Clear Aligner Therapy and Marginal Edge Design: Clinical and Laboratory Evidence on Periodontal and Biological Outcomes—A Scoping Review
Emilia (Prodea) Rusu, Ana-Petra Lazăr, Bianca Luminița Erhan, Eugen Bud, Mariana Păcurar, Luminița Lazăr

TL;DR
This review examines how clear aligner therapy affects periodontal health, focusing on the design of the aligner's edge and its impact on gums and inflammation.
Contribution
The study maps and synthesizes clinical and laboratory evidence on periodontal outcomes of clear aligners, highlighting the lack of research on marginal edge design.
Findings
Clinical and laboratory evidence on periodontal outcomes of clear aligner therapy is methodologically diverse.
Only three studies specifically examined aligner marginal edge design, with one comparing configurations and finding differences in gingival response.
Standardized protocols and targeted studies are needed to better understand the periodontal relevance of aligner trimline configurations.
Abstract
Background: Clear aligner (CA) therapy has been increasingly adopted as an alternative to fixed orthodontic appliances. However, evidence regarding its periodontal effects, including gingival inflammation, biofilm composition, and the potential role of aligner marginal edge design, remains insufficiently mapped. The objective of this scoping review was to map and synthesize available clinical and laboratory evidence on periodontal and biological outcomes associated with CA therapy, with particular attention to the potential influence of aligner marginal edge design. Methods: This scoping review followed PRISMA-ScR and the Population–Concept–Context (PCC) framework. PubMed, Scopus, and Web of Science were searched from 1 January 2015 to 24 October 2025. A total of 1587 records were identified; after deduplication, 770 unique records were screened by title and abstract, followed by…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
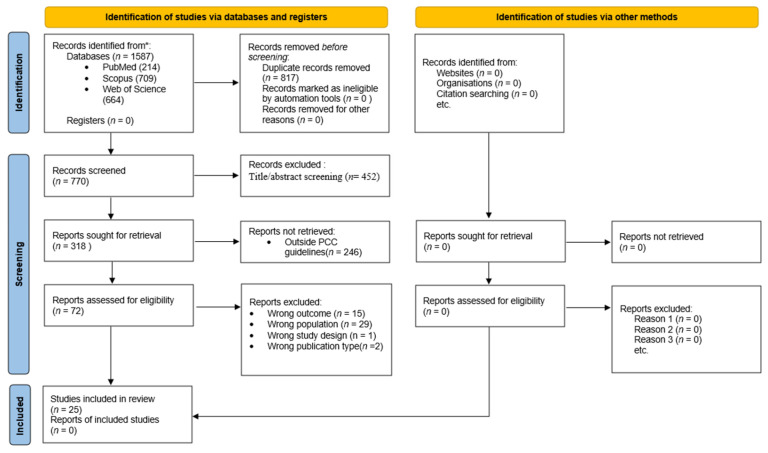 Figure 1
Figure 1- —project “FOCUS: Training and Guidance for UMFST Researchers in Health”, contract no. 100455/29.08.2025
- —European Union under the Health Programme of the Ministry of Investments and European Projects
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthodontics and Dentofacial Orthopedics · Oral microbiology and periodontitis research · Periodontal Regeneration and Treatments
1. Introduction
In the past decade, orthodontic treatment using clear aligners (CAs) has become an increasingly common alternative to conventional fixed appliances, with growing adoption reflecting increased patient demand for more esthetic and comfortable treatment options that facilitate oral hygiene maintenance [1,2].
Although the esthetic and functional advantages of aligners are well documented, their impact on periodontal health remains an area of active investigation [3]. Unlike fixed appliances, aligners are removable and may permit more effective plaque control [4]. However, their trimline configuration (scalloped, straight-cut, or hybrid) may influence local gingival response and biofilm dynamics [5]. Clinical findings remain mixed: some studies report improvements in periodontal parameters [6,7,8], while others document variations in inflammatory or microbiological markers [9,10,11]. Laboratory investigations have further examined bacterial adherence to aligner materials and surface modifications aimed at reducing microbial colonization [12,13].
The aim of this scoping review is to map and synthesize clinical and laboratory evidence on the periodontal and biological effects of CA therapy, with particular attention to aligner marginal edge design.
