Selection of Recipient Vessels in Double-Barrel STA-MCA Bypass Surgery with the Assistance of Intraoperative ICG Fluorescence: A Case Report and Review of the Literature
Stefanie Bauer, Timo Kahles, Michael Diepers, Gerrit A. Schubert, Lukas Andereggen, Serge Marbacher

TL;DR
This case report shows how intraoperative ICG fluorescence can help choose the best blood vessels for a brain bypass surgery in patients with blocked arteries.
Contribution
The paper demonstrates the novel use of ICG fluorescence for real-time perfusion assessment to guide recipient vessel selection in double-barrel STA-MCA bypass.
Findings
ICG-VA visualizes relative cortical perfusion delay during bypass surgery.
Qualitative ICG-VA supports intraoperative decision-making without invasive imaging.
Postoperative angiography confirmed graft patency and neurological stability in the patient.
Abstract
What are the main findings? Intraoperative indocyanine green video angiography (ICG-VA) visualizes relative cortical perfusion delay in steno-occlusive disease during STA-MCA bypass surgery.This case report demonstrates the application of ICG-VA for recipient vessel selection in double-barrel STA-MCA bypass. Intraoperative indocyanine green video angiography (ICG-VA) visualizes relative cortical perfusion delay in steno-occlusive disease during STA-MCA bypass surgery. This case report demonstrates the application of ICG-VA for recipient vessel selection in double-barrel STA-MCA bypass. What are the implications of the main findings? Perfusion-oriented assessment may complement conventional anatomical criteria during flow-augmentation bypass.Qualitative real-time fluorescence imaging may support intraoperative decision-making without additional invasive imaging. Perfusion-oriented…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
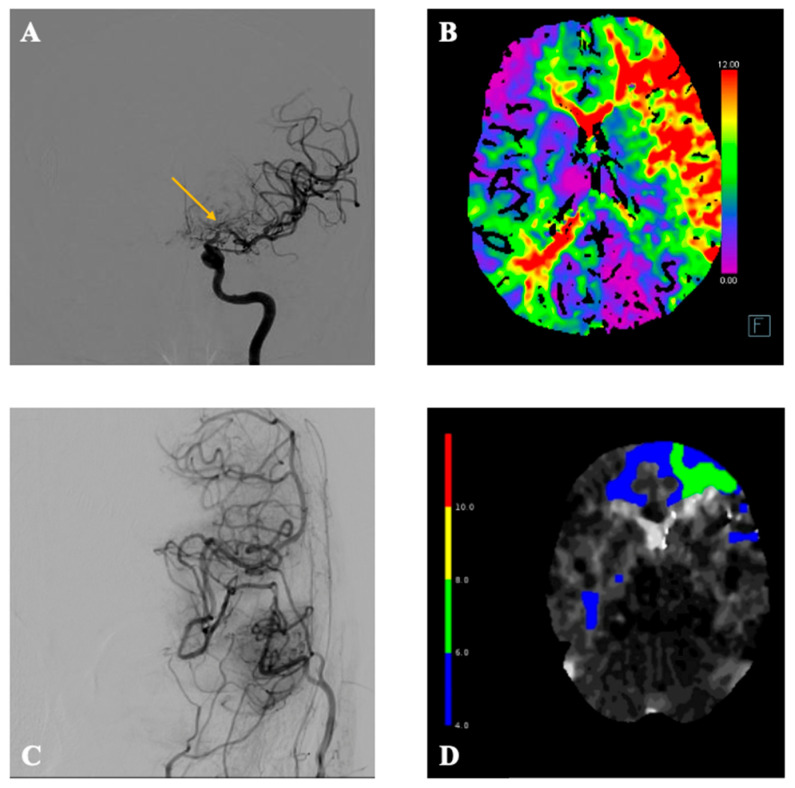 Figure 1
Figure 1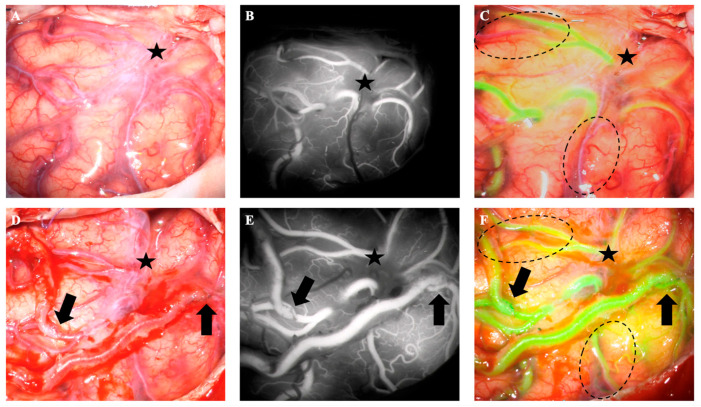 Figure 2
Figure 2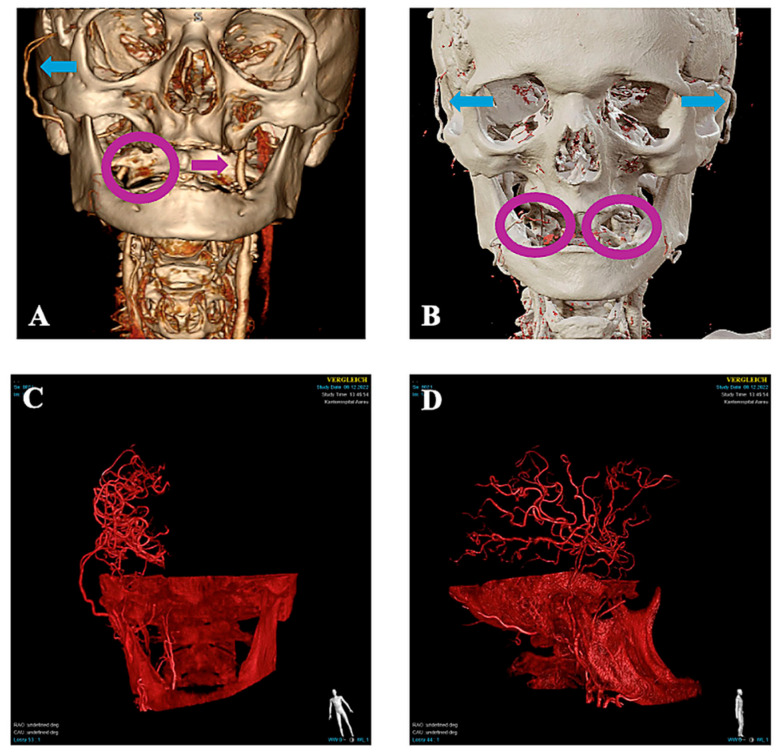 Figure 3
Figure 3| Author | Year | Number of Cases | SB or DB | Indication for EC-IC Bypass | Tools for Recipient Vessel Identification |
|---|---|---|---|---|---|
| Rodríguez-Hernández [ | 2011 | 3 | 3 SB | Aneurysm surgery (100%) | ICG-VA (‘Flash-Fluorescence’) |
| Esposito [ | 2012 | 7 | 5 SB, 2 DB | Aneurysm surgery (100%) | ICG-VA (‘primary’ and ‘secondary’ identification) |
| Esposito [ | 2014 | 2 | SB | Aneurysm surgery (100%) | ICG-VA (‘primary’ and ‘secondary’ identification) |
