Attachment Style and Perinatal Depressive Symptoms Across the Perinatal Period in Japan
Michiko Oyamada, Mitsue Sato, Tatsuma Nakao, Masahiro Sugimoto

TL;DR
The study finds that insecure attachment and high stress responses are linked to depressive symptoms during pregnancy and after childbirth in Japan.
Contribution
The study provides culturally specific evidence from Japan linking attachment insecurity and stress responses to perinatal depression.
Findings
Attachment insecurity was associated with elevated depressive symptoms at one month postpartum.
Higher psychological stress responses consistently increased odds of depressive symptoms across pregnancy stages.
Lower satisfaction with childcare environment was linked to depressive symptoms during pregnancy.
Abstract
What are the main findings? Attachment insecurity was associated with elevated depressive symptoms across the perinatal period.Higher psychological stress responses were consistently linked to EPDS positivity.Salivary cortisol showed no consistent association with depressive symptoms. Attachment insecurity was associated with elevated depressive symptoms across the perinatal period. Higher psychological stress responses were consistently linked to EPDS positivity. Salivary cortisol showed no consistent association with depressive symptoms. What is the implication of the main findings? Brief psychosocial screening during pregnancy may help identify women at risk for perinatal depression. Brief psychosocial screening during pregnancy may help identify women at risk for perinatal depression. Background/Objectives: Perinatal depressive symptoms are influenced by psychosocial and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
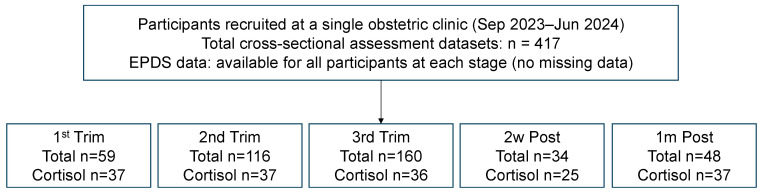 Figure 1
Figure 1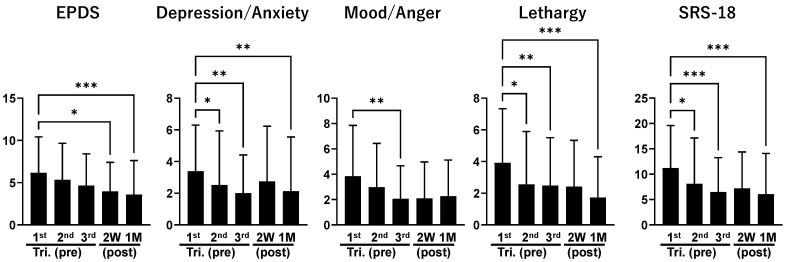 Figure 2
Figure 2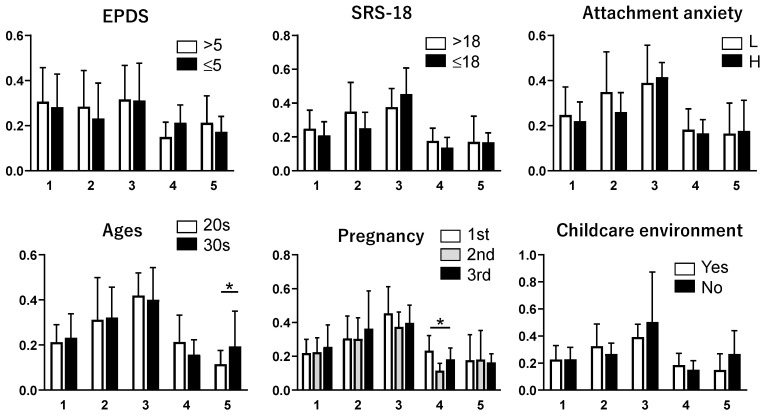 Figure 3
Figure 3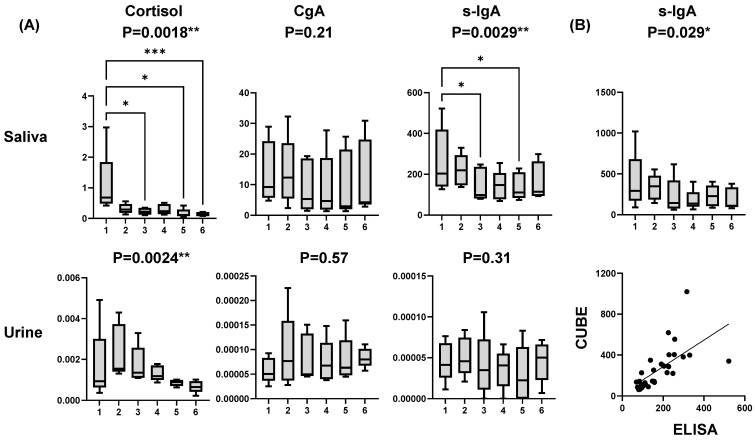 Figure 4
Figure 4- —JSPS KAKENHI
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal Mental Health During Pregnancy and Postpartum · Attachment and Relationship Dynamics · Stress Responses and Cortisol
1. Introduction
Postpartum depression (PPD) is a significant mental health problem affecting approximately 13–19% of new mothers worldwide [1,2]. PPD has profound effects on both mothers and infants, leading to impaired mother-infant bonding, difficulties with breastfeeding, and long-term developmental problems in children [3,4]. Furthermore, in the most severe cases, it can lead to maternal suicide, which is a leading cause of maternal mortality in the postpartum period [5,6]. In Japan, the prevalence of PPD is reported to be around 10% [7,8], indicating a serious maternal mental health problem. In Japan, there is an increasing trend of suicide among women within the first year postpartum [9], highlighting the importance of early identification and intervention to mitigate these adverse outcomes.
