Hybrid Digital Workflow for Accurate Distal Extension Reproduction in Free-End Removable Dental Prosthesis: A Technical Report
Thais Marques Simek Vega Gonçalves, Zuila Maria Lobato Wanghon, Liliane da Rocha Bonatto Drummond, Laura Costa Beber Copetti, Renata Blummer, Gabriella Aparecida Cruz dos Reis, Patrícia Pauletto, Analucia Gebler Phillippi

TL;DR
This paper introduces a new digital workflow for making dental prostheses that improves accuracy and reduces the need for traditional techniques.
Contribution
The novel hybrid workflow combines plaster-cast scanning with intraoral scanning to enhance accuracy in distal extension dental prostheses.
Findings
The hybrid workflow produces more accurate models of the distal extension region compared to direct intraoral scanning.
Digitally capturing mobile mucosa morphology eliminates the need for the traditional altered-cast technique.
The method reduces clinical time, technical sensitivity, and material costs.
Abstract
Background/Objectives: This technical report introduces an innovative hybrid digital workflow that integrates diagnostic plaster-cast scanning with intraoral scanning to produce an accurate 3D-printed model for fabricating distal-extension removable dental prostheses (RDPs). Methods: The technique aims to overcome the challenges of reproducing the mobile mucosa in free-end saddles, a critical factor for denture base accuracy and stability. The workflow began with conventional clinical procedures, including clinical examination, impression-making, and cast surveying. After performing the required mouth preparations according to the prosthetic design, the diagnostic cast was digitized and selectively modified to allow intraoral rescanning. The prepared teeth were then scanned intraorally and merged with the digitalized cast, producing a refined virtual model for CAD-based metal framework…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 3
Figure 3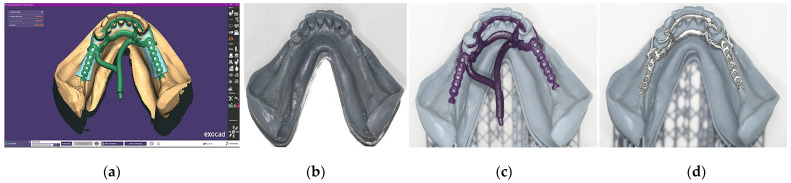 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDental materials and restorations · Dental Implant Techniques and Outcomes · Reconstructive Facial Surgery Techniques
1. Introduction
Removable dental prostheses (RDPs) remain a widely used treatment modality for partially edentulous patients; however, the conventional fabrication of metallic frameworks is often complex, time-consuming, costly, and susceptible to human error [1,2,3]. Recent advances in computer-aided design and computer-aided manufacturing (CAD-CAM) have transformed RDP fabrication, allowing for digital cast generation, virtual surveying, undercut elimination, and the design and production of 3D-printed or castable frameworks [4]. Recent studies [4,5,6] have shown that digitally fabricated RDPs exhibit comparable, and often superior, framework adaptation compared with conventional methods—particularly in framework seating and posterior strap fit. Additionally, digital design can be completed in approximately 15 min, reducing production time by 60 to 70% [7].
Despite these benefits, challenges remain in specific clinical scenarios, such as free-end RDPs. The anatomical complexity and mucosa flexibility of distal extension areas present challenges for direct intraoral scanning, frequently resulting in incomplete data acquisition and insufficient reproduction of these regions in the 3D-printed cast (Figure 1) [7,8]. Because an optimal resin base extension is critical for achieving maximum residual ridge support, inadequate coverage can lead to uneven occlusal load distribution, potential overloading of abutment teeth, and accelerated bone resorption of the alveolar ridge [4,6,8,9]. In such cases, the altered-cast technique has been frequently used to improve denture base adaptation by creating a functional impression of the edentulous region during framework try-in [10,11]. However, this technique is time-consuming and technique-sensitive as it requires additional clinical and laboratory steps, carries a high risk of distortion during cast sectioning and reassembly, and offers limited reproducibility [10,11]. These limitations often increase overall treatment complexity and may compromise the consistency of the final prosthesis [10,11].