| Matsumoto [ | 2018 | 1 | SB | Acute cerebral ischemia | ICG-VA (delayed filling) |
| Goldberg [ | 2021 | 60 | SB | MMV (68%), ACVD (32%) | ICG-VA, FLOW800 |
| Current Case | 2025 | 1 | DB | Steno-occlusive disease (bilateral M1 stenosis) | ICG-VA (delayed filling) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMoyamoya disease diagnosis and treatment · Cerebrovascular and Carotid Artery Diseases · Intracranial Aneurysms: Treatment and Complications
1. Introduction
In patients with steno-occlusive cerebrovascular disease who present with recurrent ischemic symptoms and impaired cerebrovascular reserve (hemodynamic failure type II), STA-MCA bypass surgery may be considered when medical therapy is insufficient [1,2]. Although the COSS trial did not demonstrate an overall reduction in ipsilateral stroke risk [3], surgical revascularization remains a therapeutic option in carefully selected patients with documented hemodynamic compromise, where cerebral blood flow augmentation may be beneficial [1,4,5]. In the past decade, the DB STA-MCA bypass has emerged. This bypass may offer advantages in patients with steno-occlusive disease and limited collateral capacity, especially when perfusion deficits involve broader cortical regions requiring augmented flow [6]. Cherian et al. showed that DB STA-MCA bypasses may be considered ‘high-flow’ bypasses with relatively large flow capacities of 30–120 cc/min [7]. Nonetheless, the success of any cerebral bypass depends on selecting the right recipient vessel. Several tools can be used during the surgery such as navigation guidance through preoperative imaging, intraoperative Doppler sonography, intraoperative digital subtraction angiography (DSA) or intraoperative ICG-VA [8]. We review the literature and present a case using ICG-VA to select the optimal recipient vessels during DB STA-MCA bypass surgery.
2. Case Description
A 68-year-old male patient initially presented with a history of recurrent ischemic stroke due to atherosclerotic right-sided M1 occlusion of the MCA. The patient was successfully treated with a traditional DB STA-MCA bypass on the right side three years ago. During follow-up, an occlusion of the contralateral M1-branch occurred with subsequent hemodynamic failure type II. Clinically, the patient presented with blood pressure-dependent right-sided faciobrachial hemiparesis. The