A Systematic Review on Amnion as a Cell Delivery Scaffolding Material for Cartilage Regeneration in Pre-Clinical and Clinical Studies
Shu-Yong Liow, Sik-Loo Tan, Alvin Jiunn-Hieng Lu, Kwong Weng Loh, Seow Hui Teo, Chan Young Lee, Le Wan, Azlina Amir Abbas, Kyung-Soon Park

TL;DR
This review shows that amnion is a safe and effective scaffold for cartilage regeneration in both lab and clinical studies.
Contribution
The study systematically evaluates amnion's efficacy as a scaffold for cartilage repair across preclinical and clinical settings.
Findings
Amnion scaffolds improve cell attachment, viability, and cartilage-related marker expression in vitro.
In vivo studies show better cartilage integration and collagen production with amnion treatment.
Clinical outcomes indicate improved knee function and reduced pain in patients using amnion-based therapies.
Abstract
Cartilage is an important yet vulnerable tissue with limited self-healing capacity, where damage often progresses to joint degeneration, which eventually leads to severe osteoarthritis (OA). Current tissue engineering strategies focus on biocompatible scaffolds for cartilage regeneration, particularly amnion (or amniotic membrane), emerging as a promising biomaterial due to its wide availability, low immunogenicity, and naturally derived microenvironment that is advantageous for cartilage regeneration. This systematic review aims to evaluate the existing evidence on the efficacy of amnion as a tissue scaffolding material for cartilage regeneration in both preclinical and clinical studies. Using terms such as “cartilage damage”, “cartilage injuries”, “amnion” and “amniotic membrane”, 19 relevant studies were identified across three major databases (PubMed, Scopus and Web of Science)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
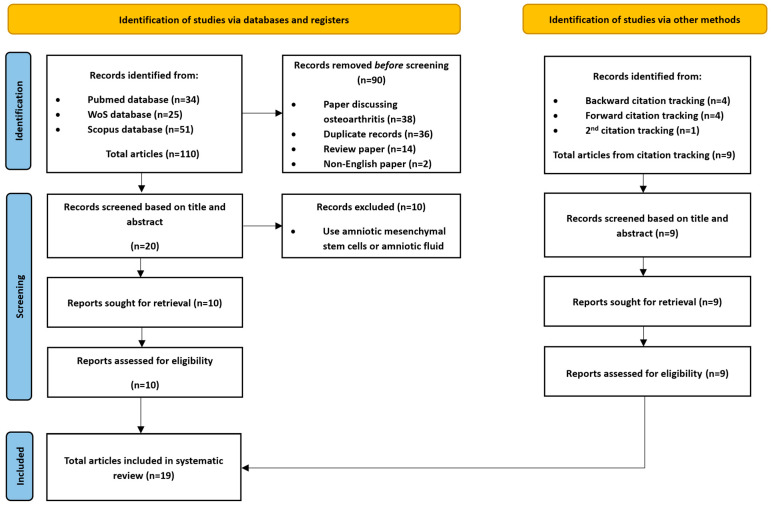 Figure 1
