgar score, use of mechanical ventilation and presence of ROP and BPD were calculated. The codominant model was chosen as the main model. Additionally, analyses were performed under dominant, recessive and overdominant models. No association between studied variants and the grade of IVH was found.
3. Discussion
Prematurity and its associated complication, IVH, represent significant challenges for global medicine [17]. IVH is characterised by the occurrence of bleeding within the germinal matrix [1,17]. Whilst it is generally accepted that the first and second grades of IVH rarely induce further complications and that neurodevelopmental prognosis is excellent, there is a growing body of evidence to suggest that the third and fourth grades may be more prone to inducing significant damage, including but not limited to obstructive, non-obstructive and post-haemorrhagic hydrocephalus, developmental impairment, cerebral palsy and seizures [1,5]. The issue of prematurity is a global concern, with 15 million infants being born each year [18]. On a global scale, the prevalence of IVH ranges from 5 to 52% among newborns delivered at or beyond the 28th week of gestation. However, the precise incidence of the condition is subject to variation depending on the continent and, within those continents, specific countries [17].
The objective of this study was to evaluate the association between variants of MMP-1, MMP-9, TIMP-1 and TIMP-2 genes and IVH in the population of Polish neonates whose functional role had previously been investigated. The MMP-1 rs1799750 variant is characterised by an insertion or deletion within the promoter region. Research has indicated that the 2G/2G genotype is associated with elevated transcriptional activity of the MMP-1 gene [19]. MMP-9 rs17576 and rs17577 are non-synonymous single-nucleotide polymorphisms resulting in amino acid substitutions Gln279Arg and Arg668Gln, respectively. The rs17576 polymorphism leads to a Gln → Arg substitution within the fibronectin type II domain of MMP-9, a region that plays a critical role in substrate recognition and binding to extracellular matrix components such as fibronectin. Functional characterisation of MMP-9 polymorphisms has indicated that this amino acid substitution may alter interactions with ECM substrates and modulate enzymatic activity, supporting a functional relevance of rs17576 rather than a purely marker effect [20]. In addition, previous studies have demonstrated that the fibronectin type II domains of gelatinases are essential for efficient binding and degradation of ECM proteins, underscoring the biological plausibility that sequence variation within this region may influence MMP-9-mediated ECM remodelling [1,21]. In contrast, the rs17577 variant is located in the hemopexin domain, a region that has been implicated in modulating both substrate and inhibitor binding [20]. The TIMP1 rs4898 variant is a missense mutation in the coding sequence that has been shown to influence TIMP-1 expression and circulating levels, potentially modifying MMP inhibition. Genetic interaction analyses with MMP-9 haplotypes further suggest that rs4898 may modulate ECM remodelling pathways [22]. The TIMP2 rs2277698 polymorphism is a synonymous mutation, characterised by a C > T substitution at position 303 (Ser101). While the precise effects of this variant on gene expression remain to be elucidated, it has been hypothesised that it may influence splicing processes and modify transcriptional regulation [23]. The TIMP2 rs55743137 variant is an intron variant resulting in a G > T substitution [24].
A thorough analysis of clinical data pertaining to IVH risk factors was conducted, revealing substantial disparities between preterm infants with IVH and the control group (free of IVH) across several pivotal parameters. Neonates with IVH were characterised by a lower GA (median 27 weeks vs. 29 weeks) and lower BW (median 955 g vs. 1243 g) compared to preterm infants without IVH. The findings of this study indicate that prematurity and low BW are statistically significant risk factors for the development of IVH [24]. Furthermore, lower Apgar scores in the first and fifth minute after birth (4 vs. 6 and 7 vs. 8, respectively), a higher incidence of perinatal asphyxia (16.7% vs. 3.8%), and increased use of mechanical ventilation (68.8% vs. 32.7%) in infants with IVH, compared to those without, underscore the impact of hypoxia and intensive respiratory support on the risk of IVH [25]. It is noteworthy that previous studies have likewise identified a significant association between low Apgar scores and the incidence of other complications of prematurity [16,26]. Additionally, a higher prevalence of intrauterine and late-onset infections was observed among neonates with IVH, thereby underscoring the role of infectious and inflammatory processes in the pathogenesis of IVH. Moreover, infants with IVH who were born preterm exhibited a greater frequency of complications such as ROP (68.8% vs. 11.5%) and BPD (56.3% vs. 21.2%). Further analysis of IVH severity demonstrated a correlation between more severe cases (particularly grades III and IV) and lower GA, lower BW, reduced Apgar score in the fifth minute after birth, increased utilisation of mechanical ventilation, and a higher prevalence of BPD and ROP. These variables were statistically associated both with the occurrence and greater severity of IVH in the analysed cohort.