In this context, continuing refinement of digital impression techniques in free-end RDPs is crucial to improve functional replication of soft-tissue dynamics and clinical performance of such prostheses, simplifying the process and improving laboratory and clinical workflows [12,13]. Thus, this technical report presents an innovative digital workflow cast impression that integrates the diagnostic plaster-cast scan with the intraoral scan to produce a final 3D-printed cast with accurate reproduction of the distal extensions in free-end removable RDPs.
2. Materials and Methods
Evaluate the clinical appearance of the mandible arch. The mucosa was healthy, and bilateral posterior edentulism was noted, indicating the need for a distal extension RDP (Figure 2a).Make a conventional impression using a metallic stock tray with the border modeling customized with utility wax and a high-viscosity alginate (Cavex Cream; Cavex, Haarlem, The Netherlands) (Figure 2b). The impression was then poured in type IV dental stone (Zero Stone; Dentona, Dortmund, Germany) to obtain a diagnostic cast (Figure 2c). This cast was analyzed using a conventional surveyor to evaluate and plan the necessary mouth preparations for support, stability, and retention of the RDP (Figure 2d).
3.Perform all necessary mouth preparations according to the treatment plan. In this case, incisal reconstructions with direct restorations were completed on all incisors and canines, followed by conventional free-hand lingual rest preparations. Additional composite resin was applied to the buccal surfaces of teeth 34 and 43 to improve clasp retention, and a conventional mesial occlusal rest was prepared on the mesial area of the occlusal face of tooth 34 (Figure 3a).4.Digitally scan the diagnostic cast using a manual scanner (TRIOS 3; 3Shape A/S, Copenhagen, Denmark) to capture the entire basal area, including the retromolar pads and retromylohyoid fossae (Figure 3b). The scan should be performed in the pre-preparation mode using the CAD software (3Shape Dental System v. 2023.1; 3Shape, Copenhagen, Denmark) to allow subsequent image merging (Figure 3c). For a better performance of the scanner, in the tools button, choose the scan model. Save the file in standard tessellation language (STL) format.5.In the digitized STL file, apply block-outs to all areas unrelated to the prepared teeth (Figure 3d). Then, remove the regions corresponding to the prepared teeth to enable subsequent intraoral rescanning of these areas (Figure 3e).6.Switch to the main scanning mode and select “Intraoral Scanning” from the tool’s menu. Perform a direct scan of the prepared teeth using the TRIOS3 (3Shape, 3Shape A/S, Copenhagen, Denmark). The software will automatically merge the intraoral scan with the previously digitized cast to generate the final digital model (Figure 3f). Save the model in STL format and send it to the dental technician for metal framework design and fabrication.
Digital scanning procedures. (a) Occlusal view of the prepared teeth, including incisal reconstructions, lingual and occlusal rests, and resin increments on the buccal surface of teeth 34 and 43 to enhance clasp retention. (b) Digital scanning of the diagnostic plaster cast. (c) Digital image of the diagnostic plaster cast. (d) Prepared digital image of the diagnostic plaster cast with block-outs of all areas not related to the prepared teeth. (e) Digital image of the diagnostic cast with the regions corresponding to the prepared teeth removed. (f) Digital image of the final cast after merging the previous image with the intraoral scanning of the prepared teeth.
7.The framework was digitally designed by the dental technician using CAD software (Exocad Dental DB, v. 3.1, Exocad, Darmstadt, Germany) (Figure 4a). The connectors, rests, and clasps were modeled according to standard design principles. A 3D model was then printed (Model Resin Standard, Monile Lab, Curitiba, Brazil) to verify the framework adaptation (Figure 4b).8.A resin framework pattern (VisiJet M3 Dentcast, 3D Systems, Rock Hill, SC, USA) was printed by the dental technician using a 3D printer machine (ProJet MJP 3600 Dental, 3D Systems, Rock Hill, SC, USA), and its adaptation was verified on the printed model (Figure 4c). Once confirmed, the resin pattern was invested and cast in a cobalt–chromium (Co–Cr) alloy following a conventional workflow to produce the definitive metallic framework, which was subsequently rechecked for adaptation on the 3D-printed cast (Figure 4d).
