Analysis of Molecular Markers of HPV Infection Persistence: A Narrative Review
Dominik Pruski, Sonja Millert-Kalińska, Katarzyna Wszołek, Victoria Musiałowicz, Jacek P. Grabowski, Robert Jach, Mustafa Zelal Muallem, Jalid Sehouli, Marcin Przybylski

TL;DR
This paper reviews how different molecular tests detect persistent HPV infections, which are a major cause of cervical cancer, and how these tests can improve screening and risk assessment.
Contribution
The paper provides a narrative synthesis of three complementary molecular approaches to define HPV persistence and their implications for cervical cancer screening.
Findings
HPV DNA testing identifies persistent infection with high sensitivity but limited specificity.
E6/E7 mRNA testing detects active oncogenic infection and improves specificity for clinically relevant lesions.
DNA methylation biomarkers reflect epigenetic changes linked to long-term infection and cancer progression.
Abstract
Persistent infection with high-risk human papillomavirus is the key driver of cervical cancer development. Molecular diagnostics have evolved through three complementary approaches that reflect different biological stages of HPV persistence. The earliest approach, HPV DNA testing, identifies repeated detection of the same viral genotype over time and provides high sensitivity for identifying infection but limited specificity for predicting disease progression. The second approach, HPV E6/E7 mRNA testing, detects expression of viral oncogenes responsible for cell cycle dysregulation, representing active oncogenic infection and offering improved specificity for clinically relevant lesions. The most recent approach involves DNA methylation biomarkers, which measure epigenetic alterations in viral and host genes associated with long-term infection, viral integration, and progression to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
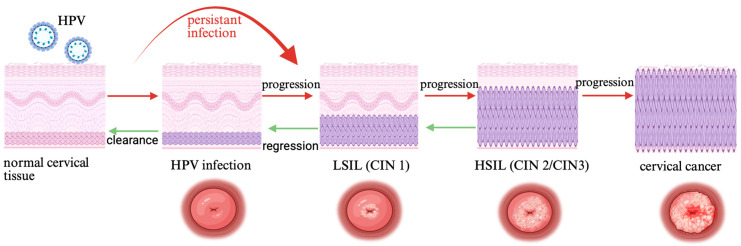 Figure 1
Figure 1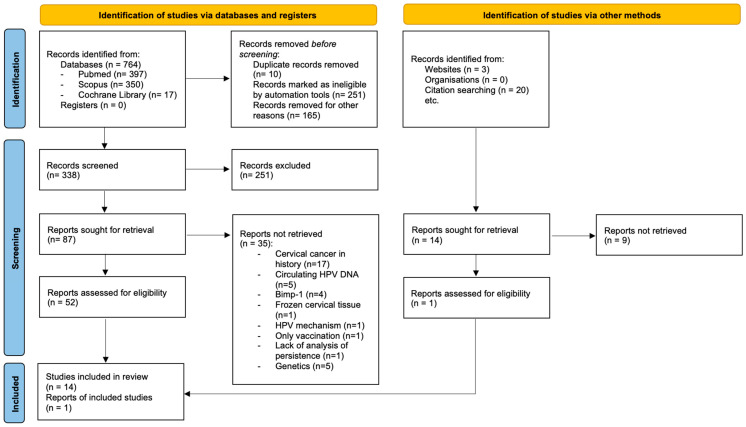 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCervical Cancer and HPV Research · Head and Neck Cancer Studies · Reproductive tract infections research
1. Introduction
Human Papillomavirus (HPV) is the most common sexually transmitted infection in the human population. According to World Health Organization reports, in 2024, cervical cancer was diagnosed in 670,000 cases and was the cause of 350,000 deaths worldwide. This makes it the fourth most frequent cancer in women globally. Therefore, the WHO announced in May 2018 a global strategy to eliminate cervical cancer by 2030, following the 90–70–90 targets. Ninety percent of girls should be fully vaccinated by age 15, 70% of women have access to high-performance screening tests, and 90% of women with precancerous lesions and diagnosed invasive cancer cases receive appropriate treatment [1]. HPV infection prevalence peaks in two age groups. Young adults aged 18–25 years are the most sexually active group. The second peak occurs around age 50, when entering new relationships. Around 90% of infections are transient, meaning they are cleared spontaneously within 2 years of primary detection. The remaining 10% remains persistent, eventually leading to invasive cancer if the neoplasia remains untreated [2]. Several factors have been identified that can contribute to the persistence of HPV infection: having many pregnancies, a high number of sexual partners, genetic predispositions, smoking, the use of immunosuppressive medications, and co-infections with other sexually transmitted pathogens such as herpes simplex virus type 2 and Chlamydia trachomatis [3,4].
