The Ductus Dilemma: To Close or Not to Close in the Fight Against Endocarditis/Endarteritis
Tessa A. E. Soede, Gabriëlle G. van Iperen, Johannes M. P. J. Breur

TL;DR
Closing small, non-significant arterial ducts in patients does not prevent endocarditis and may cause more harm than benefit.
Contribution
Demonstrates that audible and silent PDAs similarly contribute to infective endocarditis without justifying routine closure.
Findings
Infective endocarditis is rare in patients with both audible and silent persistent arterial ducts.
Percutaneous ductal closure has a 23.3% adverse event rate, with 10.1% clinically significant complications.
IEE occurs in both audible and silent PDAs through similar hemodynamic mechanisms.
Abstract
What are the main findings? Infective endocarditis is rare in patients with an audible and non-audible persistent arterial duct.The benefits of ductal closure do not outweigh the drawbacks in cases involving hemodynamically insignificant ducts. Infective endocarditis is rare in patients with an audible and non-audible persistent arterial duct. The benefits of ductal closure do not outweigh the drawbacks in cases involving hemodynamically insignificant ducts. What is the implication of the main finding? Hemodynamically insignificant ducts should not be closed. Hemodynamically insignificant ducts should not be closed. Background: Patent ductus arteriosus (PDA) is a common congenital heart defect. While closure of hemodynamically significant PDAs is well established, closure of small, hemodynamically insignificant PDAs for prevention of infective endocarditis or endarteritis (IEE)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
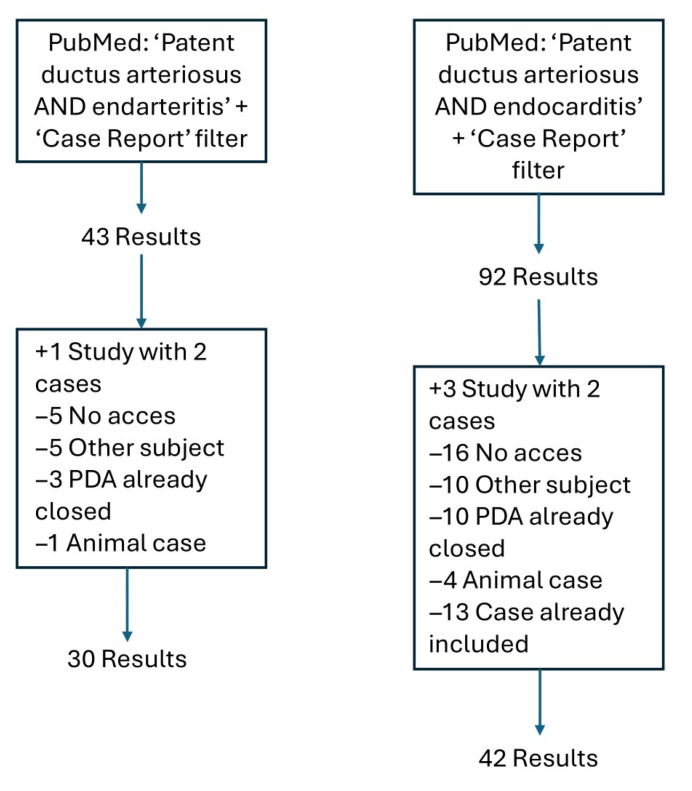 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Conditions and Treatments · Infective Endocarditis Diagnosis and Management · Congenital Heart Disease Studies
1. Introduction
The ductus arteriosus is a normal fetal blood vessel that connects the descending aorta to the main pulmonary artery. After birth, this shunt becomes redundant, and in most healthy newborns, the ductus closes spontaneously within 12 to 24 h of life [1]. When the ductus fails to close completely, it results in a condition known as patent ductus arteriosus (PDA), a common congenital heart defect. In the general population, the incidence of PDA is estimated at roughly 1 in 2000 live births [2]. The clinical relevance of a PDA depends on its size and shunt magnitude: large PDAs may cause left-sided volume overload and heart failure, whereas small PDAs are often asymptomatic [3]. Very small PDAs are often referred to as “(clinically) silent” as they produce little to no murmur, cause no symptoms, and present with no other clinical signs. Such silent PDAs may go unnoticed until they are incidentally detected through screening or echocardiography performed for unrelated reasons [4].