Figure 1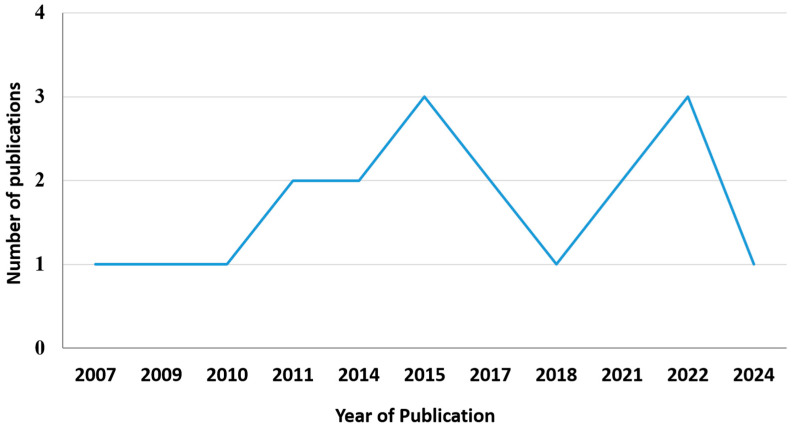 Figure 2
Figure 2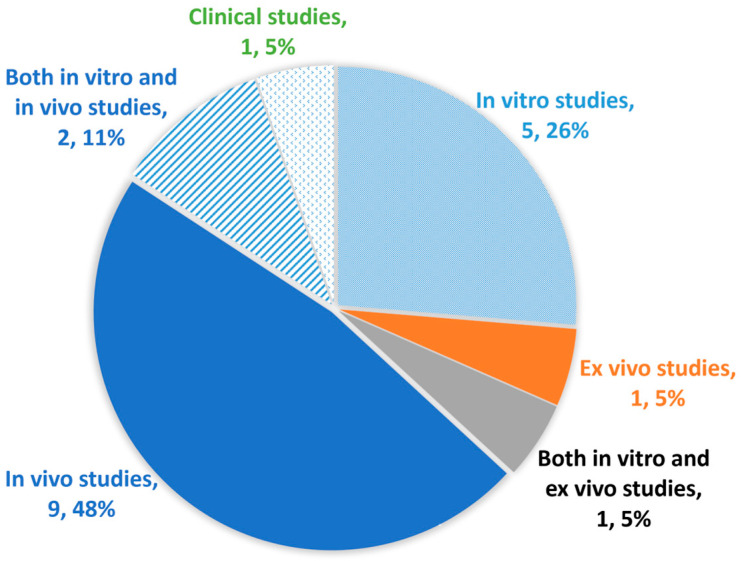 Figure 3
Figure 3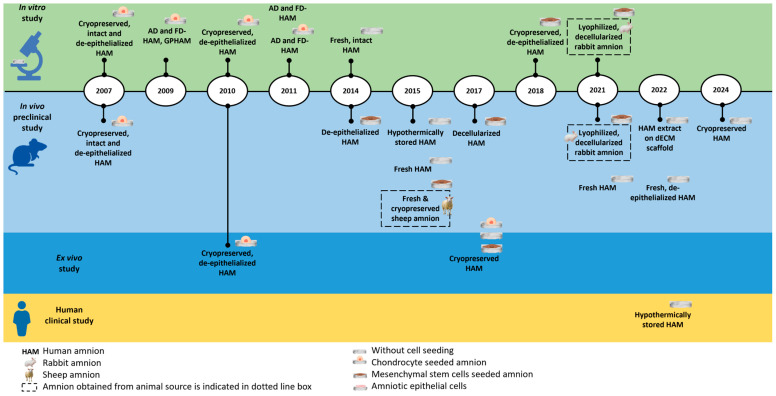 Figure 4
Figure 4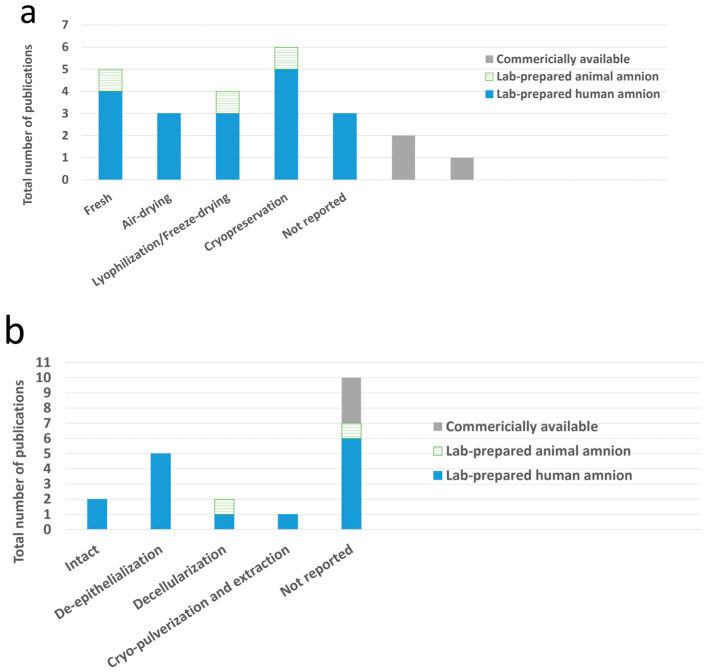 Figure 5
Figure 5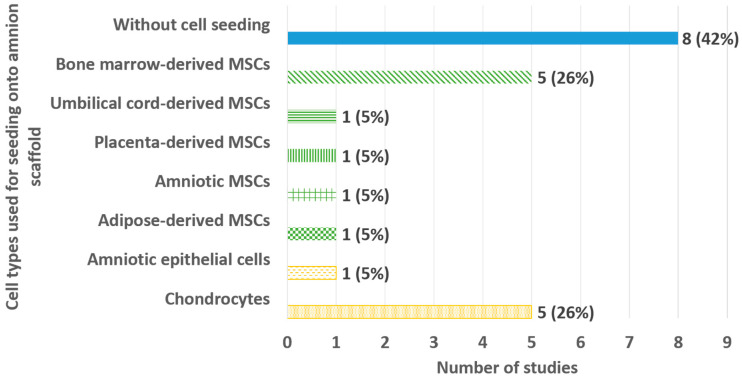 Figure 6
Figure 6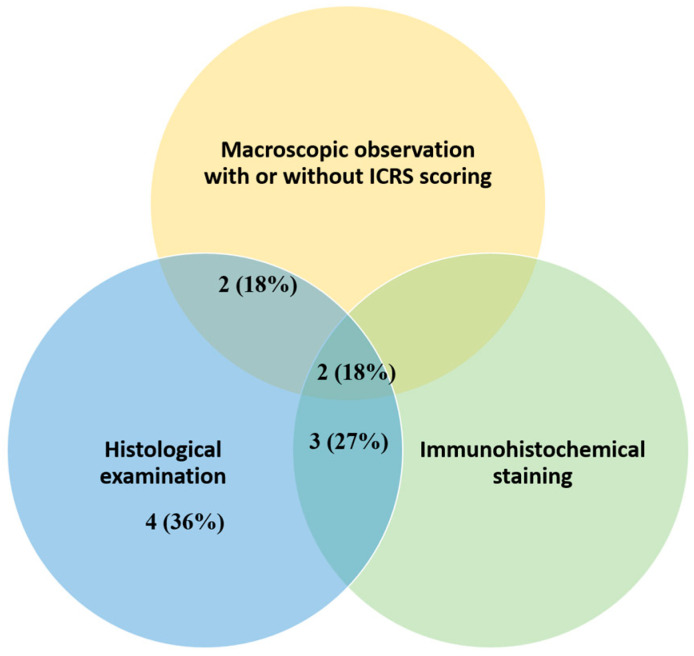 Figure 7
Figure 7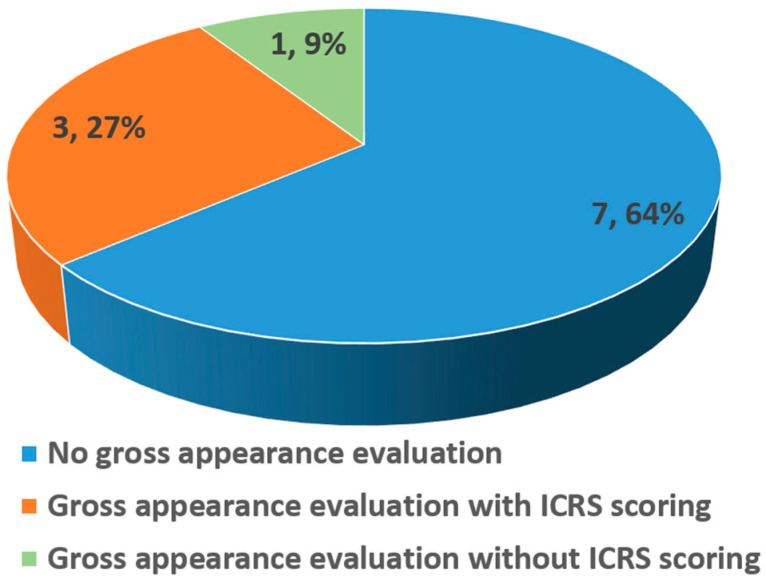 Figure 8
Figure 8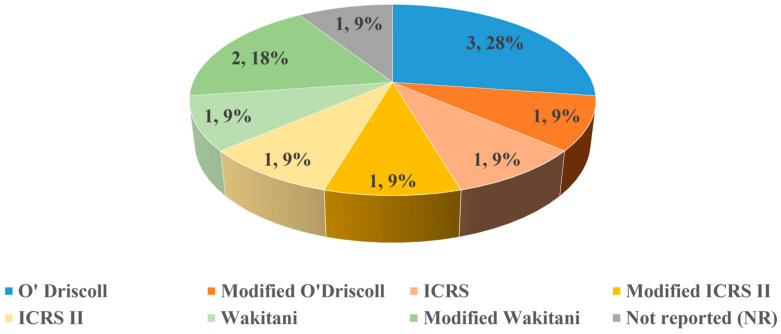 Figure 9
Figure 9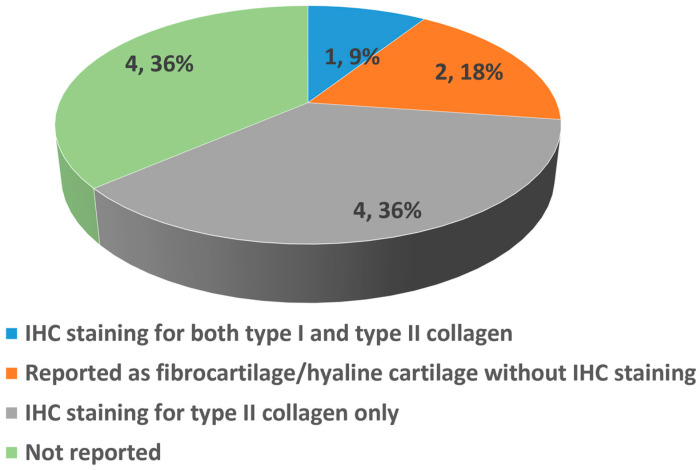 Figure 10
Figure 10- —Ministry of Higher Education Malaysia via Prototype Research Grant Scheme
- —UM International Collaboration Grant—2023 SATU Joint Research Scheme Program
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCorneal Surgery and Treatments · Osteoarthritis Treatment and Mechanisms · Mesenchymal stem cell research
1. Introduction
Cartilage is a type of resilient connective tissue that plays an important role in facilitating flexible movement by functioning as a cushion and lubricant between the joints. While cartilage injury may not be immediately life-threatening, it can significantly reduce quality of life by causing pain, stiffness and functional deficits [1]. Focal cartilage injuries are commonly caused by acute traumatic impacts or repeated microinjuries over time and can occur at any age. These injuries can extend to different layers of the joint, including partial- and full-thickness cartilage injuries that involve only the cartilage layer, as well as osteochondral injuries that also involve the underlying subchondral bone [2,3]. The avascular and aneural nature of cartilage and low cell chondrocyte density limit its self-healing capacity. Any form of cartilage injury can predispose individuals to progressive joint degeneration and ultimately lead to osteoarthritis (OA), a more severe condition that affects the entire joint [4,5].