Specifically, this review addresses the following research question: What is the impact of CA therapy on periodontal health, and what evidence exists regarding the influence of aligner marginal edge design on periodontal outcomes?
2. Methodology
This synthesis focused on identifying thematic patterns, methodological approaches, and existing knowledge gaps, rather than evaluating comparative effectiveness, causality, or clinical superiority. Data were synthesized descriptively without formal comparison between interventions.
The present review was structured according to the Population–Concept–Context (PCC) framework recommended by the Joanna Briggs Institute for scoping reviews [14,15]. The PCC framework provides a structured approach to defining eligibility criteria in scoping reviews, where Population describes the important characteristics of participants, Concept encompasses the core elements under examination (which may include interventions, phenomena of interest, or outcomes), and Context specifies the setting and relevant circumstances.
The population of interest included adolescent and adult patients, aged 12 years or older, undergoing orthodontic treatment with CA. The central concept addressed aligner therapy and marginal edge design (scalloped, straight-cut, or hybrid) in relation to periodontal parameters, inflammatory biomarkers, and microbiological characteristics. The context considered both clinical and laboratory investigations published between 2020 and 2025 within the interdisciplinary fields of orthodontics and periodontology.
This review was conducted in accordance with the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) guidelines to enhance methodological transparency and consistency with current reporting standards for scoping reviews.
2.1. Study Type and Aim
The searches aimed to identify clinical and laboratory studies reporting periodontal parameters (plaque index (PI), gingival index (GI), bleeding on probing (BOP), probing pocket depth (PPD), and clinical attachment level (CAL)), inflammatory markers (IL-1β, TNF-α, MMP-8, and CRP), or microbiological characteristics (biofilm, bacterial load, and adhesion patterns associated with different margin designs).
Study selection was performed in collaboration with a research team through a well-structured process in successive stages: database searches, deduplication, title and abstract screening, full-text assessment, and final inclusion.
2.2. Search Strategy
The search was performed across the PubMed, Scopus, and Web of Science databases. The database search covered 1 January 2015 to 24 October 2025 to capture both earlier foundational and recent evidence; however, in line with predefined eligibility criteria, the final included studies were published between 2020 and 2025.
The search strategy combined terms for orthodontic treatment with CA and periodontal or inflammatory indicators and was limited to human clinical studies and laboratory studies using human participants or human-derived biological samples, published in English. Romanian-language records were also screened to minimize language bias; however, none met the final inclusion criteria.
The PubMed (MEDLINE) search combined MeSH terms with free-text keywords, and full texts were retrieved when available. Terms describing orthodontic treatment with aligners included the MeSH descriptor “Orthodontic Appliances, Removable” and keywords such as “clear aligner”, “orthodontic aligner”, and “Invisalign”. These were combined with terms related to periodontal health and gingival inflammation, including “gingival diseases”, “periodontal diseases”, “gingival inflammation”, “PI, GI, BOP, PPD, and CAL”, as well as microbiological terms such as “biofilm, bacterial adhesion, microbiome, bacterial load, cytokines, IL-1β, TNF-α, and MMP-8”.
To include articles investigating the morphological aspects of aligners, the search was expanded to terms referring to margin design—”scalloped, straight cut, trimline, marginal finish, edge design, and gingival margin”—to identify studies addressing the potential influence of margin design on gingival tissues.
Detailed database-specific search strategies and screening steps are provided in the Supplementary Materials [16].
2.3. Study Integration and Selection
The search performed in the PubMed (MEDLINE), Scopus, and Web of Science databases generated a total of 1587 records. After deduplication using the Zotero reference manager, 770 unique records remained for screening. The selection of articles was performed in two successive stages.
In the first stage, records were screened by title and abstract for relevance to periodontal outcomes associated with CA therapy. In the second stage, full-text assessment was conducted for potentially eligible articles. Secondary research articles (systematic reviews and meta-analyses) were excluded from the final inclusion set; however, their reference lists were screened when relevant.
