Clinical Impact of a LAG3 Single-Nucleotide Polymorphism in Relapsed, Refractory DLBCL Patients Treated with Glofitamab
Maeva Ullmann, Katja Seipel, Henning Nilius, Martina Bertschinger, Vera Rentsch, Ulrike Bacher, Thomas Pabst

TL;DR
A genetic variant in the LAG3 gene is linked to better outcomes in lymphoma patients treated with glofitamab.
Contribution
Identifies a LAG3 single-nucleotide polymorphism as a potential prognostic marker for glofitamab treatment in DLBCL.
Findings
Homzygous LAG3 T455 carriers had extended progression-free and overall survival.
Homozygous LAG3 I455 carriers showed shorter survival outcomes.
CTLA4 genotype had no significant impact on treatment outcomes.
Abstract
Glofitamab is a newly approved bispecific antibody for the treatment of relapsed, refractory diffuse large B-cell lymphoma. Treatment response may vary depending on the genetic background of the patient. Here, we evaluate clinical outcomes in patients with DLBCL treated with glofitamab according to LAG3 and CTLA4 genotypes. While there was no apparent clinical impact associated with the CTLA4 genotype, there was a significant association of the LAG3 genotype with clinical response. Future personalized therapeutic strategies may evolve in consideration of a specific LAG3 gene polymorphism. Background: Glofitamab is a bispecific antibody engaging CD3 on T-cells and CD20 on B-cells. Glofitamab is approved for the treatment of relapsed, refractory diffuse large B-cell lymphoma (R/R DLBCL). Lymphocyte-activation gene 3 (LAG3) and T-lymphocyte-associated protein 4 (CTLA4) are immune…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
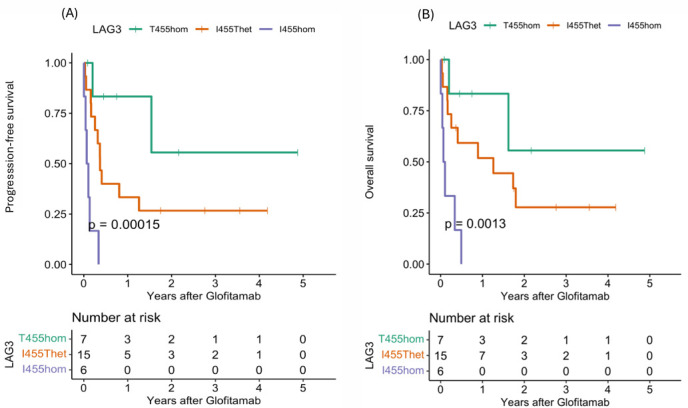 Figure 1
Figure 1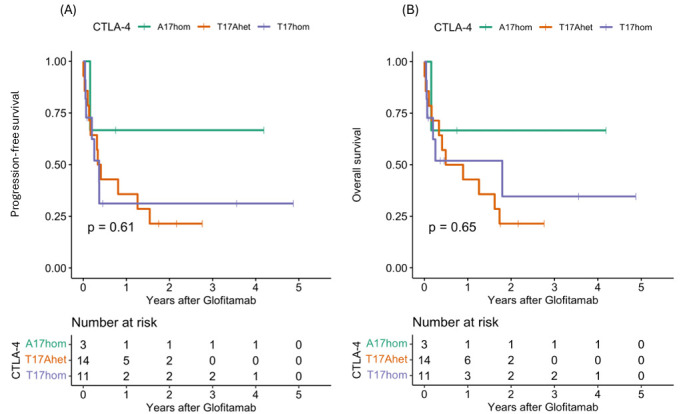 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Immunotherapy and Biomarkers · CAR-T cell therapy research · Monoclonal and Polyclonal Antibodies Research
1. Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most frequent aggressive non-Hodgkin lymphoma [1,2,3,4]. While around 60% of DLBCL patients can be cured by frontline therapy with R-CHOP, a significant proportion of patients experience relapse or refractory disease [1,5,6]. Glofitamab is a bispecific antibody (BsAb) and T-cell engager (BiTE) binding CD3 on endogenous T-cells and CD20 on malignant B-cells, resulting in T-cell activation and tumor cell lysis [5,7,8]. Glofitamab has emerged as an effective immunotherapy for relapsed or refractory DLBCL (R/R DLBCL), with durable response in heavily pretreated patients [5,9,10]. Glofitamab therapy is approved for R/R DLBCL after two or more prior lines of systemic therapy [11]. There is marked variability in glofitamab response rates among R/R DLBCL patients, indicating that patients’ immune systems may affect clinical outcomes.