Ongoing research is examining the role of the vaginal microbiome in the development of precancerous and cancerous lesions. Alterations in the microbiome may impair viral clearance, thereby promoting persistent infection [5,6]. More than two hundred viral genotypes have been identified. The vast majority of cervical cancers are associated with persistent infection by high-risk types, including 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, and 59. A breakthrough in the diagnosis of precancerous lesions and cervical cancer was Harald zur Hausen’s discovery. The scientist proved that human papillomavirus infection is responsible for carcinogenesis, and this way is recognized as the principal factor in the development of cervical cancer. Persistent HPV infection may lead to the development not only of cervical cancer, but also of anogenital (vulvar, vagina, penile, anal) and oropharyngeal cancers. Apart from malignant lesions, benign papillomas may occur in the anogenital area as well as in the oral cavity [7].
Detection methods for precancerous conditions and cervical cancer have evolved over the years, from the conventional Pap smear, through liquid-based cytology, to the link with the human papillomavirus and molecular assessment of HPV infection in the cervix. Subsequent molecular approaches include HPV mRNA testing, methylation testing, immunocytochemical assessment of p16 and Ki-67 in cytological specimens, and immunohistochemical detection of E4, E6, and E7 proteins in cervical tissue specimens. Cutting-edge medical discoveries are supporting physicians, including the use of AI in colposcopic software, devices such as DYSiS, which uses advanced photonics to measure the speed, intensity, and duration of the acetowhitening process on the cervix, creating a special map of the cervix with suggested biopsy areas. Some innovative methods, but with little clinical application so far, are spectroscopic methods—LuViva, and optoelectronic methods—Truscreen and Zedscan. The field of cervical cancer screening has evolved across multiple research traditions, each with distinct conceptual foundations, theoretical parameters, and methodological assumptions. Because these traditions have developed in parallel and often produce incompatible findings, a narrative review—designed to map and compare storylines of scientific inquiry—provides a suitable approach. Our work focuses in particular on the historical approach to molecular markers detecting features of persistent HPV infection—HPV DNA positivity, the presence of HPV mRNA, and the detection of HPV DNA methylation. The natural history of HPV infection in the cervical epithelium and the risk of progression and regression are shown in Figure 1.
1.1. What Is Already Known on This Topic?
-Cervical cancer is primarily caused by persistent infection with high-risk human papillomavirus (HPV).-Conventional cytology (cytology) has historically reduced mortality from cervical cancer but has limited sensitivity and reproducibility.-HR HPV testing is increasingly recommended as the primary screening method worldwide.-Molecular markers (HPV mRNA, HPV DNA genotyping, DNA methylation) are considered indicators of persistent HPV infection and are actively assessed for triage and subsequent treatment decisions.
1.2. What This Paper Adds
-This review synthesizes the evolution of diagnostics for persistent HPV infection in the cervix across three research traditions: detection of HR HPV in serial assays, HPV mRNA testing, and assessment of HPV DNA methylation in the cervix.-It presents a perspective on future diagnostics, highlighting molecular markers for screening strategies in the era of diagnostic tragedies and the search for the most convenient methods for patients.-Using a narrative approach, the article integrates diverse scientific paradigms into a coherent account of “yesterday, today, and tomorrow” in the diagnosis of persistent HR HPV infection leading to cervical cancer.
