Clinical Utility of Copy Number Abnormality Analysis in the Evaluation of Melanocytic Lesions for Diagnosis and Prognosis: An Evidence-Based Review from the Cancer Genomics Consortium Working Group for Melanocytic Lesions
Cynthia Reyes Barron, Katherine B. Geiersbach, Ahmed K. Alomari, Kristen L. Deak, Shivani Golem, Eli S. Williams, Umut Aypar, Ying S. Zou, Lei Wei, Alka Chaubey, Nikhil Sahajpal, Ravindra Kolhe, Tanzy M. Love, Larry Prokop, M. Anwar Iqbal

TL;DR
This paper reviews how copy number abnormalities can help diagnose and predict outcomes in melanocytic lesions when traditional methods are uncertain.
Contribution
The study provides evidence-based recommendations for using copy number abnormality testing in ambiguous melanocytic lesion cases.
Findings
Copy number abnormalities are common in melanomas but rare in benign lesions.
CNA testing helps distinguish between benign and malignant melanocytic lesions.
CNAs differ between primary and metastatic melanomas and can inform prognosis.
Abstract
Background/Objective: Although most melanocytic lesions are diagnosed as benign or malignant by histopathologic evaluation, with or without the aid of immunohistochemistry, diagnosis may remain uncertain in a minority of cases. Assessment of copy number abnormalities (CNAs) may provide sufficient additional evidence to favor either a benign or malignant diagnosis in both pediatric and adult cases and in melanocytic lesions of various subtypes, including Spitzoid, mucosal, and acral. CNAs are common in melanomas, while they are rare, with few exceptions, in benign lesions. Detection of CNAs by fluorescence in situ hybridization (FISH) and chromosomal microarray (CMA) has been well established for melanocytic lesions, with advantages and disadvantages for each. The objective of this meta-analysis was to evaluate the utility of CNA testing for the diagnosis of melanoma, across subtypes,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1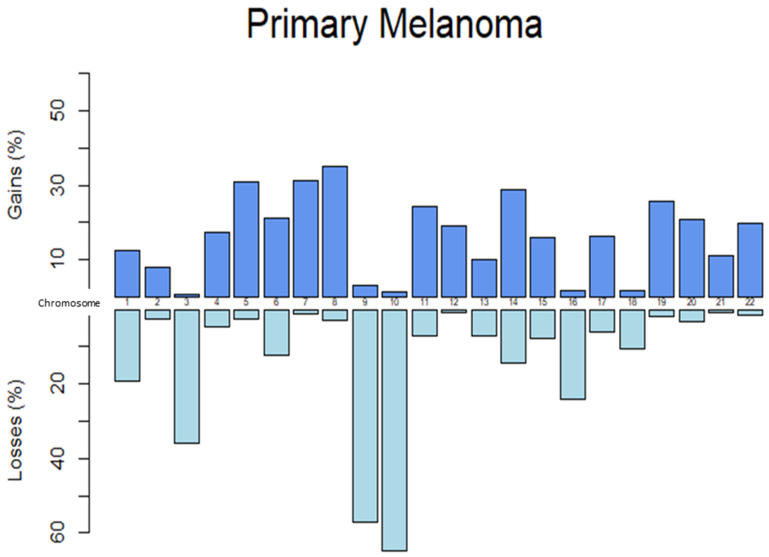 Figure 2
Figure 2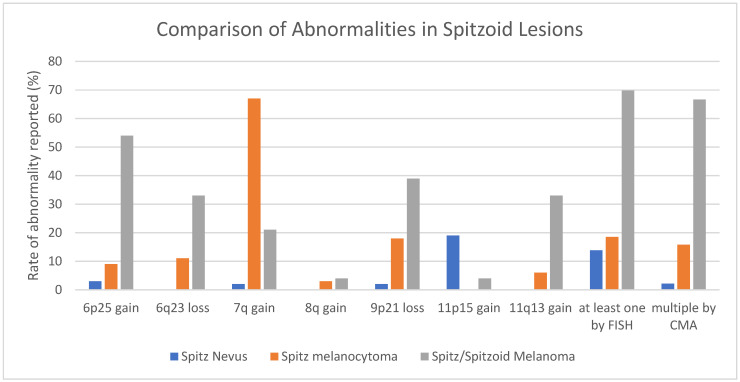 Figure 3
Figure 3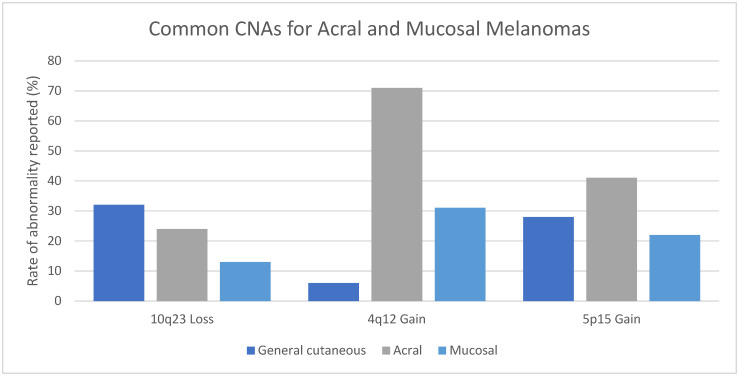 Figure 4
Figure 4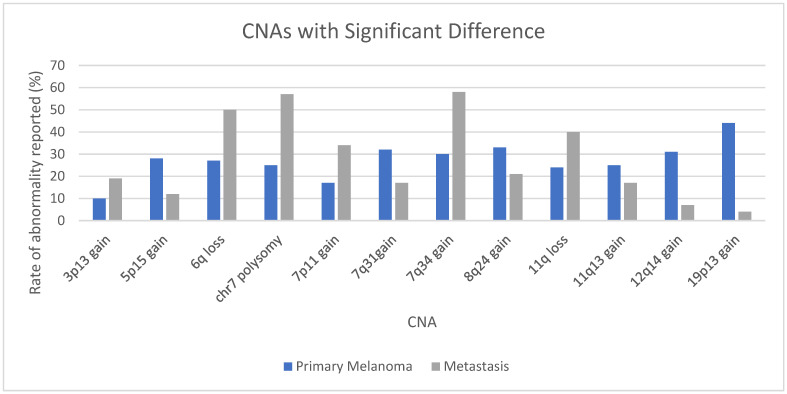 Figure 5
Figure 5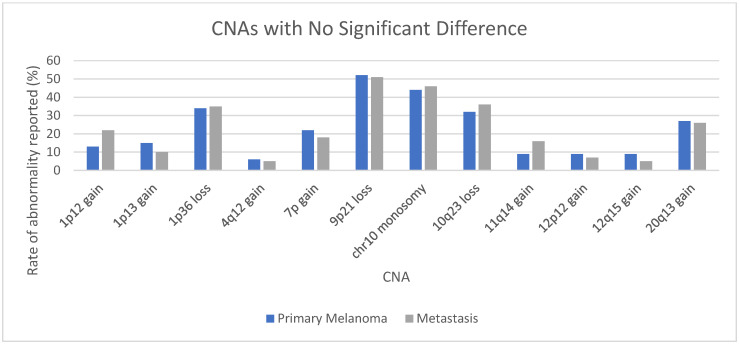 Figure 6
Figure 6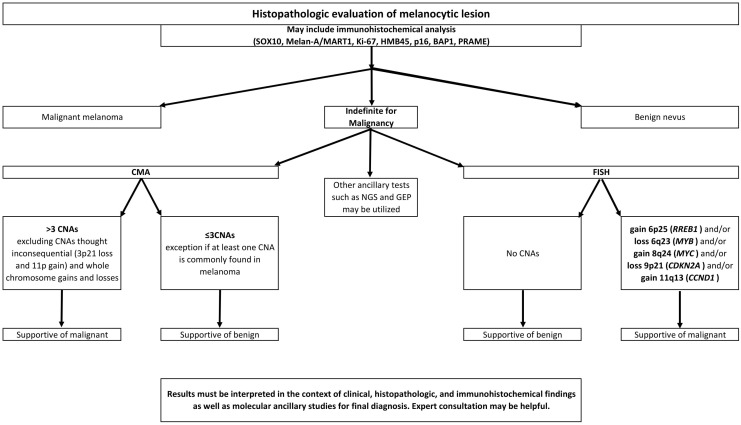 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCutaneous Melanoma Detection and Management · Ocular Oncology and Treatments · Melanoma and MAPK Pathways
1. Introduction
1.1. Overview of Diagnostic Challenge
Benign melanocytic proliferations are extremely common, with most people possessing several benign melanocytic nevi or moles. Nevi may be present at birth or be acquired through adulthood and often regress later in life. Almost all will remain benign and never become malignant [1,2]. Melanoma is a complex malignancy arising from melanocytes. The estimate of new cases in the United States in 2025 is over 100,000 (https://seer.cancer.gov/statfacts/html/melan.html (accessed on 24 August 2025)). Sun exposure has long been recognized as a risk, yet damage from ultraviolet radiation is not always a factor in malignancy. The World Health Organization categorizes melanoma into nine pathways, only three of which are typically associated with cumulative solar damage. Precursor lesions and characteristic genetic mutations are considered along each pathway [3]. These pathways help our understanding of tumor biology and, in some cases, progression from benign precursor lesions to malignancy. Copy number abnormalities (CNAs), diffuse aneuploidy, and loss of heterozygosity may be important events in melanoma progression, with greater involvement in late-stage and metastatic disease [4].
Both clinical history and dermoscopy can play a role in the initial evaluation of pigmented lesions, and the findings should be considered through further assessment [5]. Histopathologic evaluation of the biopsy tissue then serves to categorize a particular lesion as benign or malignant and either confirm or refute a clinical suspicion. In the vast majority of cases, histopathologic assessment, with or without the aid of immunohistochemical stains, is sufficient for diagnosis. However, a minority of cases possess features that are ambiguous and may be suspicious for malignant melanoma but not definitive (see Figure 1). This melanocytic lesion from a 10-year-old male displayed cytologic atypia, lack of maturation, and increased proliferative activity with scattered atypical mitoses on histopathologic evaluation. CMA was abnormal, demonstrating loss of 6q11.1q27 and loss of 16q11.2q24.3. The final diagnosis was malignant melanoma, Spitzoid type. Subsequently, the patient underwent sentinel lymph node biopsy, which demonstrated metastatic disease.
