A Complete Response to Immunotherapy in a Patient with Locally Advanced Squamous Cell Lung Cancer Harboring a Novel TMEM178B::BRAF Fusion: A Case Report
Juan Carlos Redondo-González, Iñigo San Miguel, Marta Rodríguez-González, Juan Carlos Montero, José María Sayagués, Mar Abad Hernández, Emilio Fonseca Sánchez, Edel Del Barco-Morillo, Alejandro Olivares-Hernández

TL;DR
A patient with squamous lung cancer and a rare BRAF fusion achieved complete response to immunotherapy, suggesting new treatment possibilities.
Contribution
This case report identifies a novel TMEM178B::BRAF fusion in squamous lung cancer and links it to successful immunotherapy response.
Findings
A patient with a TMEM178B::BRAF fusion achieved complete radiological response after chemoradiotherapy and immunotherapy.
The fusion suggests a potential predictive marker for immunotherapy response in squamous NSCLC.
The case highlights the importance of molecular profiling in patients without traditional risk factors.
Abstract
Background: The development of advanced genomic sequencing techniques now makes it possible to identify novel biomarkers and guide the design of targeted therapeutic strategies. For advanced squamous non-small cell lung cancer (NSCLC), V-Raf murine sarcoma viral oncogene homolog B1 (BRAF) fusions have not been evaluated as a therapeutic target. However, agents that block the pathway activated by these fusions have shown efficacy in other solid tumors, such as melanoma, astrocytoma, acinar carcinoma of the pancreas, and papillary thyroid tumors. Case Report: Here, we present the case of a patient with locally advanced squamous NSCLC and minimal smoking history who was found to harbor a TMEM178B::BRAF fusion. Following curative-intent chemoradiotherapy (CRT) and subsequent maintenance immunotherapy, the patient achieved a complete radiological response at 12 months, accompanied by a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
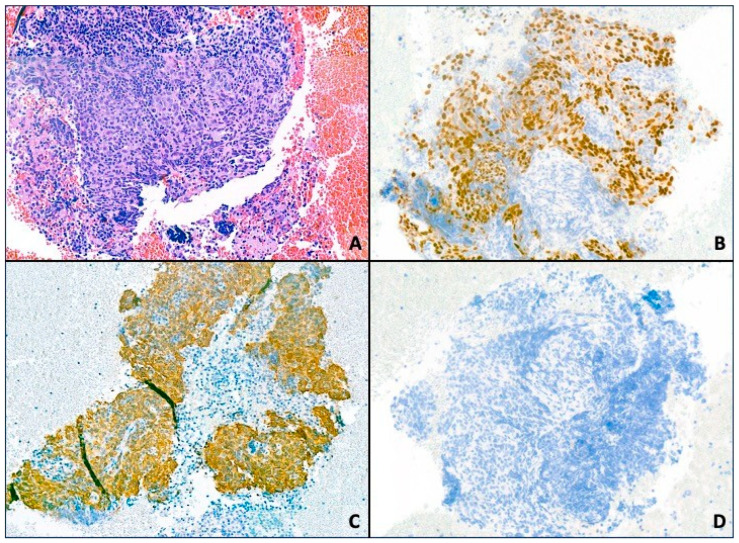 Figure 1
Figure 1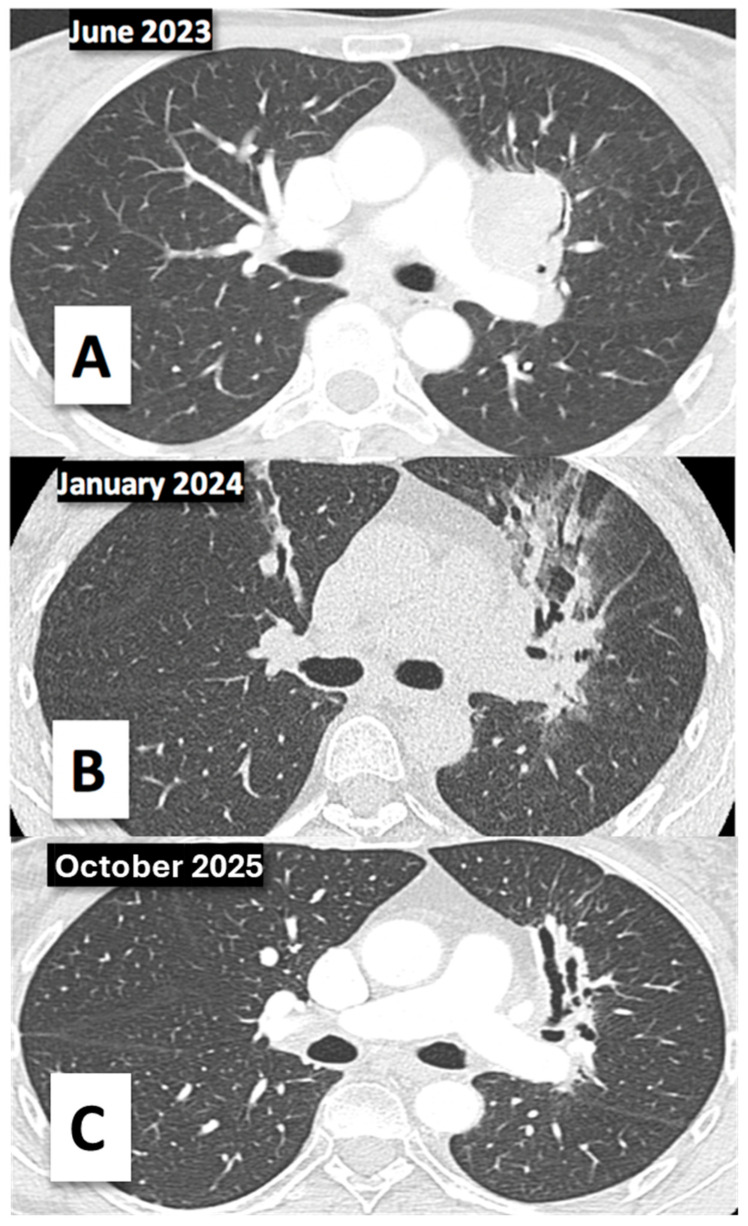 Figure 2
Figure 2| Case | Date of Publication | Diagnosis | Age (yr)/Gender | BRAF Fusion | Targeted Therapy | Response |
|---|---|---|---|---|---|---|
| Castellano-Damaso et al. [ | 23 May 2024 | Low-grade glioma | 18/male |
| Trametinib | PR |
| Zhou et al. [ | 28 March 2024 | Tenosynovial giant cell tumor | 27/male |
| Surgery + Chemotherapy | CR |
| Yasui et al. [ | 23 February 2024 | Lung adenocarcinoma | 75/female |
| Trametinib | PR |
