Real-World Treatment Patterns and Survival in Patients with ROS1-Positive Advanced Non-Small Cell Lung Cancer in Canada and Europe
Winson Y. Cheung, Adam Lee, Helena Bote de Cabo, Kathrin Burdenski, Petros Christopoulos, Bárbara Pinto-Correia, Simon Deshayes, Nicolas Girard, Pooja Hindocha, Áine Madden, Marta Mella, Joana Moreira, Silvia Rizzi, Delvys Rodríguez Abreu, Marta Soares, Joseph Thomas, Maria Han

TL;DR
This study examines real-world treatment patterns and survival outcomes for patients with ROS1-positive advanced non-small cell lung cancer in Canada and Europe, finding that targeted therapies may offer better survival than non-targeted treatments.
Contribution
The study provides real-world evidence on treatment patterns and survival outcomes for ROS1-positive advanced NSCLC patients across multiple European countries and Canada.
Findings
ROS1-targeted therapies showed a tendency for longer survival compared to non-targeted treatments like chemotherapy.
Median overall survival for patients on ROS1-targeted therapy was 47.9 months, versus 29.3 months for non-targeted therapy.
Most patients had a de novo diagnosis of advanced NSCLC, with limited survival outcomes highlighting the need for better treatments.
Abstract
There is currently an insufficient amount of real-world information on treatments and outcomes among people with advanced-stage non-small cell lung cancer (NSCLC) who have mutations in the ROS1 gene, termed ROS1-positive advanced NSCLC. We used pooled data collected between 2009 and 2024 from clinical sites in Canada, France, Germany, Portugal, and Spain to assess patients with ROS1-positive advanced NSCLC with the aim of describing