Many approaches have been established to treat cartilage injuries. These include palliative treatments that primarily aim to alleviate symptoms, as well as surgical techniques designed to achieve cartilage repair through bone marrow stimulation or regenerative modalities. Bone marrow stimulation techniques, such as microfracture, allow the infiltration of bone marrow stem cells into the injured site but typically result in fibrocartilage formation, which is less durable than native hyaline cartilage. Meanwhile, existing regenerative modalities, such as osteochondral graft transplantation and autologous chondrocyte implantation, also encounter issues, including limited graft availability and the risk of graft failure [6,7,8]. These limitations have highlighted the need to introduce more advanced tissue engineering strategies for effective cartilage regeneration. Tissue engineering is a complex field that utilizes a combination of cells, scaffold materials, and growth factors to repair and restore the structure and functionality of tissues [9,10,11]. Scaffolds derived from natural or synthetic biomaterials provide a supportive framework for cell attachment and development and facilitate the integration of newly generated tissue with the host [12,13].
Since the amnion (or amniotic membrane) was first introduced for skin transplantation in 1910, its use has significantly expanded to various medical fields, including orthopedics. This growth is largely attributed to its unique biological and mechanical properties [14]. In terms of biological properties, amnion exhibits immunosuppressive, antifibrotic, antimicrobial and anti-inflammatory effects, which are desirable features for transplantation [15,16]. Regarding biomechanical properties, amnion possesses flexibility, rigidity, and tensile strength. Together with its extracellular matrix (ECM), which mimics the native environment for cartilage regeneration, these features make the amnion an ideal scaffold, offering high immune tolerance, minimal complications, and effective cartilage tissue regeneration [17,18].
Despite these promising characteristics, the application of amnion as a tissue engineering scaffold is comparatively well established in other fields such as wound healing and ophthalmology. Although there is growing interest in the amnion for cartilage regeneration, there are currently no comprehensive systematic reviews that consolidate reported outcomes across all preclinical (in vitro, in vivo, and ex vivo) and clinical studies covering the broad spectrum of cartilage injuries. Therefore, this systematic review aims to evaluate the existing evidence on the efficacy of amnion as a tissue scaffolding material for cartilage regeneration in both preclinical and clinical studies, to guide future research directions and facilitate clinical translation. In this review, the preclinical studies, both in vitro and ex vivo, showed evidence of the amnion as a biomaterial that supports chondrocyte proliferation and sustains chondrocyte phenotypic expression and chondrogenic differentiation in multipotent mesenchymal stem cells (MSCs).
In the in vivo preclinical models, both leporine (rabbits) and ovine (sheep) models showed hyaline cartilage-like tissue formation at the repaired site post-treatment with amnion-derived biomaterials, either with or without cells seeded onto the amnion. One clinical study used the commercially available hypothermically stored amnion (HSAM) to treat chondral lesions with International Cartilage Repair Society (ICRS) grade 3 or grade 4A (of the femur). It reported improved KOOS Sports and Recreation and Quality of Life (QoL) scores, in addition to improvements in VAS Average Pain and Maximum Pain scores, at 24 months compared to baseline. The Modified Magnetic Resonance Observation of Cartilage Repair Tissue (MOCART) scoring based on MRI scans showed that 7 of 10 subjects had complete defect repair and filling by 24 months. Three out of the 10 enrolled subjects reported at least one mild to moderate adverse event, though none were related to the use of amnion. This systematic review summarized the current evidence supporting the efficacy of amnion as a tissue scaffolding material for cartilage regeneration.
2. Materials and Methods
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [19]. The study protocol was prospectively registered in the PROSPERO database under the ID 1178444. The complete PRISMA 2020 checklist has been provided to the editorial office as part of the submission documentation.
2.1. Search Strategy
We conducted a systematic search for research articles published over the last 25 years (from January 2000 to December 2025; up to 25 December 2025) across three primary databases: PubMed, Web of Science, and Scopus. The search was conducted using selected keywords (i.e., “cartilage damage”, “cartilage injuries”, “amnion” and “amniotic membrane”), combined with Boolean operators to identify articles with relevant titles, abstracts or keywords. The specific search strategies applied for each database are shown in Table A1. All non-redundant search outputs from all the databases (with their titles and abstracts) were uploaded to the Abstrackr for the screening process. All records were independently screened by two reviewers (S.-Y.L. and A.J.-H.L.) using Abstrackr, followed by full-text assessment. Conflicts that arose among the two reviewers were addressed through team discussion and full-text assessment until a consensus was reached. The articles included from the Abstrackr screening process were also re-evaluated together in a team discussion to ensure the finalized list of the included articles met all the inclusion/exclusion criteria. Subsequently, the reference lists of the included articles were manually screened to identify any additional relevant studies.
2.2. Selection (Eligibility) Criteria
All preclinical (in vitro, ex vivo, and in vivo) and clinical studies on the application of any form of amnion as scaffolds for cartilage regeneration were included. This encompasses the use of amnion alone, amnion–chorion composites, or amnion combined with other biomaterials, while studies utilizing the chorion layer alone were excluded. Studies involving only the utilization of cells derived from amnion were also excluded. Only research articles published in English were selected. The detailed inclusion and exclusion criteria were listed in Table 1.
This current review focused on focal cartilage defects, and OA is regarded as an exclusion criterion. It is important to differentiate between these two conditions, as both involve cartilage injury but differ in pathology and relevance to the review. Focal traumatic defects typically occur locally within a relatively healthy joint, allowing for a controlled assessment of scaffold-based treatment. On the other hand, OA is a systemic joint disease characterized by chronic pro-inflammatory conditions with elevated catabolic cytokines that affect the whole joint. This environment might impair healing and diminish the effects of the amnion on tissue regeneration [20]. Thus, the exclusion of OA models is essential to avoid the confounding effects on the scaffold performance and ensure the validity of our findings regarding amnion’s efficacy for localized cartilage regeneration.