| Hirosi et al. [ | 22 September 2023 | Melanoma | 71/female |
| Dabrafenib/trametinib | PR |
| Heinrich et al. [ | 26 June 2023 | Pancreatic cancer adenocarcinoma | ~ |
| Chemotherapy + ICI | CR |
| Toshiro et al. [ | 6 November 2022 | Melanoma | 73/female |
| ICI | PR |
| Kong et al. [ | 30 January 2023 | Lung adenocarcinoma | 53/female |
| iEGFR | PR |
| Clarck et al. [ | 21 May 2022 | Melanoma | 19/female |
| ICI | PR |
| Yang et al. [ | 19 August 2022 | Lung adenocarcinoma | 60/male |
| Trametinib | PR |
| Yun-Tse et al. [ | 18 March 2022 | Lung adenocarcinoma | 67/male | Dabrafenib/trametinib/cacpmatinib | SD | |
| Domen et al. [ | 17 January 2022 | Myoepithelial carcinoma | 57/female |
| Cobimetinib | PR |
| Cheng-You et al. [ | 5 November 2021 | Lung adenocarcinoma | 66/male |
| Trametinib | PR |
| Kervarrec et al. [ | 1 October 2021 | Primary melanoma of the lung | 55/female |
| ICI | SD |
| Chew et al. [ | 15 April 2021 | Melanoma | 40/female |
| Trametinib | PR |
| Hasegawa et al. [ | 18 June 2021 | Rectal cancer | 40/female |
| Chemotherapy + iEGFR | PR |
| Shao-Jie et al. [ | 24 May 2020 | Malignant soft tissue tumor | 52/female | Crizotinib | SD | |
| Isaacson et al. [ | 25 February 2019 | Urothelial carcinoma | 69/male |
| Trametinib | PR |
| You-cai et al. [ | 4 March 2019 | Lung adenocarcinoma | 60/male |
| Vemurafenib | PR |
| Huat et al. [ | 12 February 2018 | Cholangiocarcinoma | 58/male |
| Chemotherapy | PR |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Treatments and Mutations · Cancer Immunotherapy and Biomarkers · Lung Cancer Diagnosis and Treatment
1. Introduction
Lung cancer currently has the highest incidence of any cancer in both sexes, with 2,480,675 new diagnoses in 2022, accounting for 12.4% of all new cancer diagnoses worldwide. In the female subgroup it already ranks second (908,630 cases, 9.4%) [1]. Global statistics estimate that 15% of lung cancers in men and 53% in women are not attributed to smoking, representing 25% of all lung cancer cases worldwide. Historically this subgroup has been under-represented in clinical trials and research studies, but it constitutes a pathological entity with different molecular development. Few reports have explored their structure and impact on clinical course [2].