The Edinburgh Postnatal Depression Scale (EPDS) is a widely used self-report questionnaire for screening PPD [10]. The EPDS has demonstrated reliability and validity in diverse populations and is considered a widely used and well-validated screening instrument for postpartum depression [11]. In addition, studies have examined antenatal EPDS scores and pregnant women’s background factors to predict early PPD [12,13]. These studies have identified risk factors for postpartum depression and indicated the potential for preventive interventions. However, while the EPDS provides valuable insight into the psychological aspects of PPD, it does not capture the biological basis.
Recent research has explored the role of biological markers in diagnosing and understanding PPD. Cortisol, a hormone released in response to stress, is primarily measured in biological samples such as blood, urine, and saliva. In particular, cortisol has been identified as a potential biomarker for PPD [14]. Salivary cortisol measurement is a non-invasive and convenient method for assessing hypothalamic–pituitary–adrenal (HPA) axis activity [15]. Studies investigating the relationship between salivary cortisol and PPD have reported that women with postpartum depression have abnormal cortisol secretion patterns [16,17]. Furthermore, elevated cortisol levels are associated with both antenatal and postnatal depression, suggesting a link between stress and the onset of depressive symptoms in new mothers [18,19]. These studies indicate that salivary cortisol measurements may provide valuable insights into the physiological stress response of postpartum women and may be helpful for the early detection and intervention of PPD.
Attachment theory, proposed by John Bowlby (1969), posits that the emotional bond formed between infants and their primary caregivers plays a crucial role in subsequent social and emotional development [20]. Bowlby theorized that attachment serves as a secure base, enabling children to explore their surroundings and cope with stress with confidence. Mary Ainsworth further advanced this theory by employing the “Strange Situation” experimental procedure to categorize children’s attachment styles as “secure,” “insecure–avoidant,” or “insecure–ambivalent” [21]. Although these classifications were originally developed for infants, similar conceptual frameworks have been applied to adult attachment patterns. PPD has been demonstrated to exert an influence on maternal attachment styles, with the potential to exert adverse effects on mother-infant interactions and child development [22]. Research findings indicate that insecure attachment styles may serve as risk factors for the development of PPD [23]. Consequently, it is imperative to incorporate the assessment of maternal attachment styles into postpartum mental health evaluations to facilitate the timely identification and management of PPD.