Clinical and laboratory workflow for the fabrication of the mandibular removable dental prosthesis (RDP) and maxillary complete denture. (a) Digital design of the metal framework using dental CAD software (Exocad Dental DB, v. 3.1, Exocad, Darmstadt, Germany). (b) 3D-printed model (Model Resin Standard, Monile Lab, Curitiba, Brazil). (c) 3D-printed resin framework pattern (VisiJet M3 Dentcast, 3D Systems, Rock Hill, SC, USA) to check for fit on the printed 3D model. (d) Metallic framework (Co–Cr) adapted to the printed cast.
9.Following standard RDP fabrication protocols, make the intraoral try-in of the framework to confirm proper adaptation (Figure 5a). Fabricate bilateral acrylic bases using auto-polymerized polymethyl methacrylate to preserve accurate denture base extension (Figure 5b). Mount the maxillary definitive cast on a semi-adjustable articulator using a facebow. Define the interocclusal registration at centric relation to establish the occlusal vertical dimension in the mandibular wax rim and mount the mandible 3D-printed cast on the semi-adjustable articulator (Figure 5c). After the artificial teeth are mounted (Figure 5d), make the intraoral try-in to evaluate functional and esthetic aspects and obtain patient approval (Figure 5e).10.Install the polymerized and finished prosthesis and perform the necessary occlusal and functional adjustments (Figure 6).
3. Results
The proposed technique resulted in an RDP with an accurately reproduced distal extension of the acrylic base (Figure 6a). Compared to the 3D-printed model generated from direct intraoral scanning, the 3D-printed model produced through the proposed digital workflow showed markedly superior reproduction of the distal extension area (Figure 7). Additionally, in case of thin and/or flaccid mucosa, this correct extension of the resin base allows for pressure equalization throughout the direct impression with light silicon during prosthesis try-in and posterior resin polymerization. These outcomes highlight the technique’s ability to enhance anatomical fidelity in the distal extension region, improving denture base accuracy and overall prosthesis quality.
4. Discussion
The described technique introduces an innovative digital workflow for fabricating free-end RDPs, integrating diagnostic cast data with intraoral scans to produce a 3D-printed cast that accurately replicates the distal extension areas. Notably, this method does not modify the conventional sequence, as the diagnostic cast remains part of the routine treatment planning and surveying [1,13].
Accurate reproduction of the distal extension area is critical in Kennedy Class I RDPs to ensure proper support, load distribution, and tissue adaptation, all of which directly affect prosthesis retention, stability, and patient comfort during function [3,9]. Insufficient coverage of the distal basal seat may lead to uneven load distribution, mucosal trauma, food impaction, and prosthesis instability, ultimately overloading abutment teeth and contributing to periodontal deterioration and progressive loss of support [3,8]. However, direct intraoral scanning of distal extension regions remains challenging due to anatomical and physiological constraints, especially in the mandible [7,12]. Tongue interference, mobile soft tissues, and complex mucosal contours often compromise scan accuracy, reducing cast precision and prosthesis adaptation [12,13]. Scan quality is also operator-dependent and may be affected by patient discomfort and data stitching errors [14,15,16].
To address these limitations, clinicians commonly apply the altered-cast technique, which records the edentulous ridge under functional conditions with the framework in place and incorporates this record by sectioning and reassembling the master cast [10,11,12]. Although effective, this method is technique-sensitive, time-consuming, and cost-intensive, requiring additional clinical appointments, materials, and laboratory procedures [11,12]. Cast sectioning and reassembling also introduce the inherent risks of distortion and misalignment, and outcomes depend heavily on clinical and laboratory expertise, reducing reproducibility in routine practice [10,11,12].
The proposed workflow mitigates the limitations of direct intraoral scanning while reducing reliance on altered-cast impressions. By combining intraoral scans of prepared teeth with digitalized diagnostic casts, it enables reliable distal extension reproduction without applying cast sectioning or functional impression procedures [5,15]. The workflow functions as a digital analog of the altered-cast concept instead of a direct replacement, since distal extension support is inferred from the diagnostic cast rather than functionally recorded under controlled loading. Nevertheless, compared with altered-cast-based digital adaptations [14,15,16], the hybrid approach offers greater procedural simplicity and lower technique sensitivity, while maintaining the conventional clinical sequence. In situations involving thin mucosa or pronounced retentive areas, pressure equalization can be achieved using a light-body silicone impression of the edentulous area and consequent inclusion and resin polymerization, without sectioning the master cast or sealing the borders [4,6]. This further reduces laboratory steps and minimizes the risks of distortion and misalignment when compared to the conventional altered-cast method [11].