The efficacy of glofitamab therapy depends on the presence of functional T-cells [7,12]. Lymphocyte Activation Gene 3 (LAG3) and T-lymphocyte-associated protein 4 (CTLA4) are immune checkpoint receptors that are both expressed on T-cells [13,14]. Common germline single-nucleotide polymorph (SNP) variants in CTLA4 and LAG3 genes have been associated with clinical response in DLBCL treated with CAR T-cell therapy [15,16]. By transmitting inhibitory signals, LAG3 and CTLA4 can limit T-cell expansion and inhibit effector function [17,18]. LAG3 expression is significantly upregulated in DLBCL [19,20,21]. Elevated LAG3 expression and specific LAG3 gene polymorphisms are associated with an impaired T-cell response and inferior outcomes in patients treated with T-cell-engaging therapies, such as CAR T-cell therapy in DLBCL [16]. Preclinical studies indicate that T-cell exhaustion, characterized by upregulation of inhibitory receptors such as LAG3, can reduce the cytotoxic potential of endogenous T-cells, which are engaged by glofitamab [7,22].
Combining glofitamab with an immune checkpoint blockade by LAG3 inhibition can increase T-cell activation, maintain effector function, and improve antitumor efficacy in lymphoma models [22]. This supports the hypothesis that LAG3-mediated immune regulation is an important determinant in the response to glofitamab. Moreover, the LAG3 genotype may serve as predictive biomarker for the response to BsAb therapy in DLBCL [9,22,23]. In this exploratory investigation, we evaluated clinical outcomes in R/R DLBCL patients treated with glofitamab according to LAG3 rs870849 and CTLA4 rs231775 SNPs.
2. Materials and Methods
2.1. Patients
This retrospective, single-center observational study included 28 DLBCL patients treated with glofitamab in 2020–2025 at the University Hospital of Bern, Switzerland.
As per established standard-of-care procedure [6], patients received one single dose of 1000 mg obinutuzumab (Gazyvaro^®^, Roche, Basel, Switzerland) on cycle 1 day 1 (C1D1) to achieve a depletion of B-cells in peripheral blood and secondary lymphoid tissues, thereby attenuating subsequent T-cell activation and reducing the incidence and severity of cytokine release syndrome (CRS). Thereafter, step-up dosing of glofitamab was performed with 2.5 mg on C1D8 and 10 mg on C1D15, followed by administration of a fixed 30 mg dose every 21 days, starting from cycle 2, day 1 (C2D1).
This study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the Ethics Committee in Bern, Switzerland (decision number: 2021-01294; date of approval: 9 December 2021).
2.2. Study Endpoints
The primary endpoint of this study was clinical outcome after glofitamab treatment in DLBCL patients according to germline variants LAG3 rs870849 and CTLA4 rs231775. The secondary endpoints of this study were toxicities after glofitamab treatment, including cytokine release syndrome (CRS) and immune-effector cell-associated neurotoxicity syndrome (ICANS).
2.3. Statistical Analysis
Progression-free survival (PFS) was defined as the time interval from cycle 1 day 1 (C1D1) to progression, relapse, death, or cut-off date 1 November 2025. Overall survival (OS) was defined as the time interval from C1D1 to death from any cause or cut-off date 1 November 2025. Baseline characteristics were analyzed according to LAG3 rs870849 and CTLA4 rs231775 somatic genetic variants. Continuous variables are reported as median and interquartile range (IQR), while categorical variables are presented as counts and percentages. Comparisons of continuous variables between groups were performed using the Kruskal–Wallis test. Categorical variables were compared using the Chi-square test or Fisher’s exact test when expected cell counts were <5. Survival outcomes were estimated using Kaplan–Meier curves and compared between genetic groups using the log-rank test. In addition, univariable and multivariable Cox proportional hazards regression models were fitted to estimate the hazard ratios and corresponding 95% confidence intervals. Multivariable models were adjusted for age, sex, prior CAR T-cell therapy, prior high-dose chemotherapy with autologous stem cell transplantation (HDCT/ASCT), number of prior lines of therapy, and remission status before glofitamab treatment. All analyses were done in R Version 4.5.1.