2.3. Data Collection
To harmonize the terminology used in different articles, the term “amnion” is used to collectively describe the “amnion scaffold”, “amniotic membrane”, “acellular amniotic membrane”, and “HAM” reported in the different studies. The term ‘amnion” covers multiple preservation/processing methods, where the preservation/processing methods will be added as a prefix to differentiate the “amnion” preserved/processed by different methods, e.g., “glycerol-preserved amnion” was used to describe the “amnion” preserved in glycerol; “air-dried amnion” was used to describe amnion processed by the air-drying method. The term “fresh amnion” is used to describe any “amnion” used in the studies without any preservation. The term “intact” is used to describe “amnion” without decellularization/de-epithelialization processing.
Data were extracted from the included articles using a standardized Excel spreadsheet by the first reviewer and checked by the second reviewer to ensure accuracy. General data extraction focused on: the details of the articles (e.g., author, article title, journal, year of publication and aim of study), amnion sources, procurement criteria and amnion preparation methods; types of cell/composites applied on the amnion; and animal species, defect models and dimensions. For in vitro studies, the findings for the chondrogenic marker expression profiles were tabulated in the data charting spreadsheet. For ex vivo and in vivo studies, data extracted to the spreadsheets include the gross observations (with and without ICRS scores), histological examinations (with and without scoring) and immunohistochemical (IHC) staining for hyaline cartilage-related markers. In addition, patient-reported outcome measures such as the Knee Injury and Osteoarthritis Outcome Score (KOOS) and the Visual Analogue Scale (VAS) scores were extracted from the included clinical study. Studies lacking reported results for a specific section in the spreadsheets were marked as “Not Reported” or “NR”.
Meta-analysis was not performed due to the considerable heterogeneity observed in the study methodologies, including variations in amnion preparation techniques, the animal models employed, the types of defects created, and the cell types seeded. Furthermore, standardized quantitative outcome measures were lacking for synthesizing the data for further statistical comparisons. Therefore, qualitative synthesis of the evidence was conducted in this systematic review.
3. Results
3.1. Selection of Sources of Evidence
A total of 110 records were retrieved from all databases. During the initial screening stage, prior to title and abstract screening, all non-English papers, review articles, and duplicates were removed manually (using EndNote Citation Manager). Of the 90 articles excluded at this stage, half were related to OA. A total of 20 articles proceeded to the title and abstract screening in the Abstrackr. The reviewers reached an initial agreement of 85% (17/20; Table A2). After conflicts were resolved, only ten articles (out of the 20 articles) met all the inclusion/exclusion criteria and proceeded for full-text review. Most excluded articles were articles reporting on the use of amnion-derived stem cells and amniotic fluid rather than the amnion itself.
Subsequently, manual citation tracking was performed to identify any additional relevant records that might have been missed during the keyword searches. A total of nine additional studies were included from citation tracking. Ultimately, 19 articles were included in this systematic review (Figure 1). All these 19 articles reported on using amnion alone, and none of these studies used amnion/chorion in their studies.
3.2. Characteristics of Source of Evidence
This systematic review included a total of 19 articles published between 2007 and 2024. During the screening process, 10 studies were excluded for the following reasons: utilization of amnion-derived mesenchymal stem cells (AMSCs) on scaffolds without amnion (n = 4); use of AMSCs as the scaffolding materials instead of amnion (n = 3); use of amniotic fluid (n = 1); application of whole decellularized placenta rather than the isolated amnion membrane (n = 1); and the application of amnion membrane extract in culture medium instead of acting as a scaffold (n = 1). All excluded studies are listed in Table A3. Two articles reporting on cartilage ex vivo models [21,22] were reviewed, with a conflict between the two reviewers as the studies used osteoarthritic cartilage samples. The final decision made after discussion was to include these two articles because both aimed to evaluate the amnion as a scaffold for cartilage repair, utilizing osteoarthritic cartilage tissue samples as an ex vivo cartilage injury model rather than as an ex vivo OA model. The details of all 19 included articles are summarized in Table 2.
The risk of bias for the included studies was assessed using the Office of Health and Translation (OHAT) risk of bias tool for preclinical studies and the Methodological Index for Non-Randomized Studies (MINORS) tool for the clinical study. Detailed individual assessments are provided in Table A4 (OHAT) and Table A5 (MINORS).
Overall, the total number of publications on the use of amnion as a scaffold for cartilage regeneration has remained relatively low but constant over the years, ranging from one to three publications per year (Figure 2). This indicates sustained interest in this research field. Among these studies, five were in vitro, one was ex vivo, and nine were in vivo (Figure 3). Additionally, one study combined both in vitro and ex vivo models, while two studies combined both in vitro and in vivo experiments. Only one clinical study was identified in this review. This highlights that current research is predominantly at the preclinical level, underscoring the need for further clinical investigations to establish its therapeutic feasibility. The summary for the publication timeline of all 19 articles is shown in Figure 4.
3.3. Source and Processing Techniques of Amnion
The systematic review included studies that utilized human amnion (HAM) as the primary source for cartilage regeneration scaffolds, with 89% (17/19) of the studies employing human-derived amnion. The amnion was typically obtained from healthy women undergoing caesarean sections and screened for infectious diseases, particularly blood-borne diseases, including human immunodeficiency virus (HIV), Hepatitis B virus (HBV), Hepatitis C virus (HCV), and syphilis (Table 3). In addition to human-derived amnion, one study used amnion sourced from rabbits [29] and another from sheep [31].
Preservation methods for the amnion varied among the selected studies (Figure 5a), encompassing fresh, air-dried, lyophilized (freeze-dried), and cryopreserved amnions. Five studies utilized fresh amnion, six used cryopreserved, three used air-dried and four used freeze-dried. Notably, some studies employed commercially available products, including glycerol-preserved human amnion (GPHAM) [23] and hypothermically stored amnion (HSAM) [33,39]; however, three studies did not specify a preservation method. Regarding processing methods (Figure 5b), four major techniques were identified: utilization of intact amnion, de-epithelialization, decellularization and cryo-pulverization, followed by extraction. The most frequently used technique was de-epithelialization (n = 5), followed by decellularization (n = 2), and used in its intact state (n = 2). One study utilized amnion extract obtained via cryo-pulverization, incorporated with a decellularized osteochondral ECM scaffold [36]. Ten studies did not specify the processing methods.
Cell seeding strategies were employed in 11 out of 19 studies (58%) to promote chondrogenic differentiation and tissue regenerative potential of the amnion scaffolds (Figure 6). The most commonly seeded cells were bone marrow-derived mesenchymal stem cells (BMSCs) and chondrocytes (n = 5 for each, Figure 6). Other cell types utilized in the studies included umbilical cord-derived mesenchymal stem cells (UMSCs), placenta-derived mesenchymal stem cells (PMSCs), amnion-derived stem cells (AMSCs), adipose-derived mesenchymal stem cells (ADSCs) and amniotic epithelial cells (AECs) (n = 1 for each).
