The Role of Hysteroscopy for the Treatment of Interstitial Ectopic Pregnancy: A Systematic Review
Guglielmo Stabile, Laura Vona, Stefania Carlucci, Francesco Nappi, Stefania Biffi, Anna Pitsillidi, Stefano Restaino, Giuseppe Vizzielli, Luigi Nappi

TL;DR
This paper reviews hysteroscopy as a minimally invasive treatment for interstitial ectopic pregnancy, showing it can preserve fertility with limited risks.
Contribution
The study systematically evaluates hysteroscopy's safety and effectiveness for interstitial ectopic pregnancy, emphasizing fertility preservation.
Findings
Hysteroscopic management was successful in 76% of cases.
Mean time to β-hCG normalization was 32 days.
Reduced residual myometrial thickness was linked to treatment failure.
Abstract
Background/Objectives: Interstitial ectopic pregnancy is a rare and potentially life-threatening condition, accounting for 1–6% of ectopic pregnancies. Its location complicates diagnosis and management, and no standardized treatment guidelines exist. Fertility-preserving, minimally invasive approaches have been proposed as alternatives to medical therapy or radical surgery. This systematic review evaluates the safety and effectiveness of hysteroscopic treatment, focusing on uterine preservation and reproductive outcomes. Methods: This systematic review was conducted according to PRISMA guidelines and registered in PROSPERO (CRD420251249508). Web of Science, Scopus, and PubMed were searched from inception to January 2026. Eligible articles included case reports and case series describing interstitial pregnancies managed hysteroscopically, alone or combined with minimally invasive…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
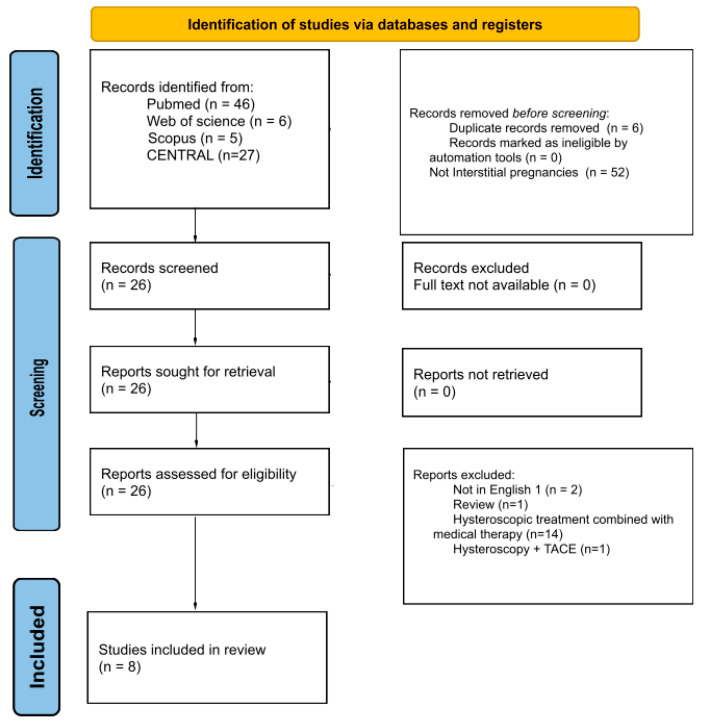 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEctopic Pregnancy Diagnosis and Management · Gynecological conditions and treatments · Appendicitis Diagnosis and Management
1. Introduction
The 2020 ESHRE classification standardises the terminology used to describe ectopic pregnancies on ultrasound. In this classification, interstitial pregnancy is considered a subtype of tubal ectopic pregnancy when the gestational sac implants in the portion of the fallopian tube that penetrates the uterine muscle [1]. The incidence of this condition is estimated at 1–6% of all ectopic pregnancies, with a maternal mortality rate of 2–2.5% [2]. These data identify a relatively rare ectopic pregnancy that is difficult to differentiate from a lateralised eutopic pregnancy [1]. Interstitial ectopic pregnancy has few early clinical symptoms (abdominal pain in the first trimester of pregnancy) and vaginal bleeding [3]. A diagnostic process based on clinical findings, gestational age at diagnosis, human chorionic gonadotropin (β-HCG) dosage, ultrasound features, and patient preferences are useful factors in the decision-making process regarding the best treatment [4]. Treatment may be medical, surgical, or close observation. There are no guidelines in the literature for the management of this condition. Therefore, authors prefer surgical or medical intervention based on their skills and experience [5]. This review aims to understand the outcomes of hysteroscopic treatment as a monotherapy, in combination with another minimally invasive surgical technique (e.g., suction and curettage) or under laparoscopic guide without any medical treatment. Furthermore, considering that standard management traditionally includes cornual resection or systemic methotrexate administration, this review seeks to contextualize hysteroscopy as a potentially less invasive alternative, assessing its safety and efficacy in the management of a rare and difficult-to-treat condition.