In recent years, the expanding use of next-generation sequencing (NGS) as a standard of care has enabled the identification of uncommon but actionable alterations found in fewer than 5% of lung cancer patients. Although biomarker research in NSCLC has advanced considerably over recent years, most discoveries have focused on adenocarcinoma, leaving squamous cell carcinoma with limited molecular targets and making it an increasingly important priority for current research efforts. One of the key genes under investigation is BRAF (V-Raf murine sarcoma viral oncogene homolog B1), first described as an oncogenic driver in 2002, and a critical signaling molecule in the MAPK/ERK pathway [3]. BRAF encodes a RAF kinase downstream of EGFR and ROS1, whose activation promotes uncontrolled cell growth and tumorigenesis, with well-known roles in tumors such as pilocytic astrocytoma, low-grade neuroepithelial tumors, and acinar cell carcinoma of the pancreas.
In NSCLC, BRAF alterations, including point mutations, rearrangements, and other less common variants, are found in approximately 4–4.5% of cases overall. In adenocarcinomas, the prevalence is higher, reported to be between 1% and 5%, with many studies centering around 2–4% [4]. Notably, BRAF rearrangements represent a particularly rare subset of these alterations, occurring in only 0.2% of NSCLC cases [4]. By contrast, BRAF mutations in squamous cell carcinoma are exceedingly rare; for example, in a cohort of nearly 1000 NSCLC patients (646 adenocarcinomas, 231 squamous), no BRAF V600E/K mutations were detected in squamous cases [5]. Another study that analyzed the mutational status of BRAF in 2001 NSCLC cases found only one squamous carcinoma with a BRAF mutation among all BRAF-mutated samples [6].
In this paper, we report a patient with locally advanced squamous cell carcinoma (SCC) harboring a TMEM178B::BRAF fusion who was treated with concurrent chemoradiotherapy followed by one year of maintenance immunotherapy, achieving a complete radiological response at the end of the treatment and maintaining this response to date, two years after completing therapy.
2. Case Report
We present the case of a 54-year-old female patient with no significant medical history, except for her father who died at the age of 70 due to a gastric adenocarcinoma. She was an ex-smoker, with a pack-year index of 7.5 and did not consume alcohol or other toxic substances.
In June 2023, she presented to the emergency department with pleuritic pain in the left hemithorax accompanied by a persistent cough. There were no signs of constitutional syndrome or other associated symptoms, and her laboratory tests were unremarkable. A chest X-ray revealed a left perihilar lesion with increased density.