1.3. Aim of the Narrative Review
This study aims to present a narrative review to synthesize available evidence on differences in approaches to molecular diagnostic methods for persistent HPV infection.
1.4. The Specific Review Questions Are
What studies (or epistemic traditions) have addressed inequalities in molecular methods for detecting persistent HPV infection in the cervix?How has each tradition conceptualized this topic, and what methods have they used?What theoretical assumptions about how and why inequalities in methods for detecting persistent HPV infection in the cervix persist are present in these narratives?What changes have been observed in the narratives, and what has prompted these changes?What conclusions can be drawn by combining and comparing the results of different traditions?How does a narrative approach improve understanding of inequalities in molecular methods for detecting persistent HPV infection in the cervix?
1.5. Eligibility Criteria
Studies were included if they met the following criteria:
- Reported original research,
- Investigated molecular markers used to define or assess persistent hrHPV infection in the cervix,
- Addressed HPV DNA detection, HPV oncogene (E6/E7) mRNA expression, or HPV-related DNA methylation,
- Were published in English.
Review articles, analyses, commentaries, discussion papers, conference abstracts, and studies not focused on cervical HPV infection were excluded.
2. Methods
The narrative review was methodologically designed using the RAMSES [8] and Greenhalgh et al.’s [9] methodological guidance for planning, searching, mapping, appraisal, and synthesis. The PRISMA guidelines have been included for complete transparency [10]. PRISMA scheme modified for a narrative review is shown in Figure 2. Three databases (Medline, SCOPUS, and Cochrane Library) were searched for full-text articles published between 2016 and 2025 related to molecular methods for detecting persistent HPV infection in the cervix. Literature reviews, meta-analyses, and discussion papers were excluded. Keywords used during search were as follows: (marker* OR biomarker*) AND (persistent OR persistence OR persist*) AND (cervical) AND (HPV OR “human papillomavirus”). The registration number at the International Prospective Register of Systematic Reviews is 1291648.
Narrative reviews are a growing, increasingly important approach to qualitative and mixed-methods systematic reviews that enable the synthesis of heterogeneous information drawn from different paradigms [8,9]. The six guiding principles of the narrative review—Pragmatism, Pluralism, Historicity, Contestation, Reflexivity, and Peer review—are integrated into the review process as articulated in Table 1. Given the development of diagnostic and detection methods for precancerous conditions and cervical cancer, a narrative review approach will enable researchers to identify, formulate, synthesize, and interpret the diverse literature on various approaches to molecular markers of persistent HPV infection, which is the initial stage of cervical cancer development.
2.1. Selection and Appraisal
Titles and abstracts were screened, and relevant articles were assessed in full by the lead investigator (DP) for eligibility using the technique of survey, question, read, recall, and review. Outcomes were peer-reviewed by project supervisors (JG and RJ), and uncertainties were discussed for consensus. Research articles focusing on molecular markers of HPV persistence were included. Literature reviews, concept analyses, commentaries, and discussion papers were excluded. We also excluded text in languages other than English.
2.2. Data Extraction
Details of included articles (author, year, title, journal, country) and their abstracts (aim, methods, sample, key findings, conclusion) were extracted and compiled into a summary table for this review.
2.3. Data Analysis and Synthesis
Data analysis and synthesis involved an interpretive process of immersion in the data and regular discussions between the research team to consider how the data addressed the research aim, the synthesis of concepts, and the development of narratives [8]. Frequency counts were obtained to describe characteristics of included articles and capture the development of the research topic over time. Interventions and key findings were analysed thematically using an adapted reflexive approach through familiarisation with the data, generating categories, constructing and revising sub-themes, defining themes, and presenting results. Background information was analysed to identify the historical basis for the research (principle of historicity), that is, the research purpose, key molecular markers of HPV infection persistence concepts or assumptions that underpinned the research, and commonly cited authors or works. Research purpose data were categorised into common themes that emerged from the literature.