3.4. Effects of Amnion Scaffolds in Enhancing Chondrocytes and Chondrogenic MSCs Proliferation and Phenotypic Expressions In Vitro
The articles reported on in vitro studies on amnion are summarized in Table 4. Most of the preclinical in vitro studies showed that amnion scaffolds supported cell attachment, proliferation, and chondrogenic differentiation of various cell types, including chondrocytes, bone marrow-derived mesenchymal stem cells (BMSCs), PMSCs, UMSCs and ADSCs.
Among all in vitro studies, there is only one study that did not apply cell seeding. Lindenmair et al. [26] examined the chondrogenic potential of the amnion with its native cells in different media; they found that amnion in chondrogenic media (with or without FGF) consistently showed positive effects on GAG/viability, type II collagen (COL-II) content, and cartilage-related gene expression. Boo et al. [23] found that chondrocytes proliferated on all amnion scaffold types; however, commercially available glycerol-preserved human amnion showed higher cell attachment stability compared to air-dried or freeze-dried forms. Krishnamurithy et al. [24] reported overall superior effects of amnion over monolayer culture, noting that the cell proliferation and GAG content in both air-dried (AD HAM) and freeze-dried (FD HAM) membranes were significantly higher than in monolayer culture.
Tan et al. [25] reported cell attachment on both AD and FD HAM and statistically significant increases in GAG expression in rabbit BMSCs seeded on amnion scaffolds versus monolayer controls. Naseer et al. [27] demonstrated that treated cells seeded on both HAM and plastic surfaces yielded better results compared to control cells in terms of proteoglycan and aggrecan contents and COL-II expression. Díaz-Prado et al. [22] found that the basement membrane of the amnion was a superior surface for chondrocyte seeding and differentiation compared to the epithelial side, indicated by better growth of chondrocytes and the presence of COL-II on the basement layer.
Jin et al. [28] observed high chondrocyte attachment and viability across multiple human amnion substrates, with immunohistochemistry detecting COL-II primarily in the group where the chondrocyte was seeded on the de-epithelialized stromal side. Finally, Cao et al. [29] demonstrated that the combination of an amnion scaffold, platelet-rich plasma (PRP) and ADSCs resulted in the highest levels of cell proliferation, viability, chondrogenic gene and protein expression, and COL-II production.
3.5. Application of Amnion Scaffolds in Ex Vivo Model
Two ex vivo studies (Table 5) were included in this review [21,22]. Both studies collected cartilage biopsies from healthy donors and patients with OA, which were sectioned into 6 mm diameter cartilage discs to examine the effects of amnion on cartilage repair. Notably, there were distinct differences in the model preparation between these two studies. While Muinos-Lopez et al. [21] created 2 mm diameter defects in the cartilage prior to amnion treatment, Díaz-Prado et al. [22] applied the amnion scaffolds directly onto a 6 mm cartilage disc without any defect creation.
Muinos-Lopez et al. [21] reported that HAM seeded with various cell types (including chondrocytes, hBMSCs, hACEs, and hAMSCs) showed no significant differences in the ICRS histological scores across the groups. Nevertheless, based on the Masson Trichrome-stained histopathology analysis, chondrocyte-seeded HAM-treated cartilage disc showed enhanced tissue integration compared to the other groups; the hAMSCs-seeded HAM-treated group exhibited a high abundance of COL-II expression in the IHC analysis. In the ex vivo study without defect creation on the cartilage discs, Díaz-Prado et al. [22] reported that only the chondrocyte-seeded HAM group observed new tissue formation on the cartilage disc compared to the HAM-only control-cartilage disc group; the new cartilage tissue formation was characterized by the presence of COL-II and the absence of type I collagen (COL-I) in IHC analysis, as well as mild proteoglycan expression, as indicated by Safranin-O (SO)-stained histopathology analysis.
3.6. In Vivo Application of Amnion Scaffolds in Different Animal Models and Cartilage Defect Characteristics
Among the 11 articles reporting on the in vivo cartilage defect models, eight studies (73%) used rabbit models, while the other three (27%) used sheep models. Scaffold retention issues were reported in two studies utilizing sheep models [32,33], in which both studies reported that 50% of the sheep failed to retain the amnion scaffold due to a lack of immobilization.
Defect models were generally classified by depth into three types (Table 5): partial-thickness defects (n = 1, 9%), full-thickness defects (n = 3, 27%), and osteochondral defects (n = 3, 27%); however, defect types were not specified in four studies (n = 4, 36%). Defects were predominantly created in the femoral groove, also known as the patella groove or trochlear groove (n = 5, 45%), followed by the lateral femoral condyle (n = 2, 18%) and the medial femoral condyle (n = 2, 18%, Table 5). One study [37] examined laryngeal cartilage defects at the thyroid lamina, while another study did not specify the defect location (Table 5).
There was an apparent inconsistency in the reporting of defect dimensions in the in vivo preclinical models (Table 6). For instance, some studies reported diameter only (n = 2, [28,37]), depth only (n = 1, [38]), width × length (n = 2, [31,34]), or diameter × depth (n = 3, [30,35,36]), with the dimension ranging from 3 to 7 mm (Table 6). In addition, in some studies, the cartilage defects were reported by area [33]. One study each from the rabbit and sheep models did not report the defect dimensions.
3.7. Assessment of Cartilage Regeneration Outcomes in In Vivo Studies Using Amnion
Among the in vivo studies reported in the selected articles, three main evaluation methods were used to assess the efficacy of amnion for cartilage repair in (Figure 7). All reported studies utilized histological analysis to evaluate the new cartilage formed at the study endpoint.
Macroscopic evaluation was reported in four of 11 in vivo studies (Figure 8, Table 7), with three studies reporting gross results guided by the ICRS scoring system and one reporting gross examination without a scoring system. Typically, ICRS macroscopic assessment covers the area and morphology of the newly formed tissue, as well as its integration with the surrounding native tissues [40]. An increase in the ICRS macroscopic score indicates enhanced outcome of cartilage repair [41]. All studies reporting ICRS macroscopic evaluation demonstrated superior results in the amnion-treated groups [31,35,36]. Studies by Jun et al. [35] and Rastegar Adib et al. [36] reported that the amnion-treated groups (HAAM + JCFs and dECM + amnion extract (AME), respectively) achieved the highest ICRS scores, indicating the best apparent repair, compared to the control group and other treatment groups. This is concordant with the findings where the defect area was completely covered by newly formed tissue that integrated well and appeared similar to the native cartilage tissue [35,36]. In another study by Liu et al. [30], although the study did not evaluate the cartilage repair using the ICRS scoring system, the repair outcome was reported in terms of morphology and integration of the regenerated tissue in the femoral condyle defect. Both HAAM groups (with or without cell seeding with BMSCs) showed new tissue formation; however, the tissue formed in the HAAM + BMSCs group exhibited a more favorable quality compared to the HAAM only group. Specifically, a smooth and surrounding color-matched tissue with good integration was observed in the HAAM-BMSCs group, while a fibrous and less smooth surface was observed in the regenerated tissue from the HAAM-only group. A study by Garcia et al. [31] presented only the final grading of the newly generated tissue. Consistently, all amnion-treated groups showed a grade II “nearly normal” cartilage tissue formation, based on the ICRS macroscopic evaluation, while the control group without any treatment showed a grade III “abnormal” cartilage tissue in the repaired lateral femoral condyle.