According to the American Heart Association (AHA) guidelines, transcatheter closure is strongly recommended for moderate-sized or large PDAs with a left-to-right shunt causing heart failure, pulmonary over-circulation, or left heart enlargement [5]. This recommendation is supported by Level A evidence, based on data derived from multiple randomized clinical trials or meta-analyses (class I recommendation). For small PDAs with a left-to-right shunt and normal heart size, closure is considered reasonable when the ductus is audible on auscultation (class IIa recommendation). According to the AHA guidelines, transcatheter PDA occlusion may be considered for PDAs with a small left-to-right shunt, normal heart size, and an inaudible murmur (class IIb recommendation). The latter two recommendations concern hemodynamically insignificant PDAs and are based on Level C evidence, reflecting expert consensus, case studies, or standard of care. As a result, many hemodynamically insignificant but audible PDAs discovered incidentally during screening or echocardiographic evaluation are closed during percutaneous intervention, whereas silent PDAs are often not closed. According to the AHA guidelines, in addition to closure for hemodynamic reasons, an indication for PDA closure is the need to prevent PDA-associated infective endocarditis or endarteritis (PDA-IEE).
IEE is an infection of the endothelium and develops through a sequence of endothelial injury, bacteremia, bacterial adhesion, and in situ persistence. Healthy endothelium is normally resistant to bacterial colonization; however, abnormal flow patterns associated with a PDA generate non-physiological shear stress [6]. Common causative organisms, such as Staphylococcus aureus, possess specific adhesins that allow them to adhere to the endothelium [7]. Studies have shown that shear stress outside the normal physiological range induces upregulation of lectin-type oxidized low-density lipoprotein receptor 1 (LOX-1) expression [8]. This upregulation facilitates binding of bacterial wall teichoic acids (WTAs) to the receptor [9]. Shear stress also increases the release of the von Willebrand factor (VWF) by human vascular endothelium [10], which acts as a binding partner for staphylococcal protein A [11]. Shear stress also induces vascular matrix remodeling, in which fibronectin reorganization plays a key role [12], thereby increasing its availability for interaction with fibronectin-binding proteins of S. aureus [13]. Also, fibronectin from ECM may become available as a binding partner due to endothelial damage caused by shear stress. Collagen can also become available as a binding partner for bacterial collagen-binding adhesins in this way. Under high-shear-stress conditions, S. aureus adheres even more strongly to collagen [14]. Together, these mechanisms suggest that the altered hemodynamic environment of a PDA may facilitate endothelial colonization and subsequent IEE.
The guideline recommendations highlight important gaps in the current evidence base. The benefit of closing hemodynamically insignificant but audible PDAs for the prevention of IEE remains uncertain, and the rationale for differentiating between audible and silent PDAs is not well established. Given that percutaneous PDA closure is an invasive procedure, while IEE is a rare but potentially fatal complication, a clear understanding of the balance between risks and benefits is essential. This review therefore examines the available evidence to determine to what extent percutaneous closure of a hemodynamically insignificant PDAs in pediatric patients reduces the risk of developing IEE, in order to determine whether this represents optimal care.
2. Materials and Methods
2.1. Case Report Research
A comprehensive literature search for previously described PDA-IEE cases was conducted using the PubMed database in May 2025. The following search terms were used: “patent ductus arteriosus AND endarteritis” and “patent ductus arteriosus AND endocarditis”. A filter for case reports was applied. In cases where two relevant patient reports were described within a single article, both were included. Articles were excluded if full-text access was not available online, even via the Utrecht University library. Additional exclusion criteria were: reports on unrelated topics, cases of IEE occurring after PDA closure, or studies involving animal subjects. No publication date restrictions were imposed.
The following information was extracted from the articles: author, publication year, patient age, PDA size, PDA flow, whether the PDA was silent or not, pathogen, and location of the vegetation. The assessment of silent PDAs was made based on the following criteria:
- If the article explicitly stated “silent PDA” → silent.
- If the article stated “no past history of a heart murmur” → silent.
- If the article stated “a new murmur” → silent.
- If the article stated “heart murmur was previously known” → not silent.
- If the article stated “heart murmur was heard, consistent with a PDA” → not silent.
- If the article stated “continuous murmur was best heard in the second left intercostal space” → not silent [15].
2.2. National Case Volume
To estimate the number of annual percutaneous PDA closures in The Netherlands, data from the Dutch society of Pediatrics were used. The National Working Group for Cardiac Catheterization in Congenital Heart Disease has prepared documents containing information on cardiac catheterizations performed in the Netherlands in children and adults with a congenital heart defect [16]. From these documents, the number of PDA closures was extracted for each center. For each year, all closures were summed, and then an annual average was calculated.
