Serum Protein Electrophoresis and the Albumin-to-Globulin Ratio in the Differential Diagnosis of Minimal Change Disease and Focal Segmental Glomerulosclerosis
László Bitó, Tamás Lantos, Krisztina Jost, Amir Reza Manafzadeh, Béla Iványi, Levente Kuthi

TL;DR
This study explores how serum protein electrophoresis and the albumin-to-globulin ratio can help distinguish between two kidney diseases, MCD and FSGS, especially in severe cases.
Contribution
The study identifies the albumin-to-globulin ratio as a novel biomarker for differentiating secondary FSGS from immune-mediated podocytopathies using routine electrophoretic profiles.
Findings
Secondary FSGS has significantly higher albumin-to-globulin ratios compared to MCD and primary FSGS.
An A/G ratio > 0.49 identifies primary FSGS with high sensitivity and specificity in severe cases.
The inverse correlation between albumin and α2-globulin is stronger in immune-mediated diseases than in secondary FSGS.
Abstract
Background/Objectives: Differentiating minimal change disease (MCD) from focal segmental glomerulosclerosis (FSGS) remains a diagnostic challenge. We hypothesised that differences in glomerular protein selectivity could translate into distinct serum protein electrophoresis (SPEP) profiles, particularly in severe nephrotic syndrome. Methods: We retrospectively analysed SPEP profiles of adults with biopsy-proven MCD (n = 