patient characteristics, treatment patterns, and survival. In this study, results from 103 patients with ROS1-positive advanced NSCLC who received systemic anticancer therapy indicated a tendency for longer survival using currently available treatment that specifically targets ROS1-positive disease than with non-targeted treatments, such as chemotherapy. However, the observed survival outcomes were less than optimal, highlighting the importance of more…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
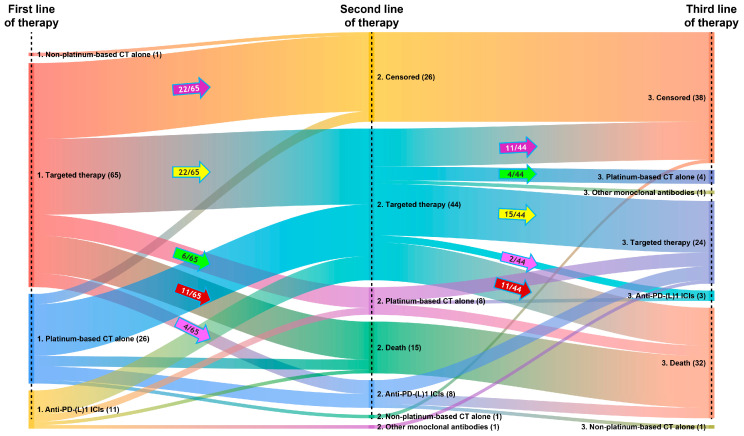 Figure 1
Figure 1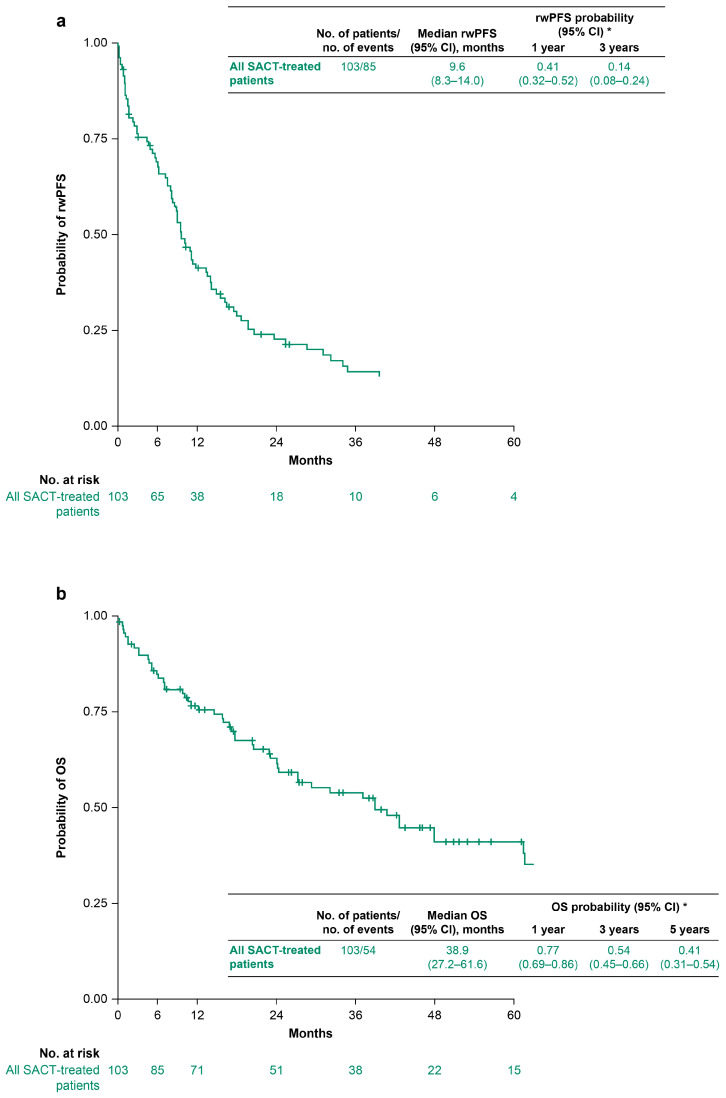 Figure 2
Figure 2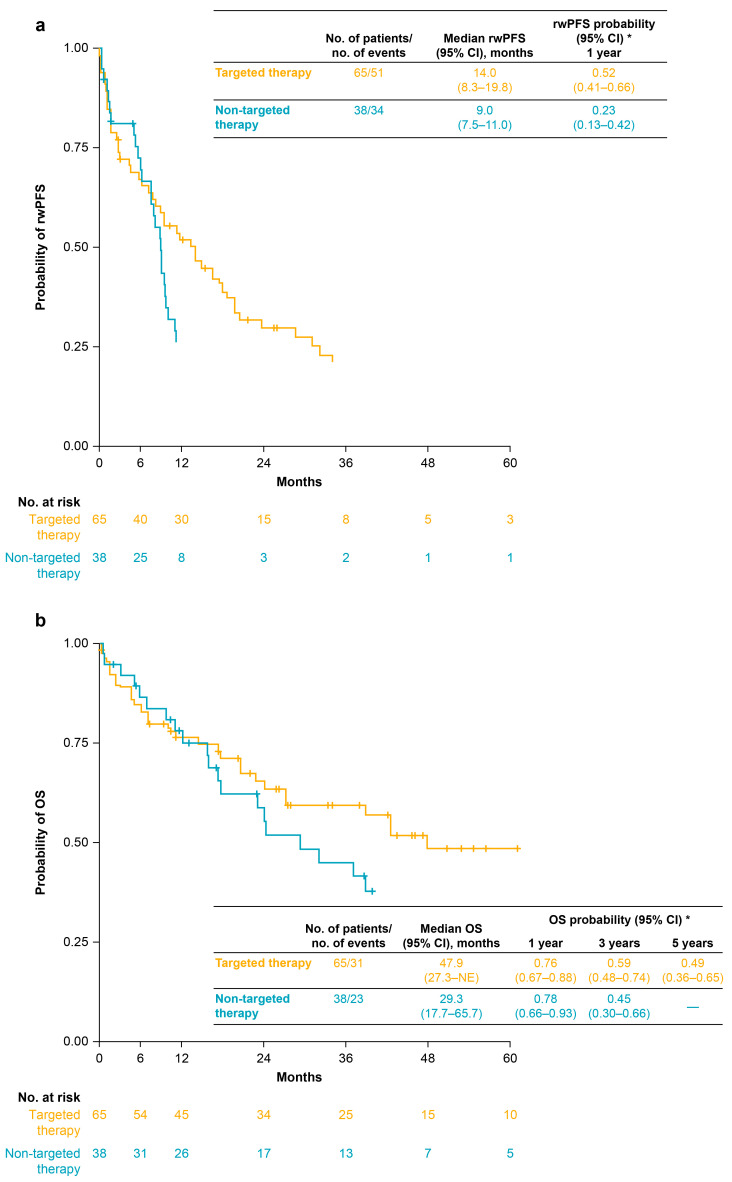 Figure 3
Figure 3- —Bristol Myers Squibb
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Treatments and Mutations · Lung Cancer Diagnosis and Treatment · Lung Cancer Research Studies
1. Introduction
About 50% of patients with non-squamous non-small cell lung cancer (NSCLC) carry actionable genomic alterations, including those in the EGFR, KRAS, ALK, or ROS1 genes [1]. Due to the prevalence of these actionable alterations, North American and European guidelines recommend broad-spectrum biomarker testing for all patients with advanced non-squamous cell carcinoma and for certain subpopulations with squamous cell carcinoma (e.g., younger patients and never-smokers) [2,3,4]. Alterations in the ROS1 gene, termed ROS1 rearrangements, occur in approximately 0.5–3% of tested patients with NSCLC [5,6,7,8,9,10], and are more frequent in younger patients, female patients, never-smokers, and those with advanced disease; they are also more prevalent in lung adenocarcinomas than in other NSCLC histologies [5,6].