Targeted fluorescence in situ hybridization (FISH) and chromosomal microarray analysis (CMA)/comparative genomic hybridization (CGH) may add evidence for either a benign or malignant diagnosis [6]. The National Comprehensive Cancer Network (NCCN) guidelines list immunohistochemistry (IHC), comparative genomic hybridization (CGH), fluorescence in situ hybridization (FISH), gene expression profiling (GEP), single-nucleotide polymorphism array (aSNP), and next-generation sequencing (NGS) as ancillary tests that may help in the diagnosis of ambiguous melanocytic lesions. * The American Society of Dermatopathology (ASDP) appropriate use criteria for ancillary testing in melanocytic lesions are rated CGH/CMA, FISH, qRT-PCR, and TERT promoter mutation tests for 80 clinical scenarios. CGH/CMA and FISH were deemed to be usually appropriate in most scenarios involving melanocytic lesions that were suggestive or suspicious for melanoma but not definitive histopathologically [7]. However, classification of melanocytic lesions is not a simple dichotomy even with the aid of all recommended ancillary studies. There are lesions categorized as melanocytomas, with specific histopathologic and molecular findings and malignant potential that is intermediate between benign nevi and melanoma. Melanocytic tumors of uncertain malignant potential (MELTUMPs) are designated as such when the malignant potential is unknown and the histopathologic findings and molecular alterations are insufficient for a definitive diagnosis of melanoma [8]. An accurate classification, whether benign, malignant, intermediate, or uncertain, will guide clinical management appropriately.
- Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines^®^) for Melanoma: Cutaneous V.3.2024. © National Comprehensive Cancer Network, Inc., Plymouth Meeting, PA, USA, 2024. All rights reserved. Accessed [25 November 2024]. To view the most recent and complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.
1.2. Overview of FISH and CMA Techniques
FISH to detect chromosomal abnormalities, including CNAs, is a practical and widely used technique across malignancies. FISH analysis can detect and enumerate specific DNA sequences of targeted genes within cell or tissue samples by using fluorescent probes. This method allows for visualization of the interrogated loci but is typically limited to five or fewer probes per hybridization. FISH requires approximately 50–200 nuclei per probe set, either individual cells fixed on a glass slide or unstained FFPE tissue cut at approximately 3–4 microns, and has a limit of detection between 5 and 20% depending on sample type, abnormality, and probe design.
CMA is a high-resolution technique used to detect genetic imbalances, such as deletions, duplications, and chromosome aneuploidy, across the entire genome. The ability to utilize CMA using DNA extracted from formalin-fixed, paraffin-embedded tissue (FFPE) expanded the exploration of CNAs in melanomas over 25 years ago [9]. Unlike cytogenetic testing for other malignancies, the necessity of CNA evaluation for melanocytic lesions is usually determined after tissue has been processed, fixed in formalin, embedded in paraffin, and assessed histopathologically. Microarray DNA requirements vary by platform but typically require 10 consecutive unstained, ~5 micron-thick sections of FFPE tissue placed on positively charged slides and require approximately 30% lesional cells. The interpretation of CNAs may vary slightly by laboratory. In general, ≥1 megabases (Mb) for deletions, ≥2 Mb for copy gains, and ≥10 Mb for loss of heterozygosity are considered adequate for reporting abnormalities, although changes in fewer Mb are acceptable if involving clinically relevant genes [10].