In the staging study a nodule in the lingula (4.3 × 2.6 cm) was described, compatible with a primary tumor, which was associated with a left perihilar conglomerate measuring 3.5 × 3.2 cm, along with subcarinal and right paratracheal lymphadenopathy measuring 1.7 cm. The tumor was staged as cT2bN3M0 (stage IIIB), confirmed by PET-CT. The sample obtained by bronchoscopy confirmed basaloid-type SCC. The diagnosis was not morphologically straightforward, as the tumor lacked clear features of squamous differentiation such as keratinization, and we therefore relied on immunohistochemistry. The histological immunophenotype was: Cam 5.2+, p40+, TTF1−, and CK7−. CAM 5.2 was mainly used to confirm the epithelial nature of the tumor, although it does not determine the squamous subtype. Tumor cell expression of programmed death ligand 1 (PD-L1) was 40%, determined by the immunohistochemistry assay pharmDX^®^ clone 22C3 in the cell membrane (Figure 1).
By October 2023, a multidisciplinary committee decided on concomitant chemoradiotherapy (CRT) with radical intent and to expand the molecular study using massive genetic sequencing (NGS) due to the low exposure of carcinogenic agents in the patient. Rearrangements at the BRAF gene level (TMEM178B::BRAF) were detected using an Oncomine Precision Assay (OPA) genomic panel and an Ion Torrent GX5 Chip on a Genexus sequencer (Thermo Fisher^®^, Waltham, MA, USA). The event was classified as a gain-of-function fusion, with 90 supporting reads. No additional concurrent genetic alterations (including SNVs, indels, or copy number variations) were identified.
She began treatment with carboplatin (AUC 5) and paclitaxel (175 mg/m^2^) every 21 days concurrent with radiotherapy, which was completed after two cycles and 33 sessions (total dose of 66 Gy to the primary tumor and lymphatic area). She was unable to receive the third cycle due to hematological toxicities (grade 2 thrombocytopenia, CTCAE 5.0). She achieved a partial response in her December 2023 CT scan and began subsequent maintenance immunotherapy (durvalumab 10 mg/kg every two weeks) 6 weeks after the completion of chemoradiotherapy. However, treatment had to be discontinued due to grade 2 pneumonitis, confirmed by high-resolution CT, which required corticosteroid therapy at 1 mg/kg. After that, the patient was successfully treated for a respiratory tract infection with a regimen of antibiotic therapy based on amoxicillin and clavulanic acid.
Finally, the patient reached complete radiological response in April 2024, which was maintained at her last re-evaluation in October 2025 (Figure 2). She is currently undergoing quarterly CT scans with an excellent quality of life and is completely asymptomatic, with an ECOG performance status of 0.
3. Discussion
In recent decades, a substantial body of knowledge has accumulated regarding biomarkers in NSCLCs. Despite these advances, most clinically relevant biomarkers have been identified in the adenocarcinoma subtype, where more than 1 in 3 patients (33% of cases) benefit from targeted molecular therapies [7].
In contrast, treatment options and prognosis for SCC remain comparatively limited, making this subtype a critical focus of ongoing research. Notably, only 1 in 25 patients (approximately 5%) with SCC exhibit clearly targetable genomic alterations, meaning that just a small subset of this population is able to benefit from targeted therapies [8]. This low prevalence underscores the importance of comprehensive molecular profiling to identify the minority of SCC patients who may still achieve meaningful clinical benefit from precision-based treatments. In this regard, SCC subsets have been characterized by The Cancer Genome Atlas (TCGA) to support the development of new, effective targeted therapies tailored to individual patients [9].
Only 2% of NSCLCs harbor BRAF gene alterations, which may represent actionable targets and have the potential to improve clinical outcomes. In our case, NGS was performed individually to identify actionable alterations, given the patient’s young age, squamous cell carcinoma diagnosis, minimal few risk factors and low smoking history (IPA 7.5 pack-years). This analysis revealed a TMEM178B::BRAF fusion.