Crizotinib, a tyrosine kinase inhibitor (TKI) originally used to treat ALK-positive NSCLC, was the first agent to receive national/regional approvals in North America and Europe specifically for the treatment of patients with ROS1-positive disease, with approval in the United States and Europe in 2016 and in Canada in 2017 [11,12,13]. Entrectinib subsequently received national/regional approval for the treatment of ROS1-positive NSCLC in the United States in 2019 and in Canada and Europe in 2020 [14,15,16], with national/regional approval of repotrectinib following in the United States in 2023 and Canada and Europe in 2025 [17,18,19]. Recently, taletrectinib was also approved in the United States [20]. In alignment with these approvals, North American and European guidelines for patients with ROS1-positive advanced NSCLC were updated to recommend first-line treatment with crizotinib, entrectinib, or repotrectinib [3,4,21], with the latest North American guidelines also recommending taletrectinib [4]. Recommended second- and later-line approaches vary but typically involve use of an alternative ROS1-targeting TKI, an ALK-targeting TKI that has shown benefits in patients with ROS1-positive NSCLC (e.g., lorlatinib [22]), or, if no alternative TKI options are available, other systemic therapy approaches, such as platinum-based chemotherapy [3,4,21]. However, despite regional-level approvals and guideline-based recommendations, timings and decisions regarding reimbursement of ROS1-targeting therapies vary considerably across countries. For example, although crizotinib was approved for ROS1-positive disease in Europe in 2016, it has only been reimbursed in France since 2020 (with funding restricted to second- or later-line settings only) [23] and in Portugal since 2022 [24]. Likewise, despite the European approval of entrectinib in 2020, an unfavorable decision on reimbursement was recorded in France in 2021 [25], and it has only been reimbursed in Portugal since 2023 [26]. Similarly, although Canadian authorities approved crizotinib in 2017 and entrectinib in 2020, pan-Canadian reimbursement of these agents was not recommended until 2019 and 2021, respectively [27,28], with initiation of provincial reimbursement occurring even later (e.g., funding of crizotinib in the province of Alberta was only initiated in July 2020) [29].
Real-world data on patients with ROS1-positive advanced NSCLC remain scarce, for both those treated with ROS1-targeting therapies and those not receiving targeted treatments. Moreover, based on real-world studies showing a median overall survival (OS) of only 2–3 years after first- or second-line crizotinib [30,31,32], and clinical studies suggesting comparable efficacy for crizotinib and entrectinib [33,34], there remains an unmet need for alternative therapies for ROS1-positive disease. As such, further real-world studies could provide useful insights into clinical care pathways, treatment decisions, and survival outcomes in this patient population. Onco-Optimise (formerly known as I-O Optimise) is an ongoing, international collaborative research initiative designed to provide timely insights into the evolving management of various thoracic malignancies, including NSCLC [35,36]. As part of Onco-Optimise, the present study was designed to leverage data from multiple high-quality real-world data sources to describe demographic and clinical characteristics, treatment patterns, and associated survival outcomes among patients with ROS1-positive advanced NSCLC in Canada and Europe.
2. Materials and Methods
2.1. Study Design and Patient Population
This descriptive observational retrospective cohort study was conducted using secondary data pooled from clinical sites included in the Oncology Evidence Network (OEN). The OEN is a collaboration of large hospital centers with strong clinical informatics capabilities across multiple countries (primarily Canada and European countries) that work with the support of an industrial partner (IQVIA) to provide high-quality real-world oncology data reflecting routine clinical care [37]. For this study, data were derived from patient electronic medical records collected at Oncology Outcomes in Canada (using data from the province of Alberta); the Institut Curie and Center Hospitalier Universitaire de Caen in France; the University Cancer Center Frankfurt, Thoraxklinik at Heidelberg University Hospital, and Vivantes Klinikum in Friedrichshain in Germany; the Portuguese Oncology Institute of Porto in Portugal; and the Hospital Universitario Insular de Gran Canaria and Hospital Universitario 12 de Octubre in Spain. Based on the design of the OEN, a common data model was implemented across these sites to ensure data harmonization and consistency in data curation and reporting [37].