27), primary FSGS (n = 27), and secondary FSGS (n = 20). Diagnoses were established according to KDIGO guidelines and the Mayo Clinic classification. A severe subgroup was defined by a relative albumin fraction <40% to evaluate patterns in marked hypoalbuminaemia. Results: Secondary FSGS demonstrated significantly higher albumin-to-globulin (A/G) ratios compared with immune-mediated podocytopathies (MCD and primary FSGS), yielding excellent discrimination (AUC > 0.98). In…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
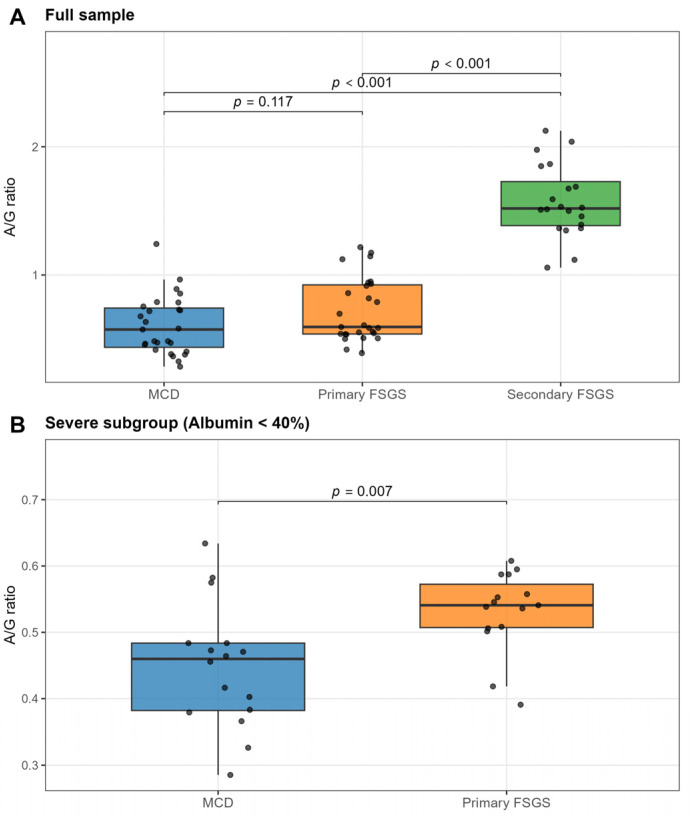 Figure 1
Figure 1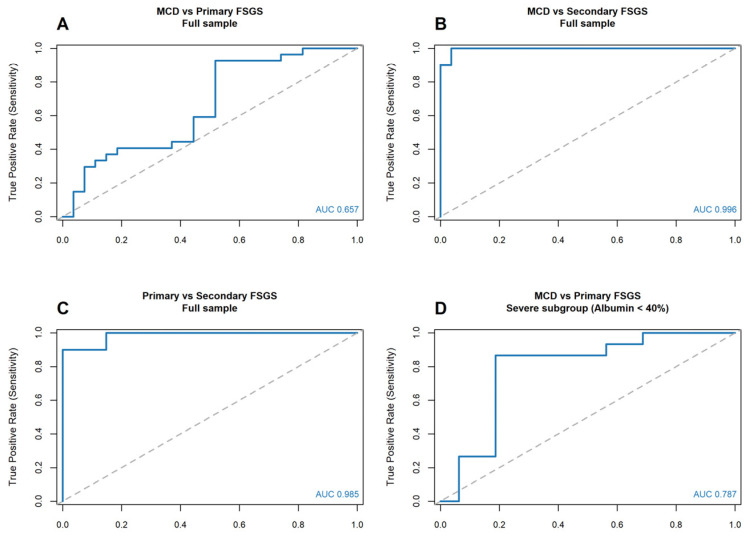 Figure 2
Figure 2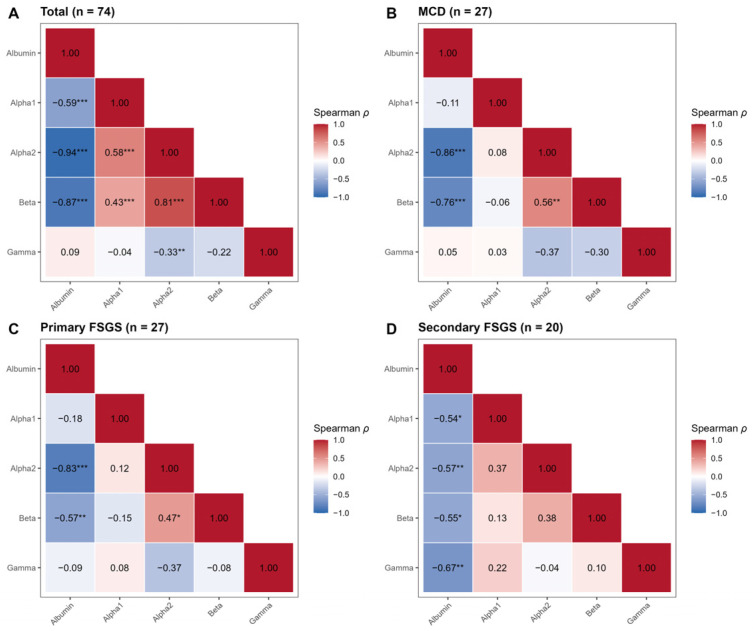 Figure 3
Figure 3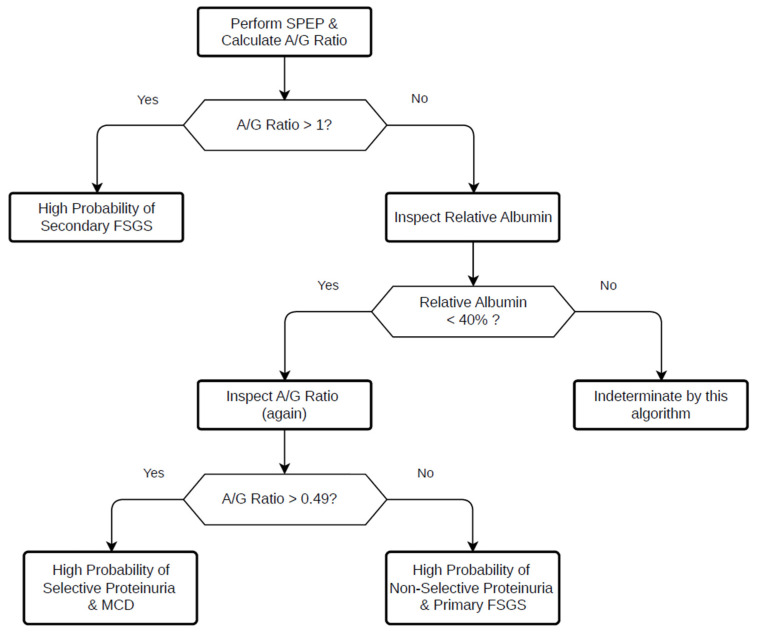 Figure 4
Figure 4- —University of Szeged Open Access Fund
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRenal Diseases and Glomerulopathies · Vasculitis and related conditions · Amyloidosis: Diagnosis, Treatment, Outcomes
1. Introduction
Podocytopathies, including minimal change disease (MCD) and focal segmental glomerulosclerosis (FSGS), represent major causes of idiopathic nephrotic syndrome in adults [1]. Although membranous nephropathy remains prevalent, epidemiological data from large biopsy registries indicate a rising incidence of FSGS, which has become the leading cause of primary nephrotic syndrome in several multiethnic populations [1].