3. Results
3.1. HPV Genotyping Test
Following Professor Harald zur Hausen’s discovery, numerous investigators focused on detecting human papillomavirus (HPV) DNA in cervical tissue specimens. In 1988, the U.S. Food and Drug Administration (FDA) approved the first commercially available assay for detecting HPV genetic material. In the year 1983, HPV-16, the most oncogenic and prevalent type, was first identified in cervical cancer tissue. Next year, another high-risk HPV-18 genotype was identified. After years of research by Professor Harald zur Hausen on the HPV virus, infection with the highly oncogenic HPV was linked to an increased risk of precancerous conditions. This led to the awarding of the Nobel Prize in Medicine to Professor Hausen’s team in 2008. This prompted research into the application of HPV detection in the cervix in clinical practice.
At the turn of the 1990s and 2000s, the first reports linking persistent HPV infection with the risk of advanced precancerous conditions of the cervix, such as CIN 2+, began to appear. Ho GY et al. were among the first to present results from a cohort study of young women in 1995, showing that most HPV infections are transient. Researchers proved that persistent HPV infections increase the risk of precancer lesions and cervical cancer [10]. The results of another study published in the same year confirmed that the phenomenon of persistent infection with the same HPV genotype carries an increased risk of progression to cervical intraepithelial neoplasia (CIN) [11]. In parallel, HPV genotypes 6 and 11 were also discovered, which were associated with changes that did not cause cervical cancer [12]. Thus, the first division into “oncogenic” and “benign” genotypes was created. In the following years, new HPV genotypes were discovered and sporadically detected in cancers (e.g., HPV 31, 33, 35). Only the results of cohort studies introduced a new category of potentially oncogenic genotypes. The first official classification of genotypes was introduced in 2003 by the International Agency for Research on Cancer, which divided genotypes into Group 1 (oncogenic), Group 2A/2B (probably/potentially carcinogenic), and Group 3 (non-oncogenic) [13]. The final tripartite division of HPV genotypes was published in 2003 in the New England Journal of Medicine, where the classification into oncogenic, potentially oncogenic, and non-oncogenic types was clear [14]. For nearly a quarter of a century, we have been accompanied by the following:
- -high-risk: 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59,
- -probable high-risk: 26, 53, 66, 68, 73, 82,
- -low-risk: 6, 11, 40, 42, 43, 44, 54, 61, 70, 72, 81.
With advances in technology, the Polymerase Chain Reaction (PCR) has been used to detect human papillomavirus. PCR uses fluorescent probes that bind to the amplified DNA, enabling the real-time quantification and detection of specific HPV types. A variant of this method is multiplex PCR, which amplifies multiple HPV types in a single reaction for simultaneous detection and genotyping. The advantages of this method may include high sensitivity and specificity, rapidity, the ability to quantify viral load, and the potential to identify specific viral types (genotyping). On the other hand, high sensitivity can lead to false positives from contamination; some methods are technically complex or costly.
Currently, the two most popular methods are available: the Linear Array test, which uses PCR and hybridization, and the Cobas test, which uses real-time PCR [15,16]. The Linear Array test can detect multiple HPV genotypes with high accuracy, unlike the Cobas method, which detects only a limited number of types. They also differ in the reading method—strips versus digital smears—and the degree of test automation.
Initially, HPV DNA testing was recommended exclusively for women with abnormal cervical cytology categorized as atypical squamous cells of undetermined significance (ASC-US) as part of follow-up, to identify those who would benefit from referral for colposcopic examination. Despite the breakthrough in the diagnosis of cervical precancerous lesions represented by the introduction of HPV DNA testing, researchers encountered a significant limitation: high-risk HPV DNA tests do not directly detect cervical neoplasia but rather indicate an increased risk of its development. These assays do not differentiate between transient and persistent HPV infections. Consequently, HPV DNA testing demonstrates high sensitivity but limited specificity.
Most HPV infections (approximately 80–90%) are transient and do not lead to the development of precancerous conditions or cervical cancer. This typically affects young women, and the infection resolves within 6–24 months. In this case, HPV DNA does not integrate into the host genome. Much less frequently, HPV infection is persistent and leads to the development of SIL. If the same highly oncogenic HPV type persists in the cervix for 12–24 months, it might lead to integration of HPV DNA into the host cell genome.