Our primary analysis reveals a significant association between the T allele in the TIMP1 rs4898 gene and the occurrence of IVH, with the mutation being substantially more frequent in affected neonates than in the control group. The variation was found to be statistically significant, with frequencies of 66% and 50%, respectively, corresponding to OR of 0.524 (CI: 0.296–0.926; p = 0.026). A similar association was identified in male infants with IVH, where the TIMP1 rs4898T allele was observed to be significantly more prevalent than in the male group without IVH (OR 0.413; 95% CI: 0.186–0.914; p = 0.029; 69% vs. 48%). No statistically significant association was observed among male CC homozygotes (p = 0.06; OR 0.26; 95% CI: 0.064–1.056). Moreover, this association did not remain statistically significant after multivariate adjustment (AOR 0.31; 95% CI: 0.060–1.556; p = 0.153), and therefore these results should be interpreted with caution.
In the present study, no statistically significant associations were observed between MMP9 rs17576 and TIMP2 rs2277698 polymorphisms and the occurrence of IVH. Similarly, no statistically significant association was found between MMP1 rs1799750 or MMP9 rs17576 variants and IVH grade. These findings do not support a relationship between these polymorphisms and IVH in the studied cohort.
MMPs are a family of zinc-dependent, structurally related proteolytic endopeptidases that mediate both physiological and pathological tissue remodelling. Their enzymatic activity is tightly regulated by specific TIMPs. In humans, over 20 MMP family members have been identified and characterised, each endowed with the capacity to degrade a broad spectrum of ECM proteins, thereby contributing to diverse processes such as embryogenesis, implantation, wound healing, inflammation, tumour progression, and angiogenesis, while simultaneously modulating bioactive molecules including cell-surface receptors, apoptotic ligands, and cytokines [27]. Beyond these well-established roles, the involvement of MMPs in neural tissue organisation and cerebral vascular development is increasingly recognised. Dysregulation of MMP activity has been hypothesised to heighten the structural vulnerability of the neonatal brain, potentially contributing to the pathogenesis of IVH. The endogenous regulators of this process, TIMPs, comprise four members—TIMP1, TIMP2, TIMP3, and TIMP4—which are 21–28 kDa proteins either secreted in soluble form or anchored to the ECM [28]. TIMPs reversibly inhibit MMP activity through their N-terminal domain, which folds intramolecularly to bind the MMP active site. In plasma, MMP activity can additionally be modulated by α2-macroglobulin. The MMP/TIMP system is critical for the maintenance of a delicate balance in ECM remodelling, vascular integrity and neural development, all of which are particularly critical in the context of neonatal brain vulnerability [29].
The extant literature does not provide unequivocal evidence for a direct association between MMP-1 and MMP-9 gene polymorphisms and the risk of IVH in neonates. However, there are relevant findings suggesting that MMP-1 may indirectly influence the development of IVH. For instance, research by Fujimoto et al. (2002) [30] demonstrated that the MMP-1-1607 1G/2G polymorphism in the MMP-1 promoter region affects gene transcription and MMP-1 enzyme levels in non-malignant cells. This polymorphism has been linked to elevated levels of MMP-1 expression, which may have a detrimental effect on vascular integrity and tissue remodelling. Conversely, Okamoto et al. (2008) [31] demonstrated that transforming growth factor-beta 1 (TGF-β1) induces MMP-9 expression in meningeal cells. The present study highlighted the role of MMP-9 in ECM remodelling, a process which is crucial in the pathogenesis of IVH. Further studies, such as those by Schulz et al. (2004) [29], have investigated the activities of MMP-2 and MMP-9 in the plasma of preterm neonates. The findings suggest that there is elevated MMP-9 activity in critically ill preterm infants with BPD and/or IVH, indicating a potential involvement in the pathogenesis of these conditions. Additionally, studies conducted on a Polish cohort have demonstrated that polymorphisms in MMP genes are associated with ROP [16]. Moreover, research by Okamoto et al. (2010) [32] examined cerebrospinal fluid (CSF) levels of MMP-9 in infants with posthaemorrhagic hydrocephalus. The study revealed that patients with resolved ventricular dilation without shunt surgery exhibited significantly elevated CSF levels of MMP-9, suggesting a potential role for MMP-9 in the resolution of ventricular dilation following IVH.