2. Materials and Methods
2.1. Search Strategy
This systematic review was conducted in accordance with the PRISMA guidelines for systematic reviews (see Supplementary Table S1 PRISMA checklist) [6]. Two independent reviewers (L.V. and G.S.) performed a comprehensive literature search of the Web of Science, Scopus, PubMed and Cochrane Central Register of Controlled Trials (CENTRAL) databases, from database inception through 31 January 2026. No publication date restrictions were applied. The search strategy combined the following keywords and MeSH terms: ectopic pregnancy, interstitial pregnancy, treatment, hysteroscopy.
Studies in which interstitial pregnancies were treated with hysteroscopic management alone or in combination with another minimally invasive surgical intervention (suction and curettage, laparoscopic guide or laparoscopic milking) were considered. The study selection process is detailed in the PRISMA flow diagram (Figure 1).
2.2. Eligibility Criteria
Eligible study designs included case reports, randomized controlled trials, prospective controlled studies, prospective cohort studies, retrospective studies, and case series. Only full-text articles published in English were included. Only articles reporting cases of interstitial pregnancies treated with hysteroscopic management alone or assisted by minimally invasive surgical treatments like suction and curettage, laparoscopic guide or laparoscopic milking were included. Studies were included if they reported cases of interstitial pregnancy diagnosed according to established ultrasound criteria. Interstitial pregnancy was defined by the presence of: (1) an empty uterine cavity; (2) a gestational sac located laterally in the interstitial (intramural) portion of the fallopian tube; and (3) the presence of the interstitial line sign. When the diagnostic criteria were not explicitly detailed, studies were considered eligible if the described ultrasound findings were consistent with these features.
2.3. Exclusion Criteria
Systematic reviews, meta-analyses, letters to the editor, and conference abstracts were excluded. However, reference lists of relevant reviews were manually screened to identify additional eligible studies. Articles not written in English, or those including non-interstitial ectopic pregnancies, as well as cases in which interstitial pregnancies were treated with non-hysteroscopic surgical management, medical therapy or a combination of these, were excluded. The use of alternative treatments, such as interventional radiology procedures (e.g., TACE—Transcatheter Arterial Chemoembolization) [7] were also exclusion criteria.
2.4. Data Extraction and Risk of Bias Assessment
Two reviewers (G.S. and L.V.) independently screened all records retrieved through the database search, beginning with publication year, citation details, title, authorship, and abstract, followed by full-text evaluation. Duplicate entries were manually identified and removed prior to screening. After eliminating irrelevant studies based on titles and abstracts, the reviewers independently assessed the full texts of the remaining articles for eligibility. Any disagreements were resolved through discussion and consensus.
The methodological quality of the included studies was evaluated using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist (Supplementary Table S2). The study protocol was registered in the PROSPERO database (registration number: CRD420251249508). As this review includes exclusively case reports and case series, a potential risk of bias is acknowledged.
2.5. Data Synthesis
Data extracted included patient demographics (age, obstetric history), method of conception, gestational age at diagnosis, serum β-hCG levels, and ultrasonographic parameters such as residual myometrial thickness, gestational sac diameter, and the presence of embryonic cardiac activity. Treatment-related variables included the type of hysteroscopic approach, the use of laparoscopic or ultrasonographic guidance, catheter size for suction, and the use of hemostatic agents. The extracted outcomes comprised treatment success, the need for rescue interventions, and time to β-hCG normalization (Table 1). Treatment success was defined as complete resolution of the interstitial pregnancy without the need for additional surgical or medical interventions, confirmed by ultrasound evidence of absence of residual trophoblastic tissue and/or a progressive decline of serum β-hCG levels until normalization.