Distinguishing MCD from FSGS remains a clinical challenge [2]. Although the two conditions often present with similar clinical features characterised by heavy proteinuria, their underlying pathobiology differs substantially. In MCD, injury is characterised by diffuse podocyte foot process effacement without significant podocyte loss, thereby allowing potential reversibility [3,4]. In contrast, FSGS is defined by podocyte depletion and irreversible segmental scarring, reflecting permanent structural damage to the glomerular filtration barrier [5,6].
These distinct pathological processes result in differences in glomerular permeability. MCD typically produces highly selective proteinuria predominantly involving albumin, whereas FSGS is associated with nonselective proteinuria characterised by leakage of higher-molecular-weight proteins. [7]. Although renal biopsy remains the diagnostic gold standard, its diagnostic accuracy is limited by sampling variability, particularly in FSGS, where lesions are focal and segmental [3,8]. Moreover, distinguishing primary from secondary FSGS has direct therapeutic implications, as inappropriate immunosuppression may expose patients to unnecessary risk [9].
Serum protein electrophoresis (SPEP) is routinely performed in the evaluation of nephrotic syndrome. Beyond its established role in detecting monoclonal gammopathies, SPEP reveals a characteristic “nephrotic pattern” marked by hypoalbuminaemia and relative elevation of α2 and β fractions [10]. These changes reflect both urinary protein loss and compensatory hepatic synthesis [11,12]. While this pattern is generally regarded as a uniform response to nephrotic-range proteinuria [13], it remains unclear whether subtle differences in electrophoretic profiles reflect the selectivity of the underlying glomerular injury.
Albumin contributes disproportionately to plasma oncotic pressure due to its abundance and molecular characteristics [14]. Selective albumin loss may therefore trigger distinct systemic responses compared with non-selective proteinuria [15]. We hypothesised that differences in glomerular size-selectivity between MCD and FSGS could translate into measurable differences in serum protein fractions, particularly in the albumin-to-globulin (A/G) ratio.
This study aimed to compare SPEP profiles in patients with biopsy-proven MCD and FSGS and to determine whether electrophoretic patterns can serve as a non-invasive adjunct in differentiating podocytopathies. To our knowledge, a systematic comparative analysis of SPEP patterns across these podocytopathies has not previously been reported in the English-language literature.
2. Materials and Methods
2.1. Study Population
The study was approved by the Regional Human Biomedical Research Ethics Committee (Licence No. 26/2024-SZTE RKEB). We retrospectively analysed 74 adult patients with biopsy-proven podocytopathies treated at the University of Szeged between 2009 and 2025. The final study cohort comprised patients with MCD (n = 27), primary FSGS (n = 27), and secondary FSGS (n = 20). Within the MCD group, a secondary aetiology was identified in 18.5% of patients. Inclusion criteria were a definitive histological diagnosis of MCD or FSGS and the availability of complete clinical and laboratory data from the peri-biopsy period. To minimise systemic confounders that might affect SPEP profiles, strict exclusion criteria were applied. Patients with monoclonal gammopathy, liver cirrhosis, or prior immunosuppressive therapy before sampling were excluded. Furthermore, patients with a documented history of active infectious diseases (e.g., HIV, hepatitis B or C) and those with severe secondary metabolic nephropathies (e.g., advanced diabetic nephropathy) were also excluded from the analysis. Because the primary aim of this study was the differential diagnosis among specific pathological entities presenting with nephrotic syndrome, a healthy control (negative) group was not included. Diagnoses were established based on clinical and histopathological findings. The kidney samples were obtained by an ultrasound-guided percutaneous biopsy. All samples were evaluated by light microscopy using special staining, direct immunofluorescence (IF) on frozen sections (FITC-conjugated antibodies to IgG, IgA, IgM, C3, C1q, kappa, lambda, and fibrinogen [Dako, Glostrup, Denmark]), and electron microscopy (EM).