The site-specific patient inclusion periods for this study all occurred between 2009 and 2023 and were driven by the respective timings of ROS1 rearrangement testing implementation at each site. Patients were included in the study at their date of diagnosis of advanced NSCLC (inclusion date) and followed until death or end of the study period, whichever occurred first. Site-specific follow-up periods extended from the start date of each site-specific patient inclusion period up to 2024, allowing at least 1 year of potential follow-up at each contributing site before the end of the study period.
The study population included all patients within the participating sites who were aged at least 18 years at initial lung cancer diagnosis and who had advanced NSCLC (including patients with a de novo diagnosis and those with recurrent disease) and confirmed ROS1-positive disease. A “de novo diagnosis” refers to patients with newly diagnosed locally advanced or metastatic (stage III or IV) NSCLC whose initial treatment was non-curative and who received a first line of systemic anticancer therapy (SACT) or best supportive care (BSC). “Recurrent disease” refers to patients first diagnosed with stage I–III NSCLC who received curative treatment (protocol-defined as surgery, radiotherapy, neoadjuvant therapy, and/or adjuvant therapy administered in the curative setting) but whose disease progressed to advanced NSCLC before receiving a first line of SACT or BSC, with the date of recurrence captured at the participating sites. Confirmation of ROS1-positive status was based on tests performed between 30 days before diagnosis of advanced NSCLC and the end of the site-specific patient inclusion period. Patients required a positive ROS1 test using a non-immunohistochemistry technique (e.g., fluorescence in situ hybridization or next-generation sequencing) or a positive ROS1 test using immunohistochemistry, but without evidence of a negative test using non-immunohistochemistry technique. Patients were excluded if they had any previous primary malignancy (excluding non-melanoma skin cancer) in the 5 years before initial NSCLC diagnosis or at any point after their diagnosis date, or if they participated in a clinical trial before the start of their first line of SACT.
Analyses were conducted for the overall population and stratified by Canadian versus European sites.
2.2. Variables
Data on patient demographic and clinical characteristics were collected at the time of initial NSCLC diagnosis and/or diagnosis of advanced NSCLC. Testing patterns for ROS1 rearrangements were assessed in the full study population. For the classification of initial treatment, patients were categorized as receiving either SACT (patients who were administered at least one line of SACT within the first 180 days after diagnosis of advanced NSCLC) or BSC (patients who were either administered a treatment for management of disease-related symptoms only or were untreated within the first 180 consecutive days after diagnosis of advanced NSCLC). For this analysis, SACT was further categorized as “platinum-based chemotherapy alone,” “non-platinum-based chemotherapy alone,” “targeted therapy,” “anti-programmed death-(ligand) 1 [PD-(L)1] immune checkpoint inhibitor (ICI) monotherapy,” “anti-PD-(L)1 ICI plus chemotherapy,” or “other monoclonal antibodies,” as defined in Supplementary Table S1. Lines of therapy and treatment sequences were determined by each participating site based on available data.
Real-world progression-free survival (rwPFS) and OS were assessed in patients receiving SACT. For this analysis, rwPFS was defined as the time from the start date of first line of SACT to the date of recorded disease progression or date of death from any cause, with the date of recorded disease progression based on radiological and/or clinical progression as assessed by physicians at the respective clinical sites. Patients without a recorded rwPFS event were censored at the earliest of the start of second line of therapy, the date of loss to follow-up, the date of starting a clinical trial, or the end of the study period. OS was defined as the time from start date of first line of SACT to the date of death due to any cause. Patients without an OS event were censored at the earliest of the date of loss to follow-up, the date of starting a clinical trial, or the end of the study period.
2.3. Statistical Analysis
Descriptive statistics were used for data on demographic and clinical characteristics, ROS1 rearrangement testing patterns, and treatment patterns. Time-to-event endpoints (rwPFS and OS) were described using the Kaplan–Meier method. For subgroups with fewer than 20 patients, both the Kaplan–Meier curve and associated median value were suppressed; additionally, all Kaplan–Meier curves were truncated when the number of patients at risk fell below 10. Based on OEN study requirements regarding the privacy of Canadian data, for any data stratified by geographic region (Canada vs. Europe), patient numbers between one and nine were masked and patient numbers ≥10 were rounded to the nearest 10, with associated percentages rounded to the nearest 5%. No imputation methods were used to handle missing data except for date variables. Due to the descriptive nature of the study, no statistical testing was performed and confounding adjustment was not conducted.