3.2. HPV mRNA Test
The implementation of screening programs and new molecular techniques for assessing the presence of HPV infection in cervical tissues contributed to a decline in the number of women developing cervical cancer. Similar trends were observed in cervical cancer deaths in the United States and European countries after the 1990s and in the following decade. However, it became necessary to distinguish between incident and persistent infection. While HPV DNA tests were the standard by 2007, with DNA tests like HC2 (Digene, Gaithersburg, MD, USA) approved for co-testing in 2003, the first mRNA HPV tests, like the APTIMA (Gen-Probe, San Diego, CA, USA), and the PreTect HPV-Proofer (detecting E6/E7 mRNA for types 16, 18, etc.) emerged a bit later, used as triage tools, with significant adoption and studies in the late 2000s [17,18,19,20]. These tests began to lead the mRNA protocols by around 2010–2011, offering better specificity than DNA tests. In 2007, mRNA tests and the precise E6/E7 extension were used as molecular markers of HPV oncogenic activity. These tests demonstrated higher specificity than general HPV DNA testing [21]. Currently, there are three most common commercial tests for detecting hrHPV E6/E7 messenger RNA (mRNA). The PreTect HPV-Proofer (NorChip AS, Klokkarstua, Norway) and the NucliSENS Easy Q HPV (bioMérieux, Marcy-l’Étoile, France) are based on the same technology. Still, they are produced by different companies, with small differences in mRNA extraction protocol and data analysis [22,23]. The third one—the APTIMA HPV Assay (Hologic, San Diego, CA, USA)—is a target-amplification nucleic acid probe test for the qualitative detection of E6/E7 viral mRNA [24]. All tests received the CE-IVD mark, and the APTIMA HPV assay is additionally an FDA-approved test. The HPV mRNA tests differ not only in their biological principle but also in the range of genotypes they detect—from a broad, pooled panel of 14 HR-HPV (Aptima, Woburn, MA, USA) to selective detection of the five most oncogenic types—16, 18, 31, 33, 45 (PreTect, NucliSENS), reflecting different strategies for conceptualizing persistent infection.
The advantage of using HPV mRNA tests is their similar sensitivity combined with slightly higher specificity compared to HPV DNA tests for the detection of CIN 2+ lesions [25]. Furthermore, HPV mRNA tests can also be used for follow-up after treatment for CIN lesions (test-of-cure). Limitations of this method include a limited number of detectable genotypes and the fact that they cannot be used combined with self-sampling for cervical cancer screening.
3.3. Dual-Staining p16/Ki67
A separate issue is the dual-staining p16/Ki67, which has recently been proposed as a new triage tool for HPV infections instead of LBC in a population of HPV-positive women [26,27,28]. In 2020, p16/Ki67 DS was approved by the Food and Drug Administration for the triage of HPV-positive women to colposcopy. Many studies have investigated and validated DS’s high detection rate of CIN compared to cytology or co-testing. This relatively novel approach may also have other uses in the cervical cancer screening and management pathway.
3.4. HPV DNA Methylation Test
The late 20th century also saw the development and understanding of epigenetics’ role in cancer. Epigenetic changes (such as DNA methylation or histone modifications) do not alter the DNA sequence, but by influencing gene expression, they play a key role in cancer development. Epigenetic changes can result in the deactivation of tumor suppressor genes (inhibiting growth) or the activation of oncogenes (promoting growth), leading to uncontrolled cell proliferation. The first reports of HPV genome methylation appeared in 1987, when it was observed that HPV DNA integrated into the host genome exhibited epigenetic changes (including methylation). Researchers from Germany published a paper, “The effect of DNA methylation on gene regulation of human papillomaviruses” in 1993 [24]. These data were groundbreaking and suggested that DNA methylation is an important regulatory pathway in modulating HPV expression and, consequently, the proliferation rate of virus-infected cells. Methylation of the HPV genome and host genes is a key epigenetic mechanism associated with long-term infection persistence, viral integration, and progression to CIN3+ and cervical cancer. High methylation of the L1/L2 regions and the CADM1, FAM19A4, and miR124-2 genes is characteristic of transforming infections and has significant diagnostic and prognostic implications.