BRAF mutations account for approximately 1% of NSCLCs, with the BRAF V600E mutation representing around 50% of these cases. This mutation has already demonstrated clinical utility when combined with MEK 1/2 inhibitors for the treatment of various solid tumors [10]. Rearrangements at the level of the BRAF gene represent a different pathogenic mechanism. They were first described in 2005 in thyroid cancer, and like point mutations they contribute to aberrant activation of the MAPK signaling pathway [11]. Since then, BRAF fusions have been identified across a wide spectrum of solid tumors, suggesting a broader oncogenic role beyond their initial description. In fact, several recent reports have documented BRAF rearrangements in diverse malignancies, often associated with variable but sometimes meaningful responses to targeted therapies. Table 1 summarizes the clinical cases published to date, highlighting the heterogeneity of tumor types harboring BRAF fusions, the diversity of fusion partners, and the therapeutic strategies implemented. Their potential as a therapeutic target in solid tumors has been recently explored by Ross et al. [12], who reported a discrete representation of all NSCLC cases (around 0.2%). The study highlighted the effectiveness of BRAF inhibitors, particularly in spitzoid melanoma, pilocytic astrocytoma, pancreatic acinar and papillary thyroid cancers.
In contrast to NSCLCs with other actionable driver mutations, BRAF-mutated NSCLC has been shown to exhibit high susceptibility to immune checkpoint inhibitors. Notably, BRAF mutations and their functional classes do not appear to negatively affect the clinical outcomes of advanced NSCLCs and are instead associated with immunotherapy susceptibility [13]. In this context, several published case reports and small series have documented meaningful clinical responses to immune-checkpoint inhibitors in tumors harboring non-V600 BRAF mutations. For example, durable responses to anti-PD-1 agents have been described in patients with class II and class III BRAF mutations, even in metastatic settings refractory to multiple prior lines of therapy [14,15]. Moreover, retrospective cohorts have suggested that BRAF-mutant, particularly non-V600, NSCLCs may exhibit higher tumor-infiltrating lymphocyte densities and immune-active transcriptional signatures compared with other oncogene-driven subsets [16,17]. These observations, although derived from limited sample sizes, support the notion that the functional class of BRAF mutation shapes tumor immunobiology and may help guide therapeutic decision-making in advanced NSCLC.
Currently, combinations of dabrafenib–trametinib or encorafenib–binimetinib are indicated for advanced NSCLC with BRAF V600E mutation. However, the use of BRAF inhibitors such as vemurafenib as monotherapy may paradoxically enhance MAPK pathway signaling in tumors with BRAF fusions, making their benefits uncertain. This may be explained by the fact that BRAF fusions typically function as Class II BRAF alterations (RAS-independent dimers), which accounts for their intrinsic resistance to first-generation BRAF monomer inhibitors. Although case reports have explored targeted approaches, the study by Wang et al. [18] described a novel VPS41::BRAF fusion identified in a patient with lung adenocarcinoma using NGS but did not report targeted treatment outcomes.
Recent studies suggest that the activation of the MAPK pathway could regulate PD-L1 expression in tumor cells [19]. This regulation occurs primarily at the transcriptional level, where downstream components of the MAPK cascade, particularly ERK, enhance PD-L1 gene transcription. As a result, tumor cells upregulate PD-L1 on their surface, inhibiting T-cell activity and enabling immune evasion, which is a key mechanism of cancer progression and therapeutic resistance [20].