MCD was diagnosed in patients with nephrotic syndrome who exhibited minimal or no abnormalities on light microscopy or IF, and diffuse podocyte foot process effacement (≥80% of the capillary circumference) was observed on EM [16].
The clinicopathologic approach of the Mayo Clinic was used to differentiate primary and secondary FSGS. Primary FSGS was diagnosed in patients with massive proteinuria or nephrotic syndrome when segmental sclerosis was identified in at least one glomerulus; IF microscopy excluded immune complex deposition, EM demonstrated diffuse podocyte foot process effacement, and secondary causes of FSGS, such as long-standing hypertension, adaptive-functional responses, malignancy, drug exposure, or viral infection, were clinically excluded [17].
Secondary FSGS was diagnosed when a proteinuric patient exhibited an FSGS lesion on light microscopy; there were no immune complexes on IF, EM revealed segmental podocyte foot process effacement, and secondary causes of FSGS were present clinically [9].
For analytical purposes, primary FSGS and the entire MCD cohort (including secondary forms) were collectively referred to as immune-mediated podocytopathies [18], consistent with current pathophysiological concepts.
2.2. Laboratory Analysis
Serum samples were obtained at the time of renal biopsy or during the immediate peri-biopsy period, before initiation of disease-specific immunosuppressive therapy.
SPEP was performed using a Sebia Hydrasys 2 system (Sebia, Lisses, France) with agarose gel (Sebia Hydragel B1–B2), and standard fractions were quantified (albumin, α1, α2, β, and γ) [10].
The A/G ratio was calculated from relative electrophoretic fractions as:
where globulins represent the sum of the α1, α2, β, and γ fractions.
2.3. Definition of Severe Subgroup
Patients were stratified into a severe subgroup defined by a relative albumin fraction <40%. This threshold corresponds approximately to the classical nephrotic range of absolute serum albumin (<25 g/L; <30 g/L in contemporary guidelines) [19]. The relative albumin fraction was selected to minimise the influence of volume status and haemodilution, which may confound absolute albumin concentrations [20].
This stratification enabled comparison among patients with similarly severe hypoalbuminaemia.
2.4. Statistical Analysis
Normality was assessed using histograms and the Shapiro–Wilk test. Normally distributed continuous variables were analysed using the independent samples t-test or one-way ANOVA with Tukey’s HSD post hoc test and are presented as mean ± SD. Non-normally distributed variables were analysed using the Mann–Whitney U test or the Kruskal–Wallis test with Dwass–Steel–Critchlow–Fligner post hoc comparisons and are presented as median (interquartile range, IQR). Associations were assessed using Spearman’s rank correlation coefficient (ρ). Categorical variables were compared using the chi-squared test. Diagnostic performance was evaluated using receiver operating characteristic (ROC) curves, and the area under the curve (AUC) was calculated. All tests were two-sided, with p < 0.05 considered statistically significant. All analyses were performed using R version 4.4.1 (R Foundation for Statistical Computing, Vienna, Austria).
3. Results
3.1. Baseline Characteristics of the Study Population
Baseline demographic and laboratory characteristics are summarised in Table 1. No statistically significant differences were observed among the three groups with respect to age (p = 0.114) or sex distribution (p = 0.251), indicating comparable demographic comparability.