CT-angiogram (CTA) visualized a large perfusion mismatch on the left hemisphere due to progression of the already known stenosis of the M1 branch on the left side with decompensation of the collateral vessels (Figure 1). The preoperative DSA with selective vertebral artery injection revealed leptomeningeal collateralization from the posterior cerebral artery (PCA) to distal MCA branches, particularly supplying the temporal cortical region. This retrograde filling pattern reflected compensatory pial anastomoses due to proximal M1 occlusion. The patient was discussed at our interdisciplinary neurovascular board, where the treatment with a DB STA-MCA bypass on the left side was indicated.
Intraoperatively, we used ICG-VA to guide decision-making in choosing the most promising recipient arteries. After dural opening, 25 mg ICG was applied via peripheral venous line. We used a ZEISSS KINEVO 900 microscope (Carl Zeiss Meditec AG, Jena, Germany) with the integrated INFRARED 800 module to visualize the fluorescence. Several cortical MCA branches demonstrated delayed fluorescence arrival compared to adjacent vessels. Two superficial cortical branches on the frontal and temporal convexity exhibited the most pronounced perfusion delay. Recipient selection was based on the relative fluorescence delay suggesting hemodynamic compromise, sufficient vessel diameter (≥1 mm) for safe anastomosis, and favorable accessibility within the operative field (Figure 2). After anastomosis of both vessels to the STA branches, another ICG-VA was performed to evaluate the patency of both bypasses (Figure 2). The patient recovered quickly after surgery with complete regression of symptoms.
At the follow-up visit 2 months postoperatively, the patient demonstrated sustained clinical stability, reporting feeling higher energy levels than before surgery and with no new neurological deficits. Although CTA and CTP at 2 months raised suspicion of possible compromise of the left frontal bypass due to focal perfusion delay, a confirmatory DSA demonstrated the patency of all four bypass grafts (Figure 1 and Figure 3), and MRI excluded new ischemia. Serial neurovascular ultrasound examinations at 1 and 5 months postoperatively likewise demonstrated the sustained patency of both STA donor branches. The patient is still closely monitored in the neurologic outpatient clinic with regular clinical checks and neurovascular ultrasound.