3. Results
3.1. Patients
In total, 108 patients with confirmed ROS1-positive advanced NSCLC were included (Table 1). Overall, the median (interquartile range [IQR]) duration of follow-up from diagnosis of advanced NSCLC was 24.1 (10.9–46.8) months and was similar among patients from Canada (26.5 [11.2–43.4] months) and Europe (23.4 [10.9–44.4] months). One hundred and five patients (97.2%) had a de novo diagnosis of advanced NSCLC, with 89 of these patients (82.4% of the overall study population) having metastatic (stage IV) disease at diagnosis and the remaining 16 (14.8% of the overall study population) having locally advanced disease at diagnosis (stage IIIA, n = 4; IIIB, n = 9; IIIC, n = 3). Only three patients (2.8%) had recurrent advanced disease, after initial diagnosis at stage IB (n = 1), IIIA (n = 1) or IIIC (n = 1). For these three patients, the median (IQR) time from initial diagnosis of NSCLC to advanced diagnosis was 24.7 (4.6–24.7) months.
Overall, median (IQR) age at diagnosis of advanced NSCLC was 57 (48–68) years, 68 patients (63.0%) were female, 106 (98.1%) had non-squamous cell NSCLC (all adenocarcinoma), 58 (53.7%) were never-smokers, and 20 (18.5%) had brain metastases at diagnosis of advanced NSCLC (Table 1). Ten patients (9.3%) were diagnosed with advanced NSCLC between 2009 and 2015 (i.e., before first formal approval of crizotinib for ROS1-positive disease), a further 57 (52.8%) were diagnosed with advanced NSCLC between 2016 and 2019 (i.e., after first regional/country-specific approval of crizotinib for ROS1-positive disease, but before reimbursement in this setting in most of the participating countries), and the remaining 41 patients (38.0%) were diagnosed between 2020 and 2023. Characteristics of the patients from Canada and Europe were mostly similar, although the Canadian population was slightly younger and included a larger proportion of never-smokers (Supplementary Table S2).
3.2. ROS1 Testing
Most testing samples originated from tissue (n = 95; 88.0%) and came from the primary tumor site (n = 60; 55.6%; Table 2). Overall, 78 patients (72.2%) underwent multi-gene (gene panel) testing, with the most common techniques being next-generation sequencing (n = 48; 44.4%) or fluorescence in situ hybridization (n = 45; 41.7%). The majority of patients (n = 98; 90.7%) were tested for ROS1 rearrangements after diagnosis of advanced NSCLC, with a median (IQR) time from diagnosis to testing of 31.0 (11.0–110.0) days; 10 patients (9.3%) were tested for ROS1 rearrangements before diagnosis of advanced NSCLC, with a median (IQR) time from testing to diagnosis of 6.0 (1.0–9.0) days (Table 2).
3.3. Treatment Patterns and Pathways
Of the 108 included patients, 103 (95.4%) received at least one line of SACT and five (4.6%) received BSC. Sixty-five of the 103 patients treated with SACT (63.1%) received first-line targeted therapy, most commonly crizotinib monotherapy (n = 45; 43.7%), crizotinib-based combination regimens (n = 10; 9.7%), or entrectinib monotherapy (n = 9; 8.7%) (Table 3). Thirty-eight of the 103 patients treated with SACT (36.9%) received first-line non-targeted therapy, most commonly platinum-based chemotherapy (n = 26; 25.2%) (Table 3). First-line use of anti-PD-(L)1 ICIs plus chemotherapy, anti-PD-(L)1 ICI monotherapy, and non-platinum chemotherapy was limited (Table 3).
Of the 103 patients treated with SACT, 15 (14.6%) died and 26 (25.2%) were censored during first-line treatment; 62 patients (60.2%) went on to receive a second line of therapy (Figure 1). Forty-four of the 62 patients (71.0%) treated with a second line of SACT received second-line targeted therapy, most commonly crizotinib monotherapy (n = 19; 30.6%) or lorlatinib monotherapy (n = 12; 19.4%) (Table 3). Eighteen of the 62 patients (29.0%) treated with a second line of therapy received second-line non-targeted therapy, most commonly platinum-based chemotherapy (n = 8; 12.9%) or anti-PD-(L)1 ICI monotherapy (n = 7; 11.3%) (Table 3).
Of the 62 patients who received a second line of SACT, 17 (27.4%) died and 12 (19.4%) were censored during second-line treatment; 33 patients (53.2%) went on to receive a third line of therapy (Figure 1). Twenty-four of the 33 patients treated with a third line of SACT (72.7%) received third-line targeted therapy, most commonly lorlatinib monotherapy (n = 15; 45.5%) (Table 3). Only 17 of the 103 patients administered at least one line of SACT (16.5%) went on to receive a fourth line of therapy, and only five (4.9%) received a fifth line of therapy.