HPV genome methylation affects cytosines within CpGs in viral DNA and increases with the duration of infection, HPV integration into the host genome, and progression of epithelial lesions. Methylation of the L1/L2 regions (so-called late genes) is low in transient infection, whereas methylation is high in CIN 2+ lesions and cervical cancer. Methylation of these regions correlates with the loss of the productive viral cycle and indicates the transition from the replicative to the transforming phase. Clinically, L1/L2 methylation is one of the best markers of cervical lesion progression. The regulatory gene E2 inhibits the expression of the E6/E7 oncogenes, and E2 methylation leads to loss of E2 control over E6/E7, promoting neoplastic transformation. Regarding the host genome, chronic HPV infection disrupts host cell epigenetics and hypermethylates tumor suppressor gene promoters. This leads to their silencing, loss of proliferation control, and epithelial destabilization. CADM1/FAM19A4/miR124-2 methylation is a molecular biomarker strongly correlated with CIN2+ lesions and progression to cervical cancer and is also used in the triage of HPV-positive patients.
Commercial HPV methylation tests, such as GynTect^®^, QIAsure Methylation Test, and CisCer^®^, measure methylation at specific loci in the viral and host genomes to identify hrHPV-positive women at high risk of CIN2+ or CIN3+ lesions. Unlike DNA and mRNA tests, these panels analyze persistent epigenetic “footprints” of long-term infection, offering high specificity for triaging HPV-positive women.
All identified and analysed studies are described in Table 2.
4. Discussion
The present narrative review demonstrates that the concept of persistent high-risk HPV infection has been shaped by three distinct molecular narratives, each emerging from different scientific traditions and addressing different dimensions of viral persistence. These narratives—persistent DNA positivity, persistent oncogene expression, and persistent epigenetic imprint—reflect an evolving understanding of HPV biology and carcinogenesis, progressing from viral presence to functional activity to long-term cellular reprogramming.
The earliest and most widely implemented narrative, persistent DNA positivity, conceptualizes persistence as the continued detection of HPV DNA during subsequent cervical swabs. This approach, rooted in epidemiology and virology, was instrumental in establishing HPV as the necessary causal factor of cervical cancer and in transforming screening strategies worldwide. Longitudinal cohort studies demonstrated that repeated detection of the same high-risk genotype confers a substantially increased risk of CIN2+ lesions and cervical cancer. However, despite its high analytical sensitivity, HPV DNA testing cannot distinguish between transient and clinically meaningful infections. As a result, this narrative inherently prioritizes sensitivity over specificity, leading to over-referral and the need for additional triage strategies.
In response to these limitations, a second narrative emerged, defining persistence as persistent oncogene expression, measured by detection of E6/E7 mRNA. This paradigm represents a conceptual shift from viral presence to viral activity. By focusing on transcriptional activity directly responsible for cell cycle deregulation and malignant transformation, mRNA-based assays better align with the biological mechanisms underlying disease progression. Consequently, HPV mRNA testing offers higher clinical specificity for CIN2+ lesions. Nevertheless, this approach captures only infections with ongoing oncogenic transcription and may fail to identify lesions in which viral activity is intermittent or has already induced downstream cellular alterations.
The most recent narrative, persistent epigenetic imprint, extends the concept of persistence beyond real-time viral detection to encompass the cumulative biological consequences of long-term infection. DNA methylation of viral regions (L1/L2, E2) and host tumor suppressor genes (e.g., CADM1, FAM19A4, miR124-2) reflects sustained exposure to oncogenic stimuli, viral integration, and transition from productive to transforming infection. Importantly, methylation-based markers are less dependent on current viral transcription and instead capture a stable molecular footprint of past and ongoing oncogenic processes. This characteristic explains their strong association with CIN3+ and invasive cancer and their high specificity in triage of HPV-positive women.