3. Discussion
Selecting the right recipient vessel is crucial to achieving optimal revascularization in cerebral bypass surgery. Traditional recipient vessel selection relies on preoperative imaging, anatomical landmarks, and intraoperative vessel appearance upon visual inspection and Doppler sonography. For the STA-MCA bypass, the recipient vessel should have a diameter similar to the diameter of the STA [2]. Some tools have emerged in the past that help in recipient vessel selection. Some surgeons may use intraoperative doppler sonography to evaluate the blood flow of potential recipients. However, doppler signal interpretation is difficult and remains subjective for the interpreter [9]. Intraoperative digital subtraction angiography may not only be used to evaluate bypass patency but also to support the surgeon in recipient vessel identification and evaluation of perfusion of cortical vessels. But its routine use in cerebral bypass surgery is limited by its invasiveness, high costs and increased duration of surgery [8]. ICG-VA and its quantitative analysis with, e.g., FLOW800 (Carl Zeiss Meditec AG, Jena, Germany) are established tools in cerebrovascular surgery and have long been used to assess the patency of anastomoses [10,11]. Lawton and colleagues proposed the technique called ‘flash fluorescence’ in 2011, which is a convenient method to identify recipient vessels in aneurysmal bypass surgery (Table 1). Hereby, ICG is applied after temporary clipping of the necessary artery showing perfusion delay in some cortical arteries. If these arteries fill rapidly with ICG after removal of the temporary clips, they are deemed suitable as recipient vessels [12]. Furthermore, ICG-VA emerged to be useful in refining recipient vessel selection. ICG-VA is readily available and provides real-time perfusion data, thus facilitating the identification of vessels with delayed perfusion [13]. In 2012, Esposito et al. defined a primary and secondary identification of recipient vessels using ICG-VA in cerebral bypass surgery for the treatment of complex MCA aneurysms. In primary identification, the baseline ICG-VA already showed a delayed filling of a cortical artery due to increased resistance to flow. In secondary identification, the involved cortical arteries were identified with a flow delay after temporary occlusion of an MCA branch [13].
In cases of steno-occlusive disease, the baseline ICG-VA already shows delayed vessel filling. Thus, the concept of primary identification from Esposito et al. [13]. may be used. In our case, we identified a frontal and a temporal cortical (M4) branch of the left MCA with delayed filling upon ICG-VA. Both these branches had a diameter >1 mm and were easily accessible in the operating field, allowing a structured selection strategy that combined perfusion-based assessment with conventional anatomical criteria. Postoperative imaging studies revealed the restored perfusion of the entire left hemisphere, and the neurologic symptoms fully regressed—supporting the adequacy of the selected recipient vessels.
In routine surgical practice, sequential intraoperative ICG-VA assessment may further refine hemodynamic evaluation during bypass procedures. Performing ICG-VA at baseline, after completion of the first anastomosis, and again after the second bypass can help assess the degree of perfusion improvement following each step of revascularization. If cortical perfusion improves sufficiently after the first anastomosis, performing a second anastomosis may be unwarranted and could theoretically increase the risk of postoperative hyperperfusion syndrome. Intraoperative perfusion assessment using ICG-VA and its quantitative analysis have been shown to detect bypass-related hemodynamic changes and may help identify patients at risk for hyperperfusion [14,15]. In the present case, the decision to perform a double-barrel bypass had already been established preoperatively, based on the CT perfusion imaging demonstrating pronounced hemispheric hypoperfusion and insufficient collateralization, suggesting that more extensive flow augmentation would be required.
Nevertheless, the interpretation of ICG-VA remains qualitative, as quantitative intraoperative flow measurements such as FLOW800-based fluorescence analysis were not performed in this case. Consequently, the objective assessment of flow volume or pressure gradients across the anastomoses was not available. In addition, longitudinal quantitative perfusion imaging beyond the early postoperative phase was limited. While clinical and neurovascular ultrasound confirmed patency at 5 months postoperatively, the degree of long-term hemodynamic augmentation cannot be precisely quantified.