2.4. LAG3 and CTLA4 Gene Analysis
Peripheral blood monocytes (PBMCs) were collected prior to glofitamab treatment. Genomic DNA was extracted; LAG3 gene exon seven and CTLA4 gene exon one were amplified and sequenced as previously described [15,16].
3. Results
3.1. Baseline and Clinical Characteristics
This retrospective observational study included 28 R/R DLBCL patients treated with glofitamab at the University Hospital of Berne, Switzerland. Most patients were multi-drug resistant and refractory to CAR-T-cell therapy. The patient characteristics were analyzed in the entire cohort and in the three rs870849 genetic subgroups LAG3 T455hom, I455Thet, and I455hom (Table 1). The median age at initial diagnosis ranged from 62 years in the I455Thet and I455hom subgroups to 72 years in the T455hom subgroup (p = 0.16). In the LAG3 genetic subgroups, males and females were distributed unequally, with male predominance in the T455hom subgroup and female predominance in the I455hom subgroup (p = 0.0001). The majority of patients presented with Ann Arbor stage IV. The T455hom and I455Thet subgroups incorporated a higher proportion of de novo DLBCL (57 and 73%), with equal proportions of de novo and transformed DLBCL in the I455hom subgroup. All patients received R-CHOP as first-line immuno-chemotherapy, and most patients received radiotherapy prior to glofitamab therapy. In total, 25% of the patients had a pretreatment with HDCT/ASCT and 75% had a prior CAR T-cell therapy, with a significantly lower proportion of patients receiving CAR T-cell therapy in the I455hom subgroup (p = 0.029).
The patient characteristics were separately analyzed in the three rs231775 genetic subgroups CTLA4 A17hom, T17Ahet, and T17hom (Table 2). The median age at initial diagnosis ranged from 62 years in the T17Ahet subgroup to 69–70 years in the T17hom and A17hom subgroups, respectively (p = 0.56). In the CTLA4 genetic subgroups, both sexes were equally represented. The T17Ahet and T17hom subgroups had higher proportions of de novo DLCBL (64% and 73%, respectively) compared to the A17hom subgroup (33%). Most patients in the T17hom subgroup received radiotherapy, and the majority of patients across all genetic subgroups received CAR T-cell therapy prior to glofitamab treatment.
3.2. Clinical Outcomes After Glofitamab Therapy
The clinical outcomes were analyzed in the entire cohort and in the three LAG3 genetic subgroups (Table 3). In the I455hom subgroup, 50% of the patients developed CRS following glofitamab treatment, with one patient each experiencing grade 2, 3 and 4 CRS. In contrast, fewer than one third of patients in the I455Thet and T455hom subgroups developed CRS after glofitamab treatment. Two patients experienced grade 2 ICANS following glofitamab treatment: one in the T455hom and one in the I455hom subgroup. One third of the patients experienced relapse, with a higher proportion in the I455hom subgroup (50%). The complete remission (CR) rate was high in the T455hom and I455het subgroups (40–50%), with no overall response in the I455hom subgroup (p = 0.07). Dose-dependent effects of LAG3 rs870849 emerged in the analysis of progression-free survival (PFS) and overall survival (OS) in the three LAG3 genetic subgroups: T455hom, I455Thet, and I455hom (Figure 1A,B). While the T455hom genetic variant was associated with favorable outcomes with median PFS of 19 months and one-year PFS and OS rates of 83%, the I455Thet genetic variant was associated with inferior outcomes with median PFS of 4 months and one-year PFS and OS rates of 31% and 45% and the I455hom genetic variant was associated with dismal outcomes with early disease progression and death (PFS p = 0.0002, OS p = 0.013, PFz and OS rates p = 0.0001). In fact, all of the I455hom patients had progressive disease as the best response, indicating resistance to glofitamab therapy. In the multivariate analysis, LAG3 I455hom was an indicator of inferor treatment outcome with a hazard ratio (HR) of 14 in PFS (p = 0.002) and a HR of 16 in OS (p = 0.004) compared to T455hom (Table 4). The number of prior therapy lines was associated with inferior treatment outcome with a HR of 2.6 in PFS (p = 0.022) and a HR of 3.1 in OS (p = 0.007). Surprisingly, patients with a CAR T-cell therapy prior to glofitamab treatment had a superior response to glofitamab with HR 0.2 in PFS and OS (p = 0.08). No significant differences were detected in the three CTLA4 genetic subgroups in respect to clinical outcomes (Table 5, Figure 2). CRS and ICANS, however, were absent in the A17hom and prevalent in the T17hom subgroup, indicating an association of CTLA4 genotype with T-cell activity.