1.3. Clinical Application of FISH Versus CMA
The four-probe FISH set, including 6p25, 6q23, CEP6, and 11q13, was established by Gerami et al. (2009) [11] and has been shown to detect melanoma with high sensitivity and specificity [12]. Gerami determined that detection of CNAs using that limited set of probes provided excellent distinction between benign and malignant lesions [13]. Its utility has been tested extensively in cutaneous melanomas of various subtypes. The set was subsequently expanded to improve sensitivity with the inclusion of probes for 8q24 and 9p21. The methodology and criteria for defining abnormalities have varied slightly depending on the laboratory, with similar conclusions—FISH distinguishes benign nevi from melanoma with high specificity and sensitivity [14]. Although results in ambiguous lesions may still be challenging and tetraploidy may give false positive results [15], there are many advantages to using FISH to identify CNAs in melanocytic lesions.
FISH can be performed on limited samples without the need to purify DNA [16], which may be challenging in some cases. Because FISH is performed on a tissue section and abnormalities can be assessed in different regions of the same lesion, it has the potential to discriminate between benign and malignant components of a melanocytic proliferation. FISH abnormalities have been detected in regions of melanocytic proliferations that are malignant, while the benign components in the same lesions have no abnormalities, affording the means to stage melanomas more accurately [17,18]. This ability to discriminate between populations has also provided insight into melanoma tumorigenesis. Dysplastic nevi appear to possess some abnormalities, while melanomas arising in dysplastic nevi acquire additional CNAs [18].
However, FISH requires skill to interpret, and the heterogeneity in melanomas may further complicate interpretation, making FISH difficult to automate [19]. Also, melanomas presenting with specific histopathologic characteristics are challenging to evaluate using FISH. For example, CMA seems to have improved sensitivity in detecting superficial spreading melanoma than FISH [20]. FISH may also be more challenging in lesions where the melanocytes are growing in a sclerotic stroma [21]. Furthermore, detection of CNAs using CMA may be more sensitive and specific than FISH in lesions with borderline features, using a cutoff of >3 or ≥3 CNAs for favoring malignant [22,23]. The criteria for counting CNVs are detailed in a review by Ebbelaar et al. [23]. Briefly, aberrations including gains, losses, amplifications, chromothripsis, copy-neutral loss of heterozygosity and chromosomal fusions each count as one, while homozygous losses count as two. Although aneuploidy is counted as one by Ebbelaar, the recommendation proposed by this group excludes counting whole-chromosome gains and losses for cutaneous melanomas given that they are relatively common in benign melanocytic neoplasms, particularly in pediatric patients. These alterations are well documented in proliferative nodules arising within congenital melanocytic nevi [24,25]. Importantly, such large-scale chromosomal copy number changes do not appear to confer adverse biologic behavior in these settings. Accordingly, they are often discounted when enumerating copy number alterations in cutaneous melanocytic tumors. In contrast, copy number changes in atypical and malignant melanocytic cutaneous neoplasms more often reflect underlying genomic instability or crisis, resulting in numerous segmental gains and losses rather than isolated whole-chromosome events. From a biologic standpoint, one would, therefore, not expect isolated whole-chromosome gains or losses to carry the same diagnostic or prognostic significance in this context.
In one study, the sensitivity and specificity for definitive melanomas were 82.4% and 100%, respectively, using FISH and 97.1% and 100%, respectively, using CMA [10]. In the same study, the sensitivity dropped in ambiguous lesions to 47.1% using FISH and 61.2% using CMA [10]. Because CMA has the advantage of assessing the entire genome, while FISH is limited by specific probes, sensitivity and specificity may be improved. Lesions that are negative by FISH may show aberrations by CMA [26]. Most melanomas are associated with sun exposure, and melanomas arising in sun-protected sites may harbor different CNAs [27]; thus, a limited probe set may miss abnormalities at such sites. It is important to note that CMA is also subject to false-negative results. As CMA analyzes the entire cell population of the submitted tissue, CNAs in specimens with a low tumor percentage may not meet the detection threshold, even with microdissection. DNA extraction and purification may be challenging in cases with abundant melanin pigment [28]. Additionally, the size resolution of a particular CMA may exclude potentially significant intragenic CNAs from detection. These assay limitations must be carefully considered when interpreting a negative CMA result [29].
The decision to use either FISH or CMA to assess an ambiguous melanocytic lesion largely depends on availability of the test, adequacy of the specimen, and preference of the pathologist and clinician. CMA, with the capability of analyzing CNAs across the entire genome, is now often preferred. CMA analysis has shown utility in both pediatric and adult populations for analyzing ambiguous lesions, including melanoma arising in large congenital nevi [30,31]. More recently, digital PCR has been documented to yield sensitivity comparable to FISH for targeted CNA detection and may provide an inexpensive alternative if CMA testing is not available [32,33,34].
Given the potential importance of CNA analysis in melanocytic lesions, the Cancer Genomics Consortium Melanoma Working Group set out to review published research with an aim to evaluate the diagnostic utility and clinical significance of CNA analysis. This evidence-based review encompasses the findings. For the purposes of this review, CNAs detected by FISH and CMA were considered in aggregate. While the working group acknowledges differences in sensitivities and resolution of FISH and CMA approaches, as described in the preceding sections, aggregation of CNA data provides a more comprehensive review of the existing literature. Both techniques have demonstrated clinical utility for CNA detection in melanocytic lesions. The genetic landscape of melanoma is complex. Mutations and translocations were not assessed in this review, although certain mutations, such as TERT promoter mutations, may also be helpful in distinguishing benign from malignant lesions, and some mutations may be associated with specific CNAs [35].
2. Methods
Extensive literature searches were conducted for peer-reviewed manuscripts in the English language published from January 1998 through September 2022 through Ovid. Criteria included all manuscripts with findings of copy number abnormalities in melanocytic lesions. Publications with research conducted only on cell lines or animal models were excluded. Case reports and manuscripts with germline CNAs associated with melanoma predisposition were also excluded. In addition, manuscripts with CNAs detected by methods other than CMA or FISH and manuscripts reporting results only from cases in The Cancer Genome Atlas (TCGA) were excluded. A total of 516 manuscripts were assessed, and 235 were retrieved and deemed eligible for inclusion after thorough review by working group members (see Supplementary Figure S1 and Supplementary Table S13) [36]. Working group members assessing individual manuscripts evaluated study quality and risk of bias, and recommendations for exclusion/inclusion were evaluated by other working group members during the selection process. Manuscripts eligible for inclusion were assigned to individual working group members for review and data collection. Data was further reviewed by the primary author (CRB) and any issues were discussed in regular meetings of working group members. The findings of individual manuscripts were tabulated, the number of published cases with a given CNA was summarized, and statistical analysis was performed resulting in a comprehensive meta-analysis. (The meta-analysis is not registered).