As this is a scoping review, the purpose was to map the breadth of available evidence rather than to formally appraise methodological quality or estimate effect sizes. Therefore, no risk-of-bias assessment, critical appraisal, or meta-analysis was performed. A review protocol was not prospectively registered, consistent with Joanna Briggs Institute guidance for scoping reviews focused on evidence mapping rather than comparative effectiveness assessment.
Full-text assessment was based on the following inclusion criteria: clinical studies (randomized, cohort, case–control, or cross-sectional) or laboratory studies using human participants or human-derived biological samples; adolescent or adult participants (≥12 years old); orthodontic treatment with CA; and reporting of one or more periodontal or gingival clinical indicators (PI, GI, BOP, PPD, and CAL) or biological parameters (inflammatory biomarkers, microbiological characteristics). When reported, information regarding aligner marginal edge design (scalloped, straight-cut, or hybrid) was extracted and synthesized.
Study selection was initially conducted by one reviewer following the predefined protocol. To minimize selection bias, the entire screening process, including title/abstract screening and full-text eligibility assessment, was subsequently re-screened by additional members of the research team, strictly adhering to the same methodological criteria. Any discrepancies were discussed and resolved through consensus.
The exclusion criteria targeted articles lacking periodontal data, information on the research methodology, or results; studies focused exclusively on comfort, esthetics, pain, speech, or tooth movement mechanics; editorials, letters, or conference abstracts; and articles from unrelated medical fields (orthopedics, ophthalmology, molecular biology, optics, etc.). Single case reports were generally excluded; however, those providing clinically or biologically relevant information on periodontal outcomes were retained for descriptive mapping purposes.
2.4. Data Charting and Synthesis
Data from included studies were systematically extracted using a standardized charting form developed by the research team. For each study, the following information was recorded: first author and publication year; study design and setting; population characteristics (sample size, age range); intervention details (aligner type, marginal edge design when specified, treatment duration); periodontal outcomes measured (clinical indices: PI, GI, BOP, PPD, CAL; and biological parameters: inflammatory markers, microbiological characteristics); key findings; and study conclusions.
The extracted data were synthesized descriptively and organized thematically according to outcome type (clinical periodontal indices, inflammatory biomarkers, microbiological analyses) and study design (clinical trials, observational studies, laboratory investigations). This approach allowed for comprehensive mapping of the evidence landscape while acknowledging the methodological heterogeneity that precluded quantitative synthesis.
3. Results
A total of 25 eligible articles were identified and analyzed, with the final search conducted on 24 October 2025. Studies were grouped by outcome type: clinical periodontal indices, inflammatory biomarkers, and microbiological analyses. The study selection process is shown in Figure 1.
3.1. Study Characteristics and Thematic Grouping
The eligible articles were grouped into three thematic domains: gingival/periodontal inflammation, biofilm and inflammatory markers, and aligner margin design. The distribution of these studies and their corresponding fields of analysis are presented in Table 1. This thematic grouping organized studies across overlapping research areas and highlighted differences in study focus regarding periodontal outcomes. Only a small subset of studies addressed aligner margin design, primarily from a clinical design perspective, with periodontal outcomes reported indirectly or qualitatively.
3.2. Study Designs and Methodological Diversity
Beyond thematic classification, the methodological characteristics of the included articles were examined to highlight diversity in study design and approaches used in investigating the association between aligner use and periodontal health (Table 1).
Based on study design and methodological approach, the eligible articles were grouped into four main categories:
- (i)Prospective and observational clinical studies;
- (ii)Experimental and laboratory studies (in vitro and ex vivo);
- (iii)Case reports with high clinical relevance;
- (iv)Interdisciplinary studies combining orthodontics, periodontology, and molecular biology.
3.2.1. Prospective and Observational Clinical Studies
Fourteen articles employed a prospective or observational design, including comparisons between CA therapy and fixed orthodontic appliances. These studies monitored parameters such as the evolution of periodontal biomarkers, biofilm dynamics, microbiological and immunological changes, and clinical outcomes at different stages of orthodontic treatment. The main characteristics of these studies are summarized in Table 2.