4. Discussion
In this retrospective observational study, we evaluated treatment outcomes in patients with relapsed/refractory DLBCL after glofitamab treatment, stratified according to the LAG3 rs870849 genetic variants T455hom, I455Thet, and I455hom, and separately according to CTLA4 rs231775 genetic variants. Clinical outcome to glofitamab therapy was associated with LAG3 genotype of the recipients. PFS and OS analyses demonstrated inferior outcomes in LAG3 I455hom, superior outcomes in LAG3 T455hom, and intermediate outcomes in LAG3 I455Thet, a response pattern consistent with the dose-dependent effects of LAG3 rs870849 in DLBCL treated with glofitamab. In contrast, clinical outcomes of glofitamab therapy were not associated with the CTLA4 genotype of the recipients. In a previous study in DLBCL treated with CD19-directed CAR T-cell therapy, LAG3 rs870849 had dominant positive effects on survival and was not dose-dependent, while CTLA4 rs231775 had dose-dependent effects on survival [15,16]. Therefore, it can be assumed that LAG3 and CTLA4 functions may differ in anti-CD19 CAR T-cell therapy and anti-CD20 bsAB therapy.
The LAG3 polymorphism may regulate T-cell function by altering the inhibitory signaling capacity, thereby modulating T-cell activation, proliferation, and differentiation. LAG3 receptor localizes to the immunological synapse and associates with the T-cell receptor (TCR)-CD3 complex in CD4+ and CD8+ T-cells [24,25,26]. Variants that reduce LAG3 expression result in lower inhibitory signaling at the immunological synapse, leading to enhanced T-cell activation and increased proliferation [27]. Polymorphisms altering LAG3 expression or function may influence the threshold for T-cell activation, given that LAG3 suppresses T-cell activation by disrupting TCR-CD3 signaling [24]. In allogenic hematopoietic stem cell transplantation, LAG3 polymorphism in donor cells can enhance T-cell reactivity and lead to severe Graft versus host disease (GVHD) [27,28]. The rs870849 snp causes a substitution of isoleucine to threonine (I455T) within the LAG3 transmembrane domain, affecting protein processing and proteolytic cleavage [28]. In the R/R DLBCL LAG3 I455hom carriers, glofitamab treatment triggered an abortive T-cell activation accompanied by excessive inflammatory cytokine production, but did not induce the sustained cytolytic activity necessary for tumor destruction, due to a combination of low efficacy and high toxicity, characteristic of an abnormal immune response. This biochemical disorder may result from decreased cleavage of the LAG3 molecule at the cell surface, leading to T-cell dysfunction.
This is the first study that investigates the impact of LAG3 and CTLA4 polymorphisms on treatment outcomes in relapsed, refractory DLBCL patients treated with glofitamab. Efficacy, safety, and clinical endpoints after glofitamab treatment have been previously studied [5,11]. Other studies revealed that LAG3 and PD1 gene expression were significantly upregulated in DLBCL [19,20,29]. Lee et al. investigated the expression patterns of immune checkpoint receptors in DLBCL and revealed a unique LAG3 expression pattern distinct from other immune checkpoint receptors in DLBCL and proposed a combination therapy of LAG3- and PD-1-inhibitors in the treatment of DLBCL [30].