Continuous variables were summarized as means where possible, while categorical variables were presented as frequencies or percentages. The results of individual studies were visually displayed using tables. Baseline characteristics were stratified by treatment outcome and summarized separately for treatment failure and treatment success. Given the small number of patients and heterogeneity among the included studies, some data were synthesized descriptively.
3. Results
3.1. Study Selection and Methodological Quality Assessment
The literature search identified a total of 84 records from electronic databases, including PubMed (n = 46), Web of Science (n = 6), Scopus (n = 5) and CENTRAL (n = 27). Before screening, 58 records were removed: 6 duplicates and 52 records that were not related to interstitial pregnancies. The remaining 26 records were screened, and all were sought for retrieval. No reports were excluded due to unavailability of full text. All 26 reports were assessed for eligibility. Twenty reports were excluded for the following reasons: not in English (n = 2), review articles (n = 1), hysteroscopic treatment combined with medical therapy (n = 14), and hysteroscopy combined with Transcatheter Arterial Chemoembolization (n = 1). Ultimately, eight studies were included in the final review, comprising 21 patients.
The methodological quality of the included case reports was assessed using the JBI Critical Appraisal Checklist. Overall, the studies demonstrated good methodological quality. Six of the eight reports met all eight appraisal criteria. Two studies showed unclear reporting regarding patient demographic characteristics and the description of diagnostic tests or assessment methods [8,10]. Clear reporting of the intervention, post-intervention outcomes, and adverse or unanticipated events was observed across all included studies.
3.2. Patients’ Characteristics and Pregnancy Data
The mean age was 31 years (range 20–42). Obstetric history was reported in six studies. The method of conception was described for 2 patients, who conceived through IVF [13,14].
The mean gestational age was 55 days (range 35–85). The mean β-hCG level was 7981 IU/L (range 1440–32,000), although two studies did not report this value [10,11].
3.3. Ultrasound Findings
Regarding the ultrasonographic data, the residual myometrial thickness between the ectopic pregnancy and the uterine serosa was reported in only three studies, ranging from 1 to 4 mm (mean 1.8 mm) [12,14,15]. The gestational sac diameter ranged from 5 to 67 mm (mean 40). The presence of an embryonic pole with cardiac activity was documented two studies [11,15].
3.4. Treatments
In four studies, laparoscopy was used as guidance to visualize the suction and hysteroscopic procedures (successful in 12 of 17 patients—71%) [8,9,10,12]. In the studies by Nezhat et al., laparoscopic milking —a technique in which the ectopic gestational tissue is gently mobilized from the fallopian tube toward the uterine cavity—was used to displace the gestational sac toward the uterine cavity prior to hysteroscopic removal, with or without suction and curettage [11,13]. In four studies, the size of the Karman Cannula used for suction was reported [8,9,10,12], and in two of these, a pediatric 8-Fr cannula was employed [8,9]. Among patients treated with the 8-Fr cannula, 6 of 9 achieved procedural success, while all 6 patients treated with 15- or 18-Fr cannulas had successful outcomes.
In the 2025 case by Liu hysteroscopic treatment was performed under ultrasound guidance alone (success rate 100%) [14]. In the case reported by Cronin et al., the gestational sac was removed hysteroscopically, followed by US guided curettage to remove the remaining tissue [15]. A hemostatic agent (Oxytocin or Vasopressin) was used by Cai et al. and Nezhat et al. [9,11].
3.5. Outcomes
The treatment approach was successful in 16 of 21 patients (76%). Treatment failure occurred in 5 patients (26%), all of whom required rescue management.
In four of these cases, surgical intervention was necessary: laparoscopic cornual resection was performed in three patients (two reported by Niu et al. and one by Cai et al.) [9,12], while one patient in the study by Cai et al. required laparotomic cornual resection associated with salpingectomy [9]. In the remaining case, reported by Cai et al., adjuvant methotrexate (MTX) therapy was administered because of persistent residual amnio chorionic tissue [9].