The findings were tabulated in aggregate and by specific melanoma subtype, including general cutaneous, uveal, Spitzoid, nevoid, desmoplastic, blue nevus like, mucosal, and acral melanomas, as well as findings in benign melanocytic nevi, when available. Amplifications and gains were combined, as were deletions and losses, to accommodate for differences in reporting between the publications. Only cases with a final diagnosis of benign or malignant were included, regardless of how that final diagnosis was reached. In some cases, the diagnosis was obtained by histopathologic evaluation with or without the aid of immunohistochemistry, and in others, CNA analysis played a role. Lesions with a diagnosis that remained ambiguous or uncertain were not tabulated. Atypical Spitzoid tumors/Spitz melanocytomas were an exception as the diagnosis is considered a definitive category.
We aimed to present the findings from numerous studies in aggregate. One of the challenges was drawing conclusions when the results from the various studies were reported differently. Some manuscripts reported regions on chromosome arms only (i.e., gain of 11p), while others reported findings implicating a specific gene (i.e., 11p15-HRAS). When the locus of an abnormality was reported differently, separate entries were tabulated for statistical purposes. Also, the CMA platforms and FISH probes used to identify aberrations varied. For statistical analysis, identical CNAs were tabulated together regardless of the platform used to identify them.
For each proportion of interest, a 95% confidence interval was calculated by inverting the score test. For the finding of many by CMA, a one-sided lower bound for the population proportion was calculated by the same method. When a proportion was tested to see if it was common (at least 5%), a one-sample test for proportions with Yates continuity correction was performed against the null hypothesis of 5% prevalence. When two proportions were compared, for example, gains compared to losses, a two-sample test for proportions with continuity correction was performed against the null hypothesis that the two proportions were equal. For all statistical tests, ɑ = 0.05 was used as the threshold of significance.
3. Results
3.1. Overview
Overall, gains were significantly more prevalent than losses in general cutaneous, desmoplastic, mucosal, and acral melanoma, while losses were more prevalent in uveal melanoma (all p < 0.005, see Supplementary Table S1). The rates (percentage of cases) reporting gains and losses were also tabulated across each chromosome for primary melanoma of all subtypes combined (see Supplementary Table S2 and Figure 2). The chromosome with the highest rate of gain was chromosome 8, likely due to commonly seen gain in 8q24. The chromosome with the highest rate of loss was chromosome 10, likely due to commonly seen monosomy and separate losses in both 10p and 10q. Gains and losses in specific chromosome arms and regions reported in significantly greater than 5% of cases and published in three or more manuscripts were tabulated (see Table 1 and Table 2). The region with the greatest rate of gain was 6p25 (including RREB1) in 58% (95% CI 55–61%) of melanomas. Although 6q25 (ARID1B) had the highest rate of loss overall at 44% (95% CI 34–55%), it was only reported in mucosal melanomas. Loss of 9p21 (CDKN2A) had the second highest rate of loss at 38.1% (95% CI 36–40%) and was reported in general cutaneous, uveal, Spitzoid, nevoid, mucosal, and acral melanomas at high rates.
3.2. Ocular Melanoma
Uveal melanoma is rare, comprising only 3–5% of all melanomas, with an incidence of approximately 5 cases per million [37,38]. It includes malignancies in the iris, choroid, and ciliary body. CNAs in uveal melanoma have been well studied and carry important prognostic significance. NCCN guidelines recommend molecular or chromosomal testing when a biopsy is performed at the time of diagnosis or on resected tumors to determine prognostic information. The guidelines specify that disomy 3 and gain of chromosome 6p are seen in cases with low risk of metastases, while cases with monosomy 3 and gain of 8q are high risk. * The guidelines are based on a large body of research with patient outcomes. This review confirmed these findings. The results of chromosome 3 ploidy, detected by FISH or CMA, have been published for thousands of cases. Monosomy 3 was found in 49% (95% CI 48–50%) of uveal melanomas [39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109], while whole-chromosome gains (polysomy 3) were reported very rarely [43,60,81,96]. Partial loss of chromosome 3 was seen in approximately 8% (95% CI 7–9%) of cases [51,79,85,101,110,111,112,113]. Monosomy 3 was consistently associated with a worse prognosis and greater risk of metastasis. Monosomy 3 was related to extraocular extension [63] and larger tumor size [73].
- Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines^®^) for Melanoma Uveal V.1.2024. © National Comprehensive Cancer Network, Inc. 2024. All rights reserved. Accessed [25 November 2024]. To view the most recent and complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.
Tumor heterogeneity in uveal melanoma is common [62,95]. Although the higher percentage of cells with loss of chromosome 3 appears to indicate worse patient outcomes [114], detection of monosomy 3 in greater than 5% of tumor cells may be sufficient for increased risk of death due to metastasis [71]. In cases with partial loss, the loss of BAP1 at 3p21 was associated with a worse prognosis than cases without this loss [75,93]. BAP1 may play a critical role in uveal melanoma tumorigenesis because suppression of expression or mutation of this gene was associated with monosomy 3 [75,76]. On the other hand, 6p gain, an abnormality that occurs in 37% (95% CI 35–39%) of uveal melanomas, was rarely seen in tumors with monosomy 3 and was associated with a low risk of metastasis and less aggressive clinical behavior [39,41,42,44,45,51,52,60,61,64,67,68,74,89,96,98,101,105,107,115,116,117,118,119,120]. In particular, amplifications or gains of 6p21 including CDKN1A or 6p25 including RIPK1 or FOXC1 may play a role in improved outcomes [53,94,113]. Gain of 6q was seen in only 5% (95% CI 4–7%) of cases but was also associated with improved outcomes [43,51,60,61,64,74,96,101,105].
Many studies have reported abnormalities of chromosome 8 in uveal melanoma. Polysomy 8, gains of 8q, isochromosome 8q, and both losses and gains of 8p were independently associated with a high risk of metastasis and worse outcomes (see Supplementary Table S3). Specifically, gains of MYC have been reported in 58% (95% CI 52–64%) of uveal melanomas and were associated with worse outcomes. Loss of 1p and gain of 1q were also associated with a worse prognosis (see Supplementary Tables S3 and S4). Gain of 1q is infrequent overall but may be a frequent occurrence in liver metastases [45]. Studies have shown that monosomy 3 observed in combination with other abnormalities, including loss of 1p and gain of chromosome 8, results in a worse prognosis than monosomy 3 alone.
CNAs common in uveal melanomas are distinct from those in cutaneous and mucosal melanomas. This distinction can be exploited when determining primary tumor site in metastases. Detecting monosomy 3 is more indicative of a uveal primary because it is rare in general cutaneous melanoma [55]. Monosomy 3 was reported in only one study in cutaneous melanoma at a rate of 6% (95% CI 0–29%) [10]. Monosomy 3 has also been detected in circulating tumor cells in patients with uveal melanoma and may be a non-invasive method of assessing disease and risk of metastasis [56]. Although gain of 8q was more common in uveal melanoma, 52% (95% CI 51–54%), than general cutaneous melanoma, 26% (95% CI 20–33%), the frequency is high for both.