Histological assessment was performed in all 11 in vivo studies. Three (3/11, 28%) utilized the O’Driscoll scoring system, while the remaining studies employed a variety of scales, including modified O’Driscoll scoring system (1/11, 9%), modified ICRS II (1/11, 9%), ICRS II (1/11, 9%), ICRS (1/11, 9%), Wakitani (1/11, 9%), and modified Wakitani (2/11, 18%) scoring systems (Figure 9). Additionally, one study (1/11, 9%) reported histological findings based solely on histopathological staining analysis without applying any scoring system [36]. The predominant histological stains used included Haematoxylin and Eosin (H&E), Safranin-O, Toluidine Blue and Masson Trichrome staining, which helped to characterize the quality and composition of the newly formed cartilage tissue. In addition, for the two ex vivo studies, one reported with ICRS scoring, and one without any scoring system.
In most of the scoring systems, specifically ICRS, ICRS II and O’Driscoll (or their respective modified scoring system), a higher score represents superior tissue quality [41,42,43]. Across these assessment systems, the amnion-treated groups consistently achieved higher scores than the control groups. For instance, a study by Turgut et al. [34], utilizing the modified O’Driscoll scoring system, found that HAM groups consistently achieved higher scores than the untreated control group at both the 4th and 8th week post-treatment. Similarly, Garcia et al. [31] reported that all amnion-treated groups had significantly higher O’Driscoll scores than the untreated control group. Both Tabet et al. [32] and Tabet et al. [33] reported descriptive observations, and they consistently reported that defects treated with amnion were filled with cells resembling hyaline cartilage, in contrast to the untreated control that only showed minimal repair (<10%) or a complete lack of cartilage formation.
Regarding the ICRS II scoring system, Jun et al. [35] observed that the HAAM + JCFs group achieved the highest score among all experimental and control groups. In a study using a modified ICRS II scoring system, Iravani et al. [37] found that the combination of amnion and collagen resulted in significantly better cell morphology and lacuna formation, alongside lower inflammation scores, compared to the untreated control group at both 45- and 90-day post-treatment. While this combination did not differ significantly from the collagen-only scaffold, the HAAM-COL-II composite showed superior cell morphology at day 45 post-treatment. Furthermore, Jin et al. [28] reported that the DHS (denuded HAM with cell seeded on stromal side) group had the highest ICRS score, indicated by complete filling with hyaline cartilage-like tissue, whereas the denuded HAM without cell seeding group showed only partial filling, and the untreated group developed fibrocartilage in the defect created at the patella groove.
Conversely, the Wakitani and modified Wakitani scoring systems utilize a scale where a lower score indicates better tissue regeneration [44]. Cao et al. [29] reported that the ADSCs + AM + PRP group achieved a significantly lower Wakitani score (indicating better cartilage regeneration) compared to all other groups (ADSCs + AM + PRP < ADSCs + AM < ADSCs + PRP < ADSCs). In addition, Liu et al. [30] observed hyaline cartilage formation in the HAAM + BMSCs group, while the HAAM-only group formed scattered chondrocyte-like cells in the repaired femoral condyle, and the untreated control group showed no new cartilage formation. In contrast, Zhang et al. [38] reported that the HAAM-only group had a significantly higher score compared to the HAAM + rBMSCs and the non-defect (normal cartilage) control.
Last but not least, Rastegar Adib et al. [36] reported the repair outcomes without using a scoring system, reporting that the dECM + AME resulted in the most effective cartilage and subchondral bone regeneration. This was evidenced by mature hyaline cartilage stained with intense SO and TB. These findings collectively suggest that the amnion provides a favorable environment for the synthesis of a hyaline-like ECM at the repaired site.
IHC analysis was conducted in five out of 11 studies (Figure 10). These studies consistently reported positive results or higher expression of COL-II in the amnion-treated groups compared to other treatment groups. A study by Liu et al. [30] reported that the HAAM + BMSCs group showed positive results for COL-II staining. The studies by Jun et al. [35] and Zhang et al. [38] demonstrated that HAAM utilized with composite or seeded with cells (HAAM + JCFs and HAAM + BMSCs respectively) resulted in a higher content of COL-II compared to the HAAM only and untreated control groups. Additionally, a study by Tabet et al. [33] showed that COL-II was explicitly present in the defects treated with HSAM, whereas it was absent in the untreated control group.
While COL-II is an indicator of high-quality regenerated tissue that represents hyaline cartilage, COL-I commonly serves as a marker for fibrocartilage. Fibrocartilage formation is generally considered an inferior outcome in hyaline cartilage repair. This biological principle is consistent with findings reported across the various anatomical sites included in this review, ranging from the knee articular cartilage examined in most studies (10 out of 11) to the laryngeal cartilage repair investigated using the lamina model [37]. However, one study reported a significantly high expression of both COL-I and COL-II in the amnion-treated cartilage (with the staining intensities highest in the ADSC + AM + PRP group, followed by the ADSC + AM group) [29].
Two studies reported their findings in terms of specific cartilage type (hyaline and fibrocartilage). Jin et al. [28] reported hyaline cartilage formation in the chondrocyte-seeded HAM group, while the untreated defect group showed fibrocartilage formation. Iravani et al. [37] reported progressive IHC evaluation at different time points. At day 45 post-treatment, control defects exhibited predominantly fibrous tissue, while both collagen-only scaffold group and amnion/collagen groups demonstrated superior fibro-hyaline cartilage formation. By day 90 post treatment, this trend had advanced further, with treatment groups achieving predominantly hyaline cartilage characteristics, in contrast to the controls, which exhibited a fibro-hyaline matrix at the repaired thyroid lamina defect. Lastly, four studies assessed neither collagen type nor cartilage type. In studies that did not specify the experimental techniques used to identify cartilage type, the amnion-treated groups generally exhibited hyaline cartilage predominance, whereas control groups exhibited fibrocartilage [28,37].
3.8. Application of Amnion Scaffolds for Cartilage Regeneration in Clinical Study
The only clinical study included in this systematic review was conducted by Tabet et al. [39], and the study details are presented in Table 8. This single-arm prospective study involved 10 patients with symptomatic knee cartilage lesions. All patients were treated with a commercially available hypothermically stored amniotic membrane (HSAM) and were monitored for a period of two years following treatment.