Nevertheless, the proposed workflow introduces additional digital steps, including scanning, segmentation, and file merging. Therefore, its efficiency advantages should be interpreted primarily as reduced procedural complexity rather than guaranteed reductions in chairside or laboratory time and should be confirmed in future time-controlled studies [17]. Although demonstrated with laboratory-grade scanners and high-resolution printers, the protocol is device-independent and can be implemented with validated desktop scanners and SLA/DLP printing systems of adequate resolution, supporting broader adoption [13]. Economically, the approach shifts costs from consumable materials and labor-intensive laboratory steps toward digital infrastructure [5]. While initial investment in hardware and software may be substantial, marginal per-case costs may decrease in practices with established digital workflows and repeated clinical use [17].
Additionally, this technical workflow provides a clinical illustration rather than quantitative outcome data. Accuracy remains device- and operator-dependent, requiring proper calibration and technical expertise [14,15,16,17]. Moreover, potential alignment errors may introduce subtle inaccuracies, and the need for multi-scan acquisition and large file handling increases data processing and management demands [13]. Thus, well-designed prospective clinical trials are needed to evaluate prosthesis fit, tissue adaptation, functional performance, and patient-centered outcomes before routine clinical implementation can be fully supported.
5. Conclusions
The proposed technique integrates intraoral and diagnostic cast scans to digitally reproduce distal extension areas with high accuracy. By preserving the conventional clinical workflow while markedly enhancing distal tissue representation, adaptation, and stability, it offers a practical and accessible advancement in the digital fabrication of RDPs. This approach not only streamlines the process but also elevates the precision and clinical performance of free-end RDPs, offering a practical and accessible solution for digitally fabricated RDPs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Campbell S.D. Cooper L. Craddock H. Hyde T.P. Nattress B. Pavitt S.H. Seymour D.W. Removable partial dentures: The clinical need for innovation J. Prosthet. Dent.201711827328010.1016/j.prosdent.2017.01.00828343666 · doi ↗ · pubmed ↗
- 2Drummond L.B. Bezerra A.P. Feldmann A. Goncalves T.M.S.V. Long-term assessment of the periodontal health of removable partial denture wearers: A systematic review and meta-analysis J. Prosthet. Dent.20251341664168510.1016/j.prosdent.2024.06.02039043477 · doi ↗ · pubmed ↗
- 3Zlataric D.K. Celebic A. Valentic-Peruzovic M. The effect of removable partial dentures on periodontal health of abutment and non-abutment teeth J. Periodontol.20027313714410.1902/jop.2002.73.2.13711895277 · doi ↗ · pubmed ↗
- 4Rokhshad R. Tehrani A.M. Nahidi R. Zarbakhsh A. Fit of removable partial denture frameworks fabricated from 3D printed patterns versus the conventional method: An in vitro comparison J. Prosthet. Dent.20241311144114910.1016/j.prosdent.2022.03.02735597606 · doi ↗ · pubmed ↗
- 5Gan N. Yao M. Ruan Y. Wang C. Xiong Y. Jiao T. Adaptation of maxillary removable partial denture frameworks fabricated with a direct digital workflow: A randomized crossover clinical trial J. Dent.202515410558810.1016/j.jdent.2025.10558839864610 · doi ↗ · pubmed ↗
- 6Heiba I.M. Mohamed Lotfy S. Rizk F.N. Sabet M.E. Effect of different digital technology on the adaptation and retention of Co-Cr partial denture frameworks J. Prosthod.20243380180710.1111/jopr.1376537688449 · doi ↗ · pubmed ↗
- 7Hu F. Pei Z. Wen Y. Using Intraoral Scanning Technology for Three-Dimensional Printing of Kennedy Class I Removable Partial Denture Metal Framework: A Clinical Report J. Prosthod.201928 e 473e 47610.1111/jopr.1271229143451 · doi ↗ · pubmed ↗
- 8Takebe J. A case series on the basic concept and design of removable partial dentures: Support and bracing considerations BMC Oral Health 20252515710.1186/s 12903-025-05553-x 39881265 PMC 11780901 · doi ↗ · pubmed ↗