The mean time to β-hCG normalization was 32 days (range 2–63).
Table 2 and Table 3 show the baseline characteristics of patients according to treatment outcome. Table 2 reports data for patients with treatment failure, while Table 3 includes patients with treatment success, including mean age, gestational age, serum β-hCG, residual myometrial thickness (RMT), and gestational sac (GS) diameter.
4. Discussion
Interstitial pregnancies are a rare type of ectopic pregnancy associated with an increased risk of severe hemorrhage and maternal morbidity [2]. The optimal management for this type of ectopic pregnancy is unclear and there are not guidelines in the literature to refer to for treatment [16]. The aim of the therapy should be to terminate the pregnancy while minimizing the risk of bleeding and preserving fertility [17]. Alternative management strategies have shown variable success rates. Combination therapy with systemic methotrexate and mifepristone was effective in 63.6% of cases [18], while in a cohort of 98 patients, surgical treatment (cornual resection) was successful in 100%, intralesional single-dose methotrexate in 70.6%, and intramuscular multidose methotrexate in 31% of cases [19]. Furthermore, in cases of advanced maternal age with recourse to medically assisted procreation, the resolution time is also an important factor to consider in choosing the best management [20]. In these cases, in fact, it would be necessary to consider the need to wait 3–6 months before a new pregnancy in the case of using methotrexate for medical therapy [21]. In addition, in many cases managed with medical therapy a longest time for β-hCG relativization is needed [20]. According to some authors the observation of pregnancy vascularization, even if subjective, could be the leading point to choose about the possibility of a medical approach [17]. A higher vascularization could suggest the presence of a wider syncytiotrophoblast and a consequent higher progesterone secretion that leads to a minor efficacy of the therapy [22]. Syncytiotrophoblast plays the most important role in maintaining pregnancy by directly contacting the endometrium for oxygen exchange [23]. It also secretes human placental lactogen, which regulates maternal metabolism to ensure an adequate supply of nutrients to the fetus and secretes β-hCG to maintain the corpus luteum of the ovary [24,25]. As our results demonstrate, hysteroscopy, even when not guided by laparoscopy, is an effective tool for the resolution of this type of pregnancy. Furthermore, compared to dilatation and curettage allows direct visualization of the uterine cavity and of the pregnancy ensuring a good hemostasis coagulating and separating the chorionic villi and placental tissues from the myometrium [20]. While many included reports still describe the use of Karman cannulas and curettage, insights from more frequent cases of cesarean scar pregnancy suggest that hysteroscopic techniques provide improved visualization, targeted tissue removal, and better control of bleeding [26]. This comparison indicates that hysteroscopy may reduce the risk of incomplete removal and uterine trauma compared to purely suction methods [20]. Where feasible, the inclusion of intraoperative images can further illustrate procedural steps and support reproducibility [27].
Minimally invasive approaches, such as hysteroscopy, provide distinct advantages over more extensive surgical procedures, including cornual resection or cornuotomy, particularly with respect to perioperative morbidity and the preservation of uterine integrity and subsequent fertility. In the study by Lee et al., patients managed with cornual resection or cornuotomy, had an overall incidence of persistent interstitial pregnancy of 6.7% [28], underscoring a clinically relevant complication that appears to be largely avoidable with minimally invasive uterine-sparing techniques, as demonstrated in our cohort. Furthermore, more radical procedures are characterized by prolonged operative times and a higher risk of significant intraoperative blood loss, while laparoscopic wedge resection has been associated with serious obstetric sequelae in subsequent pregnancies, including uterine rupture or dehiscence in up to 30% of cases [29]. In contrast, hysteroscopy minimizes disruption of the myometrium, reduces surgical trauma, and preserves the structural integrity of the uterus, as the procedure is performed under direct visualization of the uterine cavity, allowing the pregnancy to be removed under hysteroscopic guidance, further contributing to the preservation of uterine architecture and potentially reducing the risk of adverse reproductive outcomes while optimizing the prospects for future gestations [30].