Conjunctival melanomas harbor CNAs similar to cutaneous and mucosal melanomas and should be considered distinct from uveal melanomas [121].
3.3. General Cutaneous Melanoma
Most cutaneous melanomas have detectable CNAs, and with few exceptions, benign melanocytic nevi do not. In 1998, Bastian et al. determined that 94% of melanomas have CNAs and suspected that technical difficulties had prohibited detection from the remaining 6% [9]. Many subsequent studies have confirmed the significant difference in CNAs between benign nevi and cutaneous melanomas. In our analysis, FISH testing yielded abnormal results in 82% (95% CI 80–84%) of cutaneous melanomas when different probe sets were considered in aggregate (see Supplementary Table S10). The number of cases with published results was close to 1700 (see Table 3). Of the standard targeted regions, 6p25, 6q23, 8q24, 9p21, and 11q13, the most common CNA reported was gain at 6p25, present in 58% (95% CI 54–62%) of general cutaneous melanomas, followed by loss of 9p21, present in 52% (95% CI 49–55%) of published cases (see Table 4). In the general cutaneous melanoma category, 94% (95% CI 92–96%) of melanomas were deemed to have abnormal results favoring malignancy by CMA (see Table 5). A result was deemed likely indicative of malignancy if greater than three CNAs were detected or if there were fewer than three but at least one CNA had been determined to be common in melanomas.
Reportedly, benign nevi that demonstrate no atypia have chromosomal abnormalities in less than 1% of cases, while those with atypical features may harbor CNAs [122]. Gains, losses, abnormal FISH results, and abnormal CNA results by CMA were not significantly greater than 5% for benign cutaneous nevi in this study (see Supplementary Table S9). A gain of 6p25 was reported in three manuscripts in a total of four nevi out of 115 nevi studied for a rate of 3% (95% CI 1–9%) [10,123,124,125]. Whether these nevi demonstrated histopathologic atypia is unknown. The long-term clinical outcomes are also unknown. Some special classes of melanocytic neoplasms have shown more than three CNVs but still had an overall indolent behavior and did not reach morphologic criteria for a malignant diagnosis. Examples include tumors with a MAP2K1 in-frame deletion [126].
3.4. Spitzoid Lesions
Spitzoid lesions range from benign spindled and epithelioid cell nevi or Spitz nevi to atypical Spitzoid tumors/Spitz melanocytomas to malignant Spitzoid melanomas/Spitz melanomas. They can be some of the most difficult to classify on histopathologic grounds alone. Moreover, the terms Spitz melanoma and Spitzoid melanoma have been used interchangeably in the literature; however, they represent two molecularly distinct groups of neoplasms according to the latest WHO classification [127]. Benign lesions can display cellular atypia and other concerning features such as mitoses and Pagetoid spread. Ancillary studies can be very helpful for definitive diagnosis [128]. Previously described as melanoma of childhood, molecular studies have helped elucidate differences between benign Spitz nevi and melanoma [129]. These lesions, including Spitzoid melanomas, are more common in young patients than older adults. Chromosomal analysis of pediatric lesions has demonstrated that malignant lesions in this population also carry CNAs common to melanomas in adults, particularly homozygous loss of CDKN2A [130,131]. The original four-probe FISH set (6p25, 6q23, CEP6, 11q13) was suboptimal when applied to Spitzoid lesions. Addition of probes at 9p21 and CEP9 improved the sensitivity from 70% to 85% in one study [132]. A probe set with 6p25, 11q13, 9p21 and 8q24 demonstrated an overall 94% sensitivity and 98% specificity in another study [133], with improvement in detecting malignant Spitz lesions. When the results of testing with common FISH panels were considered in aggregate, the sensitivity for Spitzoid/Spitz melanoma was significantly less than for general cutaneous melanoma, with a rate of 70% (95% CI 62–77%) in our analysis (see Table 3).
As in general cutaneous melanomas, the most common CNA was gain of 6p25 (54%, 95% CI 43–64%), followed by loss of 9p21 (39%, 95% CI 31–48%) (see Table 4 and Supplementary Table S5). Gains in 6p25 or 11q13 or homozygous loss of 9p21 may have a significant association with aggressive behavior [134].
The rate of abnormalities detected by FISH in benign Spitz nevi was much greater than in other cutaneous nevi. At least one abnormality was detected by FISH in 14% (95% CI 10–19%) of benign Spitz nevi and 19% (95% CI 15–22%) of Spitz melanocytomas. Likewise, CNAs by CMA were higher in Spitz lesions than in other subtypes, with 2% (95% CI 0.1–13%) of benign Spitz nevi and 16% (95% CI 4–40%) of Spitz melanocytomas demonstrating multiple CNAs. Although CNAs are generally rare in benign Spitz nevi, one exception is isolated gain of 11p, which includes HRAS. In one study of 54 benign nevi, the only abnormality observed was gain of 11p in seven nevi, all of which had Spitzoid morphology [135]. We tabulated gain of 11p in 19% (95% CI 15–24%) of benign Spitz nevi and 4% (95% CI 0.7–16%) of Spitzoid/Spitz melanomas (see Supplementary Table S5 and Figure 3). This finding suggests that the Spitzoid/Spitz melanomas with this abnormality may have arisen from benign Spitz nevi.
In addition to gain of 11p including HRAS, copy state transitions (gains or losses) over kinase genes, including ALK, BRAF, ERBB4, FGFR1, MAP3K3, MAP3K8, MERTK, MET, NTRK1, NTRK2, NTRK3, PRKDC, RET, and ROS1, can be identified on CMA studies of Spitz neoplasms, and the finding of a CNA disrupting a kinase gene can point to an oncogenic fusion in one of these genes [3,128,136,137,138,139]. However, because CMA does not detect balanced rearrangements, it is not the ideal method for detecting gene fusions.
Studies of Spitzoid lesions in pediatric cases with clinical follow-up call into question the definition of benign and malignant. When clinical follow-up is available, pediatric patients seem to do well, even when their Spitzoid lesions carry chromosomal aberrations and when sentinel lymph nodes are positive [140]. When the diagnosis of Spitzoid/Spitz melanoma is rendered in a pediatric patient, treatment and follow-up may need to be tailored with the difference to adults in mind.
BAP1-inactivated melanocytomas were formerly considered part of the Spitzoid family of lesions [141]. The discussion of these melanocytomas is beyond the scope of this review. Like other melanocytomas, their malignant potential is considered low or intermediate between benign and malignant [8]. Yet, BAP1 loss may be seen in melanomas, including blue nevus-like melanoma [142], and loss of BAP1 in a melanocytic lesion should prompt a thorough clinical history and consideration of germline testing for BAP1 tumor predisposition syndrome.