3.2.2. Experimental and Laboratory Studies (In Vitro and Ex Vivo)
Five experimental studies were identified, focusing on the analysis of cytotoxicity, surface alterations of aligner materials, and the evaluation of molecular markers using laboratory methods (enzyme-linked immunosorbent assay (ELISA), Polymerase Chain Reaction (PCR), and microbial cultures performed on aligner materials or gingival crevicular fluid (GCF)) (Table 3).
These studies reported data on bacterial adhesion, surface characteristics of aligner materials, and inflammatory cytokine expression (IL-1β, TNF-α, MMP-8) under different experimental conditions. Variations in inflammatory marker levels were reported across observation periods.
3.2.3. Case Reports with Clinical and Interdisciplinary Characteristics
Three articles presented complex clinical cases, including severe gingival recessions and interdisciplinary treatment approaches, with periodontal parameters documented in these clinical contexts (Table 4).
3.2.4. Studies with an Interdisciplinary Orthodontics–Periodontology–Molecular Biology Approach
Ten studies noted collaborations between orthodontists and periodontists, as well as specialists in biochemistry or microbiology, integrating clinical evaluations with the analysis of inflammatory biomarkers, microbial sequencing, cytokine determination in GCF, and, in some cases, genomic associations (Table 5).
Across the included studies, periodontal assessment was conducted using a wide range of clinical indices and scoring methodologies. Plaque accumulation was evaluated using different PI, including the Silness–Löe index, the Turesky modification of the Quigley–Hein index, and the O’Leary PI, while GI was primarily assessed using the Löe–Silness GI or modified GI scales. BOP was reported using either percentage-based measures or categorical scoring systems, and PPD and CAL were assessed in selected investigations. Periodontal evaluations were performed at variable timepoints, including baseline, 1, 3, 6, and 12 months. This variability in index selection, scoring systems, and assessment timing limited direct cross-study comparability of reported periodontal outcomes.
One investigation specifically compared aligner margin configurations, with Favero et al. [5] reporting significant differences in periodontal indices between vestibular and juxtagingival rim designs over six months.
CAL was assessed in eight studies focused on adult patients or those with pre-existing periodontal considerations. Seven investigations reported stable CAL throughout treatment, with Leibovich et al. [20] describing favorable outcomes in a case series employing CA for root repositioning prior to periodontal surgery in patients with lower incisor gingival recession. The observed variability in periodontal assessment protocols, scoring systems, and examination timing complicates direct cross-study comparisons.
3.3. Influence of Aligner Margin Design
Favero et al. [5] compared vestibular rim (extending approximately 3 mm beyond the gingival margin) versus juxtagingival rim (following the gingival outline) designs in adolescent patients (n = 43, aged 14–18 years). Over a six-month observation period, juxtagingival margins were associated with significantly worse periodontal indices (PI p = 0.011, GI p = 0.03, gingival bleeding index p = 0.014), while vestibular rim margins showed no significant changes in any measured parameter.
Rouzi et al. [18] examined oral microbiota and health parameters in aligner patients using 16S rRNA gene sequencing, documenting changes in microbial community composition over three months. The study noted the scalloped design of Invisalign margins in discussion but did not systematically investigate the influence of margin configuration on periodontal outcomes.
Kredig et al. [11] investigated periodontal inflammatory biomarkers in adolescents undergoing aligner therapy with scalloped juxtagingival margins, discussing the potential clinical relevance of trimline configuration based on comparative literature.
Across these studies, the available evidence on aligner margin configuration remains limited and methodologically diverse, with variations in study design, sample populations, assessment protocols, and categorization approaches. These findings should be interpreted descriptively as a mapping of reported associations, without inferring comparative effectiveness or establishing causal relationships.
3.4. Temporal and Demographic Distribution
The included articles were published between 2020 and 2025, with publication activity increasing from 2020 onwards. The time frame of the reported investigations was generally close to the publication date (with differences of approximately 1–2 years).
Population characteristics and sample variability were also examined, the number of participants varied among studies, reflecting the diversity in research designs and objectives. In clinical studies, sample size generally ranged from 12 to 90 patients, with most investigations conducted on small cohorts subjected to close longitudinal monitoring. One study included larger samples, reporting up to 146 recessions or multiple cases per patient, depending on the periodontal parameters assessed [7].