International studies conducted in Europe and North America have similarly reported associations between attachment insecurity and perinatal depressive symptoms [24,25], suggesting that attachment-related vulnerability may represent a cross-cultural risk factor. Prospective and longitudinal research has further demonstrated that attachment insecurity may moderate the impact of perinatal stress on depressive outcomes [25]. However, the strength and expression of these associations may vary across sociocultural contexts, including family structures, partner support, and expectations regarding maternal roles [2]. Cross-national reviews have emphasized that social support systems and culturally embedded parenting norms influence the prevalence and manifestation of perinatal depression [26]. In East Asian contexts such as Japan, where extended family involvement and social norms surrounding motherhood differ from Western settings, the psychosocial dynamics of perinatal mental health may follow distinct patterns [27]. Therefore, culturally specific empirical evidence is needed to clarify whether attachment-related vulnerabilities operate similarly across contexts.
Therefore, the present study aimed to examine the cross-sectional associations between perinatal depressive symptoms and psychosocial and relational factors, including adult attachment style, psychological stress responses, and satisfaction with the childcare environment, across multiple perinatal stages in Japan. In addition, salivary cortisol was assessed as an exploratory physiological stress marker to complement psychological measures. We hypothesized that attachment insecurity, higher psychological stress responses, and lower satisfaction with the childcare environment would be associated with elevated perinatal depressive symptoms at each perinatal stage. In contrast, associations with salivary cortisol would be less consistent. To address these aims, we conducted a repeated cross-sectional study in which independent samples of women were assessed at five perinatal stages, from early pregnancy to the early postpartum period. By focusing on stage-specific associations rather than within-individual change, this study seeks to clarify patterns of psychosocial vulnerability related to perinatal depressive symptoms while avoiding causal or longitudinal assumptions.
2. Materials and Methods
2.1. Study Design
This study employed a repeated cross-sectional observational design, analyzing data collected at five separate time points as independent snapshots, without modeling within-subject changes over time. The five time points included the first trimester, the second trimester, the third trimester, two weeks postpartum, and one month postpartum. Because participant identifiers could not be consistently linked across all time points, longitudinal modeling was not feasible, and each assessment was treated as an independent cross-sectional snapshot. At each of the five perinatal stages, data were collected from different individuals. No participant contributed data at more than one point. Accordingly, all observations were independent, and each stage represents a distinct cross-sectional sample.
2.2. Participants and Recruitment
Participants were recruited from a single obstetric clinic in Japan between September 2023 and June 2024. Inclusion criteria were age ≥18 years, singleton pregnancy, and ability to complete self-administered questionnaires in Japanese. Women with known psychiatric diagnoses or pregnancy complications were excluded. Data were collected at five predefined perinatal stages (first, second, and third trimesters of pregnancy; two weeks postpartum; and one month postpartum). At each stage, participants were recruited independently during routine prenatal or postpartum visits. Each assessment represented a different individual at a single perinatal stage, and no participant contributed data at more than one assessment point. All questionnaire data were therefore analyzed as independent cross-sectional samples without linkage across stages. Salivary samples were collected at the same visits when feasible. Among all participants included in the study, 172 individuals provided saliva samples for cortisol analysis. Because saliva collection depended on visit timing, participant consent, and logistical feasibility, biological data were available only for a subset of the cross-sectional samples. Accordingly, analyses involving salivary cortisol were conducted as exploratory, stage-specific cross-sectional analyses (Figure 1). This study was conducted as an observational investigation. No structured psychological or behavioral interventions were implemented as part of the study protocol. Participants received routine obstetric care only during pregnancy and the postpartum period.
2.3. Psychological Assessments
Perinatal depressive symptoms were assessed using the Edinburgh Postnatal Depression Scale (EPDS), a 10-item self-report questionnaire validated for use in Japanese populations. Stress responses were measured using the Stress Response Scale-18 (SRS-18), which evaluates psychological stress across multiple domains. Adult attachment style was assessed using the Relationship Questionnaire (RQ), a validated self-report measure that categorizes individuals into four attachment styles: secure, fearful, preoccupied, and dismissing.