At the 24th month of study, all subjects showed significant improvement in KOOS Sports and Recreation and Quality of Life scores, the Marx Activity Scale and the Visual Analog Scale (VAS) for pain. Magnetic Resonance Observation of Cartilage Repair Tissue (MOCART) scoring revealed complete defect repair and filling in seven of the 10 subjects. Three subjects who voluntarily participated in additional biopsy assessments showed integration of the HSAM with native cartilage tissue, and immunohistochemistry staining demonstrated the presence of COL-II throughout the repair site. On the other hand, three subjects experienced mild to moderate treatment-emergent adverse effects (TEAEs), none of which were associated with the HSAM product.
4. Discussion
4.1. Amnion Procurement, Processing, Composites, and Cell Seeding Strategies
Among the 19 studies included in this review, the majority (n = 17) primarily utilized human amnion as the scaffold source for cartilage regeneration, typically obtained from healthy women undergoing Cesarean sections. In the studies that utilized human amnion, some reported screening donors for infectious diseases, including blood-borne pathogens, but a notable number (n = 5) did not disclose specific procurement criteria. Furthermore, some studies used commercially available human amnion products, which are indeed derived from raw human amnion tissue. Reporting procurement criteria, including donor health status and infectious disease screening, is important to ensure product quality and safety. The lack of uniform procurement criteria raises concerns about potential contamination and disease transmission, which are primary issues in tissue banking [45].
The two studies that utilized animal amnion also failed to report detailed inclusion and exclusion criteria. Procurement criteria are particularly crucial for human amnion because human donors vary significantly in health status, pregnancy conditions and infectious disease exposure. This contrasts with animal amnion procurement, which usually involves controlled laboratory animals with relatively lower biological variability and health risks. Thus, the lack of procurement criteria for animal amnion may be less critical than for human sources. However, to ensure the efficacy and safety of amnion scaffolds in future studies, it is recommended to clearly report all these criteria, regardless of whether the source is lab-prepared human amnion, a commercial amnion product, or animal amnion.
Processing methods varied among the selected studies, including air-drying, lyophilization, cryopreservation, de-epithelialization, and decellularization, as well as the use of fresh and intact amnion. These diverse techniques aim to reduce immunogenicity and improve scaffold integration; however, the absence of standardized protocols hinders direct comparisons across studies. Only one study incorporated collagen into amnion scaffolds [37], showing potential improvements in both mechanical properties and biological activity, thereby fostering a more supportive environment for cartilage repair. There is also a study that utilized an extract from the amnion combined with decellularized sheep osteochondral plugs [36]. Regardless of the processing methods, all amnion-derived scaffolds showed beneficial effects on chondrogenic differentiation and cartilage repair.
To ensure the safety of the amnion scaffold, decontamination and sterilization of the amnion are essential to eliminate potential pathogens prior to application. However, these procedures can impact scaffold bioactivity. Among the 19 studies included, 11 utilized antibiotic and antifungal washes to decontaminate the amnion tissue. While this is a relatively gentle method that preserves the native environment of the amnion, it is considered disinfection or decontamination rather than true sterilization. On the other hand, terminal sterilization processes such as gamma irradiation or ethylene oxide exposure, which are often required for clinical translation, can induce protein denaturation, chemical modification, collagen cross-linking and reduction in essential growth factors [46,47,48]. Hence, optimizing the sterilization dosage is crucial to balance product safety with the preservation of the amnion’s natural properties, which are vital for cartilage repair.
Cell seeding was widely employed to enhance the regenerative potential of amnion scaffolds, with chondrocytes and bone marrow-derived mesenchymal stem cells (BMSCs) being the most commonly used in the selected studies. Other mesenchymal stem cell sources, such as adipose tissue, umbilical cord, and placenta, were used less frequently. This is likely due to chondrocytes being the predominant cell type in mature cartilage [49], while the preference for BMSCs is supported by the evidence suggesting that BMSCs demonstrate superior chondrogenic potential compared to MSCs from other sources in scaffold-free approaches or on various non-amnion scaffolds [50,51]. In addition, amnion has also been reported to be seeded with dental pulp stem cells for evaluating regenerative potential [52]. A limitation of the current literature is the lack of direct comparative evaluations of different types of mesenchymal stem cells seeded on amnion scaffolds. Most of the included studies utilized a single cell source, without parallel comparison to other cell types; only two studies compared different cell types [21,27]. This restricts the ability to determine the cell–scaffold combination for optimized chondrogenic differentiation and cartilage regeneration.
Several studies in this review incorporated composite scaffolds by combining amnion with other biomaterials, including collagen, platelet-rich plasma (PRP), juvenile cartilage fragments (JCFs), and human demineralized bone (DMB), to enhance scaffold functionality. These combinations aimed to improve both the mechanical strength and biological properties of the amnion scaffold. The addition of collagen, a primary structural protein in native cartilage, potentially reinforces the scaffold’s mechanical integrity and provides an enriched microenvironment conducive to cell attachment and differentiation. These composites may better mimic the native cartilage ECM, thereby facilitating improved chondrogenesis and tissue integration. Despite these promising advantages, the limited number of studies utilizing composite scaffolds and the variability in composite formulations highlight the need for more rigorous investigation into optimal composite designs. Future research should focus on systematically comparing composite scaffolds with amnion alone to elucidate their relative benefits in cartilage regeneration applications.
Collectively, these variations in procurement, processing, composite integration, and cell seeding represent critical factors influencing scaffold performance and efficacy in cartilage regeneration. Standardization and thorough reporting of these parameters in future studies are imperative to improve reproducibility, enable meta-analyses, and accelerate clinical translation.
4.2. Experiment Models and Defect Characteristics
In the preclinical in vivo studies included in this review, rabbits and sheep are the two main types of animal models used, each offering distinct advantages and limitations. The lapine model is relatively less costly, smaller and easier to handle [53,54]. A drawback of the rabbit model is that it has relatively small joints with thinner cartilage that exhibits an intrinsic spontaneous healing capacity, which may confound regenerative outcomes and limit direct translation to human clinical contexts. On the other hand, sheep possess larger joints and thicker cartilage that more closely resemble human anatomy. This, coupled with limited intrinsic healing ability, makes them a valuable model for clinically relevant cartilage defect studies [55]. However, the larger size and higher activity levels of sheep necessitate more meticulous postoperative management, such as immobilization and scaffold fixation, to prevent scaffold displacement and ensure treatment efficacy. In this context, post-treatment care and immobilization protocols also differ markedly between models. While rabbits are easier to manage with relatively lower immobilization requirements, sheep require stringent postoperative care due to their size and higher mechanical loads, which increase the risk of scaffold displacement.