In the context of the previously discussed roles of MMP-1 and MMP-9 in the pathogenesis of IVH in neonates, it is also important to consider their endogenous regulators, TIMP1 and TIMP2. These proteins are vital for regulating MMP activity, and any imbalance in their ratio may compromise vascular integrity and neural development, potentially contributing to IVH. The extant literature suggests a correlation between neonatal serum levels of TIMP2 and the risk of certain complications. For instance, Lee et al. (2015) [33] discovered that diminished TIMP2 concentrations were correlated with the subsequent progression of BPD. Although the present study did not specifically address IVH, it indicates that alterations in the MMP/TIMP system can affect neonatal tissue integrity. In a similar vein, Schulz et al. (2004) [29] demonstrated GA-dependent differences in plasma MMP and TIMP levels, reporting reduced TIMP1 concentrations in preterm infants compared to full-term neonates. These findings suggest that limited inhibitory capacity in premature neonates may increase the vulnerability of cerebral vessels to damage. Furthermore, Nikolov et al. (2020) [34] emphasised that TIMP1 and TIMP2 play a crucial role in regulating collagen turnover, placental remodelling, and vascular development. Dysregulation of this system has been linked to pregnancy complications, including impaired foetal growth and preeclampsia, further emphasising the importance of maintaining a balanced relationship between MMPs and TIMPs in ensuring vascular stability.
Several previous studies have investigated the influence of genetic variants on complications of prematurity. For example, a study of 342 preterm infants GA ≤ 28 weeks examined associations between vascular endothelial growth factor A (VEGFA) and nitric oxide synthase (eNOS) variants and the risk of IVH and ROP [35]. Similarly, the NICHD Neonatal Research Network Cytokines Study included 826 preterm infants to identify Single Nucleotide Polymorphisms (SNPs) associated with severe IVH [36]. Smaller cohorts have also been analysed; Kosik et al. studied 105 preterm infants GA < 32 weeks to explore vascular-related gene variants and their relationship with IVH [37], while a Polish cohort of 210 preterm infants GA < 33 weeks evaluated ADRB2 polymorphisms in relation to ROP [38]. Collectively, these studies demonstrate a wide range of cohort sizes, from approximately 100 to over 800 infants, highlighting both the challenges and variability in power for detecting genetic associations in preterm populations.
The primary constraint of our study is the relatively modest sample size, which diminishes its capacity to discern statistically significant effects. Consequently, the majority of observed associations between MMP-1, MMP-9, TIMP-1, and TIMP-2 variants and IVH failed to attain statistical significance. The T allele of TIMP1 rs4898 was the only one to demonstrate a significant association with IVH. Given the exploratory nature of this study, these findings should be considered preliminary and require validation in larger, more diverse cohorts to confirm their statistical significance and ensure their clinical utility. Nevertheless, the findings of this study demonstrate that these variants do indeed exert an influence on the aforementioned condition. Moreover, the homogeneity of the study group, which consisted of Polish Caucasian neonates, serves to reinforce the significance of these findings. This study may provide an important contribution to future meta-analyses and highlights the need for further research in larger cohorts to clarify the role of MMP/TIMP polymorphisms in IVH.
4. Materials and Methods
4.1. Study Population
The current study utilised the same patient population previously characterised by Choręziak-Michalak et al. (2023) as well as the same methodological framework of this study [16]. A cohort of 100 preterm infants, entirely of Caucasian origin, was prospectively analysed at the Clinical Hospital of Gynaecology and Obstetrics in Poznan, from 1 March 2014 to 14 January 2020. Enrolment required both parental consent and GA between 22 + 0 and 33 + 0 weeks. The study population was divided into 48 IVH cases and 52 controls based on screening results. The severity of bleeding among the cases was then classified into four grades: Grade I (n = 1), Grade 2 (n = 21), Grade 3 (n = 22), and Grade 4 (n = 4).
Exclusion criteria for the study comprised infants (1) born from multiple pregnancies, (2) born from pregnancies involving the death of one of the foetuses, (3) with chromosomal abnormalities, (4) who reached death before 40 weeks of postmenstrual age and (5) diagnosed with inherited metabolic disorders.
4.2. Clinical Features
To identify potential drivers of IVH, we extracted various clinical parameters from the patients’ medical records. These were categorised into neonatal demographics (gender, GA in weeks, and BW in grams) and birth-related data, including pregnancy type (singleton vs. multiple), delivery mode, and Apgar scores at the 1st and 5th minutes. We also defined birth asphyxia specifically as an Apgar score below 6 at the 10th minute coupled with a cord blood pH < 7.0 or cord blood base excess (BE) < −15 mmol/L. Respiratory interventions were tracked by the type and duration of mechanical ventilation. The study also accounted for infectious and neonatal morbidities, ranging from intrauterine and late-onset infections (sepsis, urinary tract infections or pneumonia) to complications of prematurity such as BPD, ROP, and necrotizing enterocolitis (NEC).
4.3. Diagnostics
In Poland, transfontanelle ultrasound (TFUS) is routinely used as a screening tool for IVH in preterm infants. This method is highly sensitive and is typically performed in all neonates born before the 32nd week of gestation. The first ultrasound is conducted as soon as possible after birth to detect congenital brain abnormalities and haemorrhages. Follow-up examinations are routinely repeated throughout infancy to monitor potential changes. International guidelines support similar practices. In Poland, according to the Newborn Brain Society, first TFUS is being done directly after birth in order to identify congenital defects and haemorrhages. Next TFUS are repeated on the 3rd and 7th day of the life, then every week up to the 36th week of the adjusted age.