The attachment styles were also reclassified into two broader categories for secondary analyses. Participants were dichotomized into secure and insecure groups to enhance statistical power.
The collected information included the following variables: (1) age, (2) parity, (3) gestational age, (4) history of stillbirth or miscarriage, (5) psychiatric history, (6) social support (from husband, biological mother, and other sources), (7) economic concerns, (8) living environment, (9) attachment style, (10) SRS-18 score, and (11) EPDS score.
For the EPDS, a cut-off score of ≥11 was used to indicate potential depression during pregnancy [28,29,30], whereas a cut-off score of ≥9 was applied in the postpartum period [11,31]. These different thresholds were selected based on validation studies specific to antenatal and postpartum populations. Attachment styles were assessed and categorized into four types: secure, dismissing, preoccupied, and fearful. Attachment style was also dichotomized for the analyses into secure versus insecure categories. For the SRS-18, a score ≥18 indicated a high stress level, whereas a score <18 indicated a low stress level [32].
Adult attachment styles were assessed using the Relationship Questionnaire (RQ), which presents four brief descriptions corresponding to secure, fearful, preoccupied, and dismissing attachment styles. Participants rated the extent to which each description applied to them on a 7-point Likert scale.
For analytical purposes, attachment styles were classified in two ways. First, participants were categorized into four styles—secure, fearful, preoccupied, and dismissing—based on their forced-choice responses on the RQ. Second, attachment styles were dichotomized into secure and insecure groups for secondary analyses to increase statistical power.
2.4. Biological Data
Salivary cortisol analyses were exploratory due to the limited sample size and incomplete pairing across time points. Salivary cortisol was collected as a supplementary biological marker to explore physiological stress responses. Samples were obtained at routine prenatal and postpartum visits using a standardized passive drool method. To ensure homogeneity of sample collection, saliva samples were obtained under standardized conditions within the same clinical facility. Based on preliminary validation of diurnal variation, samples in the main study were collected after breakfast during outpatient visits to minimize circadian variation. Participants were instructed to avoid oral hygiene procedures and strenuous physical activity for at least one hour before the sample collection. All samples were immediately cooled and stored at −80 °C until analysis. Details regarding sampling times, storage procedures, and assay protocols are provided in Appendix A. Salivary cortisol was measured in a subset of participants (n = 172) who provided saliva samples at a single perinatal stage.
2.5. Statistical Analysis
All analyses were performed separately for each perinatal stage, treating each stage as an independent cross-sectional sample. Within each stage, participants were classified into high- and low-EPDS groups based on predefined cut-off values for the pregnancy and postpartum periods.
Categorical variables were analyzed using Fisher’s exact test (two-sided). For 2 × 2 comparisons, odds ratios (ORs) and 95% confidence intervals (CIs) were calculated directly. For categorical variables with more than two categories, each non-reference category was compared with the predefined reference category using separate 2 × 2 Fisher’s exact tests, and corresponding ORs and 95% CIs were calculated. ORs were not estimated when any cell count was zero, and no continuity correction was applied.
For continuous variables, comparisons between two groups were conducted using the Mann–Whitney U test. When comparisons involved three or more groups, the Kruskal–Wallis test was applied, followed by Dunn’s multiple-comparison test as a post hoc analysis. Because the sample size for salivary cortisol measurements was limited and differed across stages, analyses involving cortisol were exploratory. For these analyses, participants at each stage were dichotomized using the stage-specific median EPDS score, and cortisol concentrations were compared between groups. All statistical analyses were conducted using JMP Pro (version 16.1.0; SAS Institute, Cary, NC, USA) and GraphPad Prism (version 9.2.0; GraphPad Software, La Jolla, CA, USA). Effect sizes are presented as odds ratios (ORs) with 95% confidence intervals to facilitate interpretation of the magnitude of association. Primary analyses focused on associations between EPDS status and adult attachment, psychological stress responses (SRS-18), and satisfaction with the childcare environment. Other stage-specific variables were examined as exploratory secondary analyses. Given the number of comparisons performed, findings from secondary analyses should be interpreted cautiously, and no formal correction for multiple testing was applied.