The defect models employed across studies varied but generally fell into three categories based on the depth of cartilage involvement: partial-thickness defects, which affect only the articular cartilage layer; full-thickness defects, which extend through the calcified cartilage and may or may not expose subchondral bone; and osteochondral defects, which penetrate the subchondral bone. These diverse defect types allow for the investigation of amnion scaffold effects across a spectrum of lesion severities. The commonly used cartilage defect size in rabbit models typically ranges from 3 to 5 mm in diameter, approximately equivalent to 3 to 5 mm in width or length. However, spontaneous healing has been reported in 3 mm diameter defects [56], leading to the recommendation that defects of 4–5 mm diameter are preferred to minimize these confounding effects and improve experimental reliability [57]. Among the reviewed rabbit models, Turgut et al. [34] and Jun et al. [35] used subcritical size defects (3 mm in width and 3.5 mm in diameter, respectively), which may bias outcomes toward actual amnion scaffold efficacy. In contrast, for the sheep models, both studies that specified the dimensions have reached the critical defect size of 7 mm [57]. However, variation in defect size and inconsistent reporting units pose challenges for direct comparison. Standardized reporting of defect dimensions and types would enhance cross-study comparability and strengthen conclusions.
Overall, while small animal models like rabbits are valuable for initial scaffold evaluation due to their cost-effectiveness and ease of handling, their anatomical and functional disparities from human cartilage limit translational relevance [54,58]. Future research should emphasize larger animal models (sheep, goats, and horses) that better approximate human joint biomechanics, cartilage thickness, and defect characteristics, despite inherent challenges such as longer healing times and more complex postoperative management. Harmonizing defect characterization, animal model selection, and reporting standards across studies will enhance the reliability and applicability of preclinical findings on amnion scaffold-mediated cartilage regeneration.
Apart from the choice of animal models and standardized defect reporting, several unique experimental designs were identified. First, the inclusion of biologically distinct cartilage types, such as laryngeal cartilage defects [37], broadens the review’s scope by illustrating the versatility of amnion scaffolds in diverse contexts. However, it also introduces biological heterogeneity, as the composition and regenerative environment of laryngeal cartilage differ from those of articular cartilage. Transparent acknowledgement of these differences and cautious interpretation of such studies’ results are essential to maintain the rigor and contextual relevance of this review.
Second, one study utilized mixed healthy and osteoarthritic samples without inducing lesions on the tissue [22]. In addition, the study failed to separately report outcomes for healthy versus osteoarthritic samples. The absence of a clear distinction between these two groups results in findings that reflect a general interaction between the amnion and human cartilage, rather than definitive conclusions regarding the scaffold’s efficacy across different pathological states.
4.3. Limitation of Clinical Evidence
The clinical evidence supporting amnion scaffolds for cartilage repair is currently in its early stages, with only one prospective single-arm study identified, providing preliminary, hypothesis-generating data. This scarcity of human data underscores a critical gap in translating preclinical findings to clinical settings, highlighting the urgent need for more clinical studies evaluating amnion scaffolds for cartilage regeneration. The study by Tabet et al. [39] reported favorable clinical improvements across multiple outcome measures, with no product-related adverse effects observed. While these findings suggest the feasibility and safety of amnion scaffolds for cartilage regeneration, they remain insufficient to establish definitive clinical efficacy over existing treatments.
The utility of the results is constrained by several methodological limitations that compromise their reliability and generalizability. As a single-arm prospective design without randomization or a control group, this study lacks comparators such as conventional treatments (without the use of any scaffolding materials) or using other commercialized biomaterials, or other conservative management. In a nutshell, it remains uncertain whether the observed outcomes resulted specifically from the amnion scaffold or from natural healing processes or placebo effects. Additionally, the small sample size (n = 10), with one patient lost to follow-up after 6 months, further reduces the statistical power and confidence in the reported outcomes. The inclusion of only one clinical study also represents a limitation for this review, preventing comparisons across clinical investigations. Future studies should consider exploring additional search databases, such as Medline, for any potential additional clinical evidence.
Future clinical investigations should prioritize randomized controlled trials (RCTs) comparing amnion scaffolds against established cartilage repair modalities, e.g., the commercialized biomaterials. These trials should be supported by standardized amnion manufacturing processes to ensure product consistency across different studies. In addition, the researchers should set clearly defined clinical indications and utilize harmonized outcome measures such as KOOS and VAS alongside imaging techniques to facilitate cross-study comparisons. Lastly, the implementation of larger sample sizes, longer-term follow-up, and improved strategies to maintain subject retention will also be essential to translating these preliminary findings into evidence-based clinical practice.
5. Conclusions
This systematic review provides evidence supporting the efficacy of amnion as a tissue scaffolding material for cartilage regeneration across various in vitro, ex vivo, and in vivo models. However, clinical evidence for the use of amnion in cartilage regeneration remains limited. Future research should therefore prioritize Phase I and Phase II clinical trials. Although amnion has demonstrated promising potential, with several studies reporting superior outcomes compared with other treatment materials, further investigation is required to establish optimized and standardized protocols for amnion scaffold production. This includes focusing on cleanroom-compliant processing and validation in clinical trials before widespread clinical application.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Heir S. Nerhus T.K. Røtterud J.H. Løken S. Ekeland A. Engebretsen L. Årøen A. Focal Cartilage Defects in the Knee Impair Quality of Life as Much as Severe Osteoarthritis: A Comparison of Knee Injury and Osteoarthritis Outcome Score in 4 Patient Categories Scheduled for Knee Surgery Am. J. Sports Med.20093823123710.1177/036354650935215720042546 · doi ↗ · pubmed ↗
- 2Bhosale A.M. Richardson J.B. Articular cartilage: Structure, injuries and review of management Br. Med. Bull.200887779510.1093/bmb/ldn 02518676397 · doi ↗ · pubmed ↗
- 3Pathria M.N. Chung C.B. Resnick D.L. Acute and Stress-related Injuries of Bone and Cartilage: Pertinent Anatomy, Basic Biomechanics, and Imaging Perspective Radiology 2016280213810.1148/radiol.1614230527322971 PMC 4942997 · doi ↗ · pubmed ↗
- 4Karuppal R. Current concepts in the articular cartilage repair and regeneration J. Orthop.201714 A 1A 310.1016/j.jor.2017.05.001PMC 544063528559648 · doi ↗ · pubmed ↗
- 5Yari D. Ebrahimzadeh M.H. Movaffagh J. Shahroodi A. Shirzad M. Qujeq D. Moradi A. Biochemical Aspects of Scaffolds for Cartilage Tissue Engineering; from Basic Science to Regenerative Medicine Arch. Bone Jt. Surg.20221022924410.22038/abjs.2022.55549.276635514762 PMC 9034797 · doi ↗ · pubmed ↗
- 6Liu Y. Shah K.M. Luo J. Strategies for Articular Cartilage Repair and Regeneration Front. Bioeng. Biotechnol.2021977065510.3389/fbioe.2021.77065534976967 PMC 8719005 · doi ↗ · pubmed ↗
- 7Roseti L. Grigolo B. Current concepts and perspectives for articular cartilage regeneration J. Exp. Orthop.202296110.1186/s 40634-022-00498-435776217 PMC 9249961 · doi ↗ · pubmed ↗
- 8Moyad T.F. Cartilage Injuries in the Adult Knee: Evaluation and Management Cartilage 2011222623610.1177/194760351038397326069581 PMC 4300813 · doi ↗ · pubmed ↗