From a demographic perspective, the study populations mainly consisted of young adults (approximately 20–35 years) and adolescents (12–18 years). Some studies focused exclusively on adult patients to describe reported periodontal parameters during aligner treatment [30], while others concentrated on adolescent populations to examine periodontal indices and margin design effects [5] or inflammatory biomarkers [11].
4. Discussion
In this review, biological outcomes refer to inflammatory, microbiological, molecular, and cellular responses associated with CA, rather than definitive clinical endpoints. These outcomes are discussed in relation to the predefined aim of this scoping review, namely to map how periodontal and biological responses to CA therapy and marginal edge design have been reported across clinical and laboratory studies.
Several clinical studies reported PI, GI, and BOP during CA therapy [18]. In a longitudinal comparison between aligner and fixed appliance treatments, Lombardo et al. [34] reported differences in subgingival microbiota composition across follow-up intervals, with microbial assessments performed at 3 and 6 months in the fixed-appliance group and corresponding periodontal evaluations in the aligner group.
Microbiological studies identified both commensal and pathogenic species on aligner surfaces and reported compositional changes during therapy; these findings are constrained by methodological heterogeneity and the frequent absence of parallel clinical or biomarker assessments [28,34].
Across the included clinical studies, periodontal parameters during aligner therapy were described in relation to fixed appliances using variable study designs, follow-up durations, and oral hygiene protocols, which limited direct cross-study comparability. Some investigations reported variations in specific parameters, such as PI or GI, particularly in interdisciplinary clinical settings and among patients with distinct periodontal phenotypes [17].
The findings of this scoping review should be considered within the broader evidence base comparing periodontal outcomes between CA and fixed appliances. Previous meta-analyses have reported statistically more favorable periodontal indices in patients treated with CA. Jiang et al. [35] identified significantly lower PI and GI in aligner patients, although trial sequential analysis indicated insufficient sample size to support conclusions regarding PPD. Similarly, Llera-Romero et al. [36], in the first meta-regression addressing this topic, reported that periodontal advantages associated with CA increased with treatment duration and described a markedly reduced risk of white spot lesions.
More recent reviews have tempered these findings. Di Spirito et al. [37] concluded that reported differences between aligners and fixed appliances, although statistically significant, were clinically negligible, while Crego-Ruiz and Jorba-García [38] found insufficient evidence to support definitive superiority of CA therapy. Importantly, none of these syntheses evaluated the potential influence of aligner marginal edge design on periodontal outcomes, representing a gap that the present scoping review sought to address. Consistent observations were reported by Dipalma et al. [39], who described improved oral hygiene maintenance and reduced inflammatory parameters in aligner-treated patients, while also emphasizing the heterogeneity and risk of bias of the available evidence and the importance of patient-specific clinical decision-making.
Regarding inflammatory biomarkers, cytokine levels in GCF showed variable temporal patterns across studies. Proinflammatory cytokines (IL-1β, TNF-α, and MMP-8) were assessed at different timepoints, though inconsistent sampling schedules complicate interpretation [11,29]. This cautious interpretation is further supported by the study of Nemec et al. [40], who reported no significant longitudinal changes in salivary inflammatory markers or overall microbial community composition during orthodontic treatment with either aligners or fixed appliances in patients maintaining adequate oral hygiene.
Periodontal assessment exhibited considerable divergence in approach: diverse indices were utilized (Silness–Löe, Turesky modification, O’Leary) alongside disparate follow-up intervals (1–12 months). Examiner calibration and standardized timing relative to aligner wear were infrequently documented, thereby constraining evidence synthesis.
In vitro studies addressed thermoplastic aligner materials (polyurethanes, PETG, and medical-grade polyesters) without cytotoxic responses in human gingival fibroblasts and oral epithelial cells [29]. However, saliva from patients undergoing orthodontic treatment (both aligners and brackets) increased expression of proinflammatory markers (IL-6, IL-8, MCP-1) in gingival fibroblasts, with no significant difference between treatment modalities [29]. These results were presented within laboratory-based experimental contexts and were not directly linked to clinical outcome measures. One study discussed the potential release of residual compounds after repeated thermal cycles and noted periodic replacement within their protocols [28].