The most common treatment sequences from first to second line of therapy involved targeted therapies followed by targeted therapies. During first-line treatment, 33 of the 65 patients who received first-line targeted therapy died or were censored; the remaining 32 patients went on to receive second-line therapy, of whom 22 (68.8%) were treated with a second line of targeted therapy (Figure 1). Similarly, the most common treatment sequences from second to third line of therapy also involved targeted therapies followed by targeted therapies. During second-line treatment, 22 of the 44 patients who received second-line targeted therapy died or were censored; the remaining 22 patients went on to receive a third line of therapy, of whom 15 (68.2%) were treated with third-line targeted therapy (Figure 1).
3.4. Survival Outcomes
Among the 103 patients treated with SACT, median (95% confidence interval [CI]) rwPFS was 9.6 (8.3–14.0) months and median (95% CI) OS was 38.9 (27.2–61.6) months (Figure 2). For the 65 patients who received first-line targeted therapy (i.e., mostly crizotinib monotherapy or crizotinib-based combination regimens), median (95% CI) rwPFS and OS were 14.0 (8.3–19.8) months and 47.9 (27.3–not estimable) months, respectively (Figure 3). For the 38 patients who received first-line non-targeted therapy (i.e., platinum-based chemotherapy alone, non-platinum-based chemotherapy alone, anti-PD-[L]1 ICI monotherapy, or combinations of anti-PD-[L]1 ICIs with chemotherapy), median (95% CI) rwPFS and OS were 9.0 (7.5–11.0) months and 29.3 (17.7–65.7) months, respectively (Figure 3).
In SACT-treated patients from Canada, median (95% CI) rwPFS and OS were 8.3 (4.4–15.6) months and 42.6 (27.3—not estimable) months, respectively; in SACT-treated patients from Europe, they were 11.0 (8.9–16.5) months and 38.9 (23.1–65.7) months, respectively (Supplementary Figure S1).
4. Discussion
Using data retrospectively pooled from clinical sites in Canada and four European countries (France, Germany, Portugal, and Spain) between 2009 and 2024, this descriptive real-world observational study provides insights into patient demographic and clinical characteristics, testing patterns, treatment patterns and pathways, and survival outcomes for patients with advanced NSCLC carrying the relatively rare ROS1 rearrangement.
The population of patients providing data for this study had a relatively low median age (vs. patients with NSCLC not carrying actionable genomic alterations) and contained a predominance of female patients, never-smokers, and patients with adenocarcinoma, which aligns with literature describing common characteristics of patients with ROS1 rearrangements [5,6]. The study population was also similar to ROS1-positive patient populations in other real-world studies conducted in North America, Europe, and Asia [30,31,32,38,39,40,41,42].
The most commonly administered treatment types in this study were ROS1-targeted therapies, which were received by 63% of patients as first line of therapy, by 71% as second line of therapy, and by 73% as third line of therapy. The most common treatment was crizotinib (as monotherapy or in combination regimens) as first and second line of therapy, and lorlatinib monotherapy as third line of therapy. It was also noteworthy that the most common treatment sequences from first to second line of therapy and from second to third line of therapy involved targeted therapies followed by targeted therapies. The treatment patterns observed in this study were reflective of treatment approvals and availability in the participating regions and countries over the study period. With the analyses being conducted between 2009 and 2024, crizotinib would have been the only ROS1-targeted therapy approved in North America and Europe for most of the study [11,12,30]. Moreover, although entrectinib was approved for the treatment of ROS1-positive NSCLC in both Canada and Europe in 2020, it was restricted to patients who had not previously received crizotinib (in Canada) or who had not previously received any ROS1 inhibitor (in Europe) [15,16], which likely limited its use beyond the first-line setting in this study, and probably contributed to the high use of lorlatinib (an ALK inhibitor frequently used off label in patients with ROS1-positive NSCLC) in the second- and third-line settings. Finally, it is important to consider the influence of country-specific reimbursement decisions on the observed treatment patterns. As detailed in the Introduction, there was substantial variability in official timings and decisions regarding reimbursement of ROS1-targeting therapies across the countries participating in this study, a feature supported by a survey of pathologists or clinical scientists in molecular pathology and oncologists conducted across numerous European countries in 2023 [43]. Overall, despite Canadian and European regional-level approvals of crizotinib in 2016/2017 [12,13] and entrectinib in 2020 [15,16], both drugs were not reimbursed for the first-line treatment of patients with ROS1-positive NSCLC in most of the participating countries for most of the study period, which likely contributed to the proportion of patients in this study receiving first-line non-targeted therapy for ROS1-positive disease.