2.6. Ethical Considerations
This study followed the ethical principles of the Helsinki Declaration. Before participating in the study, participants received verbal and written information. It was emphasized that participation in the study, the option to withdraw after consent, and the interpretation of the results would not affect their subsequent medical care. Participants were informed of their right to withdraw from the study at any time. They were told they also had the right to request deletion of their data and that, in the event of publication, measures would be taken to ensure individuals could not be identified. Ethical approval was obtained from the Nihon Institute of Medical Science (No. 2022012, approved on 13 October 2022).
3. Results
Because the study employed a repeated cross-sectional design, all stage-specific comparisons reflect differences between independent samples rather than within-individual changes over time. During pregnancy (Table 1), lower satisfaction with the residential environment for child-rearing was associated with increased odds of elevated depressive symptoms, whereas higher satisfaction was associated with reduced odds. Higher psychological stress responses were consistently associated with increased odds of elevated EPDS across pregnancy stages. In the postpartum period (Table 2), attachment insecurity (two-category model) was associated with higher odds of EPDS, reaching statistical significance at one month postpartum. Higher SRS-18 scores were consistently associated with higher EPDS scores across postpartum assessments. Further exploratory results are presented in Appendix B (Table A1).
Figure 2 presents descriptive distributions of EPDS and SRS-18 scores across the five perinatal stages. Differences in score distributions were observed across stages; however, these findings are descriptive and do not represent within-individual changes over time, given the study’s repeated cross-sectional design. Overall, higher EPDS scores were more frequently observed during pregnancy, whereas lower scores were more common in the postpartum stages. Psychological stress responses, as measured by the SRS-18, showed a similar stage-dependent pattern across assessments.
Salivary cortisol analyses were conducted as an exploratory component of the study, informed by a preliminary validation study summarized in Appendix A. As shown in Figure 3, cortisol concentrations varied stage-specifically across pregnancy and the postpartum period. However, no clear or consistent associations were observed between cortisol levels and elevated depressive symptoms (EPDS>5), defined using the sample mean EPDS score as a stage-specific exploratory cut-off, at any assessment stage. Additional subgroup analyses suggested limited stage-specific differences in participant characteristics, but these findings were inconsistent across stages.
4. Discussion
This study examined stage-specific associations between perinatal depressive symptoms and psychosocial and physiological factors using a repeated cross-sectional design. Across pregnancy and the early postpartum period, attachment insecurity and higher psychological stress responses were consistently associated with elevated depressive symptoms. These findings align with previous research identifying attachment insecurity as a vulnerability factor for perinatal mood disturbances [24,33]. They are consistent with international reviews emphasizing the importance of psychosocial resilience and relational factors in perinatal mental health [34]. From a theoretical perspective, attachment insecurity may heighten perceived stress and impair emotional regulation, thereby increasing vulnerability to depressive symptoms during the perinatal period [33].
Across both pregnancy and the postpartum period, elevated depressive symptoms were consistently accompanied by higher psychological stress responses, as measured by the SRS-18. This pattern supports prior evidence that psychological stress plays a central role in the development and maintenance of perinatal mood disturbances [27,35]. In this context, the use of validated self-report instruments such as the EPDS and SRS-18 provides a practical and sensitive approach for identifying psychological vulnerability in clinical and public health settings [10,36].
These findings may be interpreted within established attachment and stress–depression frameworks. Attachment theory posits that attachment insecurity is associated with heightened sensitivity to perceived threat and reduced capacity for effective emotional regulation [33]. During the perinatal period, which is characterized by substantial psychological and physiological transitions, individuals with attachment insecurity may experience amplified stress appraisal and diminished coping resources. According to stress–diathesis models, such heightened stress reactivity may increase vulnerability to depressive symptoms when exposed to contextual stressors [37]. The present findings are consistent with this integrative perspective, suggesting that attachment-related emotional regulation patterns and psychological stress responses may jointly contribute to perinatal depressive symptoms.