Patient age, history of previous abortions, and parity do not appear to affect the outcome of hysteroscopic treatment. Interestingly, gestational age at the time of intervention also does not seem to influence the procedural outcome, contrary to what might be expected. In fact, the patients in whom the treatment was effective had a longer gestational age and a larger average size of the gestational sac compared to those in whom the hysteroscopic therapy was unsuccessful. This could be explained by a simpler hysteroscopic surgical approach in patients with a more advanced gestational age, characterized by a larger gestational sac that protrudes further into the uterine cavity [31]. In contrast, at earlier stages of pregnancy, smaller gestational sacs may make the procedure more challenging due to the difficulty of the instruments in reaching the gestational sac and the trophoblast, thereby increasing the risk of bleeding and uterine perforation. Residual myometrial thickness (RMT) is typically measured by ultrasound and represents the amount of muscular tissue between the gestational sac and the serosal surface of the uterus. RMT is an important anatomical parameter for procedural planning. What our data suggest significantly influences the outcome is the RMT, and this is easy to understand if one considers that an hysteroscopy electrode or loop approximately 0.3 mm in diameter is used to remove the pregnancy [32,33]. For this reason, in the case of a reduced RMT (even just 1 mm less) the risk of uterine perforation increases significantly.
The procedural success rate does not appear to increase when laparoscopy is used as guidance compared with ultrasound during hysteroscopy. Therefore, laparoscopy should be regarded as a secondary approach, for instance in the event of active bleeding or suspected uterine perforation, rather than being routinely employed as guidance for hysteroscopy, given that ultrasound has proven to be a reliable and effective tool. Indeed, avoiding the use of laparoscopy as a guidance modality also reduces patient exposure to more invasive and potentially unnecessary procedures [34]. However, this finding may be influenced by the fact that cases managed under laparoscopic guidance were characterized by a lower residual myometrial thickness, and ultrasound guidance has been reported in only a few cases, so evidence is limited and further studies are needed.
One of the main challenges during hysteroscopy is the operator’s limited ability to accurately assess uterine wall thickness and the extent of uterine distension during the procedure [35]. In cases where the residual myometrial thickness (RMT) is less than 2 mm, laparoscopy may serve as an additional safety adjunct to enhance procedural control.
While laparoscopy does not appear to be necessary as a diagnostic modality—given the 100% diagnostic accuracy of ultrasound in the analysed cases—it may still have a role in selected clinical scenarios, particularly when the RMT is <2 mm.
Finally, the use of uterine aspiration as an adjunct to the hysteroscopic procedure appears to be a valuable adjuvant, allowing for a more rapid and effective resolution of the pregnancy. Our analysis suggests that the size of the Karman cannula may influence procedural success. In our review, patients treated with a pediatric 8-Fr cannula had a slightly lower success rate (6 of 9) compared to those treated with 15- or 18-Fr cannulas (6 of 6). Although the sample size is small, this finding may indicate that smaller cannulas could be associated with a slightly lower likelihood of complete removal of gestational tissue.
Based on these findings, we feel that the use of ultrasound can be suggested, as it is less invasive and more effective in preserving the patient’s fertility.
4.1. Predictors of Procedural Failure
In our review, 5 patients experienced procedural failure (26%), with four requiring laparoscopic cornual resection and one requiring methotrexate. We explored whether specific preoperative characteristics could predict failure. Although patient age, parity, and history of prior abortions did not appear to influence outcomes, cases with a reduced residual myometrial thickness (<2 mm) were more likely to experience incomplete removal. Additionally, smaller gestational sacs at earlier gestational ages may contribute to technical challenges, potentially increasing the risk of failure. While these observations are limited by the small sample size, they suggest that careful assessment of RMT and gestational sac size may help identify patients at higher risk for unsuccessful hysteroscopic management.
4.2. Limitations
This review is limited by the small sample size, comprising only 21 patients across eight studies, which restricts generalizability. Comparisons between different treatment techniques are particularly challenging due to the limited number of studies employing each approach. Follow-up data and long-term reproductive outcomes were limited, preventing definitive conclusions regarding fertility preservation. Future studies should aim to report procedure-specific complication rates and, where feasible, assess post-treatment tubal patency of the affected tube, as these data would provide further insights into the safety and reproductive outcomes of minimally invasive management of interstitial pregnancy. Finally, the inclusion of primarily case reports and small case series introduces the potential for publication bias and may overestimate procedural success.