Pigmented spindle cell nevi (of Reed) are another subtype of melanocytic lesion that are usually considered part of the Spitzoid family. CNVs in these lesions are not well studied, but pigmented spindle cell nevi may also be distinguished from malignant melanoma with pigmented and spindled cells by the paucity of CNAs in the former, as demonstrated in one study utilizing FISH (original four-probe set—6p25, 6q23, CEP6, 11q13) that found CNAs in only 1 of 15 pigmented spindle cell nevi [123].
3.5. Nevoid Melanoma
Nevoid melanomas are uncommon, comprising less than 1% of all melanomas, and can be diagnostically challenging because they look deceptively benign both clinically and histopathologically [143]. Less data has been published about this melanoma subtype, and less is known about this subtype’s genomic aberrations than others. However, FISH panels were abnormal in 93% (95% CI 84–98%) of published cases (see Table 3). Loss of 9p21 was the most common CNA. Multiple CNAs (>3) by CMA were detected in 85% (95% CI 54–97%) of these melanomas (see Table 5).
Proliferative nodules arising in congenital nevi are other entities with a difficult diagnostic classification and are often assessed together with nevoid melanomas. Like melanoma, they may have increased mitotic activity and increased CNAs; however, they are rare, and limited data is available. Several reports have been published regarding the utility of CNA analysis in distinguishing benign from malignant; taken together, the available data suggests that distinguishing whole-chromosome versus intrachromosomal copy number abnormalities by CMA may aid in the accurate diagnosis of proliferative nodules and distinguish them from nevoid melanomas [24,25,144].
3.6. Desmoplastic Melanoma
Desmoplastic melanoma is associated with high ultraviolet radiation exposure and consists of spindle cells coursing through a fibrotic, scar-like stroma [3]. The malignant melanocytes may be subtle histopathologically and confused with fibroblasts in scar tissue. Detection of abnormalities by FISH may be more challenging in lesions such as these, with their distinct morphology [145,146]. By CMA, 86% (95% CI 56–97%) of cases demonstrated multiple CNAs (see Table 5).
3.7. Blue Nevi and Related Lesions
Like desmoplastic melanoma, the melanocytes in the blue nevus category of lesions usually consist of cells with a spindle morphology. However, these lesions are usually pigmented and have abundant melanophages. Blue nevus-like melanomas are rare. CMA has demonstrated utility in distinguishing between benign and malignant in this category of melanocytic lesions [147]. In this analysis, 80% (95% CI 61–92%) of blue nevus-like melanomas had greater than three CNAs by CMA (see Table 5). FISH was abnormal in 94% (95% CI 68–100%) of blue nevus-like melanomas (original four-probe set—6p25, 6q23, CEP6, 11q13) (see Table 3).
3.8. Mucosal Melanoma
Studies have shown that melanoma arising at mucosal sites, whether genital, oral, or sinonasal, are molecularly distinct from most cutaneous melanomas, perhaps because tumorigenesis is not related to chronic sun damage at these sites [148,149,150,151,152]. Gain of 4q12 harboring KIT was seen more frequently in mucosal melanomas (31%, 95% CI 26–37%) than melanomas at cutaneous sites (6%, 95% CI 4–8%) and may have implications for treatment. Although mutations in KIT make tumors susceptible to targeted therapy, gains may make them resistant [153]. The rate of gain of 6p25 was higher for mucosal melanomas than any other subtype in this study, with a rate of 97% (95% CI 82–100%, see Table 4). FISH was abnormal in 100% of 30 cases reported (using a six-probe FISH set, including 6p25, 6q23, CEP6, 9p21, CEP9, and 11q13), and CMA detected greater than three abnormalities in 95% (95% CI 72–100%) of cases (see Table 3 and Table 5).
3.9. Acral Melanoma
Awareness of the differences in CNAs between mucosal, acral and cutaneous melanomas from other sites may be helpful when evaluating challenging lesions [154]. Melanomas occurring at acral sites demonstrate CNAs that involve chromosomes 5p, 11q, and 12q more often than melanomas at other sites [135]. Gains of 5p15 encompassing TERT were reported in 41% (95% CI 38–45%) of acral melanomas and only 28% (95% CI 22–36%) of general cutaneous melanomas (see Figure 4). Moreover, gains were more common in acral melanomas than in melanomas at other sites [154]. This observation was confirmed by our study, which showed significantly more gains (33%, 95% CI 32–35%) than losses (7%, 95% CI 6.5–8.4%) in acral melanomas (p < 0.001). Differences between mucosal, acral, and melanoma at other cutaneous sites may also be seen in 10q23 and 5p15 (see Figure 4).
The four-probe FISH set has been tested specifically in acral melanomas, and the results demonstrate high sensitivity for these lesions [14]. In this study, FISH was abnormal in 88% (95% CI 81–92%) of acral melanomas (see Table 3), and abnormalities were detected by CMA in 100% of published cases (see Table 5).
3.10. Implications for Prognosis and Treatment
As knowledge of the impact of CNAs in melanoma grows, questions arise regarding not only the utility for diagnosis but also the implications they may carry for prognosis and treatment. Recent studies with clinical follow-up paired with CNA analysis in both primary and metastatic lesions in the same patient are providing important evidence for the role of CNAs. However, to our knowledge, there have been no large-scale prospective studies to evaluate the impact of CNAs in melanocytic lesions.
As expected, both primary melanomas and metastatic melanomas harbor CNAs that can be detected by FISH and CMA. The rates between primary and metastatic were similar, and there were no significant differences (see Supplementary Table S6). Yet, the detection of CNAs by FISH may be independently, significantly associated with aggressive behavior and worse outcomes [155]. The number of CNAs may also be correlated with clinical behavior, with a greater number associated with more aggressive behavior in some studies [156,157,158]. The presence of significant aneuploidy and loss of heterozygosity have been detected in advanced disease [4].
One form of CNA observed in a subset of malignancies, including melanomas, is chromothripsis or a pattern of clustered CNAs on a single chromosome arm or subregion or sometimes multiple chromosome arms or subregions. Chromothripsis was originally described in 2011 [159] and has been associated with a poor prognosis in one study of 20 melanomas, where chromothripsis or complex copy alterations were associated with reduced overall survival [160]. A more recent study of cancers using whole-genome sequencing, which included 106 melanomas, showed that over half of melanomas had evidence of chromothripsis, suggesting that this type of alteration is oncogenic in at least a subset of melanomas [161]. Chromothripsis is a mechanism for activation of kinase genes in Spitz melanocytic neoplasms via complex structural rearrangements that generate oncogenic fusions involving kinase genes, many of which are targetable with clinically approved kinase inhibitor therapies [162,163,164,165]. There is currently insufficient evidence to support enumerating genomic segments of chromothriptic gains or losses on CMA in order to determine the likelihood that a melanocytic neoplasm is malignant; however, accumulating evidence shows that chromothripsis promotes tumor progression via activation of oncogenes and inactivation of tumor suppressor genes [166,167,168].