Importantly, BRAF fusions, like other activating alterations in BRAF, can drive constitutive MAPK pathway activation. Unlike the canonical BRAF V600E mutation, BRAF fusion proteins signal as RAS-independent dimers that strongly and continuously activate MEK–ERK. This sustained MAPK activation can further amplify PD-L1 transcription, potentially creating a more immunosuppressive tumor microenvironment. Therefore, tumors harboring BRAF fusions may exhibit elevated PD-L1 expression and distinct immune-evasive properties, with implications for both targeted therapy and response to immune checkpoint inhibitors. In this sense, understanding the link between MAPK activation and PD-L1 expression can guide the development of more effective combination therapies. Targeting the MAPK pathway (e.g., MEK inhibitors) may decrease PD-L1 expression in tumor cells, thereby enhancing their susceptibility to immune-mediated attack. However, trials focusing on the response to treatments in NSCLC with BRAF fusions are still scarce and their results are still limited.
Another possible explanation for the patient’s response to immunotherapy could be a relatively high tumor mutational burden (TMB), which is often associated with increased neo-antigen presentation and improved immune recognition. In addition, favorable characteristics of the tumor microenvironment, such as the presence of infiltrating cytotoxic T cells or a pro-inflammatory cytokine profile, may have contributed to enhancing the therapeutic effect.
4. Conclusions
The case presented represents the first SCC harboring a TMEM178B::BRAF fusion described in the literature achieving a complete radiological response after immunotherapy treatment. This case highlights the potential value of expanding genetic analysis in these patients. Looking ahead, standardizing the use of comprehensive genomic sequencing will be essential to identify individuals who may benefit from targeted therapies. This approach will help broaden the existing evidence base, particularly in patients with low exposure to carcinogens, and should be considered regardless of tumor stage or histological subtype.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H. Ferlay J. Siegel R.L. Laversanne M. Soerjomataram I. Jemal A. Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries CA Cancer J. Clin.2021712092493353833810.3322/caac.21660 · doi ↗ · pubmed ↗
- 2Sun S. Schiller J.H. Gazdar A.F. Lung cancer in never smokers—A different disease Nat. Rev. Cancer 200777787901788227810.1038/nrc 2190 · doi ↗ · pubmed ↗
- 3Davies H. Bignell G.R. Cox C. Stephens P. Edkins S. Clegg S. Teague J. Woffendin H. Garnett M.J. Bottomley W. Mutations of the BRAF gene in human cancer Nature 200241794995410.1038/nature 0076612068308 · doi ↗ · pubmed ↗
- 4Yan N. Guo S. Zhang H. Zhang Z. Shen S. Li X. BRAF-Mutated Non-Small Cell Lung Cancer: Current Treatment Status and Future Perspective Front. Oncol.20221286304310.3389/fonc.2022.86304335433454 PMC 9008712 · doi ↗ · pubmed ↗
- 5Brustugun O.T. Khattak A.M. Trømborg A.K. Beigi M. Beiske K. Lund-Iversen M. HellandÅ. BRAF-mutations in non-small cell lung cancer Lung Cancer 201484363810.1016/j.lungcan.2014.01.02324552757 · doi ↗ · pubmed ↗
- 6Kinno T. Tsuta K. Shiraishi K. Mizukami T. Suzuki M. Yoshida A. Suzuki K. Asamura H. Furuta K. Kohno T. Clinicopathological features of nonsmall cell lung carcinomas with BRAF mutations Ann. Oncol.2014251381422429708510.1093/annonc/mdt 495 · doi ↗ · pubmed ↗
- 7Kris M.G. Johnson B.E. Kwiatkowski D.J. Iafrate A.J. Wistuba I.I. Aronson S.L. Engelman J.A. Shyr Y. Khuri F.R. Rudin C.M. Identification of driver mutations in tumor specimens from 1000 patients with lung adenocarcinoma: The NCI’s Lung Cancer Mutation Consortium (LCMC)J. Clin. Oncol.201129 CRA 7506
- 8Adib E. Nassar A.H. Abou Alaiwi S. Groha S. Akl E.W. Sholl L.M. Michael K.S. Awad M.M. Jänne P.A. Gusev A. Variation in targetable genomic alterations in non-small cell lung cancer by genetic ancestry, sex, smoking history, and histology Genome Med.2022143910.1186/s 13073-022-01041-x 35428358 PMC 9013075 · doi ↗ · pubmed ↗