This study has several limitations. The retrospective single-center study design and the small sample size with only a few patients in the genetic subgroups may have introduced selection bias and affected the generalizability. Due to the small sample size, this investigation is explorative, including the risk of false positive and false negative results. Furthermore, due to the lack of a control cohort, it was not possible to differentiate between prognostic and predictive value. Certain imbalances in the baseline characteristics, particularly the different prior treatments with CAR T-cell therapy, may have also influenced the outcomes. Only 33% of patients in the I455hom subgroup received CAR-T-cell therapy, whereas more than 85% of patients in the T455hom and the I455het subgroup were treated with CAR-T-cell therapy before glofitamab treatment. Also, 83% of the I455hom subgroup were men, whereas in the other genetic subgroups, men and women were equally represented, indicating an imbalance that may have influenced the results. Furthermore, as most patients were not only diagnosed with R/R DLBCL but were also multi-drug resistant and refractory to CAR-T therapy, the results of this study cannot be generalized to R/R DLBCL. Objective parameters were assessed and a multivariate analysis was performed to evaluate the potential influence of confounding factors on the observed outcomes. The multivariate analysis identified the I455hom genotype as the most significant predictor of both PFS and OS, suggesting that the genetic characteristics of the inhibitory cell surface receptor may have greater prognostic relevance than established clinical factors such as sex, age, or number of prior therapies. The use of germline SNPs as risk factors may enable the early identification of ‘high-risk’ R/R DLBCL patients, for example, those with the LAG3 I455H homozygous genotype. For these ‘high-risk’ patients, combination therapy with glofitamab may prevent early disease progression and improve survival outcomes.
5. Conclusions
This retrospective single-center study reveals a significant association between LAG3 rs870849 genotype and treatment outcomes in R/R DLBCL treated with glofitamab, with inferior outcomes in carriers of the LAG3 I455 genetic variant. The LAG3 SNP rs870849 may serve as a prognostic biomarker for treatment response in patients with R/R DLBCL receiving glofitamab treatment. To validate this hypothesis, further investigations and larger, prospective studies are required. Mechanistic studies will be required to analyze the projected differential functions of the LAG3 variant proteins.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Silkenstedt E. Salles G. Campo E. Dreyling M. B-cell non-Hodgkin lymphomas Lancet 20244031791180710.1016/S 0140-6736(23)02705-838614113 PMC 12261310 · doi ↗ · pubmed ↗
- 2Liu Y. Barta S.K. Diffuse large B-cell lymphoma: 2019 update on diagnosis, risk stratification, and treatment Am. J. Hematol.20199460461610.1002/ajh.2546030859597 · doi ↗ · pubmed ↗
- 3Sehn L.H. Salles G. Diffuse Large B-Cell Lymphoma N. Engl. J. Med.202138484285810.1056/NEJ Mra 202761233657296 PMC 8377611 · doi ↗ · pubmed ↗
- 4Chaudhari J. Shah N.N. Targeted Therapies and Immunotherapies for Diffuse Large B-Cell Lymphoma Cancers 202517251710.3390/cancers 1715251740805213 PMC 12345741 · doi ↗ · pubmed ↗
- 5Dickinson M.J. Carlo-Stella C. Morschhauser F. Bachy E. Corradini P. Iacoboni G. Khan C. Wróbel T. Offner F. TrněnýM. Glofitamab for Relapsed or Refractory Diffuse Large B-Cell Lymphoma N. Engl. J. Med.20223872220223110.1056/NEJ Moa 220691336507690 · doi ↗ · pubmed ↗
- 6Rentsch V. Seipel K. Banz Y. Wiedemann G. Porret N. Bacher U. Pabst T. Glofitamab Treatment in Relapsed or Refractory DLBCL after CAR T-Cell Therapy Cancers 202214251610.3390/cancers 1410251635626120 PMC 9139991 · doi ↗ · pubmed ↗
- 7Bröske A.M.E. Korfi K. Belousov A. Wilson S. Ooi C.H. Bolen C.R. Canamero M. Alcaide E.G. James I. Piccione E.C. Pharmacodynamics and molecular correlates of response to glofitamab in relapsed/refractory non-Hodgkin lymphoma Blood Adv.202261025103710.1182/bloodadvances.202100595434941996 PMC 8945294 · doi ↗ · pubmed ↗
- 8Heini A.D. Bacher U. Porret N. Wiedemann G. Legros M. Stalder Zeerleder D. Seipel K. Novak U. Daskalakis M. Pabst T. Experiences with Glofitamab Administration following CAR T Therapy in Patients with Relapsed Mantle Cell Lymphoma Cells 202211274710.3390/cells 1117274736078155 PMC 9454987 · doi ↗ · pubmed ↗