The median rwPFS and OS reported in this study for patients with ROS1-positive advanced NSCLC receiving first-line targeted therapy (mostly comprising crizotinib alone or in crizotinib-based combination regimens) was 14.0 and 47.9 months, respectively. These values align with ranges of survival reported in other real-world studies (PFS, 8.6–29.0 months; OS, 16.2–36.2 months) [30,31,32,38,42] and clinical trials (PFS, 15.9–22.8 months; OS, 32.5–54.8 months) [44,45,46,47,48] conducted across the world and where patients were treated with crizotinib. However, assessing outcomes from the current study in the context of other relevant real-world studies and clinical trials is difficult due to the relative scarcity of real-world data, as well as differences in study designs and patient populations. A particular challenge is that many of the previous studies have evaluated the efficacy of crizotinib when used as either first- or second-line therapy for advanced ROS1-positive NSCLC or even when used at any point in the treatment pathway [32]. The impact that this has on survival outcomes was demonstrated in a recent global meta-analysis of real-world studies of crizotinib for ROS1-positive advanced NSCLC, which showed that the pooled median PFS with crizotinib at any line of therapy was 14.5 months, whereas the pooled median PFS for first-line crizotinib was 18.1 months [49]. In addition, while many of the ROS1-positive patient populations have similar overarching characteristics (e.g., a high proportion of female patients and never-smokers), they vary in other characteristics that might impact survival. For example, clinical trials of crizotinib typically included no or only a small proportion of patients with Eastern Cooperative Oncology Group performance status >1 [44,45,46,47], whereas several of the real-world study populations included more than 10% of such patients [30,31,42], which has been shown to impact OS outcomes [31]. It is also noteworthy that crizotinib has poor intracranial penetration, and patients with existing brain metastases have shown worse survival outcomes versus those without in both clinical trials and real-world analyses [30,32,44,47]. As such, the relative proportions of patients with brain metastases (both present at start of therapy and developing during treatment) would likely impact survival outcomes in the respective studies/trials.
Results from this study indicated a tendency for longer survival with first-line ROS1-targeted therapy (mostly crizotinib) than with first-line non-targeted therapy. Although this appears to further support the benefits of crizotinib as first-line treatment for ROS1-positive advanced NSCLC, the observed median rwPFS of 14.0 months and OS of 47.9 months (i.e., approximately 1 and 4 years, respectively) from the start of treatment remain limited, especially considering the relatively young age of the ROS1-positive population (median age of 57 years). Despite these useful insights, it is important to acknowledge potential confounding factors for the comparison of patients receiving targeted versus non-targeted therapy in this study, including possible differences in baseline characteristics (e.g., Eastern Cooperative Oncology Group performance status, comorbidities, or metastatic sites) between these treatment subgroups. Additionally, the inclusion of patients diagnosed with advanced ROS1-positive NSCLC before availability/reimbursement of ROS1-targeted therapy (as well as anti-PD-[L]1 ICIs) in their respective countries (i.e., pre-2015/2016) may have impacted these outcomes. For these patients, chemotherapy would have been the only therapeutic option, regardless of whether they would be considered suitable for chemotherapy if diagnosed after more contemporary treatments became available.
Real-world data on first-line use of entrectinib for ROS1-positive advanced NSCLC are scarce, but results from an integrated analysis of three clinical trials (reporting a median PFS of 15.7 months and a median OS of 47.8 months) and from a simulated treatment comparison analysis based on phase 1–2 studies have suggested that entrectinib is unlikely to provide significant survival improvements over crizotinib [33,34]. Similarly, real-world data on the first-line use of repotrectinib are limited due to its recent approval. However, in the TRIDENT-1 trial of repotrectinib for patients with TKI-naive ROS1-positive advanced NSCLC, median PFS was 35.7 months, median OS was not reached (with an 18-month OS rate of 88%), and encouraging clinical activity against intracranial disease was observed [50]. Moreover, in a recent indirect comparison analysis in patients with TKI-naïve ROS1-positive locally advanced or metastatic NSCLC, repotrectinib was associated with statistically significant improvements in PFS, and numerically improved objective response rate and duration of response relative to crizotinib and entrectinib [51]. In addition, although real-world data are unavailable at present, two other novel ROS1-targeting therapies, taletrectinib and zidesamtinib, have shown encouraging efficacy and safety data in patients with ROS1-positive NSCLC [52]. Taken together, these emerging data suggest the potential for further improvements in survival outcomes for this patient population.