Multiple studies have focused on a specific abnormality in an attempt to elucidate which may be more common in metastases and, therefore, imply a worse prognosis when detected in a primary lesion. For example, one study concluded that deletion of 1p36 was more common in metastatic lesions [169]. Our analysis demonstrated a similar rate: 34% (95% CI 27–42%) in primary cutaneous melanomas and 35% (95% CI 27–45%) in metastases. Gains of PREX1 on 20q13 were shown to indicate lower metastasis-free survival in one study [170]. Our data showed similar rates of 20q13 gains in primary (27%, 95% CI 21–33%) and metastatic lesions (26%, 95% CI 17–37%). In contrast, gains at 7q34 harboring BRAF were more common in metastatic lesions (58%, 95% CI 49–66%) than primary melanomas (30%, 95% CI 26–35%). Copy number gains may be associated with BRAF mutations [171], and gains may be associated with a shorter time to disease progression [172].
Gains at 8q24 (MYC) and 11q13 (CCND1), both common, were reportedly associated with more aggressive behavior and metastases [173,174,175,176]. Gains of 1q (reported in 45% of metastases and 29% of primary cutaneous melanomas) and 6p (reported in 50% of metastases and 40% of primary cutaneous melanomas) may also predict lower survival [177]. Losses of 6q (reported in 50% of metastases and 27% of primary cutaneous melanomas) and 10q (reported in 40% of metastases and 39% of primary cutaneous melanomas) were associated with a poor prognosis and/or ulceration [178]. EGFR amplification/polysomy 7 may also be associated with greater tumor thickness and more aggressive behavior [179,180,181]. Polysomy 7 was seen in 57% of metastases and 25% of primary cutaneous lesions in our study (see Supplementary Table S7). When gains of EGFR were reported specifically, they demonstrated a rate of 34% in metastases and 17% in primary cutaneous lesions, supporting an association with more aggressive behavior (see Supplementary Table S7). Multiple studies have shown that increased PHIP copy number on 6q14 is associated with metastasis and decreased survival [182,183,184]. However, many additional gains and losses may be implicated [185,186], and our analysis found no reports of PHIP gains in metastases, although the rate of gain in primary lesions was 34%.
To better understand the differences between metastases and primary melanomas, a comparison was made of CNAs in general cutaneous melanomas with the inclusion criteria of being reported by at least three manuscripts in at least 50 cases each of primary melanoma and metastases. There was a significant difference in the rates in 12 CNAs. Half of these were more common in metastases, including gains of 3p13 (MITF), 7p11 (EGFR), and 7q34 (BRAF) (see Supplementary Table S7 and Figure 5). The same inclusion criteria identified 12 CNAs with no significant difference between primary and metastatic lesions, including loss of 1p36, loss of 9p21 (CDKN2A), and loss of 10q23 (PTEN) (see Supplementary Table S8 and Figure 6).
Treatment of aggressive and metastatic melanoma is continuously under investigation. Mutations are routinely assessed for targeted therapy. The question remains whether CNAs should be evaluated routinely as well. TERT copy number gain, more common in acral melanomas (41% vs. 28% in general cutaneous melanomas), may be indicative of response to therapy [187]. Although immune checkpoint inhibitors have made a significant impact in treating advanced stage melanomas, some patients progress. A study found that MDM2, MDM4, and EGFR amplifications were not associated with progression in patients with mucosal or acral melanomas on immune checkpoint inhibitors [188]. However, copy number gains of 12q14 including CDK4 were more common in patients resistant to anti-PD1 therapy [189]. CNAs of PDL1 on 9p24 were uncommon; losses were seen in 10% of cases across subtypes (see Table 2), and studies have shown they do not predict response to anti-PD1 targeted therapy [190]. Targeted therapy in melanomas harboring MET amplifications is under investigation [191]; we found a rate of 26% for this CNA in all subtypes. As targeted therapies emerge across malignancies, those associated with CNAs should be considered when applicable to melanomas.
3.11. Other Ancillary Techniques
Immunohistochemistry has been a valuable tool used by pathologists to assess melanocytic lesions for many years. Specifically, stains that are positive in melanocytes, such as SOX10, S100, and Melan-A/MART1, can help pathologists evaluate architectural features and identify malignant characteristics, such as asymmetry, Pagetoid spread, and dermal invasion. Stains for p16, Ki-67 and HMB45 are often evaluated in conjunction with determination of staining patterns indicative of malignancy, and studies have shown a high concordance with cytogenetic results [192,193,194]. PRAME is a newer stain that may also have diagnostic utility. For challenging lesions, the specificity of PRAME staining may be as high as 95%; however, the sensitivity may be only 75%, and positive staining in benign Spitz nevi is a potential hazard with interpretation [195,196]. Studies have shown a concordance of 90% between PRAME staining and cytogenetic studies in ambiguous melanocytic lesions [195]. The accessibility, low cost, rapid turnaround time and ease of IHC make it primary among ancillary tests. When the results remain ambiguous, evaluation of CNAs should be considered. For challenging cases, cytogenetics provides additional information that, when used in conjunction with histopathologic and IHC results, may yield improved diagnoses [193].
The ASDP also indicates that testing for TERT promoter mutations may have utility in determining malignancy in ambiguous melanocytic lesions. The specificity may be as high as 98.6%, while the sensitivity is lower at 77.9%, and the frequency of this mutation may vary by melanoma subtype [197,198].
Gene expression profiling (GEP) may also serve as a useful ancillary tool for diagnosis. In one study, it showed 80% concordance with FISH in unambiguous cases and 73% concordance in ambiguous cases; however, FISH results showed better concordance with histopathologic assessment (97% vs. 83%) [199]. In another study, FISH and GEP showed 69% agreement in ambiguous lesions, and CMA demonstrated better correlation with morphologic interpretation than either FISH or GEP [200]. Yet, agreement with FISH was 50.9% and 57.1% with CMA when ambiguous lesions were included [201]. Additional research is necessary to determine the validity of GEP across melanoma subtypes. For example, in desmoplastic melanoma, GEP and CMA were discordant in four cases out of nine [202].
Detection of CNAs in melanocytic lesions by CMA and FISH is well established. Publications using methods other than CMA and FISH were excluded from this review. However, there is increasing evidence that NGS and MLPA can accurately detect CNAs, and these platforms may have certain advantages for clinical use [203]. For example, NGS testing is able to assess copy number changes in addition to SNVs; therefore, it has the potential to replace SNP-array testing of melanoma in the future.
4. Discussion
Inaccuracies in melanoma diagnosis can carry critical implications for patient management. Ample studies have shown that cytogenetic analyses in melanocytic lesions are valuable for malignancy determination and, in many cases, prognosis determination. In aggregate, the total number of gains, losses, and FISH abnormalities was uncommon in benign nevi. They were not significantly greater than 5% (see Supplementary Table S9). While CNAs were present in the majority of malignant melanomas detected by either FISH or CMA across subtypes, there are differences in CNA findings between melanoma subtypes, which may be a reflection of variations in the molecular pathways involved in tumorigenesis and the involvement of damage caused by ultraviolet radiation. An algorithmic approach to the use of CNA in the evaluation of melanocytic lesions is suggested in Figure 7, applicable across subtypes.