Marked differences were observed in laboratory profiles. Patients with MCD and primary FSGS demonstrated a phenotype consistent with severe nephrotic syndrome, characterised by pronounced hypoalbuminaemia and elevated α2- and β-globulin fractions. In contrast, patients with secondary FSGS exhibited significantly higher median relative albumin fractions (60.3% vs. approximately 36–37% in MCD and primary FSGS; p < 0.001) and a comparatively preserved electrophoretic profile, consistent with the absence of overt nephrotic syndrome.
Importantly, no statistically significant differences were detected in electrophoretic patterns between patients with idiopathic MCD and those with identifiable secondary causes. Given this phenotypic overlap, these subgroups were pooled for subsequent analyses. Furthermore, strict exclusion criteria were applied to minimise potential confounders affecting the A/G ratio. In particular, monoclonal gammopathy (paraproteinaemia) was absent in all patients, ensuring that the observed electrophoretic alterations reflected podocytopathy-associated protein distribution.
3.2. The ‘Quiescent Liver’: Identifying Secondary FSGS
Secondary FSGS exhibited a markedly distinct serum protein profile compared with immune-mediated podocytopathies, as illustrated by both boxplot analysis (Figure 1A) and ROC analysis (Figure 2B,C).
The median A/G ratio was significantly higher in secondary FSGS (1.52, IQR 1.39–1.73) than in MCD (0.58, IQR 0.44–0.74) and primary FSGS (0.60, IQR 0.54–0.92) (p < 0.001 for both comparisons). Consequently, the A/G ratio demonstrated excellent discriminatory ability for identifying secondary FSGS. An A/G ratio > 1.01 effectively excluded MCD (sensitivity 100%, specificity 96.3%; AUC = 0.996) and robustly differentiated secondary from primary FSGS (AUC = 0.985). These findings indicate that preservation of the A/G ratio is characteristic of secondary FSGS and contrasts with the pronounced electrophoretic alterations observed in immune-mediated podocytopathies. This distinct pathophysiological pattern is further reflected in the correlation matrices (Figure 3). Whereas immune-mediated podocytopathies exhibited a strong inverse association between albumin fraction and α2-globulin fraction, secondary FSGS showed a significantly weaker correlation (ρ = −0.57, p = 0.009; Figure 3D). This relative attenuation suggests a reduced coupling between albumin depletion and compensatory α2-globulin increase in secondary FSGS.
3.3. MCD vs. Primary FSGS: The ‘Selective Retention’ Effect
In the overall study population, discrimination between MCD and primary FSGS was modest. As shown in Figure 1A and Figure 2A, there was substantial overlap in A/G ratios between the two groups, and the difference did not reach statistical significance (p = 0.117). Accordingly, diagnostic performance in the full cohort was modest (AUC = 0.657).
This overlap likely reflects the inclusion of patients with milder disease activity or partial remission, in whom electrophoretic alterations may be attenuated and therefore insufficient to produce distinct biochemical separation between the two entities.
However, within the severe subgroup (defined as relative albumin fraction < 40%), the biological distinction became more pronounced and clinically relevant (Figure 1B and Figure 2D).
In contrast to the full cohort, the severe subgroup (relative albumin fraction < 40%) demonstrated a statistically significant difference in the A/G ratio between MCD and primary FSGS (p = 0.007). Within this subgroup, the A/G ratio showed moderate-to-good discriminatory performance, with an AUC of 0.787. From a clinical perspective, an A/G cut-off >0.494 identified primary FSGS with a sensitivity of 86.7% and a specificity of 81.2%, indicating clinically meaningful separation in the context of advanced nephrotic syndrome. Severe MCD was characterised by a markedly reduced A/G ratio (median < 0.49), whereas primary FSGS exhibited relatively higher values. This pattern suggests differential handling of globulin fractions under conditions of profound hypoalbuminaemia. One possible explanation is that in fully developed nephrotic states, compensatory increases in α2- and other globulins are more prominently retained in MCD, whereas primary FSGS may allow relatively greater globulin loss. However, this mechanistic interpretation remains inferential and warrants further investigation.