In contrast, physiological stress markers, including salivary cortisol and chromogranin A (CgA), did not show clear or consistent associations with depressive symptoms or attachment patterns in the present study. This finding differs from some previous reports describing altered cortisol profiles among individuals with depressive symptoms or insecure attachment [15,38]. Several methodological and biological factors may account for this discrepancy. First, cortisol secretion is strongly influenced by diurnal variation, and sampling time can substantially affect measured concentrations [39]. Second, individual variability in stress reactivity and pregnancy-related hormonal changes may obscure group-level differences. Third, single-point cortisol measurements may be insufficient to capture chronic stress exposure or dysregulation of the hypothalamic–pituitary–adrenal (HPA) axis [40]. The absence of clear associations may reflect physiological adaptation of the HPA axis during pregnancy and the postpartum period rather than a true absence of stress-related biological processes.
The selection of salivary cortisol as a physiological stress marker in this study was informed by a preliminary validation experiment examining diurnal variation, summarized in Appendix A. Consistent with previous literature [15,39], this pilot study confirmed a clear circadian rhythm of cortisol, with higher levels in the morning and lower, more variable levels later in the day. In the main study, saliva samples were collected during daytime outpatient visits after breakfast, which may have reduced sensitivity compared with early morning sampling, when cortisol levels are typically higher and more dynamic. While this protocol minimized inter-individual variability and enhanced procedural consistency, it may have limited the ability to detect subtle differences associated with depressive symptoms. Future studies may benefit from standardized morning sampling or repeated measurements to better characterize stress-related endocrine activity.
CgA, a marker of sympathetic nervous system activity, also showed no robust associations with depressive symptoms or attachment patterns. Although CgA has been proposed as a potential biomarker of psychological stress [41,42], its reliability and clinical utility in pregnant and postpartum populations remain uncertain. Overall, these findings suggest that psychological indicators may currently offer greater robustness and clinical relevance than physiological stress markers for assessing perinatal mental health.
Importantly, the cortisol analyses in the present study were conducted in a sample with relatively low overall depressive symptom severity. The average EPDS score among participants included in the cortisol analyses was comparable to levels reported in previous postpartum studies [33]. This restricted range of symptom severity may have further limited the ability to detect clear associations between cortisol concentrations and depressive symptoms.
In addition, the absence of significant associations between salivary cortisol and depressive symptoms may reflect physiological adaptation of the hypothalamic–pituitary–adrenal (HPA) axis during pregnancy and the postpartum period. Pregnancy is characterized by altered baseline endocrine activity and stress responsiveness, which may attenuate detectable differences in cortisol levels between individuals with and without elevated depressive symptoms. Therefore, the present findings should not be interpreted as evidence against biological involvement in perinatal depression, but rather as an indication that single-point salivary cortisol measurements may have limited sensitivity in this context.
The present findings also highlight the potential value of attachment-based screening in perinatal care. Adult attachment styles, as assessed using the Relationship Questionnaire [41], provide insight into interpersonal functioning and emotion regulation. Attachment insecurity may serve as a useful indicator of heightened psychological stress and depressive symptoms, supporting the integration of attachment assessments into routine maternal mental health evaluations [24].
From a clinical perspective, these findings suggest that a brief assessment of adult attachment style and perceived childcare environment satisfaction during pregnancy may help identify women at increased risk for perinatal depressive symptoms. Incorporating psychosocial screening into routine obstetric care may facilitate early identification of vulnerability, particularly among women exhibiting attachment insecurity patterns or elevated psychological stress responses.
Finally, this study has several limitations. These can be broadly categorized as methodological and substantive limitations. Methodological limitations include the repeated cross-sectional design, which precludes causal inference and within-individual analysis. Substantive limitations include limited stage-specific subgroup sizes, potential participant heterogeneity, and the absence of long-term longitudinal follow-up. In addition, residual confounding by unmeasured factors such as socioeconomic conditions, detailed psychiatric history, or partner dynamics cannot be excluded. In addition, a relatively large number of stage-specific comparisons were performed, particularly in exploratory analyses, which increases the possibility of type I error. Therefore, these findings should be interpreted with caution and considered hypothesis-generating rather than confirmatory.