To distinguish between hemodynamically significant and insignificant PDA closures, for the same years used to calculate the annual number of closures, the catheterization reports from the Wilhelmina Children’s Hospital were reviewed to determine whether the PDA was hemodynamically significant or insignificant. Based on this, a percentage was calculated to represent the distribution between the two.
2.3. Incidence of Complications of Percutaneous Ductal Closure
To determine the incidence of complications of percutaneous ductus closure, a search of the literature was conducted.
3. Results
3.1. Case Report Research
In total, 72 cases of PDA-IEE have been described, of which 55 cases reported whether the PDA was clinically silent or not (Figure 1) (Appendix A). The publication years ranged from 1980 to 2025.
Of these 55 cases, 80% (n = 44) involved an audible PDA. Fifty-one of these cases provided information regarding the size and/or flow characteristics of the PDA. Most of these PDAs were described as “large” or measured between 5 and 10 mm in diameter, but there were also cases described as “small” or measuring 3 mm. In the majority of the audible cases, the PDA flow was characterized as “high-velocity turbulent flow”. In 40 of the 44 cases, the location of the vegetation was also reported. The most common sites were the main pulmonary artery (n = 28), pulmonary valve (n = 9), aortic valve or aorta (n = 5), left pulmonary artery (n = 5), the PDA itself (n = 4), mitral valve (n = 3), and other locations (n = 2). The total number of vegetation growths exceeded 40, as some cases involved multiple vegetations in different locations and each one was categorized individually.
The remaining 20% (n = 11) involved clinically silent PDAs. Among these cases, ten provided information regarding the size and/or flow characteristics of the PDA. Variable PDA size was reported, ranging from 1 to 6 mm. Flow characteristics were described in most cases as a tiny jet flow, but in others as high-velocity turbulent flow. Vegetation was predominantly located in the main pulmonary artery (n = 6), within the ductus itself (n = 4), on the aortic valve (n = 3), or on the pulmonary valve (n = 3).
Of the 72 documented cases, the causative pathogen was identified in 54 cases. The most frequently reported pathogens were S. aureus, Streptococcus viridans and Streptococcus sanguis.
During the exclusion process, 13 cases were excluded because the PDA was already closed at the time the endocarditis occurred. Full-text access was available for 11 of these cases. The articles provided the following information regarding the closure of the PDA: the PDA had closed spontaneously (n = 1) [17]; the PDA had been surgically or percutaneously closed with no residual shunt (n = 7) [18,19,20,21,22,23,24]; or the PDA had been surgically or percutaneously closed but a residual shunt remained (n = 3) [25,26,27]. In the cases with a shunt, the vegetation was located in the main pulmonary artery (n = 3) or the left pulmonary artery (n = 1). Among the seven cases in which the PDA had been completely closed surgically, endocarditis or endarteritis developed in four cases within 5 weeks after surgery. In the remaining cases, the infection occurred 6 to 11 years after the operation. In this latter group, vegetations were described as a narrowing of the aorta, left ventricle, and aortic valve.
3.2. National Case Volume
Data on percutaneous interventions for congenital heart disease were evaluated for the years 2017 through 2021. In 2017 there were 73 closures; in 2018, there were 71; in 2019, there were 75; in 2020, there were 75; and in 2021, there were 89. The average number of procedures performed in the Netherlands during these years was 76.6 per year. This included procedures performed on both children and adults.
The catheterization reports from Wilhelmina Children’s Hospital show that 39% of PDA closures involved hemodynamically significant PDAs, while the remaining 61% involved hemodynamically insignificant PDAs.
3.3. Incidence of Complications of Percutaneous Ductal Closure
A meta-analysis of the literature demonstrated a technical success rate of 92.2% for percutaneous PDA closure [28]. Procedures were primarily aborted for the following reasons: adverse events (AEs) such as bleeding or arrhythmia, device malposition within the aorta, device malposition within the left pulmonary artery, and technical failure. AEs were reported in 23.3% of cases, with 10.1% classified as clinically significant. Device- or coil-related complications were identified as the most common type of AE in a meta-analysis, and typically involved embolization or malposition. Embolizations were primarily observed within the pulmonary arteries and the aorta. In addition, a substantial number of access-related AEs were reported. These included hematoma or transient pulse loss that did not require therapy; pulse loss or thrombosis requiring treatment; and blood transfusion due to vascular compromise.