5. Conclusions
Interstitial ectopic pregnancy, increasingly observed due to assisted reproductive technologies and advanced maternal age, remains a complex clinical entity because of its rarity, absence of standardized guidelines, and heterogeneous outcomes. Our review indicates that, in hemodynamically stable patients, hysteroscopic management represents a safe, effective, and fertility-preserving minimally invasive approach, enabling direct visualization of the uterine cavity and targeted removal of gestational tissue while minimizing myometrial disruption. From a practical clinical standpoint, residual myometrial thickness (RMT) emerges as the key determinant of procedural safety. An RMT ≥ 2 mm appears to allow safe hysteroscopic management under ultrasound guidance alone, whereas an RMT < 2 mm identifies a higher-risk subgroup in whom laparoscopic assistance may serve as a safety adjunct. Therefore, RMT measurement should systematically guide preoperative planning, risk stratification, and intraoperative decision-making. However, given the limited number of reported cases, the variability among studies, and the lack of comprehensive long-term reproductive outcome data, larger prospective studies are needed to further validate this management strategy, better define its safety and efficacy, and confirm its fertility-preserving benefits in a broader patient population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The ESHRE working group on Ectopic Pregnancy Kirk E. Ankum P. Jakab A. Le Clef N. Ludwin A. Small R. Tellum T. Töyli M. Van Den Bosch T. Terminology for describing normally sited and ectopic pregnancies on ultrasound: ESHRE recommendations for good practice Hum. Reprod. Open 20202020 hoaa 05510.1093/hropen/hoaa 05533354626 PMC 7738750 · doi ↗ · pubmed ↗
- 2Moawad N.S. Mahajan S.T. Moniz M.H. Taylor S.E. Hurd W.W. Current diagnosis and treatment of interstitial pregnancy Am. J. Obstet. Gynecol.2010202152910.1016/j.ajog.2009.07.05420096253 · doi ↗ · pubmed ↗
- 3Kampioni M. Chmaj-Wierzchowska K. Wszołek K. Wilczak M. Interstitial Ectopic Pregnancy—Case Reports and Medical Management Medicina 20235923310.3390/medicina 5902023336837435 PMC 9967369 · doi ↗ · pubmed ↗
- 4Almeida A.C.D. Almeida R.R.G.D. Castelo B.B. Baccaro L.F.C. Non-tubal ectopic pregnancy: Types of treatment and occurrence of severe complications in a university hospital Rev. Bras. Ginecol. E Obs.202547 e-rbgo 7010.61622/rbgo/2025 rbgo 70PMC 1267166141341936 · doi ↗ · pubmed ↗
- 5Stabile G. Romano F. Buonomo F. Zinicola G. Ricci G. Conservative Treatment of Interstitial Ectopic Pregnancy with the Combination of Mifepristone and Methotrexate: Our Experience and Review of the Literature Bio Med Res. Int.20202020870349610.1155/2020/870349632802882 PMC 7421079 · doi ↗ · pubmed ↗
- 6Page M.J. Mc Kenzie J.E. Bossuyt P.M. Boutron I. Hoffmann T.C. Mulrow C.D. Shamseer L. Tetzlaff J.M. Akl E.A. Brennan S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews BMJ 2021372 n 7110.1136/bmj.n 7133782057 PMC 8005924 · doi ↗ · pubmed ↗
- 7Takeda A. Koike W. Hayashi S. Imoto S. Nakamura H. Magnetic Resonance Imaging and 3-dimensional Computed Tomographic Angiography for Conservative Management of Proximal Interstitial Pregnancy by Hysteroscopic Resection After Transcatheter Arterial Chemoembolization J. Minim. Invasive Gynecol.20152265866210.1016/j.jmig.2015.01.00425592772 · doi ↗ · pubmed ↗
- 8Katz D.L. Barrett J.P. Sanfilippo J.S. Badway D.M. Combined hysteroscopy and laparoscopy in the treatment of interstitial pregnancy Am. J. Obstet. Gynecol.20031881113111410.1067/mob.2003.25812712124 · doi ↗ · pubmed ↗