Furthermore, biological stress markers were available only in a subset of participants, which may have reduced statistical power for cortisol-related analyses. Despite these limitations, the present study provides culturally specific data from a Japanese clinical context, offering valuable insight into perinatal mental health and attachment-related processes in a non-Western population. Future longitudinal and multi-site studies across diverse cultural settings are warranted to clarify causal pathways and enhance generalizability.
5. Conclusions
In this repeated cross-sectional study, adult attachment insecurity, lower satisfaction with the childcare environment, and higher psychological stress responses were associated with elevated perinatal depressive symptoms across selected perinatal stages. These findings highlight the potential relevance of psychosocial and relational factors in perinatal mental health, while acknowledging that causal relationships cannot be inferred from the present design. Future longitudinal studies with repeated within-individual assessments are needed to clarify causal pathways and long-term maternal and child outcomes. From a clinical perspective, integrating a brief assessment of adult attachment style and psychosocial stress responses into routine perinatal care may facilitate earlier identification of women at increased risk for depressive symptoms and support timely, targeted interventions aimed at promoting maternal mental health.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Woody C.A. Ferrari A.J. Siskind D.J. Whiteford H.A. Harris M.G. A systematic review and meta-regression of the prevalence and incidence of perinatal depression J. Affect. Disord.2017219869210.1016/j.jad.2017.05.00328531848 · doi ↗ · pubmed ↗
- 2Hahn-Holbrook J. Cornwell-Hinrichs T. Anaya I. Economic and Health Predictors of National Postpartum Depression Prevalence: A Systematic Review, Meta-analysis, and Meta-Regression of 291 Studies from 56 Countries Front. Psychiatry 2017824810.3389/fpsyt.2017.0024829449816 PMC 5799244 · doi ↗ · pubmed ↗
- 3Field T. Postpartum depression effects on early interactions, parenting, and safety practices: A review Infant. Behav. Dev.2010331610.1016/j.infbeh.2009.10.00519962196 PMC 2819576 · doi ↗ · pubmed ↗
- 4Stewart D.E. Vigod S.N. Postpartum Depression: Pathophysiology, Treatment, and Emerging Therapeutics Annu. Rev. Med.20197018319610.1146/annurev-med-041217-01110630691372 · doi ↗ · pubmed ↗
- 5Oates M. Suicide: The leading cause of maternal death Br. J. Psychiatry 200318327928110.1192/bjp.183.4.27914519602 · doi ↗ · pubmed ↗
- 6Palladino C.L. Singh V. Campbell J. Flynn H. Gold K.J. Homicide and suicide during the perinatal period: Findings from the National Violent Death Reporting System Obstet. Gynecol.20111181056106310.1097/AOG.0b 013e 31823294 da 22015873 PMC 3428236 · doi ↗ · pubmed ↗
- 7Nishigori H. Obara T. Nishigori T. Metoki H. Mizuno S. Ishikuro M. Sakurai K. Hamada H. Watanabe Z. Hoshiai T. The prevalence and risk factors for postpartum depression symptoms of fathers at one and 6 months postpartum: An adjunct study of the Japan Environment & Children’s Study J. Matern. Fetal Neonatal Med.2020332797280410.1080/14767058.2018.156041530563402 · doi ↗ · pubmed ↗
- 8Matsumoto K. Tsuchiya K.J. Itoh H. Kanayama N. Suda S. Matsuzaki H. Iwata Y. Suzuki K. Nakamura K. Mori N. Age-specific 3-month cumulative incidence of postpartum depression: The Hamamatsu Birth Cohort (HBC) Study J. Affect. Disord.201113360761010.1016/j.jad.2011.04.02421601291 · doi ↗ · pubmed ↗