These three narratives should not be interpreted as competing diagnostic strategies but rather as complementary perspectives along a continuum of molecular persistence. HPV DNA positivity identifies viral presence, HPV mRNA expression indicates active oncogenic interference, and DNA methylation marks the accumulated epigenetic consequences of prolonged infection. This integrative framework clarifies why some HPV DNA–positive but mRNA–negative infections may still progress and why methylation markers can predict progression even in the absence of detectable viral transcription.
In conclusion, the narrative approach reveals that advances in HPV diagnostics mirror a broader conceptual evolution—from detecting the virus, to understanding its activity, to recognizing its lasting molecular legacy. Future screening and triage strategies are likely to benefit most from integrative models that combine these narratives, rather than privileging any single biomarker in isolation.
5. Conclusions
Molecular markers of HPV persistence reflect an evolving understanding of cervical carcinogenesis, progressing from viral presence to functional activity and stable epigenetic reprogramming. Integrating these complementary approaches may improve risk stratification and future HPV-based screening strategies. In particular, combining viral detection methods with host epigenetic biomarkers may allow for more precise identification of infections with true oncogenic potential. Further prospective studies and clinical validation are required to determine the optimal integration of these markers into routine cervical cancer screening and triage algorithms.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Purandare C.N. Cervical Cancer Elimination. 90:70:90. Together We Can J. Obstet. Gynecol. India 20247429229410.1007/s 13224-024-02052-x 39280207 PMC 11399510 · doi ↗ · pubmed ↗
- 2Huber J. Mueller A. Sailer M. Regidor P.-A. Human papillomavirus persistence or clearance after infection in reproductive age. What is the status? Review of the literature and new data of a vaginal gel containing silicate dioxide, citric acid, and selenite Women’s Health 2021171745506521102070210.1177/17455065211020702 PMC 878528734096424 · doi ↗ · pubmed ↗
- 3Wang S.S. Zuna R.E. Wentzensen N. Dunn S.T. Sherman M.E. Gold M.A. Schiffman M. Wacholder S. Allen R.A. Block I. Human Papillomavirus Cofactors by Disease Progression and Human Papillomavirus Types in the Study to Understand Cervical Cancer Early Endpoints and Determinants Cancer Epidemiol. Biomark. Prev.20091811312010.1158/1055-9965.EPI-08-0591 PMC 295243019124488 · doi ↗ · pubmed ↗
- 4Gao W. Weng J. Gao Y. Chen X. Comparison of the vaginal microbiota diversity of women with and without human papillomavirus infection: A cross-sectional study BMC Infect. Dis.20131327110.1186/1471-2334-13-27123758857 PMC 3684509 · doi ↗ · pubmed ↗
- 5Kwasniewski W. Wolun-Cholewa M. Kotarski J. Warchol W. Kuzma D. Kwasniewska A. Gozdzicka-Jozefiak A. Microbiota dysbiosis is associated with HPV-induced cervical carcinogenesis Oncol. Lett.2018167035704710.3892/ol.2018.950930546437 PMC 6256731 · doi ↗ · pubmed ↗
- 6de SanjoséS. Brotons M. Pavón M.A. The natural history of human papillomavirus infection Best Pract. Res. Clin. Obstet. Gynaecol.20184721310.1016/j.bpobgyn.2017.08.01528964706 · doi ↗ · pubmed ↗
- 7Betz S.J. HPV-Related Papillary Lesions of the Oral Mucosa: A Review Head Neck Pathol.201913809010.1007/s 12105-019-01003-730693456 PMC 6405797 · doi ↗ · pubmed ↗
- 8Wong G. Greenhalgh T. Westhorp G. Buckingham J. Pawson R. RAMESES publication standards: Meta-narrative reviews J. Adv. Nurs.201369987100410.1111/jan.1209223356699 · doi ↗ · pubmed ↗