Several limitations should be considered when interpreting the data presented here. First, as is typical for real-world analyses of rare diseases, the study included a relatively small overall sample size, which could impact data interpretation, particularly for some of the smaller subgroups assessed. Second, the study used secondary data from electronic medical records, which could have been subject to point-of-care data entry errors (information bias or measurement errors) that would not be detected nor corrected during the analyses. Third, due to the descriptive nature of the study, there was no statistical testing performed and no adjustments for potential confounding factors. Fourth, due to masking rules preventing a comprehensive review of Canadian patients, and because data for individual European countries were not available, the study was not able to determine if there were any country-specific differences that might have influenced the results. Fifth, possible country- or site-specific differences in the measurement and/or recording of disease progression could have impacted the reported rwPFS outcomes. Sixth, and finally, the study collected data on treatment patterns and/or survival outcomes between 2020 and 2022, and these data may have been impacted by the COVID-19 pandemic. Despite these limitations, a strength of the current study was the use of high-quality, real-world data sources that helped provide a holistic view of the treatment landscape for patients with ROS1-positive advanced NSCLC across Canada and Europe. Furthermore, the use of multiple data sources across the various countries ensured that sufficient data were available for the analysis of patients with the relatively rare ROS1 rearrangement, with the included sample (N = 108) larger than many previous real-world studies of ROS1-positive NSCLC [30,38,40,41]. Finally, the harmonization of data across sites using a common data model was important in ensuring a consistent approach to data curation and reporting throughout the current analyses [37].
5. Conclusions
This study provides unique multicountry insights into the demographic and clinical characteristics of patients with ROS1-positive advanced NSCLC and associated treatment patterns and survival outcomes. Although the results indicated a tendency for longer survival using currently available ROS1-targeted therapy versus non-targeted therapy for patients with ROS1-positive advanced NSCLC, outcomes were limited, highlighting the importance of more effective emerging therapeutic options for ROS1-positive disease.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Meyer M.L. Fitzgerald B.G. Paz-Ares L. Cappuzzo F. Janne P.A. Peters S. Hirsch F.R. New promises and challenges in the treatment of advanced non-small-cell lung cancer Lancet 202440480382210.1016/S 0140-6736(24)01029-839121882 · doi ↗ · pubmed ↗
- 2Pennell N.A. Arcila M.E. Gandara D.R. West H. Biomarker testing for patients with advanced non-small cell lung cancer: Real-world issues and tough choices Am. Soc. Clin. Oncol. Educ. Book 20193953154210.1200/EDBK_23786331099633 · doi ↗ · pubmed ↗
- 3Hendriks L.E. Kerr K.M. Menis J. Mok T.S. Nestle U. Passaro A. Peters S. Planchard D. Smit E.F. Solomon B.J. Oncogene-addicted metastatic non-small-cell lung cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up Ann. Oncol.20233433935710.1016/j.annonc.2022.12.00936872130 · doi ↗ · pubmed ↗
- 4Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Non-Small Cell Lung Cancer V.8.2025. © National Comprehensive Cancer Network, Inc. 2025. All rights reserved. Accessed August 21, 2025. To view the most recent and complete version of the guideline, go online to NCCN.org. NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way
- 5Zhu Q. Zhan P. Zhang X. Lv T. Song Y. Clinicopathologic characteristics of patients with ROS 1 fusion gene in non-small cell lung cancer: A meta-analysis Transl. Lung Cancer Res.2015430030910.3978/j.issn.2218-6751.2015.05.0126207220 PMC 4483477 · doi ↗ · pubmed ↗
- 6Fois S.S. Paliogiannis P. Zinellu A. Fois A.G. Cossu A. Palmieri G. Molecular epidemiology of the main druggable genetic alterations in non-small cell lung cancer Int. J. Mol. Sci.20212261210.3390/ijms 2202061233435440 PMC 7827915 · doi ↗ · pubmed ↗
- 7Griesinger F. Eberhardt W. Nusch A. Reiser M. Zahn M.O. Maintz C. Bernhardt C. Losem C. Stenzinger A. Heukamp L.C. Biomarker testing in non-small cell lung cancer in routine care: Analysis of the first 3,717 patients in the German prospective, observational, nation-wide CRISP Registry (AIO-TRK-0315)Lung Cancer 202115217418410.1016/j.lungcan.2020.10.01233358484 · doi ↗ · pubmed ↗
- 8Salas C. Martin-Lopez J. Martinez-Pozo A. Hernandez-Iglesias T. Carcedo D. Ruiz de Alda L. Garcia J.F. Rojo F. Real-world biomarker testing rate and positivity rate in NSCLC in Spain: Prospective Central Lung Cancer Biomarker Testing Registry (Lung Path) from the Spanish Society of Pathology (SEAP)J. Clin. Pathol.20227519320010.1136/jclinpath-2020-20728033722840 PMC 8862081 · doi ↗ · pubmed ↗