4. Discussion
In audible PDA cases, the ductus is typically large and associated with high-velocity turbulent flow, which generates significant shear stress. This stress likely contributes to the formation of vegetations within the PDA itself, as well as in the wall of the main pulmonary artery, particularly near the origin of the left PA where the turbulent jet usually impacts. The flow through the ductus into the pulmonary artery can also increase the pressure and mechanical stress on the pulmonary valve, providing a plausible explanation for vegetations observed at that site. Furthermore, as blood shunts into the pulmonary circulation and returns to the left heart, volume overload may develop, potentially affecting the mitral and aortic valves, which could account for the vegetations found in those regions. Together, these factors provide a plausible mechanistic explanation for the locations of vegetations observed in audible PDAs, supporting the notion that the ductus acts as a causative factor in IEE.
In cases involving silent PDAs, there was considerable variation in both the size of and the flow through the ductus. The vegetations found in cases with silent PDAs correspond to the locations observed in cases with audible PDAs. Based on PDA size, flow characteristics, and vegetation location, there does not appear to be a clear difference between audible and silent PDAs. This suggests that the underlying pathophysiological mechanisms are comparable.
The classification of “silent” PDAs is inherently ambiguous. A shunt may be too small or, paradoxically, too large to produce detectable turbulence. A small diameter can also lead to a high flow velocity and, thus, increased shear stress. Furthermore, the detection of murmurs relies on clinical auscultation, which is subjective and can vary between clinicians. Turbulent jets may also be misclassified as silent if the flow direction prevents them from being heard with a stethoscope. This challenging classification process, combined with the similarities in vegetation location between silent and audible PDAs, and the variation in size and flow observed in silent PDAs in the case report study, makes it unjustifiable to treat silent and audible PDAs as fundamentally separate categories in clinical guidelines. Although some characteristics may differ between the groups, there is no evidence to support managing these two groups differently. Both should be managed in the same way.
In the case of a residual shunt PDA, the residual flow may have caused turbulent flow and shear stress, potentially leading to IEE. Among the cases in which the PDA had been completely closed surgically, three IEEs developed shortly after surgery. This may indicate that PDA closure itself also carries a risk of IEE. In the remaining cases, the infection occurred years after the operation. Research has shown that endothelial healing after mechanical injury typically occurs within seven days [29]. Furthermore, the locations where vegetations were observed in these cases do not correspond to the typical sites associated with PDA-IEE. These observations suggest that the PDA was unlikely to have been the causative factor in these cases, and that PDA-IEEs reported in the literature may be overestimated.
Although a PDA appears to increase the risk of IEE, any potential benefit of closure must be weighed against the incidence of PDA IEE, the additional healthcare costs, and the adverse events associated with the closure procedure. A Canadian study reported a lesion-specific incidence of IE in patients with a PDA of 0.24 per 1000 patient-years, equivalent to approximately 1 case per 4166 patient-years [30]. As Canada is a developed country, the general incidence of IE is estimated at 22.5 (between 15 and 30) cases per million individuals per year, or approximately 1 case per 44,444 individuals annually (3). Therefore, the incidence of IE in patients with a PDA appears to be at least ten times higher than in the general population. The next step is to apply this incidence to the Dutch population. The Netherlands has approximately 18,073,424 inhabitants [31]. Based on a PDA incidence of 1 in 2000 live births, around 9037 individuals in the population would have a PDA (2). Given a PDA-IE incidence of 1 in 4166 individuals per year, an estimated 2.2 individuals per year in the Netherlands would develop PDA-IE.
Approximately 76.6 percutaneous PDA closures are performed annually in the Netherlands. Based on data from Wilhelmina Children’s Hospital, 61% of these are hemodynamically insignificant, corresponding to 46.7 percutaneous PDA closures. Therefore, the number needed to treat (NNT) per year to prevent one PDA IE is 21.2. The cost per percutaneous PDA closure ranges between €8630 and €14,020, resulting in an annual total cost of €182,956 to €297,224 [32]. Additionally, AEs occur in 23.3% of cases (approximately five Dutch patients annually), with 10.1% (approximately two Dutch patients annually) experiencing a clinically significant AE. Taken together, these figures highlight that percutaneous PDA closure carries substantial risks and costs, with many patients potentially experiencing harm without clear benefit.
The guideline, developed by cardiologists, does not cite evidence demonstrating that PDA closure reduces the risk of IEE. Instead, the recommendations are based on expert consensus, case reports, or standard-of-care practices, with closure of an audible PDA classified as Class IIa and closure of a silent PDA as Class IIb. These considerations raise concerns regarding the objectivity and the supporting evidence for the recommendations. While mechanistic reasoning and case-based observations suggest that a PDA may increase the risk of IEE, the literature shows that the benefits of closure do not outweigh the harms. The incidence of PDA IE is low, the NNT is high, AEs are frequent, and the costs are substantial. Therefore, such procedures should no longer be performed, and PDA closure for IEE prevention should be reclassified as a class III recommendation in the next AHA guideline.