3.4. Correlation Analysis: The Regulation of Hepatic Response
We examined the association between relative albumin fraction and α2-globulin fraction using Spearman’s rank correlation to characterise the consistency of the compensatory response of the liver across disease subtypes (Figure 3).
MCD demonstrated a very strong inverse correlation (ρ = −0.86, p < 0.001) (Figure 3B), indicating a tightly coupled relationship between albumin depletion and α2-globulin elevation. This pattern suggests a highly consistent compensatory response in severe nephrotic states associated with MCD. Primary FSGS similarly exhibited a strong inverse correlation (ρ = −0.83, p < 0.001) (Figure 3C), indicating preservation of the compensatory globulin response. However, in contrast to MCD, the relative A/G ratio remained higher (Figure 1B), implying that differences in serum protein profiles are unlikely to reflect impaired hepatic synthesis. Rather, they may be attributable to differences in glomerular permeability and protein handling.
4. Discussion
Our findings indicate that SPEP reflects distinct patterns that may correlate with the specific pathomechanisms underlying different podocytopathies. By integrating clinical and electrophoretic data, two principal biological divergences emerged. First, the character of secondary FSGS protein metabolism differs significantly from that of immune-mediated podocytopathies [21]. Second, within immune-mediated forms, differences between MCD and primary FSGS become evident primarily in the setting of severe nephrotic syndrome, where the A/G ratio captures differences in the preserved glomerular size-selectivity of MCD versus the non-selective protein loss of primary FSGS.
4.1. Secondary FSGS: A Distinct Metabolic Pattern
The A/G ratio demonstrated excellent performance for identifying secondary FSGS (AUC > 0.98; Figure 2B,C). In this group, relative preservation of the A/G ratio suggests the absence of the pronounced electrophoretic alterations observed in immune-mediated podocytopathies [22,23].
Correlation analysis further supported this distinction. Whereas immune-mediated forms exhibited a strong inverse association between albumin and α2-globulin fractions (ρ > 0.8), secondary FSGS showed a comparatively weaker relationship (ρ = 0.57; Figure 3D). This pattern is consistent with the concept that proteinuria in secondary FSGS, which often arises from adaptive or haemodynamic mechanisms, may not provoke the same degree of hepatic compensatory response seen in classical nephrotic states [24].
Importantly, this interpretation remains inferential and reflects associations observed in serum protein fractions rather than direct measurement of hepatic synthesis rates.
4.2. Severity-Dependent Discrimination: A Threshold Phenomenon
A central observation of our study is that discrimination between MCD and primary FSGS became clinically meaningful only within the severe subgroup (relative albumin fraction < 40%) [25]. This suggests that the systemic response to hypoalbuminaemia may not be linear across the entire disease spectrum [26].
One plausible explanation is a threshold phenomenon, whereby substantial reductions in plasma oncotic pressure are necessary to trigger maximal compensatory protein synthesis [27]. Inclusion of patients with milder disease activity may therefore dilute detectable differences in electrophoretic profiles [28].
The pathophysiological basis for this effect may relate to qualitative differences in proteinuria [7,29]. According to the Van’t Hoff principle, colloid oncotic pressure depends on particle number rather than mass concentration [30]. Because albumin (≈67 kDa) contributes more substantially to osmotic pressure per gram than larger globulins (e.g., IgG ≈ 150 kDa), highly selective albumin loss—as typically observed in MCD—may result in a more pronounced reduction in oncotic pressure per unit of proteinuria [31]. In contrast, the non-selective proteinuria of FSGS includes a significant fraction of higher molecular weight proteins (e.g., IgG) that exert comparatively lower osmotic influence per gram [32].
Under conditions of severe oncotic pressure reduction, these qualitative differences in protein loss may translate into distinct alterations in serum protein homeostasis [33]. In MCD, preserved size-selectivity of the glomerular barrier may favour retention of newly synthesised high-molecular-weight proteins, resulting in a pronounced decrease in the A/G ratio [34]. In primary FSGS, relative non-selectivity may permit partial loss of these larger proteins, attenuating their accumulation in serum [35].