In assessing conclusions from hundreds of publications in the field, several limitations were encountered. Cases that remained ambiguous after all diagnostic tools were applied were not counted in the aggregate data. Yet, CNA analysis in ambiguous lesions is the most pertinent for daily practice and patient care, as these are the lesions that are most difficult to diagnose on histopathologic grounds alone. Whether or not a final diagnosis was rendered before or after the incorporation of CNA results, cases were included in statistical analysis together, which may have resulted in incorporation bias.
Because the dichotomous view of melanocytic lesions as benign or malignant may be too biologically simple, some studies favored classifying lesions on a spectrum [204]. It is important to remember that all findings must be considered in conjunction. The number of CNAs alone does not render a diagnosis of melanoma. A recent study of seven melanocytic lesions with Spitzoid morphology and amplification of a mutant NRAS gene concluded that all seven lesions were indefinite for melanoma, although additional CNAs were present in all cases [205]. When reported, the results for dysplastic nevi were considered benign. We found insufficient data on CNAs in dysplastic nevi to reach significance in classification into mild, moderate, and severe atypia. Several studies have shown that severely dysplastic nevi have more aberrations than mild and moderately dysplastic nevi but fewer than melanoma [16,122].
Conclusions from evidence-based review in this study are limited by the paucity of follow-up data. The treatment of melanoma with complete excision with negative margins is often curative for early-stage tumors. These may be the most difficult tumors to diagnose histopathologically because the early and superficial melanomas may not be clearly demonstrating the full spectrum of histopathologic abnormalities characteristic of malignancy. Positive outcomes, when present, may be attributed to early diagnosis and adequate treatment as well as prognostically less aggressive melanomas.
Although our literature search was extensive, all searches are limited by parameters and search engines. Furthermore, new research continues to emerge. Fortunately, with each new publication, awareness of CNA assessment to aid in diagnosis of melanocytic lesions is increasing among pathologists and dermatologists.
5. Evidence-Based Recommendations
CMA or FISH do not need to be performed on all melanocytic lesions to assess malignancy. Those lesions considered ambiguous after assessment of histopathologic features, including immunohistochemical studies, may be good candidates for evaluation of CNAs (see Figure 7).For uveal melanomas, CNA studies for prognosis are validated and established.Although prognostic information may be gained by the evaluation of CNAs in primary cutaneous melanomas, routine testing has not been established.Differences in common CNAs between uveal and primary cutaneous melanomas may be exploited in determining the origin of metastases.CMA may be preferred to FISH because of its ability to assess the entire genome. FISH may be more helpful in small lesions where DNA extraction may yield insufficient material.FISH panels including probes for 6p25, 6q23, 8q24, 9p21, and 11q13 are reasonable and provide adequate sensitivity and specificity in most cases. Results are supportive of malignancy when at least one recurring CNA is detected.When results of FISH studies are inconclusive or negative, CMA, with the ability to identify abnormalities throughout the genome, may be performed.CMA is considered supportive of malignant melanoma when more than three CNAs are detected or when fewer CNAs are detected but those identified include an abnormality that is common in melanoma (>5%, see Table 1 and Table 2). CMA with three or fewer CNAs does not completely exclude a diagnosis of melanoma, and CMA with greater than three CNAs does not definitively diagnose melanoma.As with all testing modalities, limitations exist with CMA and FISH testing, and negative results do not completely exclude the presence of CNAs. Tumor heterogeneity, morphology, and percentage of tumor cells in a sample may limit detection.No single ancillary study is sufficient for diagnosis. Results must be considered in conjunction with clinical presentation and histopathologic findings. Evaluation of CNAs may add support to favor either a benign or malignant diagnosis. Although CNA testing adds evidence, a definitive diagnosis must include all other results in conjunction. Some lesions may remain ambiguous after all ancillary testing is performed and expert consultation is obtained.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Elder D.E. Precursors to melanoma and their mimics: Nevi of special sites Mod. Pathol.200619 S 4S 2010.1038/modpathol.380051516446715 · doi ↗ · pubmed ↗
- 2Tucker M.A. Melanoma epidemiology Hematol. Oncol. Clin. N. Am.20092338339510.1016/j.hoc.2009.03.01019464592 PMC 3234163 · doi ↗ · pubmed ↗
- 3Elder D.E. Bastian B.C. Cree I.A. Massi D. Scolyer R.A. The 2018 World Health Organization Classification of Cutaneous, Mucosal, and Uveal Melanoma: Detailed Analysis of 9 Distinct Subtypes Defined by Their Evolutionary Pathway Arch. Pathol. Lab. Med.202014450052210.5858/arpa.2019-0561-RA 32057276 · doi ↗ · pubmed ↗
- 4Vergara I.A. Mintoff C.P. Sandhu S. Mc Intosh L. Young R.J. Wong S.Q. Colebatch A. Cameron D.L. Kwon J.L. Wolfe R. Evolution of late-stage metastatic melanoma is dominated by aneuploidy and whole genome doubling Nat. Commun.202112143410.1038/s 41467-021-21576-833664264 PMC 7933255 · doi ↗ · pubmed ↗
- 5Nardone B. Martini M. Busam K. Marghoob A. West D.P. Gerami P. Integrating clinical/dermatoscopic findings and fluorescence in situ hybridization in diagnosing melanocytic neoplasms with less than definitive histopathologic features J. Am. Acad. Dermatol.20126691792210.1016/j.jaad.2011.05.05121962759 · doi ↗ · pubmed ↗
- 6Mesbah Ardakani N. Harvey N.T. Wood B.A. Polypoid Compound Melanocytic Proliferations: A Clinicopathological Study Am. J. Dermatopathol.20194157858410.1097/DAD.000000000000137531335410 · doi ↗ · pubmed ↗
- 7AUC Committee Members Fung M.A. Vidal C.I. Armbrecht E.A. Andea A.A. Cassarino D.S. Comfere N.I. Emanuel P.O. Ferringer T. Hristov A.C. Appropriate use criteria for ancillary diagnostic testing in dermatopathology: New recommendations for 11 tests and 220 clinical scenarios from the American Society of Dermatopathology Appropriate Use Criteria Committee J. Cutan. Pathol.20224923124510.1111/cup.1413534536035 · doi ↗ · pubmed ↗
- 8Duncan L.M. Elder D.E. Piepkorn M.W. Knezevich S.R. Blokx W.A.M. Bosenberg M. Busam K.J. Carr R. Cook M.G. Gerami P. Shifts in Cutaneous Melanocytic Tumor Diagnostic Terminology: Melanocytoma, MPATH-Dx V 2.0 and the WHO Skin 5J. Cutan. Pathol.2025539110010.1111/cup.1478840181698 · doi ↗ · pubmed ↗