One limitation of this study is that, for all years analyzed, the annual number of percutaneous PDA closures at the Center for Congenital Heart Disease Amsterdam–Leiden (CAHAL) includes ductus closures reported together with Major Aortopulmonary Collateral Arteries (MAPCAs) closures. As a result, the exact number of PDA closures cannot be determined. The same applies to UMC Utrecht/WKZ/Nieuwegein for the years 2020 and 2021. Following on from the first year in which MAPCA closures were included at the latter institution, we did not observe an increase in the total number of reported closures. Furthermore, MAPCA closure is performed only sporadically; therefore, this is likely to result in only a minor overestimation of the number of PDA closures.
5. Conclusions
Both pathophysiological mechanisms and case reports indicate that a PDA creates an environment conducive to IEE development, with audible and silent PDAs posing comparable risk. Closure of the PDA eliminates this environment and could therefore reduce the risk. When closure is complete and there is no residual shunt, IEE has been reported at atypical sites and times, suggesting a loss of causal association. However, considering the low incidence of PDA IEE, the high number of AEs, the high NNT, and the associated costs, current clinical guidelines warrant critical reassessment. Based on available evidence, routine closure of non-hemodynamically significant PDAs solely for IEE prevention is not clearly justified, and no distinction between audible and silent PDAs should influence management. In the next AHA guideline, both audible and silent PDA closure should be classified as a class III recommendations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gillam-Krakauer M. Mahajan K. Patent Ductus Arteriosus Stat Pearls Stat Pearls Publishing Treasure Island, FL, USA 2025 Available online: http://www.ncbi.nlm.nih.gov/books/NBK 430758/(accessed on 15 April 2025)28613509 · pubmed ↗
- 2Backes C.H. Hill K.D. Shelton E.L. Slaughter J.L. Lewis T.R. Weisz D.E. Mah M.L. Bhombal S. Smith C.V. Mc Namara P.J. Patent Ductus Arteriosus: A Contemporary Perspective for the Pediatric and Adult Cardiac Care Provider J. Am. Heart Assoc.202211 e 02578410.1161/JAHA.122.02578436056734 PMC 9496432 · doi ↗ · pubmed ↗
- 3Fortescue E.B. Lock J.E. Galvin T. Mc Elhinney D.B. To Close or Not to Close: The Very Small Patent Ductus Arteriosus Congenit. Heart Dis.2010535436510.1111/j.1747-0803.2010.00435.x 20653702 PMC 4240224 · doi ↗ · pubmed ↗
- 4Connuck D. Sun J.P. Super D.M. Kirchner H.L. Fradley L.G. Harcar-Sevcik R.A. Salvator A. Singer L. Mehta S.K. Incidence of Patent Ductus Arteriosus and Patent Foramen Ovale in Normal Infants Am. J. Cardiol.20028924424710.1016/S 0002-9149(01)02214-711792356 PMC 10246183 · doi ↗ · pubmed ↗
- 5Feltes T.F. Bacha E. Beekman R.H. Cheatham J.P. Feinstein J.A. Gomes A.S. Hijazi Z.M. Ing F.F. de Moor M. Morrow W.R. Indications for Cardiac Catheterization and Intervention in Pediatric Cardiac Disease Circulation 20111232607265210.1161/CIR.0b 013e 31821 b 1f 1021536996 · doi ↗ · pubmed ↗
- 6Setchi A. Mestel A.J. Siggers J.H. Parker K.H. Tan M.W. Wong K. Mathematical model of flow through the patent ductus arteriosus J. Math. Biol.2013671487150610.1007/s 00285-012-0596-823053537 · doi ↗ · pubmed ↗
- 7Moreillon P. Que Y.A. Bayer A.S. Pathogenesis of streptococcal and staphylococcal endocarditis Infect. Dis. Clin. N. Am.20021629731810.1016/S 0891-5520(01)00009-512092474 · doi ↗ · pubmed ↗
- 8Lee J.Y. Chung J. Kim K.H. An S.H. Kim M. Park J. Kwon K. Fluid shear stress regulates the expression of Lectin-like oxidized low density lipoprotein receptor-1 via KLF 2-AP-1 pathway depending on its intensity and pattern in endothelial cells Atherosclerosis 2018270768810.1016/j.atherosclerosis.2018.01.03829407891 · doi ↗ · pubmed ↗