The concept of intraoperative selection of the optimal recipient vessel in a patient with ischemic cerebrovascular disease was first described by Matsumoto in 2018 [16]. Recently, a larger case series was published describing the use of ICG-VA for intraoperative vessel-selection in patients with moyamoya disease and atherosclerotic cerebrovascular disease [17]. However, all patients in this study underwent single barrel (SB) bypasses. We presented here the first case of DB STA-MCA bypass for steno-occlusive disease using intraoperative ICG-VA for recipient vessel selection and confirmed its usefulness.
4. Conclusions
This case report demonstrates that ICG-VA can assist in recipient vessel selection during DB STA-MCA bypass surgery in patients with steno-occlusive cerebrovascular disease. The real-time visualization of delayed cortical perfusion supported structured vessel selection and was associated with favorable short-term clinical and radiological outcomes. However, larger prospective studies incorporating quantitative hemodynamic analysis are required to further evaluate the routine use of ICG-VA for recipient vessel selection in EC-IC bypass procedures.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Esposito G. Amin-Hanjani S. Regli L. Role of and Indications for Bypass Surgery After Carotid Occlusion Surgery Study (COSS)?Stroke 20164728229010.1161/STROKEAHA.115.00822026658449 · doi ↗ · pubmed ↗
- 2Wessels L. Hecht N. Vajkoczy P. Bypass in Neurosurgery—Indications and Techniques Neurosurg. Rev.20194238939310.1007/s 10143-018-0966-929536207 · doi ↗ · pubmed ↗
- 3Powers W.J. Clarke W.R. Grubb R.L. Videen T.O. Adams H.P. Derdeyn C.P. Coss Investigators F.T. Extracranial-Intracranial Bypass Surgery for Stroke Prevention in Hemodynamic Cerebral Ischemia: The Carotid Occlusion Surgery Study Randomized Trial JAMA 2011306198310.1001/jama.2011.161022068990 PMC 3601825 · doi ↗ · pubmed ↗
- 4Sadigh Y. De Haan Y. Haasdijk E.J. Verploegh I. Busse T.L. Ciobanu-Caraus O. Călăuz A.-M. Spinean A.A. Lariu A.-D. Dammers R. Indications and Outcomes of Intracranial Bypass: A Systematic Review and Meta-Analysis World Neurosurg.202520112430810.1016/j.wneu.2025.12430840701362 · doi ↗ · pubmed ↗
- 5Elder T.A. White T.G. Woo H.H. Siddiqui A.H. Nunna R. Siddiq F. Esposito G. Chang D. Gonzalez N.R. Amin-Hanjani S. Future of Endovascular and Surgical Treatments of Atherosclerotic Intracranial Stenosis Stroke 20245534435410.1161/STROKEAHA.123.04363438252761 · doi ↗ · pubmed ↗
- 6Burkhardt J.-K. Winkler E.A. Gandhi S. Lawton M.T. Single-Barrel Versus Double-Barrel Superficial Temporal Artery to Middle Cerebral Artery Bypass: A Comparative Analysis World Neurosurg.2019125 e 408e 41510.1016/j.wneu.2019.01.08930703593 · doi ↗ · pubmed ↗
- 7Cherian J. Srinivasan V. Kan P. Duckworth E.A.M. Double-Barrel Superficial Temporal Artery-Middle Cerebral Artery Bypass: Can It Be Considered “High-Flow”?Oper. Neurosurg.20181428829410.1093/ons/opx 11928961997 · doi ↗ · pubmed ↗
- 8Balamurugan S. Agrawal A. Kato Y. Sano H. Intra Operative Indocyanine Green Video-Angiography in Cerebrovascular Surgery: An Overview with Review of Literature Asian J. Neurosurg.20116889310.4103/1793-5482.9216822347330 PMC 3277076 · doi ↗ · pubmed ↗