There is a classification of IVH among newborns, according to their extent- four-point Papilla scale [1,2,5]. Grade I is a haemorrhage limited to the germinal matrix, Grade II is IVH without ventricular dilatation, Grade III–IVH with ventricular dilatation occupying > 50% of the ventricle and Grade IV–IVH with intraparenchymal haemorrhage [1,2,5]. Grade II haemorrhages and their frequency are rarely documented and described. According to population studies their frequency is 5–19%. Haemorrhages more often described and documented are haemorrhages grade III and grade IV—their incidence in newborns born up to 28 weeks of pregnancy is 5–52% globally, 5–52% in Europe and 8–22% in North America [17]. Data from countries of the European Union inform that the frequency of III and IV grade IVH is 2–25%, on average 10% [11].
4.4. Treatment
Management of IVH in preterm infants primarily focuses on supportive care, as there is currently no specific causal treatment. This includes stabilisation of respiratory and cardiovascular functions, maintenance of optimal cerebral perfusion, and monitoring for signs of post-haemorrhagic ventricular dilation. In cases where hydrocephalus develops, surgical interventions such as ventricular reservoir placement or ventriculoperitoneal shunting may be necessary. Early neurodevelopmental follow-up is crucial, as infants with IVH are at increased risk for long-term neurological impairments. Multidisciplinary care and early intervention programmes can significantly improve developmental outcomes.
4.5. Data Collection
In our study we used data collected from peripheral venous blood samples taken after delivery and stored. Genomic DNA was extracted using the QIAamp DNA Blood Mini Kit (QIA-GEN Inc., Hilden, Germany) in accordance with manufacturer’s instructions. Polymerase chain reaction (PCR) and restriction fragment length polymorphism (RFLP) techniques were used to genotype the polymorphisms. Used primers and restriction enzymes are described in Table 6. Electrophoresis on agarose gels was performed using Midori Green Advance DNA Stain (Nippon Genetics, Düren, Germany)—Figure 1. For quality assurance, about 5% of the samples were blindly repeated. All variants showed a call rate exceeding 95%.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bokiniec R. Szczapa J. Podstawy Neonatologii Wydawnictwo Lekarskie PZWL Warszawa, Poland 2008978-83-200-3456-1
- 2Starr R. De Jesus O. Shah S.D. Borger J. Periventricular and Intraventricular Hemorrhage Stat Pearls Stat Pearls Publishing Treasure Island, FL, USA 2025
- 3Hand I.L. Shellhaas R.A. Milla S.S. Committee on Fetus and Newborn, Section on Neurology, Section on Radiology Cummings J.J. Adams-Chapman I.S. Aucott S.W. Goldsmith J.P. Kaufman D.A. Martin C.R. Routine Neuroimaging of the Preterm Brain Pediatrics 2020146 e 202002908210.1542/peds.2020-02908233106343 · doi ↗ · pubmed ↗
- 4Pediatria Po Dyplomie-Noworodek Urodzony Przedwcześnie z Uszkodzeniem Mózgu Available online: https://podyplomie.pl/pediatria/12184,noworodek-urodzony-przedwczesnie-z-uszkodzeniem-mozgu-problemy-okresu-niemowlecego-i-wczesnego?srsltid=Afm B Ooq 3Km 8bgjhi Kc G 53Qd 3Iku Xm Kyqb Uiy Q 211O 4bfyybpam Ot Sm B(accessed on 26 August 2025)
- 5Intraventricular Hemorrhage in the Preterm Infant: Background, Pathophysiology, Etiology Published online 21 May 2024 Available online: https://emedicine.medscape.com/article/976654-overview?form=fpf(accessed on 26 August 2025)
- 6Szpecht D. Wiak K. Braszak A. Szymankiewicz M. Gadzinowski J. Role of Selected Cytokines in the Etiopathogenesis of Intraventricular Hemorrhage in Preterm Newborns Childs Nerv. Syst. Ch NS Off. J. Int. Soc. Pediatr. Neurosurg.2016322097210310.1007/s 00381-016-3217-9PMC 508634127541865 · doi ↗ · pubmed ↗
- 7Tsao P.-C. Pathogenesis and Prevention of Intraventricular Hemorrhage in Preterm Infants J. Korean Neurosurg. Soc.20236622823810.3340/jkns.2022.028836919227 PMC 10183267 · doi ↗ · pubmed ↗
- 8El-Atawi K. Risk Factors, Diagnosis, and Current Practices in the Management of Intraventricular Hemorrhage in Preterm Infants: A Review Acad. J. Pediatr. Neonatol.2016155556110.19080/AJPN.2016.01.555561 · doi ↗