These mechanisms remain hypothetical but are consistent with the observed restriction of diagnostic discrimination to the severe subgroup (Figure 2D).
4.3. Clinical Implications: A Practical Electrophoretic Signal
From a clinical perspective, two practical implications emerge. First, an A/G ratio > 1.0 strongly favours secondary FSGS over immune-mediated podocytopathies (Figure 2B,C). Second, in patients with severe nephrotic syndrome, a relatively preserved A/G ratio (>0.5) may indicate non-selective glomerular injury consistent with primary FSGS (Figure 2D). In such cases, careful histopathological evaluation—including examination of additional biopsy sections—may be warranted to avoid misclassification as MCD [36].
Importantly, these observations should be interpreted as adjunctive, not definitive, diagnostic indicators and require external validation.
5. Conclusions
Our findings demonstrate that serum protein electrophoresis provides clinically meaningful information in the evaluation of podocytopathies (Figure 4).
The A/G ratio shows strong discriminatory capacity for identifying secondary FSGS, where values > 1.0 strongly argue against immune-mediated disease. Within the context of severe nephrotic syndrome, a markedly reduced A/G ratio (<0.49) characterises MCD and reflects distinct differences in serum protein homeostasis compared with primary FSGS. These findings suggest that differences in glomerular selectivity contribute to divergent electrophoretic patterns once colloid oncotic pressure falls below a critical threshold.
Overall, the integration of the A/G ratio—as a simple, widely available biomarker—into clinical assessment may refine pre-biopsy probability estimates and support more targeted diagnostic strategies. Our results underscore that nephrotic syndrome is shaped not only by the magnitude of protein loss but also by its composition and the subsequent compensatory response. Further studies are required to validate these observations in independent cohorts and to elucidate the underlying mechanistic pathways.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sim J.J. Batech M. Hever A. Harrison T.N. Avelar T. Kanter M.H. Jacobsen S.J. Distribution of Biopsy-Proven Presumed Primary Glomerulonephropathies in 2000–2011 Among a Racially and Ethnically Diverse US Population Am. J. Kidney Dis.20166853354410.1053/j.ajkd.2016.03.41627138468 · doi ↗ · pubmed ↗
- 2D’Agati V.D. Kaskel F.J. Falk R.J. Focal Segmental Glomerulosclerosis N. Engl. J. Med.20113652398241110.1056/NEJ Mra 110655622187987 · doi ↗ · pubmed ↗
- 3Maas R.J. Deegens J.K. Smeets B. Moeller M.J. Wetzels J.F. Minimal Change Disease and Idiopathic FSGS: Manifestations of the Same Disease Nat. Rev. Nephrol.20161276877610.1038/nrneph.2016.14727748392 · doi ↗ · pubmed ↗
- 4D’Agati V.D. The Spectrum of Focal Segmental Glomerulosclerosis: New Insights Curr. Opin. Nephrol. Hypertens.20081727128110.1097/mnh.0b 013e 3282 f 94a 9618408478 · doi ↗ · pubmed ↗
- 5Wiggins R.C. The Spectrum of Podocytopathies: A Unifying View of Glomerular Diseases Kidney Int.2007711205121410.1038/sj.ki.500222217410103 · doi ↗ · pubmed ↗
- 6Kriz W. Lemley K.V. A Potential Role for Mechanical Forces in the Detachment of Podocytes and the Progression of CKDJ. Am. Soc. Nephrol.20152625826910.1681/ASN.201403027825060060 PMC 4310663 · doi ↗ · pubmed ↗
- 7Bazzi C. Petrini C. Rizza V. Arrigo G. D’Amico G. A Modern Approach to Selectivity of Proteinuria and Tubulointerstitial Damage in Nephrotic Syndrome Kidney Int.2000581732174110.1046/j.1523-1755.2000.00334.x 11012907 · doi ↗ · pubmed ↗
- 8Corwin H.L. Schwartz M.M. Lewis E.J. The Importance of Sample Size in the Interpretation of the Renal Biopsy Am. J. Nephrol.19888858910.1159/0001675633394725 · doi ↗ · pubmed ↗