For aligner trimline, a small number of comparative studies outlined plaque accumulation and local gingival response in relation to supragingival and juxtagingival configurations. These findings are based on limited, methodologically diverse evidence and should be interpreted as hypothesis-generating rather than practice-directing [5].
Both clinical and laboratory investigations were frequently characterized by small sample sizes, short observation periods, and non-uniform outcome measures, alongside experimental conditions that do not fully replicate the clinical oral environment, thereby affecting external validity.
The limited evidence specifically addressing aligner marginal edge design underscores the need for targeted investigations and supports the rationale for this scoping review. Notably, included studies predominantly enrolled adolescent and adult patients (aged 12–35 years) with healthy or well-controlled periodontal status; evidence for patients with moderate-to-severe periodontal disease or recent surgical interventions remains scarce. Future research should prioritize longer follow-up periods, standardized periodontal and biomarker assessments, integrated clinical–microbiological designs, and inclusion of periodontally compromised populations to better characterize the clinical relevance of marginal edge design.
5. Conclusions
This scoping review mapped clinical and laboratory evidence on periodontal and biological outcomes associated with CA therapy. Twenty-five studies published between 2020 and 2025 were included, employing diverse methodological approaches. Most investigations reported stable or favorable periodontal parameters during aligner therapy in cohorts with adequate oral hygiene, with substantial heterogeneity in assessment protocols and outcome definitions limiting cross-study comparisons.
Evidence on aligner marginal edge design remains scarce, with only three studies addressing trimline configurations and one directly comparing margin types. Current findings preclude definitive conclusions regarding optimal margin design for periodontal health.
Future research should prioritize: standardized periodontal assessment protocols enabling meaningful synthesis; adequately powered comparative studies on marginal edge designs; longitudinal investigations extending beyond active treatment; and inclusion of patients with compromised periodontal status. This review provides a foundation for targeted investigations and supports the development of standardized research protocols in this field.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tamer I. Oztas E. Marsan G. Orthodontic treatment with clear aligners and the scientific reality behind their marketing: A literature review Turk. J. Orthod.20193224124610.5152/turkjorthod.2019.1808332110470 PMC 7018497 · doi ↗ · pubmed ↗
- 2Al Mogbel A. Clear aligner therapy: Up to date review article J. Orthod. Sci.2023123710.4103/jos.jos_30_2337881665 PMC 10597356 · doi ↗ · pubmed ↗
- 3Rouzi M. Zhang X. Jiang Q. Long H. Lai W. Li X. Impact of clear aligners on oral health and oral microbiome during orthodontic treatment Int. Dent. J.20237360361110.1016/j.identj.2023.03.01237105789 PMC 10509397 · doi ↗ · pubmed ↗
- 4Ahah Aloufan A. Clear aligners vs. fixed appliances in the management of mild to moderate malocclusion: A review of treatment efficacy, stability, and patient-centered outcomes Dent. Res. Oral. Health 202588084
- 5Favero R. Libralato L. Balestro F. Volpato A. Favero L. Edge level of aligners and periodontal health: A clinical perspective study in young patients Dent. Press J. Orthod.202328 e 232112410.1590/2177-6709.28.1.e 2321124.oar PMC 1010858237075415 · doi ↗ · pubmed ↗
- 6Alasiri M.M. Almalki A. Alotaibi S. Alshehri A. Alkhuraiji A.A. Thomas J.T. Association between gingival phenotype and periodontal disease severity: A comparative longitudinal study among patients undergoing fixed orthodontic therapy and Invisalign treatment Healthcare 20241265610.3390/healthcare 1206065638540619 PMC 10970162 · doi ↗ · pubmed ↗
- 7Bucur S.M. Bud E. DecusarăM. Olteanu C.D. Retrospective study on orthodontic gingival recession correction using clear aligners Medicina 202460202410.3390/medicina 6012202439768904 PMC 11728395 · doi ↗ · pubmed ↗
- 8Almagrami I. Almaqrami M. Zhu L. Qiao Y. Class III correction and enhanced periodontal health with aligner treatment in a 53-year-old patient Angle Orthod.20259545246310.2319/020524-91.1PMC 1241897539195195 · doi ↗ · pubmed ↗